Embed Size (px)
Citation preview

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 1/202
Emergency in medicine
4 April 2012

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 2/202
Scope
Cardiopulmonary resuscitation
Cardiac arrhythmia
Acute coronary syndrome
Fast track MI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 3/202
Cardiopulmonary
resuscitation

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 4/202
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 5/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 6/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 7/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 8/202
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 9/202
VF/ Pulseless VT

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 10/202
Ventricular Fibrillation
Multiple ventricular foci rapidly discharge
producing a totally erratic ventricular
rhythm without identifiable waves

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 11/202
Ventricular tachycardia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 12/202
Ventricular Tachycardia (VT)
•Regular rhythm (may be slightly irregular)•Rate ~150-250/min
•Wide QRS complex

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 13/202
Polymorphic VT
+ Prolong QT = Torsades de pointes

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 14/202
Defibrillation Provide most effective
treatment for
ventricular fibrillation
as soon as possible

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 15/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 16/202
Manual Defibrillator

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 17/202
Manual Defibrillators

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 18/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 19/202
1.Turn on or monitor on
Step Manual Defibrillation

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 20/202
2. Set lead select•Paddle lead
•Lead I, II, III

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 21/202
3. Analyze rhythm
4. If VF or pulseless VT Defibrillation

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 22/202
Select energy level•Monophasic :360J
•Biphasic:120-200 J
(If unknown use 200J)

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 23/202
5. Apply gel to paddle
or use adhesive pad6. Apply paddle or pad
at correct position

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 24/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 25/202
7.Charge defibrillator by
•Press button on control panel
•Or at right hand apex paddle

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 26/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 27/202
8. When fully charged : voice &
number
9. Say One , I am clear Two , you are clear
Three , everybody is clear

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 28/202
10. Press 2 discharge button simultaneously
11. Check monitor. If VF/VT remains , startCPR for 5 cycles
VF/P l l VT

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 29/202
VF/Pulseless VT Give 1 shock •Manual biphasic:120-200J•Monophasic:360J• AED: device specificResume CPR immediately
Shockable rhythm?
•Give 1 shock •Resume CPR immediately after the shock
• Vasopressor when IV/IO available•Epinephrine 1mg IV/IO every 3-5 min or• Vasopressin 40 U IV/IO
Give 5 cycles of CPR
Shockable rhythm?
Give 5 cycles of CPR
Shockable
•Give 1 shock •Resume CPR immediately after the shock
•Consider antiarrhythmics• Amiodarone 300 mg IV/IO then consider additional 150 mg IV/IO•Lidocaine (1-1.5 mg/kg then 0.5-0.75 mg/kg IV/IO)
•Magnesium 1-2 g IV/IO for torsades de pointes
Shockable

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 30/202
Asystole/ PEA

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 31/202
Asystole

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 32/202
Confirm true asystole
Check lead & cable connections
Monitor power on?
Monitor gain up?
Verify asystole in another lead?

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 33/202
Pulseless Electrical activity
(PEA)Electrical mechanical dissociation
Treatment goal is to bring back perfusion
(pulse and blood pressure)Correct the reversible cause is the key
factor for success resuscitation
The process is to perform cardiopulmonarysupport and try to identify and correct the
causes

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 34/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 35/202
Search for & treat possible
contributing factors
5HHypovolemia
Hypoxia
Hydrogen ion
(acidosis)
Hypo/hyperkalemia
Hypoglycemia
Hypothermia
5TToxins
Tamponade (cardiac)
Tension
pneumothorax
Thrombosis (coronary
or pulmonary)
Trauma
(hypovolemia,increased ICP)

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 36/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 37/202
Key changes from the 2005 ACLS
Guidelines
Continuous quantitative waveform capnography for confirmation andmonitoring of endotracheal tube placement
Emphasize the importance of high-quality CPR (including chest
compressions of adequate rate and depth, allowing complete chestrecoil after each compression, minimizing interruptions in chestcompressions and avoiding excessive ventilation)
Atropine is no longer recommended for routine use in themanagement of pulseless electrical activity (PEA)/asystole
There is an increased emphasis on physiologic monitoring tooptimize CPR quality and detect ROSC

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 38/202
Cardiac arrhythmia
Tachyarrhythmia
Bradyarrhythmia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 39/202
Approach to cardiac arrhythmia
Rhythm –
qu ick look
Flat l ine
Use electrod e and loo k for 2 leads
Look for connect ion
Sti l l f lat l ine
= Asysto le
VF QRS com plex
Rate > 100
Tachycardia
Rate < 60
Bradycard ia
Narrow QRS Wide QRS
Regular Irregular
SVT
Regular Irregular
AF
Atr ial f lut ter
MAT
VT
SVT with
aberrant
SVT with BBB
AF
with
WPW

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 40/202
Tachyarrhythmia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 41/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 42/202
Tachyarrhythmia-Management in CPR
Identify the hemodynamic effects of tachyarrhythmia
Electrical therapy should be
performed at any time if the patientbecomes unstable.
Antiarrhythmic medication could be
used initially in stable tachyarrhythmia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 43/202
Unstable Tachycardia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 44/202
Cardioversion
St C di i

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 45/202
Step Cardioversion
! Consider sedation
1. Turn on or Monitor on
2. Attach monitor leads
3. Press “ sync ” button at control panel 4. Look for marker on R wave
5. Adjust monitor gain until sync marker occur
6. Select energy level and charge
7. Apply gel and place paddle at correct position
8. Clear : One , Two , Three

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 46/202
9. Press discharge botton10. Analyze rhythm again
Narrow regular 50-100 jNarrow irregular 120-200 j (Bi), 200 j (Mo)
Wide regular 100 j
Wide irregular Defib

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 47/202
Synchronized

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 48/202
Narrow QRS complex
Wide QRS complex
Stable Tachycardia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 49/202
Narrow QRS-ComplexTachycardia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 50/202
Narrow Complex Tachycardia
Regular Irregular
No P waveP wave
-AF-PAC
-MAT
-AT with block
-A.Flutter + block
A.Flutter 2:1
PSVT-AVNRT
-AVRT
-AT
Sinus tachycardia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 51/202
Irregular Narrow QRS-
Complex Tachycardia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 52/202
Atrial Fibrillation (AF)
Irregular rhythm
Not seen P wave
(fibrillate baseline)
Atrial rate ~350-500/min
Ventricular ratevariable

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 53/202
Atrial Fibrillation (AF)
•Irregular rhythm
•Not seen P wave (fibrillate baseline)
• Atrial rate ~350-500/min
•Ventricular rate variable

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 54/202
Atrial Flutter
Regular or irregular
rhythm
Atrial rate 250-
350/minVentricular rate 1/2,
1/3, … of atrial rate
“Saw tooth”
appearance
AV block 2:1, 3:1,…

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 55/202
Atrial Flutter
•Regular or irregular rhythm
• Atrial rate 250-350/min
•Ventricular rate 1/2, 1/3, … of atrial rate
•“Saw tooth” appearance
•AV block 2:1, 3:1,…

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 56/202
Recommendations for Pharmacological or
Electrical Cardioversion of AF
Class I
1. Immediate electrical cardioversion in patients with
paroxysmal AF and a rapid ventricular response who have
ECG evidence of acute MI or symptomatic hypotension,angina, or HF that does not respond promptly to
pharmacological measures. (Level of Evidence: C )
2. Cardioversion in patients without hemodynamicinstability when symptoms of AF are acceptable.
(Level of Evidence: C )

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 57/202
Electrical cardioversion
Synchronized mode, Initial energy 200 J
Increments of 100 J until a maximum of
400 J
Lower energies are required with biphasicwaveforms
Interval between 2 consecutive shocks
should not be < 1 min.

