Embed Size (px)
Citation preview

Emergency Department Status BoardsA Case Study in Information Systems Transition
Ann M BisantzPriyadarshini R PennathurUniversity at BuffaloTheresa K GuarreraRollin J FairbanksUniversity of RochesterShawna J PerryVirginia Commonwealth UniversityFrank ZwemerMcGuire VA Medical CenterRobert L WearsUniversity of Florida
ABSTRACT Patient status boards play an important role in coordinating and communi-
cating about patient care in hospital emergency departments (EDs) Status boards are
transitioning from dry-erase whiteboards to electronic systems Although electronic
systems may preserve some surface features of the manual artifacts important affor-
dances of the manual technology are not always maintained We compared informa-
tion on manual and electronic status boards in an ED Photographs of the manual
board and screen shots of the electronic system were obtained before and after a hos-
pital transitioned between systems Displayed information as well as detailed content
regarding patient chief complaints clinical plans and dispositions were coded and
analyzed to understand the type and function of information present as well as the use
of features such color Results indicated that although categories of information found
were similar the frequency with which some types of information appeared on the two
system displays was substantially different In particular information used to coordi-
nate aspects of patient treatment was more frequently found in the manual system
Results suggest that in the design of new information technologies simply matching
the format or information fields available on an existing system may not be sufficient to
sustain current work practices or to prevent unanticipated shifts in use
Introduction
AS WITH MANY COMPONENTS OF THE HEALTH CARE SYSTEM HOSPITAL EMERGENCY DEPART-ments (EDs) are transitioning to computerized information technologies An impor-tant technological change involves the replacement of manual patient status boardswith electronic patient-tracking systems The successful design of these new systems
ADDRESS CORRESPONDENCE TO Ann Bisantz Department of Industrial and Systems Engineering 438
Bell Hall University at Buffalo State University of New York Amherst NY 14260 bisantzbuffaloedu
Journal of Cognitive Engineering and Decision Making Volume 4 Number 1 Spring 2010 pp 39ndash68
DOI 101518155534310X495582 copy 2010 Human Factors and Ergonomics Society All rights reserved 39
requires a careful understanding of the functions afforded by the old systems andthe manner in which the manual systems supported clinical work
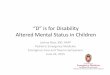
Manual status boards are typically large dry-erase boards that display informa-tion such as patient demographics (eg name age gender) location (eg roombed) caregiver assignments clinical presentation data (eg symptoms diagnoses)and workup plan (eg planned and completed tests and treatments) Informationis typically represented in rows (corresponding to beds to which patients areassigned) and columns (corresponding to a category of information) often usingsymbols and color (see Figure 1) Manual status boards are located in central areasof the ED and are accessible to and used by a variety of caregivers and staff to com-municate information and coordinate individual and group activities
From the standpoint of distributed cognition (Hutchins 1997) status boards serveas a critical cognitive artifact storing and communicating information across time andindividuals in the ED (Nemeth OrsquoConnor Nunnally amp Cook 2007 Pennathuret al 2007 Wears amp Perry 2007 Xiao 2005) For example physicians may use thestatus board to track their own activities in treating and documenting the care of apatient whereas nurses may use them to indicate needs for testing or transportationto other ED staff Status boards support the maintenance of shared situation aware-ness across ED staff and preserve critical information across shift changes (Wears ampPerry 2007) In general these boards support an ED process whereby patients areinitially screened for condition severity when they come to the ED (the triageprocess) are examined by one or more physicians physicians-in-training and med-ical students receive tests and treatments appropriate to their conditions and eitherare admitted to stay in the hospital or leave for home (discharged)
Manual status boards were developed from the ground up over the past three tofour decades by ED practitioners to meet their immediate needs (Wears amp Perry2007) Similar to paper artifacts that co-evolve with an organizationrsquos work practices(Sellen amp Harper 2003) ED status boards developed based on usersrsquo needs andfunctions that the whiteboard medium can support They evolved from a simple listof patients and locations to a rich source of clinical and workflow informationAlthough the basic row-column format is similar across locations the particular for-mat of information representation on status boards is unique and customized to theneeds of caregivers in each hospital setting the boards dynamically represent thestate of the ED in densely encoded idiosyncratic but locally meaningful ways
Interaction with the manual status boards is direct fast and flexible Staff canread portions of the board in detail or get an overview of the level of demand byassessing the overall information density Staff are visible when they gather aroundand mark the whiteboard making it possible for others to notice and infer theiractivities (which may be difficult or impossible to tell when interacting with indi-vidual workstations) Information is primarily entered using markers and includesalphanumeric input as well as hand-drawn symbols and annotations
The status boards are malleable in the sense that they are flexible enough toadapt and support a variety of functions For example in some EDs staff use spe-cially designed prelabeled magnets to provide alerts and may use magnets or tape
40 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 41
Figu
re 1
Man
ual s
tatu
s bo
ard
phot
ogra
ph (n
ames
obs
cure
d) R
epri
nted
from
Pen
nath
ur e
t al
Pro
ceed
ings
of t
he H
uman
Fac
tors
and
Erg
onom
ics
Soci
ety
Ann
ual M
eeti
ng2
007
to attach paper forms or test results to the whiteboard (Wears Perry WilsonGalliers amp Fone 2007) Inputs are not restricted to the matrix format but caninclude annotations around the edges of the board or notations that continueacross multiple cells in a row or column Manual whiteboards thus share many ofthe affordances of other manual (paper-based) systems as described by Sellen andHarper (2003) including easy direct marking allowing flexible and ldquotailorablerdquomarkings based on the circumstances providing ldquoinformation at a glancerdquo that issimultaneously available to multiple ED staff and allowing activity to be implicitlycommunicated and coordinated because team members can observe one anotherrsquosactions or the trace of those actions on the status board
Manual to Electronic Status Board TransitionElectronic patient-tracking systems are being implemented as part of an overall
movement to computerize health care information that is driven by anticipatedimprovements in care coordination patient safety and efficiency (Aspden CorriganWolcott amp Erickson 2004 Committee on Quality of Health Care in America 2001Kohn Corrigan amp Donaldson 1999) Generally speaking these boards have beendeveloped by third-party vendors and usually have visual display layouts similarin nature to the whiteboards they have replaced Researchers have noted advan-tages in having a customized electronic tool to support multitasking in ED environ-ments (Laxmisan Hakimzada Sayan Green amp Patel 2007) Electronic systemsmay also address shortcomings of manual status boards Once erased informationcannot be recovered and information entered into one system (eg at hospitalregistration) cannot automatically populate the manual status board Thus repeateddata entry tasks may be required and information may be incomplete outdated orinconsistent across systems Electronic systems are often components of or linked toother hospital information systems and have the ability to log information inputs
Unlike the bottom-up evolutionary design of manual whiteboards the elec-tronic systems are typically purchased from third-party vendors often with onlymodest abilities for customization to reflect the individual uses in each hospital(but see Aronsky Jones Lanaghan amp Slovis 2008 for an example of a ldquohome-grownrdquo electronic system) Procurement is often led by organizational informationtechnology (IT) staff rather than clinicians and can be driven by overall organiza-tional needs and management goals such as system interoperability cost abilityto collect quality and efficiency measures integration with hospital bed manage-ment systems and data storage (Poon et al 2006) These needs may overshadowthose of the clinicians who have been using the manual whiteboard to supporttheir minute-by-minute work
For a variety of economic quality and policy reasons health care providerswill continue to transition to electronic systems Research in a number of settingshas indicated that when systems are designed based on an incorrect or rational-ized model of work performance suffers (Berg 1997 2004 Bisantz amp Ockerman2002 Button amp Harper 1993 Mackay 1999 Sachs 1995) New technology oftencreates a necessity for users to reorient themselves to the electronic system and
42 Journal of Cognitive Engineering and Decision Making Spring 2010
change their existing work practices by altering their tasks and configuring thenew systems In some cases the new technology may increase workload or lead toerrors if users are forced to adapt either the system or their tasks and strategiesduring critical periods (Cook amp Woods 1996) For new technologies to success-fully support or augment evolved work practices designers must start with a deepunderstanding of what functions the manual technologies support
Research ObjectivesIn observing a transition from manual to electronic status boards in two hospi-
tal emergency departments we found that providers reported a negative impact ofthe transition on communication and their ability to make sense of the overallstate of the ED (Pennathur et al 2007) This paper investigates the two technolo-gies in detail to try to identify design-oriented reasons for these difficulties Itcould be simply that the new system does not provide access to record or view thesame type or amount of information as the manual system Alternatively problemscould stem from the format of presentation or method of interaction or the differ-ences in affordances between the two technologies
Whereas other studies have documented aspects of the manual ED white-board technology (Wears amp Perry 2007 Wears et al 2007) these studies did notprovide a detailed comparison of the manual and new systems Thus the goals ofthis study were to document the information content functionality and format ofboth manual and electronic status boards in one particular ED to gain insight intospecific changes (in functionality and availability of information) that occurredduring the transition to the new technology
Methods
Data were collected from manual and electronic systems at a large academicmedical center hospital emergency department which had a patient volume of95000 patients per year Patient-tracking systems were used in multiple func-tional areas (such as adult care trauma and pediatric care) in this ED The EDcompletely transitioned to the computerized patient-tracking system at the timethe system was installed (that is the manual whiteboards were removed once theelectronic system became operational)
Data CollectionA month before the electronic patient-tracking system was implemented
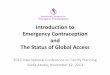
manual status boards in two ED treatment areas were systematically photographedfor their information content Similarly 18 months after the electronic system wasimplemented digital images (screen shots) of the electronic patient-tracking sys-tem were recorded (see Figure 2 for an example) To support the most direct compar-ison we took screen shots of and analyzed only the primary screen of the electronicpatient-tracking display because this display corresponded most closely to the man-ual status board and served as the default ED display We did not analyze addi-tional linked screens in the electronic system or other information sources used
Emergency Department Status Boards in Transition 43
44 Journal of Cognitive Engineering and Decision Making Spring 2010
Figu
re 2
Ele
ctro
nic
stat
us d
ispl
ay s
cree
n sh
ot (n
ames
obs
cure
d) R
epri
nted
from
Fai
rban
ks e
t al
Pro
ceed
ings
of t
he H
uman
Fac
tors
and
Erg
onom
ics
Soci
ety
Ann
ual M
eeti
ng2
008
concurrently in the manual system (eg paper charts) Additionally whereas theelectronic system included both desktop and wall-mounted large-format dis-plays the wall-mounted system consistently displayed only the primary screen(scrolling to show all patients)
Data were collected in two distinct areas of the ED the adult acute area whichtreats sick and injured patients requiring urgent or semiurgent treatment (such asheart attacks or strokes) and the adult nonacute area which treats routine nonur-gent cases (such as ankle sprains or minor lacerations) These areas are geographi-cally separated and have separate nurse stations with specifically assigned ED staffIn both cases data were captured every 30 min for continuous 8-hr periods duringa day shift (two different periods for the photographs and one period for thescreen shots because the latter could be accessed from a single remote location)
For the manual system there was a secondary board in the acute area that wasused on some days to track some (but not all) information regarding a small num-ber of ldquooverflowrdquo patients who did not fit on the primary board Typically thesewere less acute patients assigned to overflow locations This board was not pho-tographed because it was not used consistently and because not all data fieldswere represented
In all a total of 68 images (34 photos and 34 screen shots) were captured andedited for patient de-identification Example images from both systems are pro-vided in Figures 1 and 2 Note that the primary organizing scheme for both sys-tems is a matrix format with patients represented in rows (each row correspondingto a bed or location in the ED) and with different kinds of information about thepatient (demographic details assigned caregivers treatment plans) located incolumns Text symbols and colors are used in both systems
AnalysisTwo levels of analysis were conducted by an interdisciplinary research team
composed of emergency medicine physiciansresearchers and human factorsresearchers (authors TG RF AB and PP) For one analysis an overall assessmentof the range of information provided by both systems was conducted by examin-ing the photographs and screen shots We noted the type or function of the infor-mation its location on the whiteboard or screen (eg left side of board nursecolumn) the method of entry (handwritten indicated on a preprinted magnet ortaped or otherwise attached for the manual board typed picked or selected froma list or automatically filled when other entries were made for the electronic board)whether the entry was alphanumeric or symbolic (either hand-drawn or typed)whether there was color or font coding and for the electronic system whether anicon was used whether information could be clicked or selected and whetherhovering with a mouse revealed additional details
The second analysis provided additional details for specific areas of the statusboards We focused on fields that contained significant information related to clinicalcare and workflow specifically columns related to chief complaints and those relatedto patient treatment and disposition The chief complaint provides information about
Emergency Department Status Boards in Transition 45
the primary reason a patient has come to the emergency department as providedby patients to nurses during the triage process in which the criticality of patientsrsquocondition is assessed
Disposition is a term commonly used in emergency medicine to describe thepatientrsquos destination once the ED care has been completed and might include hospi-tal admission transfer to another hospital or discharge to home These areas weretranscribed into spreadsheets (maintaining the use of symbols text color etc) andcoded by the research team Columns between the two systems did not alwaysdirectly correspond For example the column labeled Disposition on the manualwhiteboard contained (among other things) clinical orders and disposition informa-tion regarding the patient On the electronic status board there were three columnsrelated to these functions two columns with alphanumericcolored codes (labeledCustom and Disposition) and one column that accepted free text or click-and-selecttext entries (labeled Comments) Thus all three columns were coded in the lattercase to allow comparison with the disposition column on the manual board
Codes were developed iteratively during the analysis using a grounded-theoryapproach (Glaser amp Strauss 1967) and represented the different functions thatthe information present on the status boards could provide Because coding wasperformed by group consensus we did not compute interrater reliability statisticsIn analyzing and categorizing the information we also computed quantitativeindicators to understand the differences between the electronic and the manualwhiteboard Each photograph or screen shot contained information about multi-ple patients and because images were obtained across a continuous time spaninformation about a particular patient typically appeared in multiple images Wecombined entries for each patient when evaluating the frequency of coded entriesso that identical information was counted only a single time for each patient
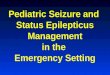
The columns we coded could contain multiple pieces of information for a sin-gle patient These were analyzed separately as they could represent different cate-gories of information Figure 3 shows two chief complaint entries associated with asingle patient The chief complaint entry changed over time (between two photo-graphs) Four different chief complaint functions were coded for this entry ldquocar vsdeerrdquo indicated the mechanism of injury ldquoL arm injuryrdquo represents the problem(injury) location of the problem (arm) and laterality (LLeft) Similarly in the com-ments column (electronic system) the entry ldquoGET EKG EKG DONErdquo contains twodisposition functions ldquoclinical workup planrdquo and ldquoplan progressrdquo That is a plan
46 Journal of Cognitive Engineering and Decision Making Spring 2010
Figure 3 Example of transcribed chief complaint data
for the clinical workflow of the patient is described by specifying the taskmdashldquoGETEKGrdquomdashto be performed as well as the status of the plan as it progressesmdashldquoEKGDONErdquo A list and definitions of all categories developed for both the chief com-plaint and dispositioncomments analysis is provided in the results section
Results
Overall 105 patients were shown on the manual whiteboards analyzed and80 on the electronic whiteboard representing differences in the patient numberstreated in the areas of the ED studied for the days on which data were collectedQuantitative results (described later) have been scaled to patient count to facilitatecomparisons between the manual and electronic systems The overall analysis isdescribed first followed by the detailed analysis of the chief complaint and dispo-sitioncomments columns of the status boards
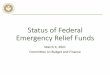
Overall Information ContentWe identified 41 categories of information across the manual and electronic sta-
tus boards as shown in Table 1 In 37 of the cases the information was present inboth systems representing the primary information fields containing patient demo-graphic details and provider information However there were important differencesSymbols (hand drawn) used by attending and resident physicians to track theirpatient-specific workflow (eg if they had examined or written notes about a patient)were present on the manual whiteboard but not in the electronic system The manualsystem also provided information about the overall ED (presenceabsence of an EDpharmacist) and individual rooms (stocked set up for pediatric patients) which wasnot available in the electronic system These annotations were either outside thematrix structure (eg notes at the top lines along the side of the board) or were indi-vidualized to care providers (workflow codes) In contrast information unique to theelectronic status board exploited the systemrsquos ability to automatically flag or computeinformation The electronic system provided the (computed) length of stay (colorcoded if longer than a specified time) rather than the time of arrival an indication ofchief complaints associated with regulatory quality measures or high-risk chief com-plaints the most recent patient viewed or edited by the user and an indication ofwhether the patient had a previous ED visit recorded in the electronic system
Both systems made use of color to code or highlight information For instanceon the manual board names and information regarding pediatric patients in thenonacute section of the ED (where both pediatric and adult patients are seen)were written in red and rooms configured for pediatric patients were highlightedwith a red line next to the room numbers In a different ED area the marker colorused changed with each shift so that the mix of colors on the board indicated(approximately) the overall progress in moving patients through the ED and afourth color was used to indicate admitted patients Previous studies have alsonoted the use of color on ED status boards (Wears et al 2007)
Emergency Department Status Boards in Transition 47
(text continues on page 54)
48 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 T
ype
s o
f In
form
ati
on
Re
pre
sen
ted
on
th
e M
an
ua
l an
do
r E
lect
ron
ic S
tatu
s D
isp
lay
Alo
ng
Wit
h M
eth
od
of
Info
rma
tio
n E
ntr
y
or
Dis
pla
y a
nd
Cla
rify
ing
No
tes
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Att
en
din
g p
hys
icia
nrsquos
x
xS
pe
cifi
c to
ph
ysic
ian
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Be
d r
ea
ssig
nm
en
t p
lan
x
xx
Loca
ted
to
th
e le
ft o
f th
e
cha
ng
ing
th
e w
ritt
en
m
atr
ix
roo
m n
um
be
r o
r st
icke
r
ED
ph
arm
aci
st o
no
ff d
uty
xx
xO
n d
uty
(gre
en
) o
ff d
uty
(re
d)
loca
ted
on
to
p o
f
the
bo
ard
Pat
ien
t is
pe
dia
tric
xP
atie
nt
nam
e w
ritt
en
in r
ed
Re
sid
en
t p
hys
icia
nrsquos
x
xx
Sp
eci
fic
to r
esi
de
nt
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Ro
om
is s
tock
ed
wit
h
xH
an
d-d
raw
n d
ot
ne
xt t
o
sup
plie
s ro
om
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

