Embed Size (px)
Citation preview

Emergency Medical Retrieval ServiceEmergency Medical Retrieval Service
Dr Pete Davis Dr Pete Davis MRCGP FACEM Dip IMC Dip Mtn MedMRCGP FACEM Dip IMC Dip Mtn Med
Emergency Physician Emergency Physician Southern General Hospital GlasgowSouthern General Hospital Glasgow

2
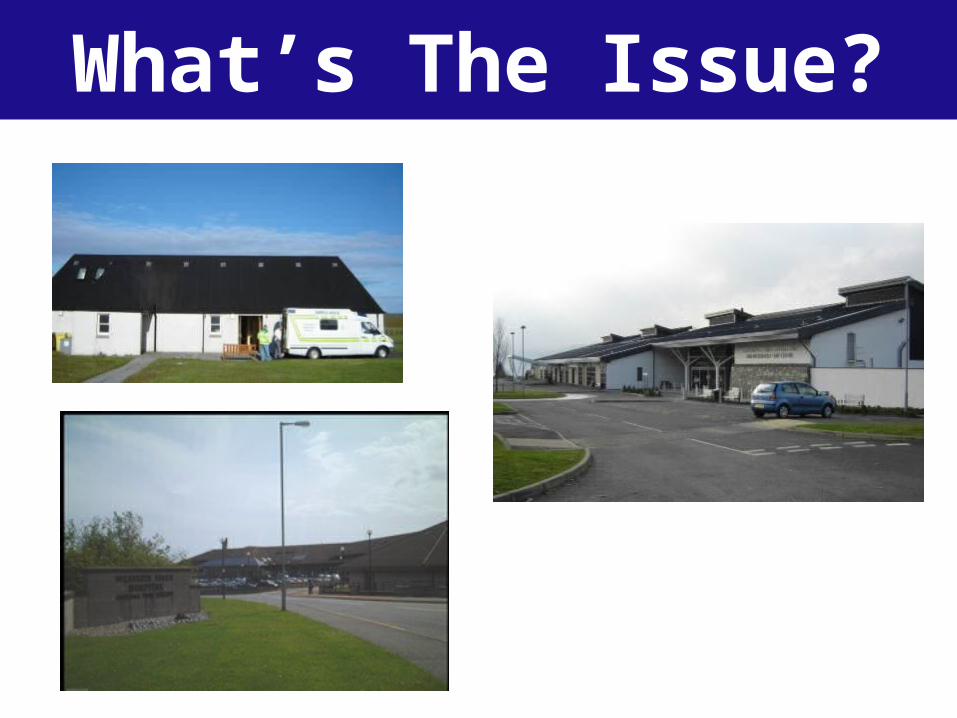
What’s The Issue?

• Snapshot of 3 months in 2004
• All A&B air transfers
• 161 patients
• 9% critically ill or injured
• 5% deteriorated in flight
• 3 cardiac arrests in flight
Aeromedical Activity Audit In Argyll & Bute Prior To EMRS

• 40 patients • 34 transferred to definitive care• 45% trauma • 60% required critical care • 40% other procedure
– chest drain, cardioversion or cardiac pacing
• 40% required drugs not available to paramedics
• > 90% of patients required medical intervention• No critical morbidity or mortality during transfer• Two patients died < 24 hours following transfer
A&B EMRS 12 Month Pilot 2004

Quality Quality pre-hospital & pre-hospital & intermediate intermediate
carecare
Direct triageDirect triageSafe transferSafe transfer
Stabilisation Stabilisation & critical care & critical care interventions interventions
ASAPASAP
What Do Patients Need?

Limited pre-transfer stabilisation
Limited patient assessment in transfer
Limited monitoring
Limited communication
Few if any interventions possible
Airway protection/ compromiseAirway protection/ compromise
Risks to medical personnel
Why Is Transfer Dangerous?

8
• Rural practitioners have suggested it
• Paramedic-delivered service suboptimal
• Ad-hoc retrievals are hazardous
• Take “ER” to the patient
• Maintain level of care throughout transfer
• Optimal triage to definitive care
Why Have A Retrieval Service?Why Have A Retrieval Service?

9
• Patient assessment
• Point-of-care investigations– US, Bio, Haem
• Critical care intervention– RSI, ventilation, inotropes
• Optimised physiology
• Invasive monitoring
• Direct triage
• Safe transfer
EMRS = Consultant & ParamedicEMRS = Consultant & Paramedic

Which Patients?•Ventilated patients
•High dependency patients
•Patients with deranged physiology
•Patients with identified major injury
•Patients with possible occult major injury
•If in doubt - please phone and discuss
•To date 2/3 medical : 1/3 trauma

EMRS patients by diagnosis
Trauma33%
CVS15%
Neuro15%
Sepsis12%
Poisoning10%
Other15%
Which Patients?

“Adults with life threatening illness or injury where advanced
medical intervention is appropriate to facilitate safe
transfer”
“On-Line Senior Support!”
ActivationActivation

Retrieval Cons
Rural Dr
ActivationActivation
Single point of contact; RAH switchboard
0141 887 9111

Retrieval Cons
Rural Dr
ActivationActivation
Consultant in RGH

Retrieval Cons
Rural Dr
Definitive care
Retrieval
ActivationActivation

Retrieval Cons
Rural Dr
Paramedic
Definitive care
Retrieval
ActivationActivation

Retrieval Cons
Rural Dr
Paramedic
Definitive care
Retrieval
MissedRetrieval
ActivationActivation

Retrieval Cons
Rural Dr
Advice only
Local care
ActivationActivation

19
““This will mean integrated working with This will mean integrated working with primary and secondary care in these areas.”primary and secondary care in these areas.”
““The Scottish Ambulance Service should….develop The Scottish Ambulance Service should….develop integrated solutions to particular healthcare integrated solutions to particular healthcare
challenges, for example in rural and remote areas” challenges, for example in rural and remote areas”

Comparison of "team ready" & "team airborne"
0
0.05
0.1
0.15
0.2
0.25
1 6 11 16 21 26 31 36 41 46 51 56 61
Mission number
ho
urs
Time from call toairborne
Time from call toteam ready
Response Time IssuesResponse Time Issues
3
2
1

21

EMRS PilotEMRS Pilot
•18 month SGHD funded pilot
•Independent evaluation
•Outcomes will influence evolution

•Clear role for EMRS
•Rural MI is different from Urban MI
•Early activation is crucial
•Specific areas of expertise:
•Liaison with aeromedical assets (MOD / SAS)
•Provide site medical teams (MERIT teams)
•Assist with triage and disposition
Rural Major IncidentsRural Major Incidents

Questions?
25