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 58/202
Risk & Complication of electrical
cardioversion
Embolism
– 1-7% : if no prophylactic anticoagulant before
cardioversion
Arrhythmia
– Hypokalemia
– Digitalis intoxication
Myocardial Injury
– Transient ST elevation and small increased bloodlevel of CK-MB.
– Probably not clinically significant

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 59/202
Prophylaxis of Thromboembolism
before Cardioversion
Anticoagulate patients with AF lasting more than 48 h or of unknown duration, for at least 3 to 4 weeks before
and after cardioversion (INR 2 to 3).
Screening for the presence of thrombus in the LA or LAA by TEE is an alternative for routinepreanticoagulation in candidates for cardioversion of AF.
M di l i At i l fib ill ti

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 60/202
Medical conversion Atrial fibrillation
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 61/202
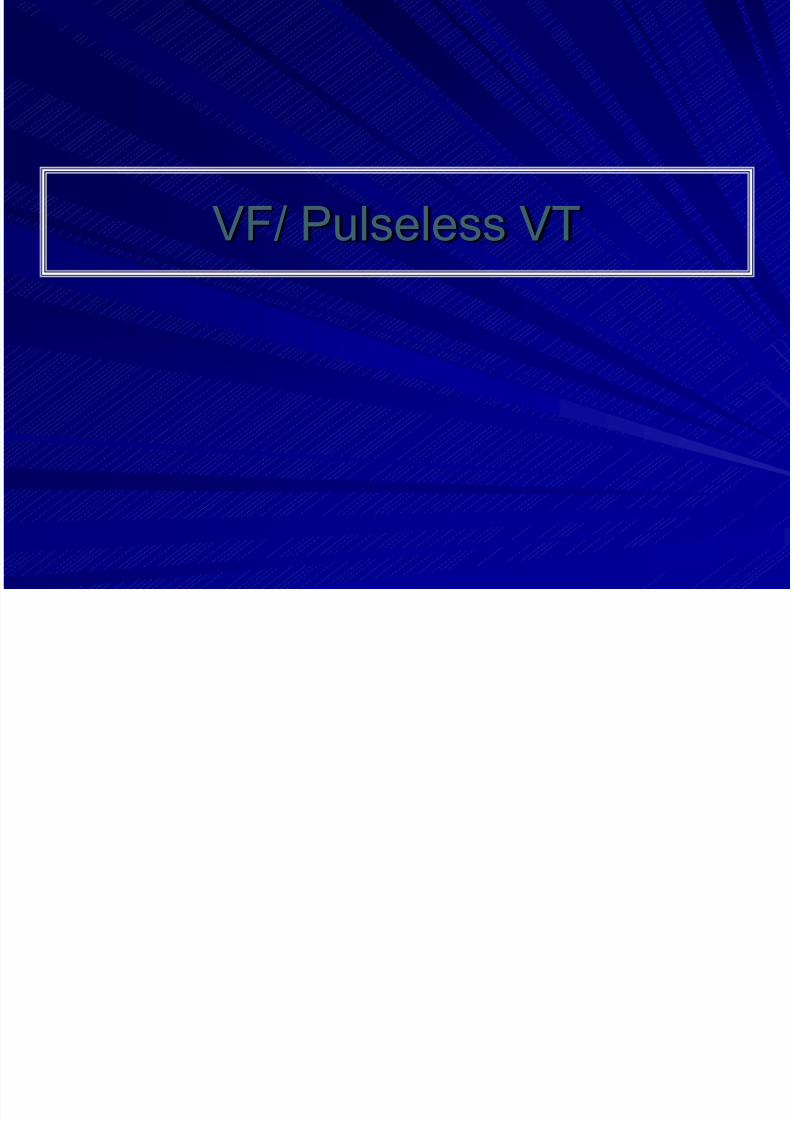
Typical Doses of Drugs Used to Maintain Sinus Rhythm
in Patients With Atrial Fibrillation

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 62/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 63/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 64/202
Anticoagulant
CHADS2 ( CHF , HT , age > 75 yrs , DM ,stroke ) ≥ 2
no contraindication
keep INR 2-3

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 65/202
Vascular disease (prior MI, PAD, Aortic plaque ) ESC 2010

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 66/202
Regular Narrow QRS-
Complex Tachycardia
Paroxysmal Supraventricular

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 67/202
Paroxysmal Supraventricular Tachycardia (PSVT)
Rate ~150-250/min,Regular rhythm
Abrupt onset &termination
Not seen sinus Pwave (usually notseen P wave or retrograde P wave)
Usually narrow QRScomplex
Paroxysmal Supraventricular

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 68/202
Paroxysmal Supraventricular Tachycardia (PSVT)
•Rate ~150-250/min, Regular rhythm
•Usually narrow QRS complex
•Abrupt onset & termination
•Not seen sinus P wave (usually not seenP wave or retrograde P wave)
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 69/202
Management
Unstable VS : sedation+Cardioversion synchronized
biphasic 50-100 j , adenosine
Stable VS : Adenosine 6 mg rapidly iv if ineffective within 1-2 min give 12 mg
Nausea,light-headedness,flushing
Contraindication in asthma, second or third degree AV
block , sick sinus syndrome
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 70/202
Management
Diltiazem 0.25 mg/kg over 2 min, further 0.35 mg/kg after 15 min if
required
Initial infusion 5-10 mg/hr , increased 5-15 mg/hr up to
24 hr, maintainance 120-360 mg oral daily
Verapamil 5-10 mg slowly iv (over 2-3 min) repeated 10 mg in 10-
15 min , oral maintainance 120-480 mg daily divided in
3-4 doses
Contraindication in hypotension , bradycardia , wide
complex tachycardia , VT
Narrow QRS

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 71/202
Narrow QRS
• Attempt vagal maneuvers•Give adenosine 6 mg IV push.If no conversion give 12 mg IV push
Irregular Narrow-ComplexTachycardia AF/atrial flutter/MAT•Consider expert consultation•Control rate
Convert?
If rhythm convertsProbable reentry SVT
If rhythm does not convertPossible atrial flutter, atrial tachycardia,
junctional tachycardia
Regular Irregular
Converts Does not convert

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 72/202
Wide QRS-ComplexTachycardia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 73/202
Approach to wide complex tachycardia
History of MI favor VT
Age,rate and hemodynamic cannot differentiate
Differential diagnosis of wide complex tachycardia
1) Ventricular tachycardia
2) SVT with aberrant conduction
3) SVT with preexisting bundle branch block
4) circus movement tachycardia in WPW

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 74/202
Clues for VT
AV dissociation
Fusion beat
Capture beat
Axis : No man’s land , LBBB with RAD
QRS morphology
Precordial concordance : negative specific more
than positive

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 75/202
AV dissociation in VT
VA conduction are also seen
Positive concordance

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 76/202
VT N ’ l d

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 77/202
VT – No man’s land

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 78/202
Management
Amiodarone Oral loading dose 1200-1600 mg daily , maintainance
200-400 mg daily
Intravenous loading 150 mg over 10 min then 360 mg
over 6 hr then 560 mg over remaining 18 hr then 0.5
mg/min
Contraindication in severe bradycardia , prolong QT
V t i l T h di (VT)