requires a careful understanding of the functions afforded by the old systems andthe manner in which the manual systems supported clinical work
Manual status boards are typically large dry-erase boards that display informa-tion such as patient demographics (eg name age gender) location (eg roombed) caregiver assignments clinical presentation data (eg symptoms diagnoses)and workup plan (eg planned and completed tests and treatments) Informationis typically represented in rows (corresponding to beds to which patients areassigned) and columns (corresponding to a category of information) often usingsymbols and color (see Figure 1) Manual status boards are located in central areasof the ED and are accessible to and used by a variety of caregivers and staff to com-municate information and coordinate individual and group activities
From the standpoint of distributed cognition (Hutchins 1997) status boards serveas a critical cognitive artifact storing and communicating information across time andindividuals in the ED (Nemeth OrsquoConnor Nunnally amp Cook 2007 Pennathuret al 2007 Wears amp Perry 2007 Xiao 2005) For example physicians may use thestatus board to track their own activities in treating and documenting the care of apatient whereas nurses may use them to indicate needs for testing or transportationto other ED staff Status boards support the maintenance of shared situation aware-ness across ED staff and preserve critical information across shift changes (Wears ampPerry 2007) In general these boards support an ED process whereby patients areinitially screened for condition severity when they come to the ED (the triageprocess) are examined by one or more physicians physicians-in-training and med-ical students receive tests and treatments appropriate to their conditions and eitherare admitted to stay in the hospital or leave for home (discharged)
Manual status boards were developed from the ground up over the past three tofour decades by ED practitioners to meet their immediate needs (Wears amp Perry2007) Similar to paper artifacts that co-evolve with an organizationrsquos work practices(Sellen amp Harper 2003) ED status boards developed based on usersrsquo needs andfunctions that the whiteboard medium can support They evolved from a simple listof patients and locations to a rich source of clinical and workflow informationAlthough the basic row-column format is similar across locations the particular for-mat of information representation on status boards is unique and customized to theneeds of caregivers in each hospital setting the boards dynamically represent thestate of the ED in densely encoded idiosyncratic but locally meaningful ways
Interaction with the manual status boards is direct fast and flexible Staff canread portions of the board in detail or get an overview of the level of demand byassessing the overall information density Staff are visible when they gather aroundand mark the whiteboard making it possible for others to notice and infer theiractivities (which may be difficult or impossible to tell when interacting with indi-vidual workstations) Information is primarily entered using markers and includesalphanumeric input as well as hand-drawn symbols and annotations
The status boards are malleable in the sense that they are flexible enough toadapt and support a variety of functions For example in some EDs staff use spe-cially designed prelabeled magnets to provide alerts and may use magnets or tape
40 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 41
Figu
re 1
Man
ual s
tatu
s bo
ard
phot
ogra
ph (n
ames
obs
cure
d) R
epri
nted
from
Pen
nath
ur e
t al
Pro
ceed
ings
of t
he H
uman
Fac
tors
and
Erg
onom
ics
Soci
ety
Ann
ual M
eeti
ng2
007
to attach paper forms or test results to the whiteboard (Wears Perry WilsonGalliers amp Fone 2007) Inputs are not restricted to the matrix format but caninclude annotations around the edges of the board or notations that continueacross multiple cells in a row or column Manual whiteboards thus share many ofthe affordances of other manual (paper-based) systems as described by Sellen andHarper (2003) including easy direct marking allowing flexible and ldquotailorablerdquomarkings based on the circumstances providing ldquoinformation at a glancerdquo that issimultaneously available to multiple ED staff and allowing activity to be implicitlycommunicated and coordinated because team members can observe one anotherrsquosactions or the trace of those actions on the status board
Manual to Electronic Status Board TransitionElectronic patient-tracking systems are being implemented as part of an overall
movement to computerize health care information that is driven by anticipatedimprovements in care coordination patient safety and efficiency (Aspden CorriganWolcott amp Erickson 2004 Committee on Quality of Health Care in America 2001Kohn Corrigan amp Donaldson 1999) Generally speaking these boards have beendeveloped by third-party vendors and usually have visual display layouts similarin nature to the whiteboards they have replaced Researchers have noted advan-tages in having a customized electronic tool to support multitasking in ED environ-ments (Laxmisan Hakimzada Sayan Green amp Patel 2007) Electronic systemsmay also address shortcomings of manual status boards Once erased informationcannot be recovered and information entered into one system (eg at hospitalregistration) cannot automatically populate the manual status board Thus repeateddata entry tasks may be required and information may be incomplete outdated orinconsistent across systems Electronic systems are often components of or linked toother hospital information systems and have the ability to log information inputs
Unlike the bottom-up evolutionary design of manual whiteboards the elec-tronic systems are typically purchased from third-party vendors often with onlymodest abilities for customization to reflect the individual uses in each hospital(but see Aronsky Jones Lanaghan amp Slovis 2008 for an example of a ldquohome-grownrdquo electronic system) Procurement is often led by organizational informationtechnology (IT) staff rather than clinicians and can be driven by overall organiza-tional needs and management goals such as system interoperability cost abilityto collect quality and efficiency measures integration with hospital bed manage-ment systems and data storage (Poon et al 2006) These needs may overshadowthose of the clinicians who have been using the manual whiteboard to supporttheir minute-by-minute work
For a variety of economic quality and policy reasons health care providerswill continue to transition to electronic systems Research in a number of settingshas indicated that when systems are designed based on an incorrect or rational-ized model of work performance suffers (Berg 1997 2004 Bisantz amp Ockerman2002 Button amp Harper 1993 Mackay 1999 Sachs 1995) New technology oftencreates a necessity for users to reorient themselves to the electronic system and
42 Journal of Cognitive Engineering and Decision Making Spring 2010
change their existing work practices by altering their tasks and configuring thenew systems In some cases the new technology may increase workload or lead toerrors if users are forced to adapt either the system or their tasks and strategiesduring critical periods (Cook amp Woods 1996) For new technologies to success-fully support or augment evolved work practices designers must start with a deepunderstanding of what functions the manual technologies support
Research ObjectivesIn observing a transition from manual to electronic status boards in two hospi-
tal emergency departments we found that providers reported a negative impact ofthe transition on communication and their ability to make sense of the overallstate of the ED (Pennathur et al 2007) This paper investigates the two technolo-gies in detail to try to identify design-oriented reasons for these difficulties Itcould be simply that the new system does not provide access to record or view thesame type or amount of information as the manual system Alternatively problemscould stem from the format of presentation or method of interaction or the differ-ences in affordances between the two technologies
Whereas other studies have documented aspects of the manual ED white-board technology (Wears amp Perry 2007 Wears et al 2007) these studies did notprovide a detailed comparison of the manual and new systems Thus the goals ofthis study were to document the information content functionality and format ofboth manual and electronic status boards in one particular ED to gain insight intospecific changes (in functionality and availability of information) that occurredduring the transition to the new technology
Methods
Data were collected from manual and electronic systems at a large academicmedical center hospital emergency department which had a patient volume of95000 patients per year Patient-tracking systems were used in multiple func-tional areas (such as adult care trauma and pediatric care) in this ED The EDcompletely transitioned to the computerized patient-tracking system at the timethe system was installed (that is the manual whiteboards were removed once theelectronic system became operational)
Data CollectionA month before the electronic patient-tracking system was implemented
manual status boards in two ED treatment areas were systematically photographedfor their information content Similarly 18 months after the electronic system wasimplemented digital images (screen shots) of the electronic patient-tracking sys-tem were recorded (see Figure 2 for an example) To support the most direct compar-ison we took screen shots of and analyzed only the primary screen of the electronicpatient-tracking display because this display corresponded most closely to the man-ual status board and served as the default ED display We did not analyze addi-tional linked screens in the electronic system or other information sources used
Emergency Department Status Boards in Transition 43
44 Journal of Cognitive Engineering and Decision Making Spring 2010
Figu
re 2
Ele
ctro
nic
stat
us d
ispl
ay s
cree
n sh
ot (n
ames
obs
cure
d) R
epri
nted
from
Fai
rban
ks e
t al
Pro
ceed
ings
of t
he H
uman
Fac
tors
and
Erg
onom
ics
Soci
ety
Ann
ual M
eeti
ng2
008
concurrently in the manual system (eg paper charts) Additionally whereas theelectronic system included both desktop and wall-mounted large-format dis-plays the wall-mounted system consistently displayed only the primary screen(scrolling to show all patients)
Data were collected in two distinct areas of the ED the adult acute area whichtreats sick and injured patients requiring urgent or semiurgent treatment (such asheart attacks or strokes) and the adult nonacute area which treats routine nonur-gent cases (such as ankle sprains or minor lacerations) These areas are geographi-cally separated and have separate nurse stations with specifically assigned ED staffIn both cases data were captured every 30 min for continuous 8-hr periods duringa day shift (two different periods for the photographs and one period for thescreen shots because the latter could be accessed from a single remote location)
For the manual system there was a secondary board in the acute area that wasused on some days to track some (but not all) information regarding a small num-ber of ldquooverflowrdquo patients who did not fit on the primary board Typically thesewere less acute patients assigned to overflow locations This board was not pho-tographed because it was not used consistently and because not all data fieldswere represented
In all a total of 68 images (34 photos and 34 screen shots) were captured andedited for patient de-identification Example images from both systems are pro-vided in Figures 1 and 2 Note that the primary organizing scheme for both sys-tems is a matrix format with patients represented in rows (each row correspondingto a bed or location in the ED) and with different kinds of information about thepatient (demographic details assigned caregivers treatment plans) located incolumns Text symbols and colors are used in both systems
AnalysisTwo levels of analysis were conducted by an interdisciplinary research team
composed of emergency medicine physiciansresearchers and human factorsresearchers (authors TG RF AB and PP) For one analysis an overall assessmentof the range of information provided by both systems was conducted by examin-ing the photographs and screen shots We noted the type or function of the infor-mation its location on the whiteboard or screen (eg left side of board nursecolumn) the method of entry (handwritten indicated on a preprinted magnet ortaped or otherwise attached for the manual board typed picked or selected froma list or automatically filled when other entries were made for the electronic board)whether the entry was alphanumeric or symbolic (either hand-drawn or typed)whether there was color or font coding and for the electronic system whether anicon was used whether information could be clicked or selected and whetherhovering with a mouse revealed additional details
The second analysis provided additional details for specific areas of the statusboards We focused on fields that contained significant information related to clinicalcare and workflow specifically columns related to chief complaints and those relatedto patient treatment and disposition The chief complaint provides information about
Emergency Department Status Boards in Transition 45
the primary reason a patient has come to the emergency department as providedby patients to nurses during the triage process in which the criticality of patientsrsquocondition is assessed
Disposition is a term commonly used in emergency medicine to describe thepatientrsquos destination once the ED care has been completed and might include hospi-tal admission transfer to another hospital or discharge to home These areas weretranscribed into spreadsheets (maintaining the use of symbols text color etc) andcoded by the research team Columns between the two systems did not alwaysdirectly correspond For example the column labeled Disposition on the manualwhiteboard contained (among other things) clinical orders and disposition informa-tion regarding the patient On the electronic status board there were three columnsrelated to these functions two columns with alphanumericcolored codes (labeledCustom and Disposition) and one column that accepted free text or click-and-selecttext entries (labeled Comments) Thus all three columns were coded in the lattercase to allow comparison with the disposition column on the manual board
Codes were developed iteratively during the analysis using a grounded-theoryapproach (Glaser amp Strauss 1967) and represented the different functions thatthe information present on the status boards could provide Because coding wasperformed by group consensus we did not compute interrater reliability statisticsIn analyzing and categorizing the information we also computed quantitativeindicators to understand the differences between the electronic and the manualwhiteboard Each photograph or screen shot contained information about multi-ple patients and because images were obtained across a continuous time spaninformation about a particular patient typically appeared in multiple images Wecombined entries for each patient when evaluating the frequency of coded entriesso that identical information was counted only a single time for each patient
The columns we coded could contain multiple pieces of information for a sin-gle patient These were analyzed separately as they could represent different cate-gories of information Figure 3 shows two chief complaint entries associated with asingle patient The chief complaint entry changed over time (between two photo-graphs) Four different chief complaint functions were coded for this entry ldquocar vsdeerrdquo indicated the mechanism of injury ldquoL arm injuryrdquo represents the problem(injury) location of the problem (arm) and laterality (LLeft) Similarly in the com-ments column (electronic system) the entry ldquoGET EKG EKG DONErdquo contains twodisposition functions ldquoclinical workup planrdquo and ldquoplan progressrdquo That is a plan
46 Journal of Cognitive Engineering and Decision Making Spring 2010
Figure 3 Example of transcribed chief complaint data
for the clinical workflow of the patient is described by specifying the taskmdashldquoGETEKGrdquomdashto be performed as well as the status of the plan as it progressesmdashldquoEKGDONErdquo A list and definitions of all categories developed for both the chief com-plaint and dispositioncomments analysis is provided in the results section
Results
Overall 105 patients were shown on the manual whiteboards analyzed and80 on the electronic whiteboard representing differences in the patient numberstreated in the areas of the ED studied for the days on which data were collectedQuantitative results (described later) have been scaled to patient count to facilitatecomparisons between the manual and electronic systems The overall analysis isdescribed first followed by the detailed analysis of the chief complaint and dispo-sitioncomments columns of the status boards
Overall Information ContentWe identified 41 categories of information across the manual and electronic sta-
tus boards as shown in Table 1 In 37 of the cases the information was present inboth systems representing the primary information fields containing patient demo-graphic details and provider information However there were important differencesSymbols (hand drawn) used by attending and resident physicians to track theirpatient-specific workflow (eg if they had examined or written notes about a patient)were present on the manual whiteboard but not in the electronic system The manualsystem also provided information about the overall ED (presenceabsence of an EDpharmacist) and individual rooms (stocked set up for pediatric patients) which wasnot available in the electronic system These annotations were either outside thematrix structure (eg notes at the top lines along the side of the board) or were indi-vidualized to care providers (workflow codes) In contrast information unique to theelectronic status board exploited the systemrsquos ability to automatically flag or computeinformation The electronic system provided the (computed) length of stay (colorcoded if longer than a specified time) rather than the time of arrival an indication ofchief complaints associated with regulatory quality measures or high-risk chief com-plaints the most recent patient viewed or edited by the user and an indication ofwhether the patient had a previous ED visit recorded in the electronic system
Both systems made use of color to code or highlight information For instanceon the manual board names and information regarding pediatric patients in thenonacute section of the ED (where both pediatric and adult patients are seen)were written in red and rooms configured for pediatric patients were highlightedwith a red line next to the room numbers In a different ED area the marker colorused changed with each shift so that the mix of colors on the board indicated(approximately) the overall progress in moving patients through the ED and afourth color was used to indicate admitted patients Previous studies have alsonoted the use of color on ED status boards (Wears et al 2007)
Emergency Department Status Boards in Transition 47
(text continues on page 54)
48 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 T
ype
s o
f In
form
ati
on
Re
pre
sen
ted
on
th
e M
an
ua
l an
do
r E
lect
ron
ic S
tatu
s D
isp
lay
Alo
ng
Wit
h M
eth
od
of
Info
rma
tio
n E
ntr
y
or
Dis
pla
y a
nd
Cla
rify
ing
No
tes
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Att
en
din
g p
hys
icia
nrsquos
x
xS
pe
cifi
c to
ph
ysic
ian
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Be
d r
ea
ssig
nm
en
t p
lan
x
xx
Loca
ted
to
th
e le
ft o
f th
e
cha
ng
ing
th
e w
ritt
en
m
atr
ix
roo
m n
um
be
r o
r st
icke
r
ED
ph
arm
aci
st o
no
ff d
uty
xx
xO
n d
uty
(gre
en
) o
ff d
uty
(re
d)
loca
ted
on
to
p o
f
the
bo
ard
Pat
ien
t is
pe
dia
tric
xP
atie
nt
nam
e w
ritt
en
in r
ed
Re
sid
en
t p
hys
icia
nrsquos
x
xx
Sp
eci
fic
to r
esi
de
nt
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Ro
om
is s
tock
ed
wit
h
xH
an
d-d
raw
n d
ot
ne
xt t
o
sup
plie
s ro
om
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

