Embed Size (px)
DESCRIPTION
Emergency Medical Countermeasures Development and Acquisition BARDA’s Role and Biodosimetry Ronald G. Manning, Ph.D. Chief, Chemical, Radiological and Nuclear Medical Countermeasures Project BioShield Biomedical Advanced Research and Development Authority (BARDA). - PowerPoint PPT Presentation
Citation preview

Emergency Medical Countermeasures Emergency Medical Countermeasures Development and AcquisitionDevelopment and Acquisition
BARDA’s Role and Biodosimetry BARDA’s Role and Biodosimetry
Ronald G. Manning, Ph.D.Chief, Chemical, Radiological and Nuclear
Medical CountermeasuresProject BioShield
Biomedical Advanced Research and Development Authority (BARDA)

ASPR HHS Assistant Secretary forPreparedness and Response (ASPR)
ASPR
Office of Medicine,Science,
& Public Health
Office of Policy & Strategic
Planning
Immediate Office of the ASPR
Biomedical Advanced Research
& Development Authority
Office of Preparedness &
Emergency Operations
Vision: A nation prepared to prevent, respond to and reduce the adverse health effects of public health emergencies and disasters.
Mission: Lead the Nation in preventing, preparing for and responding to the adverse health effects of public health emergencies and disasters.

ASPR
3
BARDA: Roles and Responsibilities
Coordinates an integrated, systematic approach to planning for, and executing research, development and acquisition of medical countermeasures for public health emergencies
Supports the ASPR in leading the Public Health Emergency Medical Countermeasure Enterprise (PHEMCE)
Drives medical countermeasure analysis and prioritization– HHS PHEMCE Strategy for CBRN Threats– HHS PHEMCE Implementation Plan for CBRN Threats
Executes advanced development and acquisition of medical countermeasures for CBRN threats and pandemic influenza
– Advanced development under BARDA– Acquisition under Project BioShield (CBRN material threats)– Acquisition with direct appropriations for pandemic influenza
CBRN: chemical, biological, radiological, and nuclear

ASPR HHS Public Health EmergencyMedical Countermeasures Enterprise
BARDANIH CDC CDC and OPEO
UtilizationResearch and Development
Advanced Development Acquisition Storage/
MaintenanceBiosurveillance/
Detection
PHEMCE COORDINATED PLANNING& EXECUTION
BARDA and CDC
National Biodefense Science Board
Deployment
CDCand DHS
FDA

ASPR
Purpose: To coordinate across the full spectrum of public health emergency preparedness activities for all intentional and naturally occurring threats Established by HHS in July 2006
HHS Public Health Emergency Medical Countermeasures Enterprise
Interagency partners include:Department of DefenseDepartment of Homeland SecurityVeterans Administration

ASPR Defining and Prioritizing Medical Countermeasure Development and Acquisition Programs
Scoping the Mission
Develop medical countermeasures that
are deployable and readily dispensable
Address a diverse set of threats:
CBRN and Influenza
Consider the needs of a large, diverse population
Prioritize acquisition and advanced
development programs with limited funding
Face product development challenges:
lengthy, risky, and expensive

ASPR Maximizing Opportunities for Collaboration Building a True Enterprise
Bring together medical and public health assets more effectively Measurement is vital
Build capacity to perform best practices Provide coordinated federal assistance to
supplement state, tribal, and local resources in response to public health and medical care needs

ASPR Establishment of Medical Countermeasure Requirements
HHS will establish concepts of operations (“conops”), including storage, maintenance, utilization policies and deployment plans for each medical countermeasure in the context of all available consequence mitigation strategies and capabilities.
HHS will define specific medical countermeasure requirements, including product specifications consistent with US Government storage plans and operational capabilities for deployment and utilization by federal, state, and local authorities.

ASPR
Plague Antibiotics
Smallpox Smallpox
vaccines (MVA and ACAM2000)
Vaccinia Immune Globulin (VIG)
Tularemia Antibiotics
Anthrax AVA Vaccine Oral ciprofloxacin Doxycycline Amoxicillin Other IV antibiotics Human polyclonal
antibody
Botulism Antitoxins from legacy
DOD program and legacy CDC/Cangene program
Other monovalent and bivalent antitoxins
Medical Countermeasure Preparedness for CBRN Threats
BIOLOGICAL THREATS
KI tablets and Pediatric KIPrussian BlueCytokinesAntibioticsAnti-emeticsBlast and burn suppliesCa & Zn DTPA
RADIOLOGICAL / NUCLEAR THREATS
CHEMICAL THREATS CHEMPACKs

ASPR
Radiological/Nuclear Threats
Nuclear Detonation Radiologic dispersive
devices (“dirty bombs”)
Industrial and shipping accidents Power plant releases Food and medical
irradiators Sealed sources

ASPR
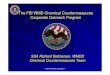
11adapted from: Blood, 15 June 2008, Vol. 111, No. 12, pp. 5440-5445.
IND Models for a 10 KT event estimate 1.8 million affected 1 million may seek information on their personal risk (dosimetry), Hundreds of thousands estimated to receive > 2 Gy if event occurs in a large metropolitan area
Radiation Exposure Events
Event Description Potential Numbers Affected
Radioactive Source Accident
Hospital irradiation source (Co-60)Industrial x-ray source (Ir-192)
Example: Goiania (Cs-137 source)individuals to many
Nuclear Reactor Accident
Release of radioactive materialExample: Chernobyl
individuals to hundreds(can cover large
geographical area)RDD –
Radiological Dispersal Device, “Dirty Bomb,” or Exposure Device
Improvised explosive device containing radioactive material May include food chain contamination Cs-137 or Ir-192 sources on a subway
individuals to thousands
Improvised Nuclear Device
(IND)
A true, or assembled, nuclear device capable of a nuclear detonation thousands to > 1 million

ASPR
12
NO mass casualty biodosimetry capabilities at this time
12
Triage and Patient Monitoringafter an IND Event
TRIAGE People requiring immediate medical intervention (burns, fractures,
blood loss) People receiving radiation doses > 2 Gy (risk of hematological ARS) Concerned citizens Expectant (likely to die)
Complications: Many inhomogeneous irradiations (partial body exposures)
Correct triage and treatment depends on rapid and accurate radiation dose estimates
Currently a multi-parametric approach is used to estimate radiation dose: Location relative to event Time from event to first emesis Peripheral blood lymphocyte counts & depletion kinetics (hours to
days) The utility of these measures in response to an IND event is not clear.

ASPR
13
Current Biodosimetry Capacity
Biodosimetry capability will be integral to triage, treatment, and medical management of radiation-exposed individuals.
Dose evaluation based on clinical signs and symptoms can lead to a high level of false positives and lead to unneeded treatment.
The "gold standard" for biodosimetry is chromosomal aberrations (i.e. dicentrics).
Dicentric quantificationo requires several days to perform;o is labor intense;o is only available in specialized centers (a Laboratory Response
Network is in development).
Immediate need: Rapid dose assessment tools or bioassays.

ASPRCBRN Dosimetry Objectives
Pursue diagnostic capabilities for dose determination
Physical dosimetry tools for exposure Rapid biodosimetry assays to estimate doses >2 Gy Rapid biodosimetry assays to determine dose 1 – 20 Gy Gold standard assays using novel biomarkers
– i.e. organ-specific radiation injury/susceptibilities Rapid determination of radionuclide exposure and body
burden
14

ASPR
Contact Information:
www.hhs.gov/aspr/barda
www.medicalcountermeasures.gov
ANY QUESTIONS?????