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 79/202
Ventricular Tachycardia (VT)
•Regular rhythm (may be slightly irregular)
•Rate ~150-250/min
•Wide QRS complex
P l hi VT

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 80/202
Polymorphic VT
Like VT but QRS complexes different inmorphology
Typical: QRS complexes spiral around the
baseline, changing their axis andamplitude.
Polymorphic VT + prolong QT interval =
Torsades de pointes

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 81/202
Bradyarrhythmia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 82/202
Bradyarrhythmia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 83/202
Bradyarrhythmia
Sinus node dysfunction AV block
1st degree AV block
2nd degree AV block
3nd degree AV block
2nd degree AV block type I
2nd
degree AV block 2:1
2nd degree AV block typeII
Advanced 2nddegree AV block
Sinus arrest /pause
Sinus exit block
Sinus bradycardia
Tachy-brady syndrome

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 84/202
E Rh th

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 85/202
Escape Rhythms
Escape beats= rescuing beats originatingoutside the sinus node
AV Node (junctional rhythm): 40 to 60
beats/minute , narrow QRS
Ventricles: 30 to 40 beats/minute , wide
QRS

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 86/202
Sinus bradycardia
Sinus rhythm
Rate<60/min

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 87/202
Sinus Arrestand SA Exit
Block
T h b d d

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 88/202
Tachy-brady syndrome
J ti l h th
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 89/202
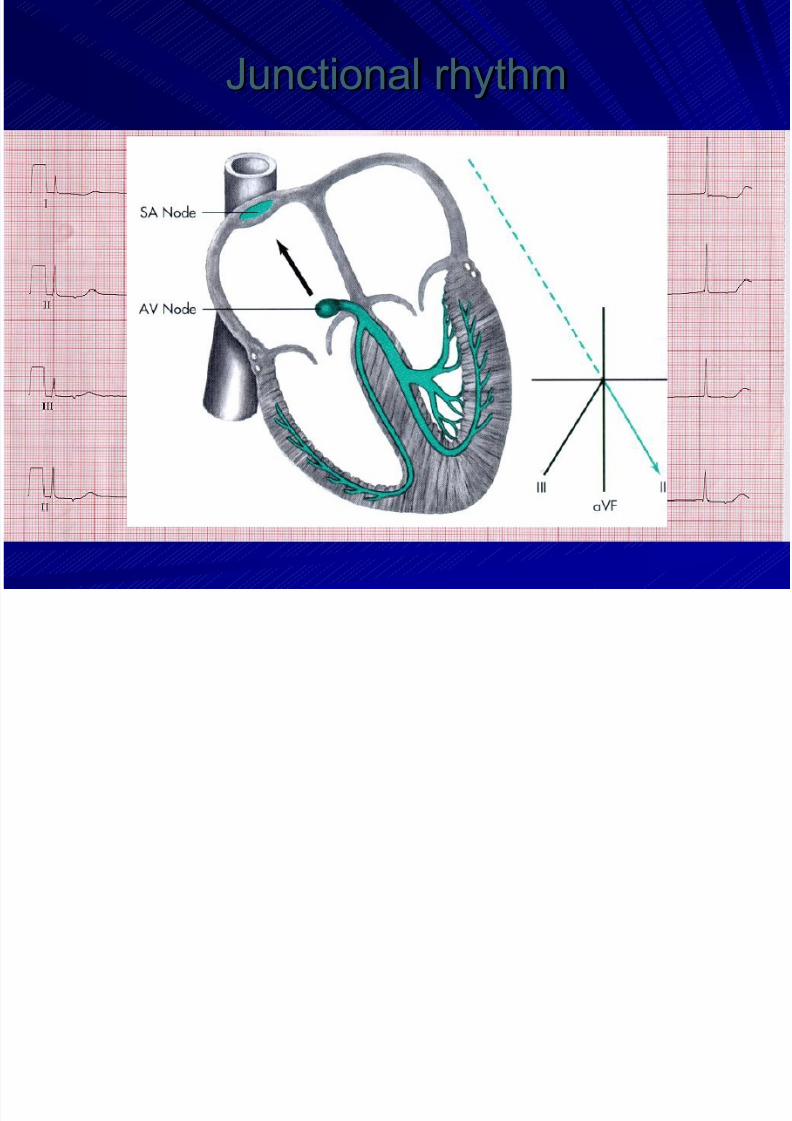
Junctional rhythm
J ti l h th

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 90/202
Junctional rhythm
Rate 40-60/min
Most often not seen P wave (Occasional
retrograde P wave)
Narrow QRS complex
Idio entric lar rh thm

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 91/202
Idioventricular rhythm
Rate 30-40 /min
Wide QRS complex
AV Block

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 92/202
First degree AV block
Second degree AV block
– Type I (Wenchkebach)
– Type II
– 2:1 second degree AV block
– Advanced second degree AV block
Third degree AV block
AV Block
1st DEGREE AV BLOCK

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 93/202
1st DEGREE AV BLOCK
PR interval >0.2 sec
All beats are conducted through to the ventricle
2nd DEGREE AV BLOCK: Mobitz

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 94/202
type I (Wenckebach)
Progressive prolongation of the PR interval until
a QRS is dropped
2nd DEGREE AV BLOCK: Mobitz

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 95/202
type II
QRS complexes are dropped at regular intervals
without prolongation of the PR interval
2nd DEGREE AV BLOCK 2:1

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 96/202
2nd DEGREE AV BLOCK 2:1
2 sinus P wave: 1 QRS complex
Constant PR interval(Impossible to tell whether it is Mobitz I or II)
High grade AV block

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 97/202
g g
(Advanced AV block)
≥ 3:1 AV block
Constant PR interval
Third degree AV block