Emergency Department Status Boards in Transition 41
Figu
re 1
Man
ual s
tatu
s bo
ard
phot
ogra
ph (n
ames
obs
cure
d) R
epri
nted
from
Pen
nath
ur e
t al
Pro
ceed
ings
of t
he H
uman
Fac
tors
and
Erg
onom
ics
Soci
ety
Ann
ual M
eeti
ng2
007
to attach paper forms or test results to the whiteboard (Wears Perry WilsonGalliers amp Fone 2007) Inputs are not restricted to the matrix format but caninclude annotations around the edges of the board or notations that continueacross multiple cells in a row or column Manual whiteboards thus share many ofthe affordances of other manual (paper-based) systems as described by Sellen andHarper (2003) including easy direct marking allowing flexible and ldquotailorablerdquomarkings based on the circumstances providing ldquoinformation at a glancerdquo that issimultaneously available to multiple ED staff and allowing activity to be implicitlycommunicated and coordinated because team members can observe one anotherrsquosactions or the trace of those actions on the status board
Manual to Electronic Status Board TransitionElectronic patient-tracking systems are being implemented as part of an overall
movement to computerize health care information that is driven by anticipatedimprovements in care coordination patient safety and efficiency (Aspden CorriganWolcott amp Erickson 2004 Committee on Quality of Health Care in America 2001Kohn Corrigan amp Donaldson 1999) Generally speaking these boards have beendeveloped by third-party vendors and usually have visual display layouts similarin nature to the whiteboards they have replaced Researchers have noted advan-tages in having a customized electronic tool to support multitasking in ED environ-ments (Laxmisan Hakimzada Sayan Green amp Patel 2007) Electronic systemsmay also address shortcomings of manual status boards Once erased informationcannot be recovered and information entered into one system (eg at hospitalregistration) cannot automatically populate the manual status board Thus repeateddata entry tasks may be required and information may be incomplete outdated orinconsistent across systems Electronic systems are often components of or linked toother hospital information systems and have the ability to log information inputs
Unlike the bottom-up evolutionary design of manual whiteboards the elec-tronic systems are typically purchased from third-party vendors often with onlymodest abilities for customization to reflect the individual uses in each hospital(but see Aronsky Jones Lanaghan amp Slovis 2008 for an example of a ldquohome-grownrdquo electronic system) Procurement is often led by organizational informationtechnology (IT) staff rather than clinicians and can be driven by overall organiza-tional needs and management goals such as system interoperability cost abilityto collect quality and efficiency measures integration with hospital bed manage-ment systems and data storage (Poon et al 2006) These needs may overshadowthose of the clinicians who have been using the manual whiteboard to supporttheir minute-by-minute work
For a variety of economic quality and policy reasons health care providerswill continue to transition to electronic systems Research in a number of settingshas indicated that when systems are designed based on an incorrect or rational-ized model of work performance suffers (Berg 1997 2004 Bisantz amp Ockerman2002 Button amp Harper 1993 Mackay 1999 Sachs 1995) New technology oftencreates a necessity for users to reorient themselves to the electronic system and
42 Journal of Cognitive Engineering and Decision Making Spring 2010
change their existing work practices by altering their tasks and configuring thenew systems In some cases the new technology may increase workload or lead toerrors if users are forced to adapt either the system or their tasks and strategiesduring critical periods (Cook amp Woods 1996) For new technologies to success-fully support or augment evolved work practices designers must start with a deepunderstanding of what functions the manual technologies support
Research ObjectivesIn observing a transition from manual to electronic status boards in two hospi-
tal emergency departments we found that providers reported a negative impact ofthe transition on communication and their ability to make sense of the overallstate of the ED (Pennathur et al 2007) This paper investigates the two technolo-gies in detail to try to identify design-oriented reasons for these difficulties Itcould be simply that the new system does not provide access to record or view thesame type or amount of information as the manual system Alternatively problemscould stem from the format of presentation or method of interaction or the differ-ences in affordances between the two technologies
Whereas other studies have documented aspects of the manual ED white-board technology (Wears amp Perry 2007 Wears et al 2007) these studies did notprovide a detailed comparison of the manual and new systems Thus the goals ofthis study were to document the information content functionality and format ofboth manual and electronic status boards in one particular ED to gain insight intospecific changes (in functionality and availability of information) that occurredduring the transition to the new technology
Methods
Data were collected from manual and electronic systems at a large academicmedical center hospital emergency department which had a patient volume of95000 patients per year Patient-tracking systems were used in multiple func-tional areas (such as adult care trauma and pediatric care) in this ED The EDcompletely transitioned to the computerized patient-tracking system at the timethe system was installed (that is the manual whiteboards were removed once theelectronic system became operational)
Data CollectionA month before the electronic patient-tracking system was implemented
manual status boards in two ED treatment areas were systematically photographedfor their information content Similarly 18 months after the electronic system wasimplemented digital images (screen shots) of the electronic patient-tracking sys-tem were recorded (see Figure 2 for an example) To support the most direct compar-ison we took screen shots of and analyzed only the primary screen of the electronicpatient-tracking display because this display corresponded most closely to the man-ual status board and served as the default ED display We did not analyze addi-tional linked screens in the electronic system or other information sources used
Emergency Department Status Boards in Transition 43
44 Journal of Cognitive Engineering and Decision Making Spring 2010
Figu
re 2
Ele
ctro
nic
stat
us d
ispl
ay s
cree
n sh
ot (n
ames
obs
cure
d) R
epri
nted
from
Fai
rban
ks e
t al
Pro
ceed
ings
of t
he H
uman
Fac
tors
and
Erg
onom
ics
Soci
ety
Ann
ual M
eeti
ng2
008
concurrently in the manual system (eg paper charts) Additionally whereas theelectronic system included both desktop and wall-mounted large-format dis-plays the wall-mounted system consistently displayed only the primary screen(scrolling to show all patients)
Data were collected in two distinct areas of the ED the adult acute area whichtreats sick and injured patients requiring urgent or semiurgent treatment (such asheart attacks or strokes) and the adult nonacute area which treats routine nonur-gent cases (such as ankle sprains or minor lacerations) These areas are geographi-cally separated and have separate nurse stations with specifically assigned ED staffIn both cases data were captured every 30 min for continuous 8-hr periods duringa day shift (two different periods for the photographs and one period for thescreen shots because the latter could be accessed from a single remote location)
For the manual system there was a secondary board in the acute area that wasused on some days to track some (but not all) information regarding a small num-ber of ldquooverflowrdquo patients who did not fit on the primary board Typically thesewere less acute patients assigned to overflow locations This board was not pho-tographed because it was not used consistently and because not all data fieldswere represented
In all a total of 68 images (34 photos and 34 screen shots) were captured andedited for patient de-identification Example images from both systems are pro-vided in Figures 1 and 2 Note that the primary organizing scheme for both sys-tems is a matrix format with patients represented in rows (each row correspondingto a bed or location in the ED) and with different kinds of information about thepatient (demographic details assigned caregivers treatment plans) located incolumns Text symbols and colors are used in both systems
AnalysisTwo levels of analysis were conducted by an interdisciplinary research team
composed of emergency medicine physiciansresearchers and human factorsresearchers (authors TG RF AB and PP) For one analysis an overall assessmentof the range of information provided by both systems was conducted by examin-ing the photographs and screen shots We noted the type or function of the infor-mation its location on the whiteboard or screen (eg left side of board nursecolumn) the method of entry (handwritten indicated on a preprinted magnet ortaped or otherwise attached for the manual board typed picked or selected froma list or automatically filled when other entries were made for the electronic board)whether the entry was alphanumeric or symbolic (either hand-drawn or typed)whether there was color or font coding and for the electronic system whether anicon was used whether information could be clicked or selected and whetherhovering with a mouse revealed additional details
The second analysis provided additional details for specific areas of the statusboards We focused on fields that contained significant information related to clinicalcare and workflow specifically columns related to chief complaints and those relatedto patient treatment and disposition The chief complaint provides information about
Emergency Department Status Boards in Transition 45
the primary reason a patient has come to the emergency department as providedby patients to nurses during the triage process in which the criticality of patientsrsquocondition is assessed
Disposition is a term commonly used in emergency medicine to describe thepatientrsquos destination once the ED care has been completed and might include hospi-tal admission transfer to another hospital or discharge to home These areas weretranscribed into spreadsheets (maintaining the use of symbols text color etc) andcoded by the research team Columns between the two systems did not alwaysdirectly correspond For example the column labeled Disposition on the manualwhiteboard contained (among other things) clinical orders and disposition informa-tion regarding the patient On the electronic status board there were three columnsrelated to these functions two columns with alphanumericcolored codes (labeledCustom and Disposition) and one column that accepted free text or click-and-selecttext entries (labeled Comments) Thus all three columns were coded in the lattercase to allow comparison with the disposition column on the manual board
Codes were developed iteratively during the analysis using a grounded-theoryapproach (Glaser amp Strauss 1967) and represented the different functions thatthe information present on the status boards could provide Because coding wasperformed by group consensus we did not compute interrater reliability statisticsIn analyzing and categorizing the information we also computed quantitativeindicators to understand the differences between the electronic and the manualwhiteboard Each photograph or screen shot contained information about multi-ple patients and because images were obtained across a continuous time spaninformation about a particular patient typically appeared in multiple images Wecombined entries for each patient when evaluating the frequency of coded entriesso that identical information was counted only a single time for each patient
The columns we coded could contain multiple pieces of information for a sin-gle patient These were analyzed separately as they could represent different cate-gories of information Figure 3 shows two chief complaint entries associated with asingle patient The chief complaint entry changed over time (between two photo-graphs) Four different chief complaint functions were coded for this entry ldquocar vsdeerrdquo indicated the mechanism of injury ldquoL arm injuryrdquo represents the problem(injury) location of the problem (arm) and laterality (LLeft) Similarly in the com-ments column (electronic system) the entry ldquoGET EKG EKG DONErdquo contains twodisposition functions ldquoclinical workup planrdquo and ldquoplan progressrdquo That is a plan
46 Journal of Cognitive Engineering and Decision Making Spring 2010
Figure 3 Example of transcribed chief complaint data
for the clinical workflow of the patient is described by specifying the taskmdashldquoGETEKGrdquomdashto be performed as well as the status of the plan as it progressesmdashldquoEKGDONErdquo A list and definitions of all categories developed for both the chief com-plaint and dispositioncomments analysis is provided in the results section
Results
Overall 105 patients were shown on the manual whiteboards analyzed and80 on the electronic whiteboard representing differences in the patient numberstreated in the areas of the ED studied for the days on which data were collectedQuantitative results (described later) have been scaled to patient count to facilitatecomparisons between the manual and electronic systems The overall analysis isdescribed first followed by the detailed analysis of the chief complaint and dispo-sitioncomments columns of the status boards
Overall Information ContentWe identified 41 categories of information across the manual and electronic sta-
tus boards as shown in Table 1 In 37 of the cases the information was present inboth systems representing the primary information fields containing patient demo-graphic details and provider information However there were important differencesSymbols (hand drawn) used by attending and resident physicians to track theirpatient-specific workflow (eg if they had examined or written notes about a patient)were present on the manual whiteboard but not in the electronic system The manualsystem also provided information about the overall ED (presenceabsence of an EDpharmacist) and individual rooms (stocked set up for pediatric patients) which wasnot available in the electronic system These annotations were either outside thematrix structure (eg notes at the top lines along the side of the board) or were indi-vidualized to care providers (workflow codes) In contrast information unique to theelectronic status board exploited the systemrsquos ability to automatically flag or computeinformation The electronic system provided the (computed) length of stay (colorcoded if longer than a specified time) rather than the time of arrival an indication ofchief complaints associated with regulatory quality measures or high-risk chief com-plaints the most recent patient viewed or edited by the user and an indication ofwhether the patient had a previous ED visit recorded in the electronic system
Both systems made use of color to code or highlight information For instanceon the manual board names and information regarding pediatric patients in thenonacute section of the ED (where both pediatric and adult patients are seen)were written in red and rooms configured for pediatric patients were highlightedwith a red line next to the room numbers In a different ED area the marker colorused changed with each shift so that the mix of colors on the board indicated(approximately) the overall progress in moving patients through the ED and afourth color was used to indicate admitted patients Previous studies have alsonoted the use of color on ED status boards (Wears et al 2007)
Emergency Department Status Boards in Transition 47
(text continues on page 54)
48 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 T
ype
s o
f In
form
ati
on
Re
pre
sen
ted
on
th
e M
an
ua
l an
do
r E
lect
ron
ic S
tatu
s D
isp
lay
Alo
ng
Wit
h M
eth
od
of
Info
rma
tio
n E
ntr
y
or
Dis
pla
y a
nd
Cla
rify
ing
No
tes
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Att
en
din
g p
hys
icia
nrsquos
x
xS
pe
cifi
c to
ph
ysic
ian
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Be
d r
ea
ssig
nm
en
t p
lan
x
xx
Loca
ted
to
th
e le
ft o
f th
e
cha
ng
ing
th
e w
ritt
en
m
atr
ix
roo
m n
um
be
r o
r st
icke
r
ED
ph
arm
aci
st o
no
ff d
uty
xx
xO
n d
uty
(gre
en
) o
ff d
uty
(re
d)
loca
ted
on
to
p o
f
the
bo
ard
Pat
ien
t is
pe
dia
tric
xP
atie
nt
nam
e w
ritt
en
in r
ed
Re
sid
en
t p
hys
icia
nrsquos
x
xx
Sp
eci
fic
to r
esi
de
nt
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Ro
om
is s
tock
ed
wit
h
xH
an
d-d
raw
n d
ot
ne
xt t
o
sup
plie
s ro
om
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

to attach paper forms or test results to the whiteboard (Wears Perry WilsonGalliers amp Fone 2007) Inputs are not restricted to the matrix format but caninclude annotations around the edges of the board or notations that continueacross multiple cells in a row or column Manual whiteboards thus share many ofthe affordances of other manual (paper-based) systems as described by Sellen andHarper (2003) including easy direct marking allowing flexible and ldquotailorablerdquomarkings based on the circumstances providing ldquoinformation at a glancerdquo that issimultaneously available to multiple ED staff and allowing activity to be implicitlycommunicated and coordinated because team members can observe one anotherrsquosactions or the trace of those actions on the status board
Manual to Electronic Status Board TransitionElectronic patient-tracking systems are being implemented as part of an overall
movement to computerize health care information that is driven by anticipatedimprovements in care coordination patient safety and efficiency (Aspden CorriganWolcott amp Erickson 2004 Committee on Quality of Health Care in America 2001Kohn Corrigan amp Donaldson 1999) Generally speaking these boards have beendeveloped by third-party vendors and usually have visual display layouts similarin nature to the whiteboards they have replaced Researchers have noted advan-tages in having a customized electronic tool to support multitasking in ED environ-ments (Laxmisan Hakimzada Sayan Green amp Patel 2007) Electronic systemsmay also address shortcomings of manual status boards Once erased informationcannot be recovered and information entered into one system (eg at hospitalregistration) cannot automatically populate the manual status board Thus repeateddata entry tasks may be required and information may be incomplete outdated orinconsistent across systems Electronic systems are often components of or linked toother hospital information systems and have the ability to log information inputs
Unlike the bottom-up evolutionary design of manual whiteboards the elec-tronic systems are typically purchased from third-party vendors often with onlymodest abilities for customization to reflect the individual uses in each hospital(but see Aronsky Jones Lanaghan amp Slovis 2008 for an example of a ldquohome-grownrdquo electronic system) Procurement is often led by organizational informationtechnology (IT) staff rather than clinicians and can be driven by overall organiza-tional needs and management goals such as system interoperability cost abilityto collect quality and efficiency measures integration with hospital bed manage-ment systems and data storage (Poon et al 2006) These needs may overshadowthose of the clinicians who have been using the manual whiteboard to supporttheir minute-by-minute work
For a variety of economic quality and policy reasons health care providerswill continue to transition to electronic systems Research in a number of settingshas indicated that when systems are designed based on an incorrect or rational-ized model of work performance suffers (Berg 1997 2004 Bisantz amp Ockerman2002 Button amp Harper 1993 Mackay 1999 Sachs 1995) New technology oftencreates a necessity for users to reorient themselves to the electronic system and
42 Journal of Cognitive Engineering and Decision Making Spring 2010
change their existing work practices by altering their tasks and configuring thenew systems In some cases the new technology may increase workload or lead toerrors if users are forced to adapt either the system or their tasks and strategiesduring critical periods (Cook amp Woods 1996) For new technologies to success-fully support or augment evolved work practices designers must start with a deepunderstanding of what functions the manual technologies support
Research ObjectivesIn observing a transition from manual to electronic status boards in two hospi-
tal emergency departments we found that providers reported a negative impact ofthe transition on communication and their ability to make sense of the overallstate of the ED (Pennathur et al 2007) This paper investigates the two technolo-gies in detail to try to identify design-oriented reasons for these difficulties Itcould be simply that the new system does not provide access to record or view thesame type or amount of information as the manual system Alternatively problemscould stem from the format of presentation or method of interaction or the differ-ences in affordances between the two technologies
Whereas other studies have documented aspects of the manual ED white-board technology (Wears amp Perry 2007 Wears et al 2007) these studies did notprovide a detailed comparison of the manual and new systems Thus the goals ofthis study were to document the information content functionality and format ofboth manual and electronic status boards in one particular ED to gain insight intospecific changes (in functionality and availability of information) that occurredduring the transition to the new technology
Methods
Data were collected from manual and electronic systems at a large academicmedical center hospital emergency department which had a patient volume of95000 patients per year Patient-tracking systems were used in multiple func-tional areas (such as adult care trauma and pediatric care) in this ED The EDcompletely transitioned to the computerized patient-tracking system at the timethe system was installed (that is the manual whiteboards were removed once theelectronic system became operational)
Data CollectionA month before the electronic patient-tracking system was implemented
manual status boards in two ED treatment areas were systematically photographedfor their information content Similarly 18 months after the electronic system wasimplemented digital images (screen shots) of the electronic patient-tracking sys-tem were recorded (see Figure 2 for an example) To support the most direct compar-ison we took screen shots of and analyzed only the primary screen of the electronicpatient-tracking display because this display corresponded most closely to the man-ual status board and served as the default ED display We did not analyze addi-tional linked screens in the electronic system or other information sources used
Emergency Department Status Boards in Transition 43
44 Journal of Cognitive Engineering and Decision Making Spring 2010
Figu
re 2
Ele
ctro
nic
stat
us d
ispl
ay s
cree
n sh
ot (n
ames
obs
cure
d) R
epri
nted
from
Fai
rban
ks e
t al
Pro
ceed
ings
of t
he H
uman
Fac
tors
and
Erg
onom
ics
Soci
ety
Ann
ual M
eeti
ng2
008
concurrently in the manual system (eg paper charts) Additionally whereas theelectronic system included both desktop and wall-mounted large-format dis-plays the wall-mounted system consistently displayed only the primary screen(scrolling to show all patients)
Data were collected in two distinct areas of the ED the adult acute area whichtreats sick and injured patients requiring urgent or semiurgent treatment (such asheart attacks or strokes) and the adult nonacute area which treats routine nonur-gent cases (such as ankle sprains or minor lacerations) These areas are geographi-cally separated and have separate nurse stations with specifically assigned ED staffIn both cases data were captured every 30 min for continuous 8-hr periods duringa day shift (two different periods for the photographs and one period for thescreen shots because the latter could be accessed from a single remote location)
For the manual system there was a secondary board in the acute area that wasused on some days to track some (but not all) information regarding a small num-ber of ldquooverflowrdquo patients who did not fit on the primary board Typically thesewere less acute patients assigned to overflow locations This board was not pho-tographed because it was not used consistently and because not all data fieldswere represented
In all a total of 68 images (34 photos and 34 screen shots) were captured andedited for patient de-identification Example images from both systems are pro-vided in Figures 1 and 2 Note that the primary organizing scheme for both sys-tems is a matrix format with patients represented in rows (each row correspondingto a bed or location in the ED) and with different kinds of information about thepatient (demographic details assigned caregivers treatment plans) located incolumns Text symbols and colors are used in both systems
AnalysisTwo levels of analysis were conducted by an interdisciplinary research team
composed of emergency medicine physiciansresearchers and human factorsresearchers (authors TG RF AB and PP) For one analysis an overall assessmentof the range of information provided by both systems was conducted by examin-ing the photographs and screen shots We noted the type or function of the infor-mation its location on the whiteboard or screen (eg left side of board nursecolumn) the method of entry (handwritten indicated on a preprinted magnet ortaped or otherwise attached for the manual board typed picked or selected froma list or automatically filled when other entries were made for the electronic board)whether the entry was alphanumeric or symbolic (either hand-drawn or typed)whether there was color or font coding and for the electronic system whether anicon was used whether information could be clicked or selected and whetherhovering with a mouse revealed additional details
The second analysis provided additional details for specific areas of the statusboards We focused on fields that contained significant information related to clinicalcare and workflow specifically columns related to chief complaints and those relatedto patient treatment and disposition The chief complaint provides information about
Emergency Department Status Boards in Transition 45
the primary reason a patient has come to the emergency department as providedby patients to nurses during the triage process in which the criticality of patientsrsquocondition is assessed
Disposition is a term commonly used in emergency medicine to describe thepatientrsquos destination once the ED care has been completed and might include hospi-tal admission transfer to another hospital or discharge to home These areas weretranscribed into spreadsheets (maintaining the use of symbols text color etc) andcoded by the research team Columns between the two systems did not alwaysdirectly correspond For example the column labeled Disposition on the manualwhiteboard contained (among other things) clinical orders and disposition informa-tion regarding the patient On the electronic status board there were three columnsrelated to these functions two columns with alphanumericcolored codes (labeledCustom and Disposition) and one column that accepted free text or click-and-selecttext entries (labeled Comments) Thus all three columns were coded in the lattercase to allow comparison with the disposition column on the manual board
Codes were developed iteratively during the analysis using a grounded-theoryapproach (Glaser amp Strauss 1967) and represented the different functions thatthe information present on the status boards could provide Because coding wasperformed by group consensus we did not compute interrater reliability statisticsIn analyzing and categorizing the information we also computed quantitativeindicators to understand the differences between the electronic and the manualwhiteboard Each photograph or screen shot contained information about multi-ple patients and because images were obtained across a continuous time spaninformation about a particular patient typically appeared in multiple images Wecombined entries for each patient when evaluating the frequency of coded entriesso that identical information was counted only a single time for each patient
The columns we coded could contain multiple pieces of information for a sin-gle patient These were analyzed separately as they could represent different cate-gories of information Figure 3 shows two chief complaint entries associated with asingle patient The chief complaint entry changed over time (between two photo-graphs) Four different chief complaint functions were coded for this entry ldquocar vsdeerrdquo indicated the mechanism of injury ldquoL arm injuryrdquo represents the problem(injury) location of the problem (arm) and laterality (LLeft) Similarly in the com-ments column (electronic system) the entry ldquoGET EKG EKG DONErdquo contains twodisposition functions ldquoclinical workup planrdquo and ldquoplan progressrdquo That is a plan
46 Journal of Cognitive Engineering and Decision Making Spring 2010
Figure 3 Example of transcribed chief complaint data
for the clinical workflow of the patient is described by specifying the taskmdashldquoGETEKGrdquomdashto be performed as well as the status of the plan as it progressesmdashldquoEKGDONErdquo A list and definitions of all categories developed for both the chief com-plaint and dispositioncomments analysis is provided in the results section
Results
Overall 105 patients were shown on the manual whiteboards analyzed and80 on the electronic whiteboard representing differences in the patient numberstreated in the areas of the ED studied for the days on which data were collectedQuantitative results (described later) have been scaled to patient count to facilitatecomparisons between the manual and electronic systems The overall analysis isdescribed first followed by the detailed analysis of the chief complaint and dispo-sitioncomments columns of the status boards
Overall Information ContentWe identified 41 categories of information across the manual and electronic sta-
tus boards as shown in Table 1 In 37 of the cases the information was present inboth systems representing the primary information fields containing patient demo-graphic details and provider information However there were important differencesSymbols (hand drawn) used by attending and resident physicians to track theirpatient-specific workflow (eg if they had examined or written notes about a patient)were present on the manual whiteboard but not in the electronic system The manualsystem also provided information about the overall ED (presenceabsence of an EDpharmacist) and individual rooms (stocked set up for pediatric patients) which wasnot available in the electronic system These annotations were either outside thematrix structure (eg notes at the top lines along the side of the board) or were indi-vidualized to care providers (workflow codes) In contrast information unique to theelectronic status board exploited the systemrsquos ability to automatically flag or computeinformation The electronic system provided the (computed) length of stay (colorcoded if longer than a specified time) rather than the time of arrival an indication ofchief complaints associated with regulatory quality measures or high-risk chief com-plaints the most recent patient viewed or edited by the user and an indication ofwhether the patient had a previous ED visit recorded in the electronic system
Both systems made use of color to code or highlight information For instanceon the manual board names and information regarding pediatric patients in thenonacute section of the ED (where both pediatric and adult patients are seen)were written in red and rooms configured for pediatric patients were highlightedwith a red line next to the room numbers In a different ED area the marker colorused changed with each shift so that the mix of colors on the board indicated(approximately) the overall progress in moving patients through the ED and afourth color was used to indicate admitted patients Previous studies have alsonoted the use of color on ED status boards (Wears et al 2007)
Emergency Department Status Boards in Transition 47
(text continues on page 54)
48 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 T
ype
s o
f In
form
ati
on
Re
pre
sen
ted
on
th
e M
an
ua
l an
do
r E
lect
ron
ic S
tatu
s D
isp
lay
Alo
ng
Wit
h M
eth
od
of
Info
rma
tio
n E
ntr
y
or
Dis
pla
y a
nd
Cla
rify
ing
No
tes
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Att
en
din
g p
hys
icia
nrsquos
x
xS
pe
cifi
c to
ph
ysic
ian
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Be
d r
ea
ssig
nm
en
t p
lan
x
xx
Loca
ted
to
th
e le
ft o
f th
e
cha
ng
ing
th
e w
ritt
en
m
atr
ix
roo
m n
um
be
r o
r st
icke
r
ED
ph
arm
aci
st o
no
ff d
uty
xx
xO
n d
uty
(gre
en
) o
ff d
uty
(re
d)
loca
ted
on
to
p o
f
the
bo
ard
Pat
ien
t is
pe
dia
tric
xP
atie
nt
nam
e w
ritt
en
in r
ed
Re
sid
en
t p
hys
icia
nrsquos
x
xx
Sp
eci
fic
to r
esi
de
nt
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Ro
om
is s
tock
ed
wit
h
xH
an
d-d
raw
n d
ot
ne
xt t
o
sup
plie
s ro
om
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