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 98/202
Third degree AV block
No beats are conducted through to the
ventricles.
AV dissociation: atrium and ventricles are driven
by independent pacemakers
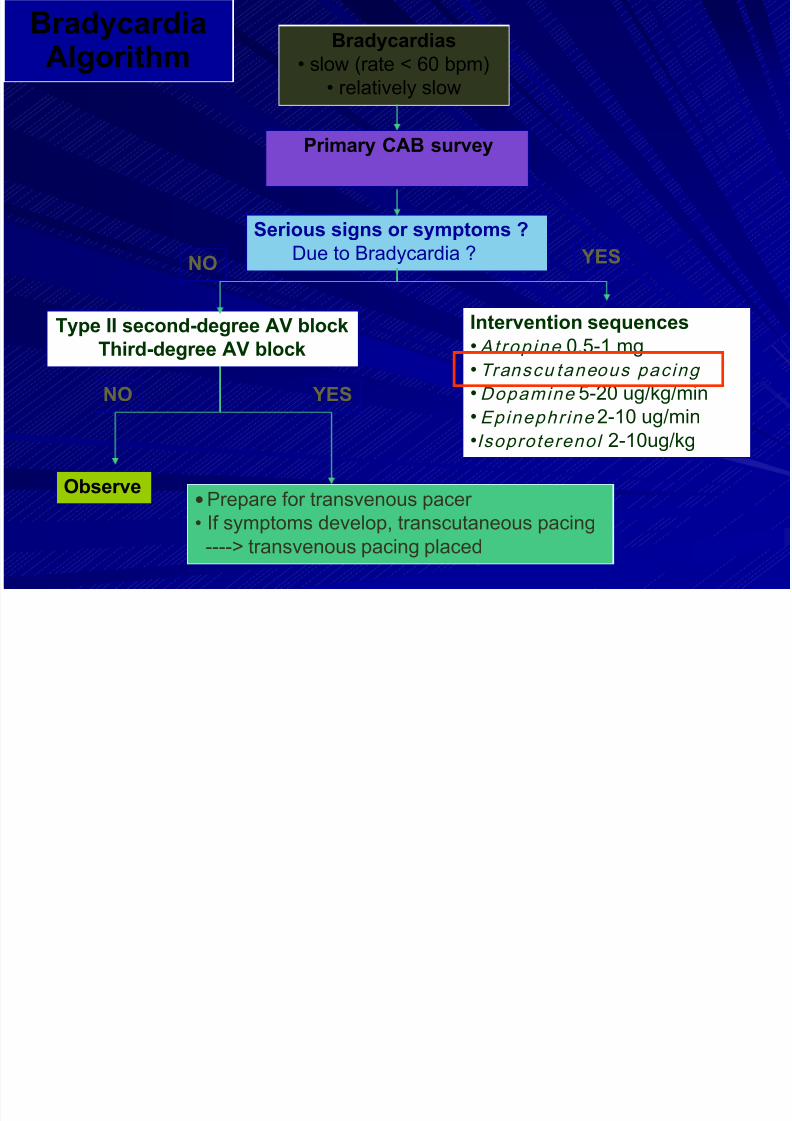
Bradycardias
• slow (rate < 60 bpm)
BradycardiaAlgorithm
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 99/202
( p )
• relatively slow
Primary CAB survey
Serious signs or symptoms ?
Due to Bradycardia ?
Type II second-degree AV block
Third-degree AV block
Intervention sequences
• Atrop ine 0.5-1 mg
• Transcu taneous pacing
• Dopamine 5-20 ug/kg/min
• Epinephr ine 2-10 ug/min
•Isoproterenol 2-10ug/kg
Observe • Prepare for transvenous pacer
• If symptoms develop, transcutaneous pacing
----> transvenous pacing placed
NO YES
NO YES
g
Search for & treat possible
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 100/202
contributing factors
5HHypovolemia
Hypoxia
Hydrogen ion
(acidosis)
Hypo/hyperkalemia
HypoglycemiaHypothermia
5TToxins
Tamponade (cardiac)
Tension
pneumothorax
Thrombosis (coronary
or pulmonary)Trauma
(hypovolemia,increased ICP)

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 101/202
Transcutaneous Pacing

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 102/202
Pacing Control

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 103/202
Pacing Control
Method

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 104/202
Method
1. Attach electrode.
2. Turn on pacemaker at desire rate.
3. In bradyasystolic arrest, set initial output tomaximum; once capture has been confirmed,↓output until threshold determined.
4. In conscious patient, start with minimumoutput and↑ until threshold is achieved.
5. Set output at 10-20% above capture
threshold.6. Give sedative & analgesia as needed.
Capture

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 105/202
Capture Definition:Cardiac depolarization and
resultant contraction caused by
pacemaker stimulus

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 106/202
Acute coronary syndrome

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 107/202
References
Guideline UA/NSTEMI ACC/AHA
2007
Guideline STEMI ACC/AHA 2007 ,
2009
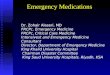
Pathophysiology of ACSL

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 108/202
Fuster V et al NEJM 1992;326:310 – 318
Davies MJ et al Circulat ion 1990;82(Suppl II):II –
38, II –
46
Lipid pool
Macrophages
Stress, tensile,internal
Shear forces,external Fissure
Largefissure
Smallfissure
Mural thrombus(unstable angina/NSTEMI)
Occlusive thrombus(STEMI)
Atheroscleroticplaque
Plaquedisruption
Thrombus
Example of atherosclerosis
disease progression
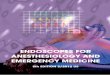
Spectrum of Acute Coronary

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 109/202
Spectrum of Acute Coronary
Syndrome
Q-wave MIUnstable Angina
Ischemic Discomfort at Rest
No ST Elevation ST Elevation
Non ST Elevation MI
Braunwald E et al . J Am Coll Cardiol 2000;36:970 – 1062.
≥0.2 mV in V1-3
≥0.1 mV in other lea
>2 contiguous leads
Di i

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 110/202
Diagnosis
Clinical presentation
ECG finding
Cardiac Biomarker
Clinical presentation

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 111/202
AnginaRetrosternal chest pain, burning, heaviness
Radiating to neck,jaw,epigastrium,shoulder ,Lt arm
Precipitated by exercise,cold weather,emotional stress
Duration < 2-10 min
Rest or unstable anginaSame as angina , more severe
Typical <20 min
Acute myocardial infarctionSame as angina , more severe
Sudden onset, often with shortness of breathing,weakness, nausea , vomitting
Usually lasting 30 min or longer
PericarditisSharp, pleuritic pain
Aggravated by changes in positions, variable in duration, pericardial friction rub
Braunwald’ s Heart disease ,textbook of cardiovascular medicine eight edition
ED Evaluation of
Patients With STEMI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 112/202
Patients With STEMI
Aortic dissection
Pulmonary embolus
Perforating ulcer
Tension pneumothorax
Boerhaave syndrome
(esophageal rupture with
mediastinitis)
Differential Diagnosis of STEMI: Life-Threatening
ED Evaluation of
Patients With STEMI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 113/202
Gastroesophageal reflux
(GERD) and spasm
Chest-wall pain
PleurisyPeptic ulcer disease
Panic attack
Cervical disc or neuropathic
pain
Biliary or pancreatic pain
Somatization andpsychogenic pain disorder
Patients With STEMI
Differential Diagnosis of STEMI: Other Noncardiac
ECG fi di

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 114/202
ECG finding
ST Elevation
> 0.2 mV in leads V1-3
> 0.1 mV in other leads
Elevation in at least 2 contiguous leads

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 115/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 116/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 117/202
Comparison of EKG Changes Associated with Acute Pericarditis,

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 118/202
Myocardial Infarction and Early Repolarization
ECG Finding
Acute
Pericarditis
Myocardial
Infarction
Early
Repolarization
ST-segment shape Concave upward Convex upward Concave upward
Q waves Absent Present Absent
Reciprocal ST-
segment changes
Absent Present Absent
Location of ST-
segment elevation
Limb and precordial
leads
Area of involved
artery
Precordial leads
ST/T ratio in lead V6 >0.25 N/ A <0.25
Loss of R-wave
voltage
Absent Present Absent
PR-segment
depression
Present Absent Absent
Marriott Practical Electrcaediography 10th
edition
Early repolarization

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 119/202
y p

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 120/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 121/202
LVH LBBB pericarditisHyper K
ASMI Brugada

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 122/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 123/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 124/202
Acute Inferior wall MI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 125/202
Acute Anterior wall MI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 126/202
Wall ST elevation

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 127/202
Wall
Septal
Anterior
Anteroseptal
Extensive anterior
LateralHigh lateral
Anterolateral
Inferior
RV infarctposterior
ST elevation
V1-V2
V3-V4
V1-V4
V1-V6
V6, I, AVLI, AVL
V3-V6, AVL
II, III, AVF
V3R-V4RTall R in V1
Corelation of Wall and coronary vessel

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 128/202
Progression of Nonreperfused Q-
AMI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 129/202
wave AMI
Biochemical Cardiac Markers

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 130/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 131/202
ESC/ACCF/AHA/WHF Expert Consensus Document,
JACC Vol. 50, No. 22, 2007 :2173 –95
Management

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 132/202
g
Generalmanagement
Oxygenation
AnalgesiaNTG
Blood sugar control
Specificmanagement
Reperfusion
Antiplatelets Anticoagulant
Betablocker
ACEI/ARB Aldosterone blockade
Statin
Analgesia