change their existing work practices by altering their tasks and configuring thenew systems In some cases the new technology may increase workload or lead toerrors if users are forced to adapt either the system or their tasks and strategiesduring critical periods (Cook amp Woods 1996) For new technologies to success-fully support or augment evolved work practices designers must start with a deepunderstanding of what functions the manual technologies support
Research ObjectivesIn observing a transition from manual to electronic status boards in two hospi-
tal emergency departments we found that providers reported a negative impact ofthe transition on communication and their ability to make sense of the overallstate of the ED (Pennathur et al 2007) This paper investigates the two technolo-gies in detail to try to identify design-oriented reasons for these difficulties Itcould be simply that the new system does not provide access to record or view thesame type or amount of information as the manual system Alternatively problemscould stem from the format of presentation or method of interaction or the differ-ences in affordances between the two technologies
Whereas other studies have documented aspects of the manual ED white-board technology (Wears amp Perry 2007 Wears et al 2007) these studies did notprovide a detailed comparison of the manual and new systems Thus the goals ofthis study were to document the information content functionality and format ofboth manual and electronic status boards in one particular ED to gain insight intospecific changes (in functionality and availability of information) that occurredduring the transition to the new technology
Methods
Data were collected from manual and electronic systems at a large academicmedical center hospital emergency department which had a patient volume of95000 patients per year Patient-tracking systems were used in multiple func-tional areas (such as adult care trauma and pediatric care) in this ED The EDcompletely transitioned to the computerized patient-tracking system at the timethe system was installed (that is the manual whiteboards were removed once theelectronic system became operational)
Data CollectionA month before the electronic patient-tracking system was implemented
manual status boards in two ED treatment areas were systematically photographedfor their information content Similarly 18 months after the electronic system wasimplemented digital images (screen shots) of the electronic patient-tracking sys-tem were recorded (see Figure 2 for an example) To support the most direct compar-ison we took screen shots of and analyzed only the primary screen of the electronicpatient-tracking display because this display corresponded most closely to the man-ual status board and served as the default ED display We did not analyze addi-tional linked screens in the electronic system or other information sources used
Emergency Department Status Boards in Transition 43
44 Journal of Cognitive Engineering and Decision Making Spring 2010
Figu
re 2
Ele
ctro
nic
stat
us d
ispl
ay s
cree
n sh
ot (n
ames
obs
cure
d) R
epri
nted
from
Fai
rban
ks e
t al
Pro
ceed
ings
of t
he H
uman
Fac
tors
and
Erg
onom
ics
Soci
ety
Ann
ual M
eeti
ng2
008
concurrently in the manual system (eg paper charts) Additionally whereas theelectronic system included both desktop and wall-mounted large-format dis-plays the wall-mounted system consistently displayed only the primary screen(scrolling to show all patients)
Data were collected in two distinct areas of the ED the adult acute area whichtreats sick and injured patients requiring urgent or semiurgent treatment (such asheart attacks or strokes) and the adult nonacute area which treats routine nonur-gent cases (such as ankle sprains or minor lacerations) These areas are geographi-cally separated and have separate nurse stations with specifically assigned ED staffIn both cases data were captured every 30 min for continuous 8-hr periods duringa day shift (two different periods for the photographs and one period for thescreen shots because the latter could be accessed from a single remote location)
For the manual system there was a secondary board in the acute area that wasused on some days to track some (but not all) information regarding a small num-ber of ldquooverflowrdquo patients who did not fit on the primary board Typically thesewere less acute patients assigned to overflow locations This board was not pho-tographed because it was not used consistently and because not all data fieldswere represented
In all a total of 68 images (34 photos and 34 screen shots) were captured andedited for patient de-identification Example images from both systems are pro-vided in Figures 1 and 2 Note that the primary organizing scheme for both sys-tems is a matrix format with patients represented in rows (each row correspondingto a bed or location in the ED) and with different kinds of information about thepatient (demographic details assigned caregivers treatment plans) located incolumns Text symbols and colors are used in both systems
AnalysisTwo levels of analysis were conducted by an interdisciplinary research team
composed of emergency medicine physiciansresearchers and human factorsresearchers (authors TG RF AB and PP) For one analysis an overall assessmentof the range of information provided by both systems was conducted by examin-ing the photographs and screen shots We noted the type or function of the infor-mation its location on the whiteboard or screen (eg left side of board nursecolumn) the method of entry (handwritten indicated on a preprinted magnet ortaped or otherwise attached for the manual board typed picked or selected froma list or automatically filled when other entries were made for the electronic board)whether the entry was alphanumeric or symbolic (either hand-drawn or typed)whether there was color or font coding and for the electronic system whether anicon was used whether information could be clicked or selected and whetherhovering with a mouse revealed additional details
The second analysis provided additional details for specific areas of the statusboards We focused on fields that contained significant information related to clinicalcare and workflow specifically columns related to chief complaints and those relatedto patient treatment and disposition The chief complaint provides information about
Emergency Department Status Boards in Transition 45
the primary reason a patient has come to the emergency department as providedby patients to nurses during the triage process in which the criticality of patientsrsquocondition is assessed
Disposition is a term commonly used in emergency medicine to describe thepatientrsquos destination once the ED care has been completed and might include hospi-tal admission transfer to another hospital or discharge to home These areas weretranscribed into spreadsheets (maintaining the use of symbols text color etc) andcoded by the research team Columns between the two systems did not alwaysdirectly correspond For example the column labeled Disposition on the manualwhiteboard contained (among other things) clinical orders and disposition informa-tion regarding the patient On the electronic status board there were three columnsrelated to these functions two columns with alphanumericcolored codes (labeledCustom and Disposition) and one column that accepted free text or click-and-selecttext entries (labeled Comments) Thus all three columns were coded in the lattercase to allow comparison with the disposition column on the manual board
Codes were developed iteratively during the analysis using a grounded-theoryapproach (Glaser amp Strauss 1967) and represented the different functions thatthe information present on the status boards could provide Because coding wasperformed by group consensus we did not compute interrater reliability statisticsIn analyzing and categorizing the information we also computed quantitativeindicators to understand the differences between the electronic and the manualwhiteboard Each photograph or screen shot contained information about multi-ple patients and because images were obtained across a continuous time spaninformation about a particular patient typically appeared in multiple images Wecombined entries for each patient when evaluating the frequency of coded entriesso that identical information was counted only a single time for each patient
The columns we coded could contain multiple pieces of information for a sin-gle patient These were analyzed separately as they could represent different cate-gories of information Figure 3 shows two chief complaint entries associated with asingle patient The chief complaint entry changed over time (between two photo-graphs) Four different chief complaint functions were coded for this entry ldquocar vsdeerrdquo indicated the mechanism of injury ldquoL arm injuryrdquo represents the problem(injury) location of the problem (arm) and laterality (LLeft) Similarly in the com-ments column (electronic system) the entry ldquoGET EKG EKG DONErdquo contains twodisposition functions ldquoclinical workup planrdquo and ldquoplan progressrdquo That is a plan
46 Journal of Cognitive Engineering and Decision Making Spring 2010
Figure 3 Example of transcribed chief complaint data
for the clinical workflow of the patient is described by specifying the taskmdashldquoGETEKGrdquomdashto be performed as well as the status of the plan as it progressesmdashldquoEKGDONErdquo A list and definitions of all categories developed for both the chief com-plaint and dispositioncomments analysis is provided in the results section
Results
Overall 105 patients were shown on the manual whiteboards analyzed and80 on the electronic whiteboard representing differences in the patient numberstreated in the areas of the ED studied for the days on which data were collectedQuantitative results (described later) have been scaled to patient count to facilitatecomparisons between the manual and electronic systems The overall analysis isdescribed first followed by the detailed analysis of the chief complaint and dispo-sitioncomments columns of the status boards
Overall Information ContentWe identified 41 categories of information across the manual and electronic sta-
tus boards as shown in Table 1 In 37 of the cases the information was present inboth systems representing the primary information fields containing patient demo-graphic details and provider information However there were important differencesSymbols (hand drawn) used by attending and resident physicians to track theirpatient-specific workflow (eg if they had examined or written notes about a patient)were present on the manual whiteboard but not in the electronic system The manualsystem also provided information about the overall ED (presenceabsence of an EDpharmacist) and individual rooms (stocked set up for pediatric patients) which wasnot available in the electronic system These annotations were either outside thematrix structure (eg notes at the top lines along the side of the board) or were indi-vidualized to care providers (workflow codes) In contrast information unique to theelectronic status board exploited the systemrsquos ability to automatically flag or computeinformation The electronic system provided the (computed) length of stay (colorcoded if longer than a specified time) rather than the time of arrival an indication ofchief complaints associated with regulatory quality measures or high-risk chief com-plaints the most recent patient viewed or edited by the user and an indication ofwhether the patient had a previous ED visit recorded in the electronic system
Both systems made use of color to code or highlight information For instanceon the manual board names and information regarding pediatric patients in thenonacute section of the ED (where both pediatric and adult patients are seen)were written in red and rooms configured for pediatric patients were highlightedwith a red line next to the room numbers In a different ED area the marker colorused changed with each shift so that the mix of colors on the board indicated(approximately) the overall progress in moving patients through the ED and afourth color was used to indicate admitted patients Previous studies have alsonoted the use of color on ED status boards (Wears et al 2007)
Emergency Department Status Boards in Transition 47
(text continues on page 54)
48 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 T
ype
s o
f In
form
ati
on
Re
pre
sen
ted
on
th
e M
an
ua
l an
do
r E
lect
ron
ic S
tatu
s D
isp
lay
Alo
ng
Wit
h M
eth
od
of
Info
rma
tio
n E
ntr
y
or
Dis
pla
y a
nd
Cla
rify
ing
No
tes
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Att
en
din
g p
hys
icia
nrsquos
x
xS
pe
cifi
c to
ph
ysic
ian
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Be
d r
ea
ssig
nm
en
t p
lan
x
xx
Loca
ted
to
th
e le
ft o
f th
e
cha
ng
ing
th
e w
ritt
en
m
atr
ix
roo
m n
um
be
r o
r st
icke
r
ED
ph
arm
aci
st o
no
ff d
uty
xx
xO
n d
uty
(gre
en
) o
ff d
uty
(re
d)
loca
ted
on
to
p o
f
the
bo
ard
Pat
ien
t is
pe
dia
tric
xP
atie
nt
nam
e w
ritt
en
in r
ed
Re
sid
en
t p
hys
icia
nrsquos
x
xx
Sp
eci
fic
to r
esi
de
nt
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Ro
om
is s
tock
ed
wit
h
xH
an
d-d
raw
n d
ot
ne
xt t
o
sup
plie
s ro
om
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

44 Journal of Cognitive Engineering and Decision Making Spring 2010
Figu
re 2
Ele
ctro
nic
stat
us d
ispl
ay s
cree
n sh
ot (n
ames
obs
cure
d) R
epri
nted
from
Fai
rban
ks e
t al
Pro
ceed
ings
of t
he H
uman
Fac
tors
and
Erg
onom
ics
Soci
ety
Ann
ual M
eeti
ng2
008
concurrently in the manual system (eg paper charts) Additionally whereas theelectronic system included both desktop and wall-mounted large-format dis-plays the wall-mounted system consistently displayed only the primary screen(scrolling to show all patients)
Data were collected in two distinct areas of the ED the adult acute area whichtreats sick and injured patients requiring urgent or semiurgent treatment (such asheart attacks or strokes) and the adult nonacute area which treats routine nonur-gent cases (such as ankle sprains or minor lacerations) These areas are geographi-cally separated and have separate nurse stations with specifically assigned ED staffIn both cases data were captured every 30 min for continuous 8-hr periods duringa day shift (two different periods for the photographs and one period for thescreen shots because the latter could be accessed from a single remote location)
For the manual system there was a secondary board in the acute area that wasused on some days to track some (but not all) information regarding a small num-ber of ldquooverflowrdquo patients who did not fit on the primary board Typically thesewere less acute patients assigned to overflow locations This board was not pho-tographed because it was not used consistently and because not all data fieldswere represented
In all a total of 68 images (34 photos and 34 screen shots) were captured andedited for patient de-identification Example images from both systems are pro-vided in Figures 1 and 2 Note that the primary organizing scheme for both sys-tems is a matrix format with patients represented in rows (each row correspondingto a bed or location in the ED) and with different kinds of information about thepatient (demographic details assigned caregivers treatment plans) located incolumns Text symbols and colors are used in both systems
AnalysisTwo levels of analysis were conducted by an interdisciplinary research team
composed of emergency medicine physiciansresearchers and human factorsresearchers (authors TG RF AB and PP) For one analysis an overall assessmentof the range of information provided by both systems was conducted by examin-ing the photographs and screen shots We noted the type or function of the infor-mation its location on the whiteboard or screen (eg left side of board nursecolumn) the method of entry (handwritten indicated on a preprinted magnet ortaped or otherwise attached for the manual board typed picked or selected froma list or automatically filled when other entries were made for the electronic board)whether the entry was alphanumeric or symbolic (either hand-drawn or typed)whether there was color or font coding and for the electronic system whether anicon was used whether information could be clicked or selected and whetherhovering with a mouse revealed additional details
The second analysis provided additional details for specific areas of the statusboards We focused on fields that contained significant information related to clinicalcare and workflow specifically columns related to chief complaints and those relatedto patient treatment and disposition The chief complaint provides information about
Emergency Department Status Boards in Transition 45
the primary reason a patient has come to the emergency department as providedby patients to nurses during the triage process in which the criticality of patientsrsquocondition is assessed
Disposition is a term commonly used in emergency medicine to describe thepatientrsquos destination once the ED care has been completed and might include hospi-tal admission transfer to another hospital or discharge to home These areas weretranscribed into spreadsheets (maintaining the use of symbols text color etc) andcoded by the research team Columns between the two systems did not alwaysdirectly correspond For example the column labeled Disposition on the manualwhiteboard contained (among other things) clinical orders and disposition informa-tion regarding the patient On the electronic status board there were three columnsrelated to these functions two columns with alphanumericcolored codes (labeledCustom and Disposition) and one column that accepted free text or click-and-selecttext entries (labeled Comments) Thus all three columns were coded in the lattercase to allow comparison with the disposition column on the manual board
Codes were developed iteratively during the analysis using a grounded-theoryapproach (Glaser amp Strauss 1967) and represented the different functions thatthe information present on the status boards could provide Because coding wasperformed by group consensus we did not compute interrater reliability statisticsIn analyzing and categorizing the information we also computed quantitativeindicators to understand the differences between the electronic and the manualwhiteboard Each photograph or screen shot contained information about multi-ple patients and because images were obtained across a continuous time spaninformation about a particular patient typically appeared in multiple images Wecombined entries for each patient when evaluating the frequency of coded entriesso that identical information was counted only a single time for each patient
The columns we coded could contain multiple pieces of information for a sin-gle patient These were analyzed separately as they could represent different cate-gories of information Figure 3 shows two chief complaint entries associated with asingle patient The chief complaint entry changed over time (between two photo-graphs) Four different chief complaint functions were coded for this entry ldquocar vsdeerrdquo indicated the mechanism of injury ldquoL arm injuryrdquo represents the problem(injury) location of the problem (arm) and laterality (LLeft) Similarly in the com-ments column (electronic system) the entry ldquoGET EKG EKG DONErdquo contains twodisposition functions ldquoclinical workup planrdquo and ldquoplan progressrdquo That is a plan
46 Journal of Cognitive Engineering and Decision Making Spring 2010
Figure 3 Example of transcribed chief complaint data
for the clinical workflow of the patient is described by specifying the taskmdashldquoGETEKGrdquomdashto be performed as well as the status of the plan as it progressesmdashldquoEKGDONErdquo A list and definitions of all categories developed for both the chief com-plaint and dispositioncomments analysis is provided in the results section
Results
Overall 105 patients were shown on the manual whiteboards analyzed and80 on the electronic whiteboard representing differences in the patient numberstreated in the areas of the ED studied for the days on which data were collectedQuantitative results (described later) have been scaled to patient count to facilitatecomparisons between the manual and electronic systems The overall analysis isdescribed first followed by the detailed analysis of the chief complaint and dispo-sitioncomments columns of the status boards
Overall Information ContentWe identified 41 categories of information across the manual and electronic sta-
tus boards as shown in Table 1 In 37 of the cases the information was present inboth systems representing the primary information fields containing patient demo-graphic details and provider information However there were important differencesSymbols (hand drawn) used by attending and resident physicians to track theirpatient-specific workflow (eg if they had examined or written notes about a patient)were present on the manual whiteboard but not in the electronic system The manualsystem also provided information about the overall ED (presenceabsence of an EDpharmacist) and individual rooms (stocked set up for pediatric patients) which wasnot available in the electronic system These annotations were either outside thematrix structure (eg notes at the top lines along the side of the board) or were indi-vidualized to care providers (workflow codes) In contrast information unique to theelectronic status board exploited the systemrsquos ability to automatically flag or computeinformation The electronic system provided the (computed) length of stay (colorcoded if longer than a specified time) rather than the time of arrival an indication ofchief complaints associated with regulatory quality measures or high-risk chief com-plaints the most recent patient viewed or edited by the user and an indication ofwhether the patient had a previous ED visit recorded in the electronic system
Both systems made use of color to code or highlight information For instanceon the manual board names and information regarding pediatric patients in thenonacute section of the ED (where both pediatric and adult patients are seen)were written in red and rooms configured for pediatric patients were highlightedwith a red line next to the room numbers In a different ED area the marker colorused changed with each shift so that the mix of colors on the board indicated(approximately) the overall progress in moving patients through the ED and afourth color was used to indicate admitted patients Previous studies have alsonoted the use of color on ED status boards (Wears et al 2007)
Emergency Department Status Boards in Transition 47
(text continues on page 54)
48 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 T
ype
s o
f In
form
ati
on
Re
pre
sen
ted
on
th
e M
an
ua
l an
do
r E
lect
ron
ic S
tatu
s D
isp
lay
Alo
ng
Wit
h M
eth
od
of
Info
rma
tio
n E
ntr
y
or
Dis
pla
y a
nd
Cla
rify
ing
No
tes
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Att
en
din
g p
hys
icia
nrsquos
x
xS
pe
cifi
c to
ph
ysic
ian
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Be
d r
ea
ssig
nm
en
t p
lan
x
xx
Loca
ted
to
th
e le
ft o
f th
e
cha
ng
ing
th
e w
ritt
en
m
atr
ix
roo
m n
um
be
r o
r st
icke
r
ED
ph
arm
aci
st o
no
ff d
uty
xx
xO
n d
uty
(gre
en
) o
ff d
uty
(re
d)
loca
ted
on
to
p o
f
the
bo
ard
Pat
ien
t is
pe
dia
tric
xP
atie
nt
nam
e w
ritt
en
in r
ed
Re
sid
en
t p
hys
icia
nrsquos
x
xx
Sp
eci
fic
to r
esi
de
nt
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Ro
om
is s
tock
ed
wit
h
xH
an
d-d
raw
n d
ot
ne
xt t
o
sup
plie
s ro
om
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

concurrently in the manual system (eg paper charts) Additionally whereas theelectronic system included both desktop and wall-mounted large-format dis-plays the wall-mounted system consistently displayed only the primary screen(scrolling to show all patients)
Data were collected in two distinct areas of the ED the adult acute area whichtreats sick and injured patients requiring urgent or semiurgent treatment (such asheart attacks or strokes) and the adult nonacute area which treats routine nonur-gent cases (such as ankle sprains or minor lacerations) These areas are geographi-cally separated and have separate nurse stations with specifically assigned ED staffIn both cases data were captured every 30 min for continuous 8-hr periods duringa day shift (two different periods for the photographs and one period for thescreen shots because the latter could be accessed from a single remote location)
For the manual system there was a secondary board in the acute area that wasused on some days to track some (but not all) information regarding a small num-ber of ldquooverflowrdquo patients who did not fit on the primary board Typically thesewere less acute patients assigned to overflow locations This board was not pho-tographed because it was not used consistently and because not all data fieldswere represented
In all a total of 68 images (34 photos and 34 screen shots) were captured andedited for patient de-identification Example images from both systems are pro-vided in Figures 1 and 2 Note that the primary organizing scheme for both sys-tems is a matrix format with patients represented in rows (each row correspondingto a bed or location in the ED) and with different kinds of information about thepatient (demographic details assigned caregivers treatment plans) located incolumns Text symbols and colors are used in both systems
AnalysisTwo levels of analysis were conducted by an interdisciplinary research team
composed of emergency medicine physiciansresearchers and human factorsresearchers (authors TG RF AB and PP) For one analysis an overall assessmentof the range of information provided by both systems was conducted by examin-ing the photographs and screen shots We noted the type or function of the infor-mation its location on the whiteboard or screen (eg left side of board nursecolumn) the method of entry (handwritten indicated on a preprinted magnet ortaped or otherwise attached for the manual board typed picked or selected froma list or automatically filled when other entries were made for the electronic board)whether the entry was alphanumeric or symbolic (either hand-drawn or typed)whether there was color or font coding and for the electronic system whether anicon was used whether information could be clicked or selected and whetherhovering with a mouse revealed additional details
The second analysis provided additional details for specific areas of the statusboards We focused on fields that contained significant information related to clinicalcare and workflow specifically columns related to chief complaints and those relatedto patient treatment and disposition The chief complaint provides information about
Emergency Department Status Boards in Transition 45
the primary reason a patient has come to the emergency department as providedby patients to nurses during the triage process in which the criticality of patientsrsquocondition is assessed
Disposition is a term commonly used in emergency medicine to describe thepatientrsquos destination once the ED care has been completed and might include hospi-tal admission transfer to another hospital or discharge to home These areas weretranscribed into spreadsheets (maintaining the use of symbols text color etc) andcoded by the research team Columns between the two systems did not alwaysdirectly correspond For example the column labeled Disposition on the manualwhiteboard contained (among other things) clinical orders and disposition informa-tion regarding the patient On the electronic status board there were three columnsrelated to these functions two columns with alphanumericcolored codes (labeledCustom and Disposition) and one column that accepted free text or click-and-selecttext entries (labeled Comments) Thus all three columns were coded in the lattercase to allow comparison with the disposition column on the manual board
Codes were developed iteratively during the analysis using a grounded-theoryapproach (Glaser amp Strauss 1967) and represented the different functions thatthe information present on the status boards could provide Because coding wasperformed by group consensus we did not compute interrater reliability statisticsIn analyzing and categorizing the information we also computed quantitativeindicators to understand the differences between the electronic and the manualwhiteboard Each photograph or screen shot contained information about multi-ple patients and because images were obtained across a continuous time spaninformation about a particular patient typically appeared in multiple images Wecombined entries for each patient when evaluating the frequency of coded entriesso that identical information was counted only a single time for each patient
The columns we coded could contain multiple pieces of information for a sin-gle patient These were analyzed separately as they could represent different cate-gories of information Figure 3 shows two chief complaint entries associated with asingle patient The chief complaint entry changed over time (between two photo-graphs) Four different chief complaint functions were coded for this entry ldquocar vsdeerrdquo indicated the mechanism of injury ldquoL arm injuryrdquo represents the problem(injury) location of the problem (arm) and laterality (LLeft) Similarly in the com-ments column (electronic system) the entry ldquoGET EKG EKG DONErdquo contains twodisposition functions ldquoclinical workup planrdquo and ldquoplan progressrdquo That is a plan
46 Journal of Cognitive Engineering and Decision Making Spring 2010
Figure 3 Example of transcribed chief complaint data
for the clinical workflow of the patient is described by specifying the taskmdashldquoGETEKGrdquomdashto be performed as well as the status of the plan as it progressesmdashldquoEKGDONErdquo A list and definitions of all categories developed for both the chief com-plaint and dispositioncomments analysis is provided in the results section
Results
Overall 105 patients were shown on the manual whiteboards analyzed and80 on the electronic whiteboard representing differences in the patient numberstreated in the areas of the ED studied for the days on which data were collectedQuantitative results (described later) have been scaled to patient count to facilitatecomparisons between the manual and electronic systems The overall analysis isdescribed first followed by the detailed analysis of the chief complaint and dispo-sitioncomments columns of the status boards
Overall Information ContentWe identified 41 categories of information across the manual and electronic sta-
tus boards as shown in Table 1 In 37 of the cases the information was present inboth systems representing the primary information fields containing patient demo-graphic details and provider information However there were important differencesSymbols (hand drawn) used by attending and resident physicians to track theirpatient-specific workflow (eg if they had examined or written notes about a patient)were present on the manual whiteboard but not in the electronic system The manualsystem also provided information about the overall ED (presenceabsence of an EDpharmacist) and individual rooms (stocked set up for pediatric patients) which wasnot available in the electronic system These annotations were either outside thematrix structure (eg notes at the top lines along the side of the board) or were indi-vidualized to care providers (workflow codes) In contrast information unique to theelectronic status board exploited the systemrsquos ability to automatically flag or computeinformation The electronic system provided the (computed) length of stay (colorcoded if longer than a specified time) rather than the time of arrival an indication ofchief complaints associated with regulatory quality measures or high-risk chief com-plaints the most recent patient viewed or edited by the user and an indication ofwhether the patient had a previous ED visit recorded in the electronic system
Both systems made use of color to code or highlight information For instanceon the manual board names and information regarding pediatric patients in thenonacute section of the ED (where both pediatric and adult patients are seen)were written in red and rooms configured for pediatric patients were highlightedwith a red line next to the room numbers In a different ED area the marker colorused changed with each shift so that the mix of colors on the board indicated(approximately) the overall progress in moving patients through the ED and afourth color was used to indicate admitted patients Previous studies have alsonoted the use of color on ED status boards (Wears et al 2007)
Emergency Department Status Boards in Transition 47
(text continues on page 54)
48 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 T
ype
s o
f In
form
ati
on
Re
pre
sen
ted
on
th
e M
an
ua
l an
do
r E
lect
ron
ic S
tatu
s D
isp
lay
Alo
ng
Wit
h M
eth
od
of
Info
rma
tio
n E
ntr
y
or
Dis
pla
y a
nd
Cla
rify
ing
No
tes
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Att
en
din
g p
hys
icia
nrsquos
x
xS
pe
cifi
c to
ph
ysic
ian
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Be
d r
ea
ssig
nm
en
t p
lan
x
xx
Loca
ted
to
th
e le
ft o
f th
e
cha
ng
ing
th
e w
ritt
en
m
atr
ix
roo
m n
um
be
r o
r st
icke
r
ED
ph
arm
aci
st o
no
ff d
uty
xx
xO
n d
uty
(gre
en
) o
ff d
uty
(re
d)
loca
ted
on
to
p o
f
the
bo
ard
Pat
ien
t is
pe
dia
tric
xP
atie
nt
nam
e w
ritt
en
in r
ed
Re
sid
en
t p
hys
icia
nrsquos
x
xx
Sp
eci
fic
to r
esi
de
nt
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Ro
om
is s
tock
ed
wit
h
xH
an
d-d
raw
n d
ot
ne
xt t
o
sup
plie
s ro
om
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

the primary reason a patient has come to the emergency department as providedby patients to nurses during the triage process in which the criticality of patientsrsquocondition is assessed
Disposition is a term commonly used in emergency medicine to describe thepatientrsquos destination once the ED care has been completed and might include hospi-tal admission transfer to another hospital or discharge to home These areas weretranscribed into spreadsheets (maintaining the use of symbols text color etc) andcoded by the research team Columns between the two systems did not alwaysdirectly correspond For example the column labeled Disposition on the manualwhiteboard contained (among other things) clinical orders and disposition informa-tion regarding the patient On the electronic status board there were three columnsrelated to these functions two columns with alphanumericcolored codes (labeledCustom and Disposition) and one column that accepted free text or click-and-selecttext entries (labeled Comments) Thus all three columns were coded in the lattercase to allow comparison with the disposition column on the manual board
Codes were developed iteratively during the analysis using a grounded-theoryapproach (Glaser amp Strauss 1967) and represented the different functions thatthe information present on the status boards could provide Because coding wasperformed by group consensus we did not compute interrater reliability statisticsIn analyzing and categorizing the information we also computed quantitativeindicators to understand the differences between the electronic and the manualwhiteboard Each photograph or screen shot contained information about multi-ple patients and because images were obtained across a continuous time spaninformation about a particular patient typically appeared in multiple images Wecombined entries for each patient when evaluating the frequency of coded entriesso that identical information was counted only a single time for each patient
The columns we coded could contain multiple pieces of information for a sin-gle patient These were analyzed separately as they could represent different cate-gories of information Figure 3 shows two chief complaint entries associated with asingle patient The chief complaint entry changed over time (between two photo-graphs) Four different chief complaint functions were coded for this entry ldquocar vsdeerrdquo indicated the mechanism of injury ldquoL arm injuryrdquo represents the problem(injury) location of the problem (arm) and laterality (LLeft) Similarly in the com-ments column (electronic system) the entry ldquoGET EKG EKG DONErdquo contains twodisposition functions ldquoclinical workup planrdquo and ldquoplan progressrdquo That is a plan
46 Journal of Cognitive Engineering and Decision Making Spring 2010
Figure 3 Example of transcribed chief complaint data
for the clinical workflow of the patient is described by specifying the taskmdashldquoGETEKGrdquomdashto be performed as well as the status of the plan as it progressesmdashldquoEKGDONErdquo A list and definitions of all categories developed for both the chief com-plaint and dispositioncomments analysis is provided in the results section
Results
Overall 105 patients were shown on the manual whiteboards analyzed and80 on the electronic whiteboard representing differences in the patient numberstreated in the areas of the ED studied for the days on which data were collectedQuantitative results (described later) have been scaled to patient count to facilitatecomparisons between the manual and electronic systems The overall analysis isdescribed first followed by the detailed analysis of the chief complaint and dispo-sitioncomments columns of the status boards
Overall Information ContentWe identified 41 categories of information across the manual and electronic sta-
tus boards as shown in Table 1 In 37 of the cases the information was present inboth systems representing the primary information fields containing patient demo-graphic details and provider information However there were important differencesSymbols (hand drawn) used by attending and resident physicians to track theirpatient-specific workflow (eg if they had examined or written notes about a patient)were present on the manual whiteboard but not in the electronic system The manualsystem also provided information about the overall ED (presenceabsence of an EDpharmacist) and individual rooms (stocked set up for pediatric patients) which wasnot available in the electronic system These annotations were either outside thematrix structure (eg notes at the top lines along the side of the board) or were indi-vidualized to care providers (workflow codes) In contrast information unique to theelectronic status board exploited the systemrsquos ability to automatically flag or computeinformation The electronic system provided the (computed) length of stay (colorcoded if longer than a specified time) rather than the time of arrival an indication ofchief complaints associated with regulatory quality measures or high-risk chief com-plaints the most recent patient viewed or edited by the user and an indication ofwhether the patient had a previous ED visit recorded in the electronic system
Both systems made use of color to code or highlight information For instanceon the manual board names and information regarding pediatric patients in thenonacute section of the ED (where both pediatric and adult patients are seen)were written in red and rooms configured for pediatric patients were highlightedwith a red line next to the room numbers In a different ED area the marker colorused changed with each shift so that the mix of colors on the board indicated(approximately) the overall progress in moving patients through the ED and afourth color was used to indicate admitted patients Previous studies have alsonoted the use of color on ED status boards (Wears et al 2007)
Emergency Department Status Boards in Transition 47
(text continues on page 54)
48 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 T
ype
s o
f In
form
ati
on
Re
pre
sen
ted
on
th
e M
an
ua
l an
do
r E
lect
ron
ic S
tatu
s D
isp
lay
Alo
ng
Wit
h M
eth
od
of
Info
rma
tio
n E
ntr
y
or
Dis
pla
y a
nd
Cla
rify
ing
No
tes
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Att
en
din
g p
hys
icia
nrsquos
x
xS
pe
cifi
c to
ph
ysic
ian
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Be
d r
ea
ssig
nm
en
t p
lan
x
xx
Loca
ted
to
th
e le
ft o
f th
e
cha
ng
ing
th
e w
ritt
en
m
atr
ix
roo
m n
um
be
r o
r st
icke
r
ED
ph
arm
aci
st o
no
ff d
uty
xx
xO
n d
uty
(gre
en
) o
ff d
uty
(re
d)
loca
ted
on
to
p o
f
the
bo
ard
Pat
ien
t is
pe
dia
tric
xP
atie
nt
nam
e w
ritt
en
in r
ed
Re
sid
en
t p
hys
icia
nrsquos
x
xx
Sp
eci
fic
to r
esi
de
nt
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Ro
om
is s
tock
ed
wit
h
xH
an
d-d
raw
n d
ot
ne
xt t
o
sup
plie
s ro
om
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

for the clinical workflow of the patient is described by specifying the taskmdashldquoGETEKGrdquomdashto be performed as well as the status of the plan as it progressesmdashldquoEKGDONErdquo A list and definitions of all categories developed for both the chief com-plaint and dispositioncomments analysis is provided in the results section
Results
Overall 105 patients were shown on the manual whiteboards analyzed and80 on the electronic whiteboard representing differences in the patient numberstreated in the areas of the ED studied for the days on which data were collectedQuantitative results (described later) have been scaled to patient count to facilitatecomparisons between the manual and electronic systems The overall analysis isdescribed first followed by the detailed analysis of the chief complaint and dispo-sitioncomments columns of the status boards
Overall Information ContentWe identified 41 categories of information across the manual and electronic sta-
tus boards as shown in Table 1 In 37 of the cases the information was present inboth systems representing the primary information fields containing patient demo-graphic details and provider information However there were important differencesSymbols (hand drawn) used by attending and resident physicians to track theirpatient-specific workflow (eg if they had examined or written notes about a patient)were present on the manual whiteboard but not in the electronic system The manualsystem also provided information about the overall ED (presenceabsence of an EDpharmacist) and individual rooms (stocked set up for pediatric patients) which wasnot available in the electronic system These annotations were either outside thematrix structure (eg notes at the top lines along the side of the board) or were indi-vidualized to care providers (workflow codes) In contrast information unique to theelectronic status board exploited the systemrsquos ability to automatically flag or computeinformation The electronic system provided the (computed) length of stay (colorcoded if longer than a specified time) rather than the time of arrival an indication ofchief complaints associated with regulatory quality measures or high-risk chief com-plaints the most recent patient viewed or edited by the user and an indication ofwhether the patient had a previous ED visit recorded in the electronic system
Both systems made use of color to code or highlight information For instanceon the manual board names and information regarding pediatric patients in thenonacute section of the ED (where both pediatric and adult patients are seen)were written in red and rooms configured for pediatric patients were highlightedwith a red line next to the room numbers In a different ED area the marker colorused changed with each shift so that the mix of colors on the board indicated(approximately) the overall progress in moving patients through the ED and afourth color was used to indicate admitted patients Previous studies have alsonoted the use of color on ED status boards (Wears et al 2007)
Emergency Department Status Boards in Transition 47
(text continues on page 54)
48 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 T
ype
s o
f In
form
ati
on
Re
pre
sen
ted
on
th
e M
an
ua
l an
do
r E
lect
ron
ic S
tatu
s D
isp
lay
Alo
ng
Wit
h M
eth
od
of
Info
rma
tio
n E
ntr
y
or
Dis
pla
y a
nd
Cla
rify
ing
No
tes
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Att
en
din
g p
hys
icia
nrsquos
x
xS
pe
cifi
c to
ph
ysic
ian
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Be
d r
ea
ssig
nm
en
t p
lan
x
xx
Loca
ted
to
th
e le
ft o
f th
e
cha
ng
ing
th
e w
ritt
en
m
atr
ix
roo
m n
um
be
r o
r st
icke
r
ED
ph
arm
aci
st o
no
ff d
uty
xx
xO
n d
uty
(gre
en
) o
ff d
uty
(re
d)
loca
ted
on
to
p o
f
the
bo
ard
Pat
ien
t is
pe
dia
tric
xP
atie
nt
nam
e w
ritt
en
in r
ed
Re
sid
en
t p
hys
icia
nrsquos
x
xx
Sp
eci
fic
to r
esi
de
nt
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Ro
om
is s
tock
ed
wit
h
xH
an
d-d
raw
n d
ot
ne
xt t
o
sup
plie
s ro
om
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