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 133/202
Morphine remains Class I for STEMIalthough may increase adverse events in
UA/NSTEMI
NSAID medications increase mortality,reinfarction, and heart failure in proportion
to degree of COX-2 selectivity
– Discontinue on admission for STEMI– Do not initiate during acute phase of
management
ACC/AHA guideline for STEMI 2007
Oxygen

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 134/202
Supplemental oxygen should be administered topatients with arterial oxygen desaturation (SaO2
< 90%).
It is reasonable to administer supplemental
oxygen to all patients with uncomplicated STEMI
during the first 6 hours.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
ACC/AHA guideline for STEMI 2007
Nitroglycerin

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 135/202
Patients with ongoing ischemic discomfort should
receive sublingual NTG (0.4 mg) every 5 minutes for atotal of 3 doses, after which an assessment should be
made about the need for intravenous NTG.
Intravenous NTG is indicated for relief of ongoing
ischemic discomfort that responds to nitrate therapy,
control of hypertension, or management of pulmonary
congestion.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
ACC/AHA guideline for STEMI 2007
Nitroglycerin Contraindications

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 136/202
Nitrates should not be administered when:
Nitrates should not be administered to
patients who have received aphosphodiesterase inhibitor for erectile
dysfunction within the last 24 hours (48
hours for tadalafil).
• systolic pressure < 90 mm Hg or ≥ to 30 mm Hg
below baseline
• severe bradycardia (< 50 bpm)
• tachycardia (> 100 bpm) or • suspected RV infarction.

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 137/202
Specific management
Reperfusion Options for STEMIPatients
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 138/202
Reperfusion Options for STEMI PatientsSelect Reperfusion Treatment.

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 139/202
Fibrinolysis generally preferred
Early presentation ( ≤ 3 hours from symptom
onset and delay to invasive strategy)
Invasive strategy not an option
Cath lab occupied or not available Vascular access difficulties
No access to skilled PCI lab
Delay to invasive strategy
Prolonged transport Door-to-balloon more than 90 minutes
> 1 hour vs fibrinolysis (fibrin-specific agent) now
If presentation is < 3 hours and there is no delay to an invasive
strategy, there is no preference for either strategy.
ACC/AHA guideline for STEMI 2007
Reperfusion Options for STEMI PatientsSelect Reperfusion Treatment.

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 140/202
Invasive strategy generally preferred
Skilled PCI lab available with surgical backup
Door-to-balloon < 90 minutes
• High Risk from STEMI
Cardiogenic shock, Killip class ≥ 3
Contraindications to fibrinolysis, including
increased risk of bleeding and ICH
Late presentation > 3 hours from symptom onset
Diagnosis of STEMI is in doubt
If presentation is < 3 hours and there is no delay to an invasive strategy,
there is no preference for either strategy.
ACC/AHA guideline for STEMI 2007
Primary PCI
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 141/202
STEMI patients presenting to a hospital with PCIcapability should be treated with primary PCI within
90 min of first medical contact as a systems goal.
STEMI patients presenting to a hospital without PCI
capability, and who cannot be transferred to a PCI
center and undergo PCI within 90 min of first
medical contact, should be treated with fibrinolytic
therapy within 30 min of hospital presentation as asystems goal, unless fibrinolytic therapy is
contraindicated.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
ACC/AHA guideline for STEMI 2007
Application of PCI for STEMI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 142/202
STEMI
Thrombolysis Primary PCI
Success Failure
Rescue PCI Routine
immediateor urgent PCI
RoutineDeferred CAG+ PCI
Selective CAG
+ PCI only for High-risk pts
Curr Prob l Cardiol, January 2003
Facilitated PCI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 143/202
Rescue and Late PCI
Assessment of Reperfusion
It is reasonable to monitor the pattern of ST elevationIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 144/202
It is reasonable to monitor the pattern of ST elevation,
cardiac rhythm and clinical symptoms over the 60 to 180
minutes after initiation of fibrinolytic therapy.
Noninvasive findings suggestive of reperfusion include:
Relief of symptoms
Maintenance and restoration of hemodynamic and/or
electrical instability
Reduction of ≥ 50% of the initial ST-segment elevation
pattern on follow-up ECG 60 to 90 minutes after
initiation of therapy.
ACC/AHA guideline 2007
Rescue PCI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 145/202
PCI in no reperfusion after fibrinolytic therapy
Failed reperfusion
ongoing chest pain
resolution of ST elevation < 50 %
Early peak of cardiac enzyme
Benefit ( Meta-analysis in 2007)
Mortality rate 10.4% to 7.3 % ( RR 0.69, 95% CI 0.46-1.05 ; p=0.09)
Reinfarction 10.7% to 6.1 % ( RR 0.58, 95% CI 0.35-0.97 ; p=0.04)
Heart failure 17.8% to 12.7 % ( RR0.73,95% CI 0.54-1.00 ; p=0.05)
Thrombolytic Therapy

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 146/202
y y
Indications ?
Contraindications ?Which drug ?
How fast to be given ?
Conjunctive antithrombotics ?
ST segment elevation
> 0 2 mV in leads V1-3

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 147/202
Indicationfor
fribinolysis
TherapyIn STEMI
> 0.2 mV in leads V1 3
> 0.1 mV in other leads
Elevation in at least 2 continuous leadsor new LBBB
Duration < 12 hr (class I)
12-24 hr with ongoing pain ( class IIa)
No contraindications
TIMI Risk Score for STEMI Risk Score Odds of death by 30D*
Mortality prediction of STEMI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 148/202
Age65-74 75
DM/HTN or angina
Weight < 67 kg
Time to rx > 4 hrs
Anterior STE or LBBB
HR >100
SBP < 100
Historical
Exam
Presentation
Killip II-IV
2 points3 points
1 point
3 points
2 points
1 point
1 point
1 point
2 points
Risk Score = Total (0 -14)
0
12
3
4
56
7
8
>8
0.1 (0.1-0.2)
0.3 (0.2-0.3)
0.4 (0.3-0.5)
0.7 (0.6-0.9)
1.2 (1.0-1.5)
2.2 (1.9-2.6)
3.0 (2.5-3.6)
4.8 (3.8-6.1)
5.8 (4.2-7.8)
8.8 (6.3-12)
*referenced to average mortality
(95% confidence intervals)

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 149/202
Thrombolytic Therapy

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 150/202
Indications ?
Contraindications ?Which drug ?
How fast to be given ?
Conjunctive antithrombotics ?
Absolute Contraindications for
Thrombolytic Rx

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 151/202
y
Any prior ICHKnown structural cerebral vascular lesion
Malignant intracranial neoplasm
Ischemic stroke within 3 monthsSuspected aortic dissection
Active bleeding diathesis (excluding menses)
Significant closed-head or facial traumawithin 3 months
Relative Contraindications for
Thrombolytic Rx

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 152/202
Chronic severe poorly controlled HTN
Severe uncontrolled HTN on presentation SBP>180,DBP>110
Prior ischemic stroke > 3 months, intracranialpathology
Traumatic or prolonged >10 min CPR or major surgerywithin 3 weeks
Recent within 2-4 weeks internal bleeding
Noncompressible vascular puncture
SK, anistreplase: prior exposure > 5 days ago or prior
allergic reactionPregnancy
Active peptic ulcer
Current use of anticoagulation
Risks for ICH After Thrombolysis