48 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 T
ype
s o
f In
form
ati
on
Re
pre
sen
ted
on
th
e M
an
ua
l an
do
r E
lect
ron
ic S
tatu
s D
isp
lay
Alo
ng
Wit
h M
eth
od
of
Info
rma
tio
n E
ntr
y
or
Dis
pla
y a
nd
Cla
rify
ing
No
tes
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Att
en
din
g p
hys
icia
nrsquos
x
xS
pe
cifi
c to
ph
ysic
ian
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Be
d r
ea
ssig
nm
en
t p
lan
x
xx
Loca
ted
to
th
e le
ft o
f th
e
cha
ng
ing
th
e w
ritt
en
m
atr
ix
roo
m n
um
be
r o
r st
icke
r
ED
ph
arm
aci
st o
no
ff d
uty
xx
xO
n d
uty
(gre
en
) o
ff d
uty
(re
d)
loca
ted
on
to
p o
f
the
bo
ard
Pat
ien
t is
pe
dia
tric
xP
atie
nt
nam
e w
ritt
en
in r
ed
Re
sid
en
t p
hys
icia
nrsquos
x
xx
Sp
eci
fic
to r
esi
de
nt
wo
rkfl
ow
sym
bo
ls
ind
ica
tin
g p
rog
ress
wit
h p
ati
en
t
Ro
om
is s
tock
ed
wit
h
xH
an
d-d
raw
n d
ot
ne
xt t
o
sup
plie
s ro
om
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

Emergency Department Status Boards in Transition 49
Ro
om
sa
ve
d f
or
pa
rtic
ula
r x
xx
Eg
ldquoS
av
e f
or
Gyn
rdquo
tre
atm
en
ts
Sh
ift
of
pa
tie
nt
arr
iva
lx
Pa
tie
nt
info
rma
tio
n
wri
tte
n in
sa
me
co
lor
thro
ug
ho
ut
a s
hif
t
ldquoold
er
colo
rsrdquo
sig
nif
y
lon
ge
r-d
ura
tio
n
pa
tie
nts
Tim
e (h
ou
r) t
ha
t n
ext
vit
als
x
x
sho
uld
be
ta
ken
Tim
e p
ati
en
t a
rriv
ed
at
xx
tria
ge
Tim
e p
ati
en
t m
ov
ed
fro
m
xx
wa
itin
g r
oo
m t
o b
ed
in E
D
Ch
ief
com
pla
int
wit
h
xb
ar
xH
igh
-ris
k ch
ief
com
pla
ints
po
ten
tia
l ris
k o
r (r
ed
ba
r to
left
of
cell)
qu
alit
y m
ea
sure
qu
alit
y m
ea
sure
(gre
en
ba
r) p
rese
nt
on
ly if
com
pla
int
wa
s
pic
k-se
lect
ed
Dia
gn
osi
s in
form
ati
on
x
xx
Blu
e le
tte
r D
en
tere
d e
lse
wh
ere
in t
he
sys
tem
Dis
po
siti
on
scr
ee
n a
cce
ssx
ba
rx
Co
lore
d b
ar
to le
ft o
f ce
ll
(gre
en
if ldquo
En
terrdquo
clic
ked
on
Dis
po
siti
on
scr
ee
n)
Flo
w s
he
et
info
rma
tio
n
xx
xLe
tte
r F
(vit
al s
ign
s) is
av
aila
ble
(ab
sen
ce o
f in
dic
ato
r
do
es
no
t in
dic
ate
ab
sen
ce o
f fl
ow
sh
ee
t)
Len
gth
-of-
sta
y a
lert
xx
xx
A c
olo
red
clo
ck ic
on
gre
en
if L
OS
lt 6
hr
red
oth
erw
ise
Co
nti
nu
ed n
ext p
ag
e
50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

50 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Len
gth
of
sta
y t
ime
sin
ce
xx
x
pa
tie
ntrsquo
s in
form
ati
on
en
tere
d a
t tr
iag
e
Mo
st r
ece
nt
pa
tie
nt
xx
Ast
eri
sks
ma
rk p
ati
en
t
acc
ess
ed
th
at
the
use
r la
st
acc
ess
ed
in s
yste
m
Pa
tie
nt
care
d f
or
by
no
n-E
D
xx
xx
OB
SB
RD
or
INP
TB
RD
tea
m (b
oa
rdin
g o
r d
isp
laye
d in
a b
lue
lab
el
ad
mit
ted
) in
dic
ate
s b
elo
w t
he
be
d n
am
e
pa
tie
nt
no
lon
ge
r in
ca
re
AD
MT
or
INP
T
of
ED
ph
ysic
ian
dis
pla
yed
inst
ea
d o
f
att
en
din
g p
hys
icia
n
na
me
Act
ion
ab
le o
r
Ho
ve
r ca
teg
ori
es
ap
ply
on
ly t
o A
DM
T o
r IN
PT
Pa
tie
nt
info
rma
tio
n c
alle
d
xx
xP
ho
ne
ico
n
in b
y p
rim
ary
ph
ysic
ian
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

Emergency Department Status Boards in Transition 51
Tri
ag
e a
cuit
yx
xB
ed
ce
ll w
as
red
ora
ng
e
yello
w g
ree
n b
lue
or
gra
y (i
f n
o a
cuit
y
sele
cte
d)
Typ
e o
f co
mm
en
tx
ba
rx
Re
d g
ree
n y
ello
w p
urp
le
gra
y b
lue
co
lore
d b
ar
to le
ft o
f co
mm
en
t ce
ll
(co
rre
spo
nd
ing
to
typ
e
of
com
me
nt)
on
ly if
th
e
mo
st r
ece
nt
com
me
nt
an
d it
wa
s p
ick-
sele
cte
d
Use
rna
me
of
seco
nd
x
xx
x
ass
ign
ed
nu
rse
Vit
al s
ign
info
rma
tio
n
xx
xx
Lett
er
V is
co
lore
d r
ed
is a
va
ilab
le o
n
yello
w o
r b
lue
co
lor
oth
er
scre
en
de
pe
nd
s o
n v
alu
es
Zo
ne
s fo
r p
rov
ide
r x
x
ass
ign
me
nt
to p
ati
en
ts
Ass
ign
ed
be
d a
rea
an
d
xx
xx
xx
roo
m n
um
be
r (E
)
roo
m n
um
be
r (M
)
Ca
re P
lan
Ord
ers
x
xx
xx
xx
xx
xx
Co
lor-
cod
ed
nu
mb
ers
(E)
Dis
po
siti
on
(se
e
ma
gn
eti
c cl
ips
ho
ldin
g
Ta
ble
4 f
or
de
tails
)p
ap
er
EK
G f
or
ph
ysic
al
ha
nd
off
of
rep
ort
s o
r
pa
tie
nt
na
me
sti
cke
rs
tap
ed
on
EK
G
stic
kers
(M)
Ch
ief
com
pla
int
xx
xx
xx
info
rma
tio
n (s
ee
Ta
ble
2 f
or
ad
dit
ion
al d
eta
ils)
Co
nti
nu
ed n
ext p
ag
e
52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

52 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
1 (
con
tin
ue
d)
Ma
nu
al S
yst
em
Ele
ctro
nic
Sy
ste
m
Info
rma
tio
n T
ype
an
d
Ad
dit
ion
al N
ote
s
De
scri
pti
on
or
Co
lor
Fo
nt
Use
Pa
tie
ntrsquo
s a
ge
xx
xx
xx
Pa
tie
ntrsquo
s g
en
de
rx
xx
xx
xT
he
lett
er
F M
O o
r U
(fe
ma
le m
ale
oth
er
un
kno
wn
) (E
) t
he
sym
bo
ls f
or
ma
le o
r
fem
ale
(M)
Pa
tie
ntrsquo
s fu
ll n
am
e (E
)
xx
xx
xx
pa
tie
ntrsquo
s la
st n
am
e a
nd
som
e f
irst
na
me
s (M
)
Ro
om
se
t u
p f
or
pe
dia
tric
sx
xx
xx
Ro
om
na
me
(E) o
r re
d b
ox
aro
un
d r
ow
s (M
)
Ro
om
sta
te (E
MP
TY
x
xx
xx
xx
Ro
w is
pa
le y
ello
w (E
)
HO
USE
KEE
PIN
G
wo
rds
line
run
acr
oss
th
e
Ne
ed
s B
ed
)co
lum
ns
for
the
ro
w (M
)
Sa
me
na
me
ale
rtx
xx
xx
Ico
n (E
) or
ma
gn
et
(M)
Use
rna
me
(E) o
r fi
rst
na
me
x
xx
xx
xx
cod
e o
f th
e n
urs
e (M
)
Location Outside of Matrix Form
Marker (handwritten)
Magnet
Drawn Symbols
Automatically Filled
AlphanumericKBD Symbol
Typed
PickedSelected
AlphanumericKBD Symbol
StickiesNotepad
Icons
Other
Actionable
Hover
Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

Emergency Department Status Boards in Transition 53
Use
rna
me
(E) o
r in
itia
ls o
f x
xx
xx
xx
xU
sern
am
e b
old
(E)
add
itio
nal
pre
vio
us
ldquoph
anto
mrdquo
colu
mn
wit
h
att
en
din
g a
ssig
ne
dse
con
d s
et
of
init
ials
in
na
me
co
lum
n (M
)
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
ssig
ne
d
resi
de
nt
ph
ysic
ian
Use
rna
me
(E) o
r in
itia
ls
xx
xx
xx
x
sym
bo
ls o
f th
e a
tte
nd
ing
ph
ysic
ian
(M)
Use
rna
me
(E) o
r th
e in
itia
ls
xx
xx
x
sym
bo
l (M
) of
ass
ign
ed
me
dic
al s
tud
en
t
Zo
ne
fo
r n
urs
e a
ssig
nm
en
t x
xx
xC
olo
r o
r Z
p
ort
ion
of
the
to p
ati
en
tsb
ed
ass
ign
me
nt
ie
ldquoSO
UT
H B
lue
51
rdquo o
r
ldquoWE
ST
08
R-(
Z3
)rdquo (E
)
gre
en
lin
es
sep
ara
tin
g
the
be
ds
into
zo
ne
s (M
)
No
tes
ldquoPic
ked
se
lect
ed
rdquo in
dic
ate
s th
at
en
trie
s co
uld
be
pic
ked
an
d s
ele
cte
d w
ith
th
e m
ou
sek
eyb
oa
rd ldquo
Sti
ckie
sn
ote
pa
drdquo
refe
rs t
o a
n ic
on
on
th
e e
lect
ron
ic
bo
ard
th
at
led
to
ad
dit
ion
al d
ata
ldquoA
ctio
na
ble
rdquo m
ea
ns
tha
t th
e e
ntr
y co
uld
be
clic
ked
or
sele
cte
d f
or
furt
he
r d
ata
en
try
or
info
rma
tio
n ldquo
Ho
ve
rrdquo m
ea
ns
tha
t a
dd
itio
na
l
info
rma
tio
n w
as
av
aila
ble
if t
he
mo
use
ho
ve
red
ov
er
pa
rt o
f th
e e
ntr
y S
ha
de
d c
ells
ind
ica
te t
ha
t th
e e
ntr
y w
as
no
t fo
un
d f
or
tha
t ty
pe
of
tech
no
log
y
On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

On the electronic board colors were associated with a variety of automatedflags or alerts For instance the background of the room number was color-codedto indicate triage acuity (the medical urgency of the chief complaint) and smallcolored bars (adjacent to the cell borders) were used to show that particular com-ment types had been entered that particular chief complaints were entered orthat some additional information screens had been accessed
The electronic system provided additional functionality in the form of items orentire cells that could be hovered over or clicked Of the 18 cells or items that hadhover capabilities only 9 provided additional relevant details including the fullnames of caregivers a link to additional patient details the categories for length-of-stay warnings (eg long gt 6 hr) definitions of codes in the Custom columnand values for patient vital signs The remaining 9 either provided the name of acolor associated with an icon (eg ldquoredrdquo when the mouse hovered over a red bar)or a text label for an icon or symbol (eg ldquoName Alertrdquo for the name alert icon)Additionally 19 items could be selected Clicking the items either selected thepatient (8 instances) provided a link to another screen with additional details (5instances) caused a care provider to be assigned or another screen to displaydepending on the situation (5 instances) or caused the same name alert to beremoved (1 instance) (Note that counts from Table 1 are higher because multipleitems in cells with hoverclick capabilities may be listed separately if they pro-vided different types of information)
Chief Complaint AnalysesA primary function of both the manual and electronic whiteboards is to provide
information about the reasons for a patientrsquos visit to the emergency department (chiefcomplaints) Chief complaints are provided by patients to triage nurses during thetriage process In the manual system a coordinating ED nurse (the charge nurse)copied the chief complaint information from the triage nursersquos chief complaint fieldon the paper chart onto the ED whiteboard at the time the patient was brought fromtriage to the ED treatment area In the electronic system the triage nurse entered thechief complaint into the patient-tracking display directly and this information wasautomatically displayed when the patient was moved to the treatment area
We analyzed several aspects of the chief complaints entered in both systemstheir syntactic variability the functional content of the information provided inthe chief complaint field of the status board and the degree to which differentinformation types were represented across the two types of systems
Chief Complaint Syntactic Analysis Both the manual and electronic status boardsallow entries to be written as free text Additionally the electronic system had anautocomplete feature that provided suggested text (standard chief complaints)based on the beginning characters that were typed To understand the degree towhich chief complaint entries were identical to standard chief complaints differedbecause of abbreviations or typographical errors or differed because of the con-tent of information presented we analyzed the words and syntax used to enterchief complaint information Chief complaint entries were inspected to identify
54 Journal of Cognitive Engineering and Decision Making Spring 2010
(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