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 153/202
Age > 65
Weight < 70 kg
FemaleHypertension
Use of tPA
Thrombolytic Therapy

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 154/202
Indications ?
Contraindications ?Which drug ?
How fast to be given ?
Conjunctive antithrombotics ?
Thrombolytic Agents

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 155/202
First generation Second generation Third generation
Streptokinase* APSAC Reteplase* (r-PA)
Urokinase Alteplase* Lanoteplase* (n-PA)
Staphylokinase Saruplase TNK-PA
Staphylokinase
Thrombolytic Agents in
Clinical Practice

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 156/202
• SK 1.5 mu IV > 1 hr
• Accelerated tPA 15 mg IV bolus
50 mg (0.75 mg/kg) IV in 30 min
35 mg (0.5 mg/kg) IV in 60 min
Clinical Practice
Comparison

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 157/202
Streptokinase Alteplase Reteplase Tenecteplase
•Dose 1.5 MU over Up to 100mg in 10U x 2 30-50mg
30-60 min 90 min (wt-based) each over 2 min based on weight
•Bolus Admin. No No Yes Yes
•Antigenic Yes No No No
•Allergic React Yes No No No
•Systemic Marked Mild Moderate Minimal
Fibrinogen Depletion
• ~90-min patency 50 75 75? 75
rates (%)•TIMI grade 3 flow, % 32 54 60 63
Antiplatelets

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 158/202
Aspirin
Thienopyridines
Glycoprotein IIb/IIIa receptor antagonist
Aspirin

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 159/202
Reduce mortality
Reduce coronary reocclusion
Reduce recurrent ischemic events
Aspirin

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 160/202
Aspirin should be chewed by patients who
have not taken aspirin before presentation
with STEMI. The initial dose should be
162 mg to 325 mg
Although some trials have used enteric-coated aspirin for initial dosing, more rapid buccal absorption occurs with
non –enteric-coated formulations.
ACC/AHA guideline for STEMI 2007
Complementary Mode of Action between
Clopidogrel and ASA

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 161/202
p g
COX, cyclooxygenase; ADP, adenosine diphosphate; TxA2,
thromboxane A2
Schafer AI Am J Med 1996;101:199 209
Clopidogrel is an advanced ADP receptor antagonist and
inhibits platelet aggregation by antagonizing the effects of ADP
ST-Elevation MI: ClopidogrelTrials

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 162/202
COMMIT / CCS-2
46,000 patients
Mortality, D / MI / CVA
AMI < 24 hrs
Age up to 100
~ 50% lytic
No loading dose China
Non-invasive strategy
3,500 Patients
Infarct artery patency
AMI < 12 hrs
Age < 75
100% fibrinolytic
Loading dose Europe / N. America
Invasive strategy
Thie
nopyridines

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 163/202
Clopidogrel 75 mg per day orally should be added toaspirin in patients with STEMI regardless of whether
they undergo reperfusion with fibrinolytic therapy or
do not receive reperfusion therapy.
Treatment with clopidogrel should continue
for at least 14 days.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
ACC/AHA guideline for STEMI 2007
Thie
nopyridines
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 164/202
In patients < 75 years who receive fibrinolytic
therapy or who do not receive reperfusion therapy, it
is reasonable to administer an oral clopidogrel
loading dose of 300 mg. (No data are available to
guide decision making regarding an oral loading
dose in patients ≥ 75 years of age.)
Long-term maintenance therapy (e.g., 1 year) with
clopidogrel (75 mg per day orally) can be useful in
STEMI patients regardless of whether they undergo
reperfusion with fibrinolytic therapy or do not
receive reperfusion therapy.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I IIa Ia Ia IIb Ib Ib III II II IIa Ia Ia IIb Ib Ib III II II IIa Ia Ia IIb Ib Ib III II II Ia Ia Ia IIb Ib Ib III II II
ACC/AHA guideline for STEMI 2007

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 165/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 166/202
ACC/AHA guideline for STEMI 2009

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 167/202
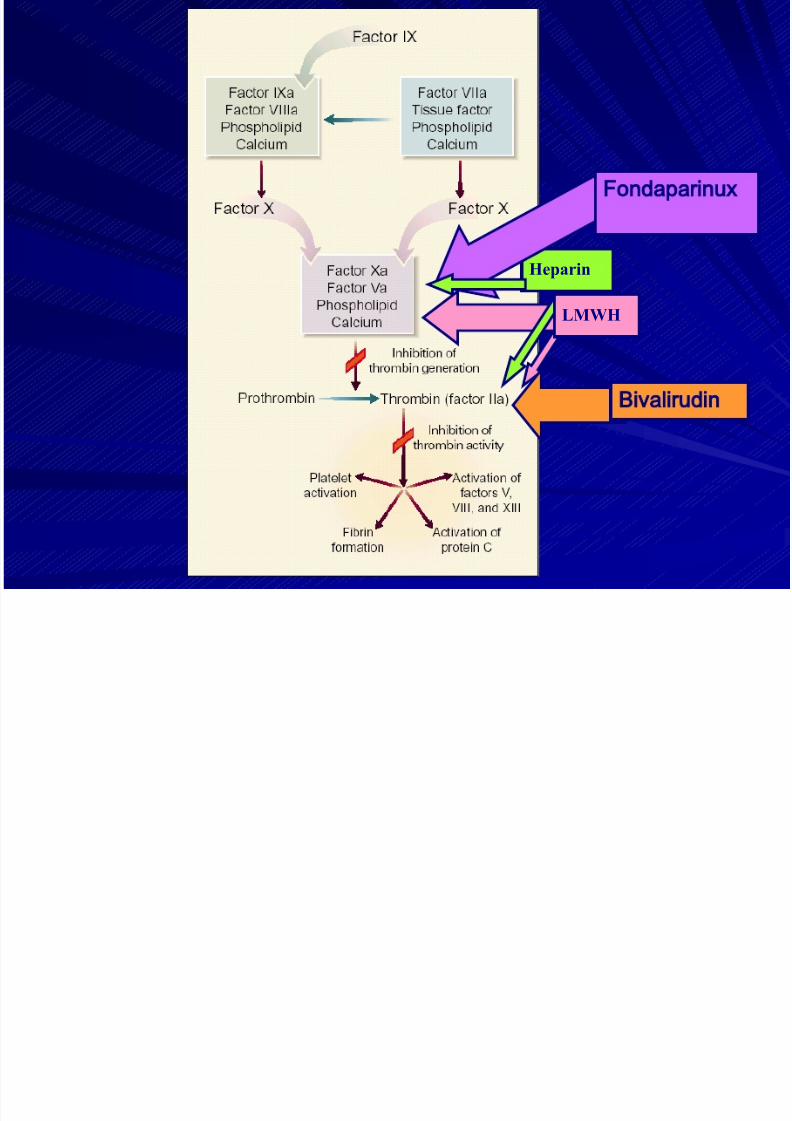
Anticoagulant

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 168/202
Anticoagulant
Reduce reocclusion
Reduce reinfarction
Reduce recurrent ischemia
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 169/202
Heparin
LMWH
Fondaparinux
Bivalirudin
Anticoagulants

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 170/202
Patients undergoing reperfusion with fibrinolytics
should receive anticoagulant therapy for a minimum of
48 hours (Level of Evidence: C) and preferably for the
duration of the index hospitalization, up to 8 days
(regimens other than unfractionated heparin [UFH] are
recommended if anticoagulant therapy is given for morethan 48 hours because of the risk of heparin-induced
thrombocytopenia with prolonged UFH treatment).
(Level of Evidence: A)
Anticoagulant regimens with established efficacyinclude:
♥ UFH (LOE: C)
♥ Enoxaparin (LOE:A)
♥ Fondaparinux (LOE:B)
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
ACC/AHA guideline STEMI 2007

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 171/202
ACC/AHA guideline STEMI 2007

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 172/202
Beta-Blockers
Beta-Blockers

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 173/202
Reduce reinfarct size
Reduce reinfarction
Reduce life threatening ventricular tachyarrhythmias
Beta-Blockers

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 174/202
Oral beta-blocker therapy should be initiated in the first 24
hours for patients who do not have any of the following: 1)signs of heart failure, 2) evidence of a low output state, 3)
increased risk* for cardiogenic shock, or 4) other relative
contraindications to beta blockade (PR interval > 0.24 sec,
2nd- or 3rd-degree heart block, active asthma, or reactive
airway disease).
It is reasonable to administer an IV beta blocker at the time of
presentation to STEMI patients who are hypertensive and who
do not have any of the following: 1) signs of heart failure, 2)
evidence of a low output state, 3) increased risk* for
cardiogenic shock, or 4) other relative contraindications to
beta blockade (PR interval > 0.24 sec, 2nd- or 3rd-degree heart
block, active asthma, or reactive airway disease).
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
ACC/AHA guideline STEMI 2007

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 175/202
Inhibition of the Renin-Angiotensin Aldosterone
System
Inhibition of the Renin-Angiotensin-Aldosterone System

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 176/202
Aldosterone System
ACEI/ARB
Reduce mortality
Aldosterone
blockadeReduce mortality
Reducehospitalization
ACE/ARB: Within 24 Hours
An ACE inhibitor should be administered orally
ithi th fi t 24 h f STEMI t th f ll i
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 177/202
within the first 24 hours of STEMI to the following
patients without hypotension or known class of contraindications:
• Anterior infarction
Pulmonary congestion
LVEF < 0.40
An ARB should be given to ACE-intolerant patients
with either clinical or radiological signs of HF or LVEF< 0.40.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
ACC/AHA guideline STEMI 2007

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 178/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 179/202
Roles of statins in ACS

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 180/202
Improve endothelial function
Repair ruptured atherosclerotic plaques
Improve plaque stabilization
Reduce thrombus formation on ruptureplaques
Cardiol Rev1999;16(Suppl.):1-6.
Prefer high dose atrovastation 80 mg/day
(MIRACL, PROVE-IT)
ST elevation
ASA clopidogrel Beta blocker statin

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 181/202
ASA, clopidogrel,Beta-blocker,statin
< 12 hours
Thrombolytic Rx
contraindicated
SK Cardiac cath with
primary PTCA
Not candidate for
reperfusion Rx
Medical Rx: ACEI, Nitrates
> 12 hours
No Yes
Consider
reperfusion Rx
Persistent
symptoms
If failed SK,
rescue (salvage)
PTCA
Eligible for
thrombolytic Rx
D to N time <30 minD to balloon time 90+30 min

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 182/202
1st
24 h
During Hosp Hosp DC +
Long Term
Summary of Pharmacologic Rx: LVD, Sec. Pre

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 183/202
24 h Long Term
ACEI Anterior MI,Pulm Cong., EF < 40 Oral
Daily
OralDaily
IndefinitelyARB ACEI intol.,
HF, EF < 40
Aldo
Blocker
No renal dysf,
K+ < 5.0 mEq/L
On ACEI,
HF or DM
Same as
during
Hosp.
Statin Oral daily Oral daily Indefinitely,LDL <70-100
JACC 2004;44:671 , Circ 2004;110:588

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 184/202

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 185/202
Fast Track MI

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 186/202
การด แลผ ป วยโรคกลามเนอหัวใจตายเฉยบพลัน โรงพยาบาลสม ทรปราการ
checklist ตามแบบคัดกรองอาการเจบหนาอก
ผปวยเจบหนาอก

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 187/202
แนวทางการด แลผ ป วย
แพทยซักประวัตตรวจรางกาย ตรวจคล นไฟฟ าหัวใจ และ Non invasive procedure เพ อทาการวนจฉัยและวนจฉัยแยกโรค

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 188/202
ภาวะหัวใจขาดเลอดเฉยบพลัน โรคหัวใจขาดเลอดเร อรัง
เหมาะสมก ับการให SK หรอไม
ST Elevation Non ST elevation
ใหยาละลายล มเลอด (SK)
เปดหลอดเลอดดวย SK ไดหรอไม
ICU / CCU
มภาวะแทรกซอนหรอไม
ตดตามและรักษาอย างต อเน อง
สงตอเพ อทา Invasive procedure
เหมาะสม
ได
ไมม
ไมเหมาะสม
ไมได
ม
แบบคั ดกรองผ ปวยกลามเน อหัวใจตายเฉยบพ ลัน ช อ – สกล ............................................................................................................
HN. ………………………………….
วันท …………………………………. เวลา ………………………………….
เพ ………………………………….
รคประจาตัว

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 189/202
รคประจ าตว ……………………………………………………………………………………
การแพยา ……………………………………………………………………………………
อาการ ขะซักประวัต 1. มอาการเจบหนาอกอย
2. ไมมอาการเจบหนาอกแลว
ลักษะการเจ บหนาอก 3. เจบแนนเหมอนถกทับกลางหนาอก
4. เจบราวไปทองแขนขางซาย, ราวข นกราม
5. เจบนานกวา 20 นาท 6. อาการเจบมากข นเม อออกแรง
7. เจบขะพัก
อาการรวม 8. เปนลมหมดสต 9. เหน อยหอบนอนราบไมได 10. อดอัดหายใจไมออก
11. เหง อแตก
12. ใจส ัน
13. คล นไสอาเจยน
ตรวจรางกายเบ องตน 14. Vital Sign BP_________mmHg, P_________ คร ัง/นาท, R_________ คร ัง
15. ซด
16. กระสับกระสาย
สงตอผ ปวยไปยัง ER [ถาเขาเก 1, 3 – 5, 8 – 10, 15 – 16 และตรวจรางการเบ องตน
SBP≥ 180, SBP < 100, P ≥ 100, P≤ 40, R ≥ 24, R ≤ 6]
หองทา ECG
พบแพทยอายรกรรม พบแพทย GP
แบบคัดกรองอาการเจบหนาอก
checklist ตามแบบคัดกรองอาการเจบหนาอก
ผปวยเจบหนาอก
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 190/202
ER
Activate fast track MI
แนวทางการดแลผ ปวย Acute STEMI (Fast Track )
ผ ปวยมาดวยอาการเจบหนาอก
*Onset เวลา .............../....................(พยาบาลER )
เวลาท มาถงหองฉกเฉน .............../....................(พยาบาล ER )
ECG 12 Lead เวลา.............../....................(พยาบาล ER )
ช อ............................สกล...................
HN………………………………….
วันท ...................................................

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 191/202
ประวัต / ตรวจรางกาย / แปลผล ECG โดยแพทยประจาหองฉกเฉน
เวลา.............../....................(แพทยประจาหองฉกเฉน)
ASA gr V 1 เมดเค ยวทันท เวลา .............../....................(พยาบาลER )
Clopidogrel 4 เมด ทันท (งด ถาอาย > 75 ป) เวลา.............../....................(พยาบาลER )
Troponin T เวลา.............../....................(พยาบาลER )
ปรกษาแพทยอายรกรรมมาด เวลา.............../....................(แพทยอายรกรรม) วนจฉัย...............................................
Admit เวลา.............../....................(แพทยอายรกรรม)
ออกจากหองฉกเฉน เวลา.............../....................(พยาบาลER )
เขาหอผ ปวย.......................................... เวลา.............../....................(พยาบาลWard)
รายงานแพทยประจา Ward เวลา.............../....................(พยาบาลWard)
แพทยประจา Ward ประเมนผ ปวยเวลา.........../..........(แพทย Ward) วนจฉัย...........................Killip……………..
*เร ม Streptokinase เวลา.............../....................(พยาบาลWard)
ประเมนผ ปวย (Symptom , ECG) หลังได Streptokinase 90 นาท เวลา.............../....................(พยาบาลWard)
ภาวะแทรกซอน (Major bleeding) ( ) ไมม ( ) ม ........................................................................
จาหนายจากหอผ ปวย ................................................................................
ถานการจาหนาย ( ) ทเลา ( ) เสยชวต
( ) ปเสธการรักษา ( ) สงตอไปท .............................................
Door to Needle time ……………hr ……………..min
าเหตท ไดรับการรักษาลาชา..................................................................................................................................................
................................................................................................................................................................................................
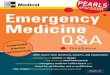
Fast track MI
checklist ตามแบบคัดกรองอาการเจบหนาอก
ผปวยเจบหนาอก

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 192/202
ER หองทาECG
Activate fast track MI
Admit
ผล ECGเขาไดก ับ STEMI
ดแลรักษาตาม Caremap
standing order
เก บขอมลตามตัวช วดั
yes no
ส ง ER เขา fast track MI
Admit ward เขา fast track MI
พบอายรแพทยถามECGผดปกต
พบแพทยท ัวไปถาECG ปกต
D/C
แผนการรักษา Acute ST Elevation MI
Fast Track

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 193/202
หนังสอยนยอม / ไมยนยอม การใหยาละลายล มเลอด
(Streptokinase)

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 194/202
( p )
แนวทางการด แลผ ป วย
แพทยซักประวัตตรวจรางกาย ตรวจคล นไฟฟ าหัวใจ และ Non invasive procedure เพ อทาการวนจฉัยและวนจฉัยแยกโรค

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 195/202
ภาวะหัวใจขาดเลอดเฉยบพลัน โรคหัวใจขาดเลอดเร อรัง
เหมาะสมก ับการให SK หรอไม
ST Elevation Non ST elevation
ใหยาละลายล มเลอด (SK)
เปดหลอดเลอดดวย SK ไดหรอไม
ICU / CCU
มภาวะแทรกซอนหรอไม
ตดตามและรักษาอย างต อเน อง
สงตอเพ อทา Invasive procedure
เหมาะสม
ได
ไมม
ไมเหมาะสม
ไมได
ม
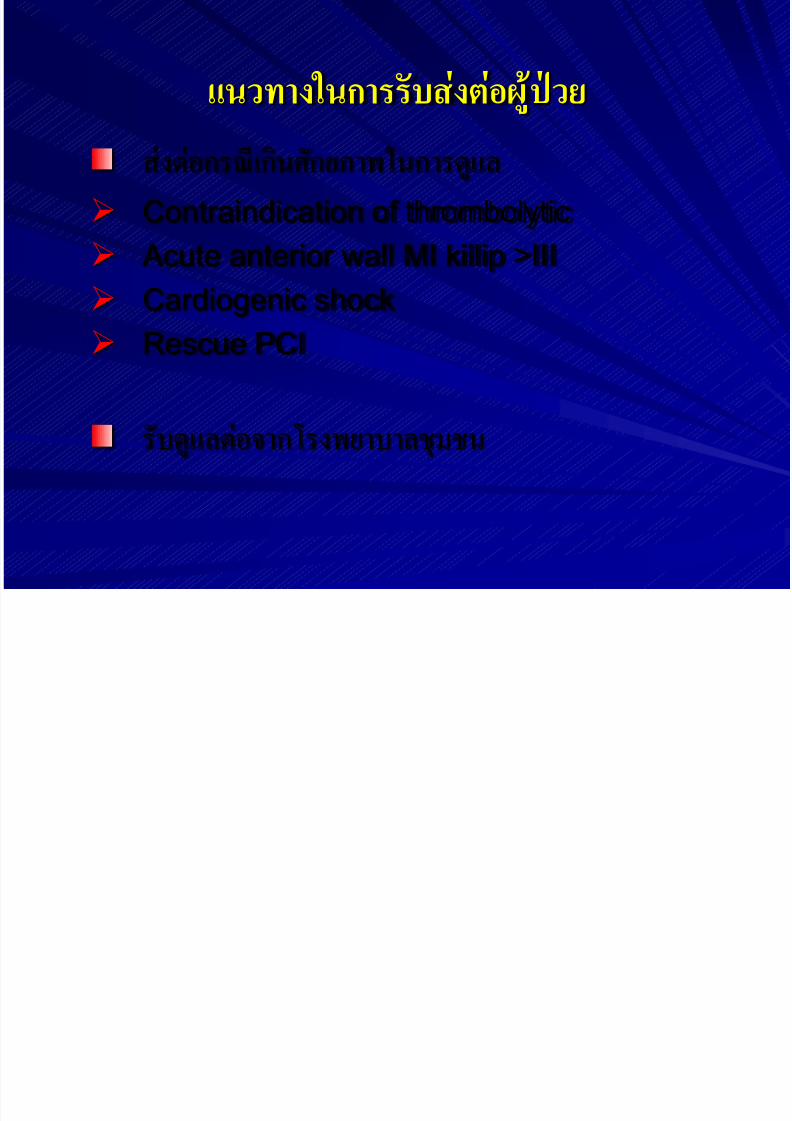
แนวทางในการรับสงตอผ ป วย
7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 196/202
ส งต อกรเก นศกัยภาพในการดแล Contraindication of thrombolytic
Acute anterior wall MI killip >III
Cardiogenic shock Rescue PCI
รับดแลต อจากโรงพยาบาลชมชน
แนวทางการสงตอผ ป วย

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 197/202
แบบฟอรมการสงตอผ ป วยโรคกลามเนอหัวใจตายเฉยบพลันชนด
STEMI ไปโรงพยาบาลชลบ ร

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 198/202
แบบฟอรมการสงตอผ ป วยโรคกลามเนอหัวใจตายเฉยบพลันชนด
STEMI ในจังหวัดสม ทรปราการ

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 199/202
ตัวชวัด

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 200/202
1. รอยละของผ ป วย Acute STEMI ไดรับยาละลายล มเลอดภายใน 30นาท
2. รอยละการเสยชวตของผ ป วย Acute STEMI
3. รอยละการรอดชวตของผ ป วย Acute STEMI แบงตาม killip
classification
4. รอยละการเกด Major bleeding จากการไดรับยาละลายล มเลอด
ตัวชวัดเสรม

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 201/202
1. ระยะเวลาเฉล ยผ ป วย Acute STEMI ท ไดรับยาละลายล มเลอดตั งแตมาถงโรงพยาบาลจนถงไดรับยา
2. รอยละของผ ป วย Acute STEMI ไดรับยาละลายล มเลอดภายใน 30
นาทเฉพาะในเวลาราชการ
3. Door to EKG time ภายใน 10 นาท
4. Door to Diagnosis time ภายใน 20 นาท

7/22/2019 Emergency in Medicine 2012
http://slidepdf.com/reader/full/emergency-in-medicine-2012 202/202