(a) identical versus unique entries (b) entries that are clinically identical exceptfor syntactic variations (eg abbreviations) and (c) chief complaints that repre-sented a general type of problem with some additional information or modifierFor example ldquoChest painrdquo ldquoCHEST PAINrdquo ldquoCHST PNrdquo and ldquoCHST Pain wSOBrdquo arefour original entries in the chief complaint column Here the words chest pain arewritten in three syntactically different ways The fourth entry adds a qualifier (ldquowithshortness of breathrdquo) but refers to the same general category of complaint (ldquochestpainrdquo) Thus there are four original entries two variations (chest pain and chestpain with shortness of breath) and one general chief complaint (ldquochest painrdquo)
As seen in Table 2 there were more unique chief complaints per patient forthe manual than for the electronic system Per-patient ratios were similar whensyntactic variations (abbreviations fonts spellings) were removed These entriescorresponded to 06 general chief complaints per patient for the manual and 045entries per patient for the electronic system Thus across all three measures therewere 14 times as many unique entries per patient in the manual versus the elec-tronic system 15 times as many entries controlled for syntactic variation and 13times as many general chief complaints in the manual system compared to theelectronic system That is the variability appeared to be caused by actual differ-ences in the presenting conditions of the patients (general chief complaints) ratherthan the manner (manual or typing) in which information was entered
One might have expected that the presence of the autocomplete feature wouldhave resulted in greater consistency in entries in the electronic as opposed to themanual system However the similarity across these ratios indicates that the elec-tronic whiteboard did not seem to provide greater control or enforce greater con-sistency in entries than did the manual board This interpretation is substantiatedby an additional analysis that was performed regarding the degree to which entriesin the electronic board could have been generated using autocomplete Only 45of entries were identical to autocomplete entries indicating that in more than halfthe cases nurses were overriding the autocomplete function to enter free text(Note that this percentage represents an upper bound It is possible that stafftyped in text that was identical to autocomplete text)
Chief Complaint Content Analysis Content analysis of the chief complaint fieldsrevealed a rich array of functional information types presented as a chief complaint
Emergency Department Status Boards in Transition 55
TABLE 2 Syntax Analysis of Chief Complaint Entries
Frequency Rate Per Patient
Manual Electronic
Manual Electronic (105 Patients) (80 Patients)
Syntactically unique entries 108 58 103 073
Identical entries syntax variations excluded 105 52 100 065
General complaint categories 63 36 060 045
In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

In addition to patient-reported symptoms and their location on the body the chiefcomplaint field included information such as past medical history hypothesizeddiagnoses and the mechanism of injury (eg motor vehicle accident) Fourteen cat-egories were identified (see Table 3 for definitions and examples) For the most partthese categories were represented in both the manual and electronic systems how-ever the frequency of representation indicated differences As indicated in Table 3ED staff were 26 times as likely (on a per-patient basis) to note ldquosignsrdquo (informationthat could be measured through tests or observation such as heart rate) in the man-ual compared with the electronic board twice as likely to note a presumed diag-noses 18 times as likely to note the mechanism of injury and twice as likely toindicate medical history information on the manual board
In contrast complaints on the electronic board were more likely to include infor-mation regarding patient-reported symptoms In several cases categories of informa-tion present in the manual board chief complaint field were not represented in thatfield on the electronic board This may reflect a subtle difference between normativeand empirical uses of the concept of chief complaint between work as imagined andwork as performed Normatively the chief complaint has been considered to be thepatientrsquos actual words (eg ldquofeeling weakrdquo) hence the predominance of symptoms inthe pick-lists and autocomplete lists of the electronic system But empirically clini-cians commonly capture not the patientrsquos exact words but their interpretive catego-rization of the patientrsquos problem (eg ldquotachycardiardquo) hence the increased prevalenceof diagnoses and signs in manual status board and free-text entries
Finally we analyzed the degree of change in the chief complaint entries over timeA higher percentage of whiteboard patients (95) showed changes made to the chiefcomplaint field during the course of the patientrsquos stay (additional details clarifica-tions or treatmentdisposition-related information) compared with only 00125 ofpatients in the electronic case This finding suggests that the chief complaint portionof the whiteboard was used more dynamically in the manual case
Workflow-Related Field AnalysisSimilar content analyses were performed for columns related to workflow and
patient care We selected columns to compare across systems with similar func-tions for the ED staff such as providing information about plans for patient treat-ment during the ED stay needs for tests or transportation to other hospital areasor plans for discharge or hospital admission On the manual board we analyzedentries from the Disposition column along with the Diet column (in which therewere only a few entries) For example during a patientrsquos stay in the ED caregiverscould add or change information in the Disposition column to indicate that a testwas needed (eg write ldquoEKGrdquo followed by a small square checkbox) indicate thetest was completed (put a check in the box) and indicate that a consulting physi-cian had been called
On the electronic board we analyzed entries in the Comments column (whichaccepted free text as well as click-and-select phrases) the Disposition column(which provided an alphanumeric code indicating the patientrsquos disposition such
56 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

Emergency Department Status Boards in Transition 57
TA
BLE
3 C
ate
go
rie
s o
f C
hie
f C
om
pla
ints
an
d T
he
ir F
req
ue
ncy
Acr
oss
Dif
fere
nt
Te
chn
olo
gie
s
Fre
qu
en
cyR
ate
Pe
r P
ati
en
t
Ma
nu
al
Ele
ctro
nic
M
an
Ra
te
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lE
lect
(1
08
Pa
tie
nts
)(8
0 P
ati
en
ts)
Ele
c R
ate
Ale
rtS
pe
cia
l ale
rts
to c
are
giv
ers
(eg
ldquoL
AT
EX
rdquo2
00
02
00
0ndash
alle
rgie
s)
Arr
iva
l mo
de
Me
cha
nis
m o
f a
rriv
al t
o t
he
ED
ldquoME
RT
rdquo (i
n-h
osp
ita
l te
am
)2
00
02
00
0ndash
ED
Co
ord
ina
tio
nW
ork
re
qu
est
s m
ov
em
en
t
ldquoAD
MIT
TE
Drdquo(
ad
mit
ted
to
ho
spit
al)
2
00
02
00
0ndash
dis
po
siti
on
pla
ns
ldquoEK
Grdquo
(pa
tie
nt
ne
ed
s a
n E
KG
)
De
sire
d v
isit
ou
tco
me
Vis
it is
pla
nn
ed
an
d e
xpre
sse
d a
s ldquoS
titc
h r
em
ov
alrdquo
ldquoN
ee
ds
Rx
Re
fillrdquo
52
00
50
03
16
7
an
ou
tco
me
Late
ralit
y D
esc
rip
tio
n o
f si
de
of
bo
dy
limb
ldquoL
Sh
ou
lde
r In
jrdquo (L
eft
sh
ou
lde
r in
jury
)1
07
00
90
09
1
aff
ect
ed
Loca
tio
nD
esc
rip
tio
n o
f b
od
y p
art
aff
ect
ed
ldquoBa
ck H
ip P
ain
rdquo ldquo
fla
nk
pa
inrdquo
64
51
05
90
64
09
2
Me
cha
nis
m o
f in
jury
De
scri
pti
on
of
ho
w t
he
inju
ry(i
es)
ldquoF
allrdquo
ldquoM
VC
rdquo (M
oto
r v
eh
icle
cra
sh)
17
70
16
00
91
78
occ
urr
ed
Me
dic
al h
isto
ryIn
form
ati
on
re
ga
rdin
g p
ast
ldquo2
m p
-de
live
ryrdquo
(2 m
on
ths
21
00
20
01
20
0
me
dic
al h
isto
ry (o
fte
n q
ua
lifyi
ng
p
ost
-de
live
ry)
a s
ymp
tom
or
dia
gn
osi
s)
Pe
rtin
en
t in
dic
ato
rsP
osi
tiv
e o
r n
eg
ati
ve
ind
ica
tors
th
at
ldquondash L
OC
rdquo (n
o lo
ss o
f co
nsc
iou
sne
ss)
15
00
10
06
01
7
are
re
lev
an
t to
a d
iag
no
ses
Pre
sum
ed
dia
gn
ose
sP
resu
me
d c
au
se o
f p
ati
en
t p
rob
lem
ldquoAst
hm
ardquo
ldquoK
idn
ey
Sto
ne
rdquo1
97
01
80
09
2
Pri
ma
ry s
ymp
tom
Co
mp
lain
t d
esc
rib
ed
by
pa
tie
nt
ldquoCh
est
pa
inrdquo
ldquoS
ho
rtn
ess
of
Bre
ath
rdquo4
84
80
44
06
00
73
Pro
ble
m
Ge
ne
ral d
esc
rip
tio
n o
f p
rob
lem
ldquoAn
kle
inju
ryrdquo
ldquoD
en
tal p
rob
lem
rdquo1
06
00
90
08
11
3
Ru
le o
ut
dia
gn
ose
sP
oss
ible
dia
gn
ose
s th
at
sho
uld
be
ldquoR
O M
Irdquo (r
ule
ou
t h
ea
rt a
tta
ck)
ldquoR
O
77
00
60
09
06
7
rule
d o
ut
(oft
en
a s
et
of
PN
Ardquo
(ru
le o
ut
pn
eu
mo
nia
)
dif
fere
nti
al d
iag
no
ses)
Sig
ns
Info
rma
tio
n g
ath
ere
d t
hro
ug
h
ldquoBlo
od
y S
too
lrdquo ldquo
Incr
ea
sed
he
art
ra
terdquo
39
11
03
60
14
25
7
ob
serv
ati
on
su
ch a
s la
b v
alu
es
vit
al s
ign
s o
r cl
inic
al o
bse
rva
tio
ns
as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

as admission to the hospital transfer to another hospital or discharge home) anda custom area displaying colored dots with numeric labels (ldquocustom codesrdquo) cor-responding to a wide variety of orders or qualifying information regarding thepatient (eg number of visitors allowed requests for EKGs communications regard-ing admissions potential security concerns)
Note that the software allowed definitions of the custom codes to be configuredby individual hospitals however the format of the codes (numbered dots) wasfixed Often codes in the custom area duplicated information in the Disposition orthe Comments column however because these could be entered independently(by different staff) and because some staff may have relied on information in onecolumn whereas other staff relied on another all entries were coded and countedseparately Similar to the manual system caregivers could enter information in thecomments area (eg indicate the need for an EKG and its completion) or selectcustom codes Because of space restrictions only the three most recent commentsappeared on the primary screen (and thus were analyzed) also comments werelimited to a set character length Information in the Disposition column appearedautomatically when other aspects of the patientsrsquo record was changed
As with the chief complaints column content analysis of the dispositioncom-ments fields indicated that these areas of both the manual and electronic boardswere used to support a variety of functions including those related to the careplans for the patient and the status of those plans with respect to processes of hos-pital admission and discharge (see Table 4) In both systems for some patientsinformation had not yet been entered into these fields Thus these data wereavailable for 62 patients in the manual case and 68 in the electronic case
Across both systems 17 functional categories of information were identified(12 for manual 16 for electronic) Although both systems were used to representa wide range of information the usage patterns were very different across the twosystems Compared with the electronic system (on a per-patient basis) the man-ual system showed 575 times more information regarding the hospital service towhich the patient would be admitted 26 times the information regarding the sta-tus of the admission process 24 times the information regarding consult requests19 times as much information regarding progress through the patientsrsquo clinicalworkup plan 15 times as much information regarding the clinical care plan itselfand approximately the same amount of information regarding patient movementto new beds within the ED
In contrast the electronic board showed more information regarding transportrequests and diet (with no entries in the manual board for transport and only oneentry for diet) 49 times the information regarding the status of in-patient beds foradmitted patients and almost 3 times the entries regarding disposition Most of thedisposition information on the electronic board was communicated through theCustom and Disposition columns (colored alphanumeric codes) rather thanthrough text entries shown in the Comments column In fact the manual boardhad five times as many disposition comments (text entries in the column) perpatient compared with the text comments area of the electronic board
58 Journal of Cognitive Engineering and Decision Making Spring 2010
Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

Emergency Department Status Boards in Transition 59
TA
BLE
4 C
ate
go
rie
s o
f D
isp
osi
tio
nC
om
me
nts
Info
rma
tio
n a
nd
Th
eir
Fre
qu
en
cy A
cro
ss D
iffe
ren
t T
ech
no
log
ies
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Ad
dit
ion
al
Pa
tie
nt
ha
s sp
eci
fic
Re
pre
sen
ted
by
a
00
02
20
00
00
30
00
info
rma
tio
n
pro
toco
ls o
n f
ile
ldquono
tep
ad
rdquo ic
on
(eg
ty
pe
s o
f
me
dic
ati
on
to
be
giv
en
)
Ad
mis
sio
n
Sta
tus
wh
en
pa
tie
nt
ldquoAd
mit
HM
Urdquo
rdquoAd
mit
5
13
31
62
20
82
03
22
56
pro
cess
g
oe
s th
rou
gh
m
ed
icin
erdquo
sta
tus
ad
mis
sio
n p
roce
ss
Ale
rtS
pe
cia
l ale
rts
to
ldquoHip
pa
filt
er
resp
pre
crdquo
00
03
30
00
00
40
00
care
giv
ers
(ne
ed
s sp
eci
al
resp
ira
tor)
Be
d
Sta
tus
of
the
ED
be
d
ldquo6R
wh
en
cle
an
ed
rdquo0
00
11
00
00
01
00
0
sta
tus
ED
ass
ign
ed
Be
d s
tatu
s
Sta
tus
of
the
po
ten
tia
l ldquo5
14
RE
AD
Yrdquo
(be
d
33
58
16
00
50
24
02
1
Inp
ati
en
tin
pa
tie
nt
ass
ign
ed
is
re
ad
y o
n in
pa
tie
nt
un
it 5
14
) ldquo
Aw
ait
ing
be
d a
ssig
nm
en
trdquo
Clin
ica
l C
linic
al d
eta
ils o
f ldquoC
T N
eck
rdquo ldquo
MR
I1
93
0rdquo
95
39
03
27
11
53
10
41
47
wo
rku
p
pla
nn
ed
lab
s
(pa
tie
nt
sch
ed
ule
d
pla
nim
ag
ing
te
sts
fo
r M
RI a
t 6
30
PM
)
me
dic
ati
on
s r
eq
ue
sts
or
rem
ind
ers
fo
r
act
ivit
ies
fo
llow
-up
s
Co
nsu
lt
Co
nsu
lt s
pe
cia
lists
wh
o
ldquoNE
UR
Ordquo
(Ne
uro
log
y 1
50
07
70
24
01
02
40
req
ue
sth
av
e b
ee
n a
ske
d t
o
con
sult
re
qu
est
ed
)
ev
alu
ate
pa
tie
nt
in t
he
ED
Co
nti
nu
ed n
ext p
ag
e
60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

60 Journal of Cognitive Engineering and Decision Making Spring 2010
TA
BLE
4 (
con
tin
ue
d)
Fre
qu
en
cy
Ra
te p
er
Pa
tie
nt
To
tal
Ma
nu
al
Ele
ctro
nic
M
an
ua
l
Typ
eD
efi
nit
ion
Exa
mp
leM
an
ua
lC
ust
om
Dis
po
siti
on
Co
mm
en
tsE
lect
ron
ic(6
2 P
ati
en
ts)
(68
Pa
tie
nts
)E
lect
ron
ic
Die
tP
ati
en
t-sp
eci
fic
die
t ldquoD
iet-
LOW
SO
DIU
Mrdquo
10
02
42
40
02
03
50
06
inst
ruct
ion
s D
isp
osi
tio
nD
isp
osi
tio
n in
stru
ctio
ns
ldquoAd
mit
ted
rdquo
28
28
57
59
00
45
13
20
34
aft
er
ED
tre
atm
en
t ldquoD
isch
arg
e
com
ple
tio
nco
mp
lete
rdquoE
mp
ha
sis
Use
of
spe
cia
l ch
ara
cte
rs
ldquoMia
mi-
J C
olla
r D
Crdquo
10
00
00
02
00
0-
to e
mp
ha
size
att
en
tio
n
to in
form
ati
on
Oth
er
Po
ssib
le lo
cati
on
of
ldquoOp
tho
Clin
icrdquo
00
03
03
00
00
04
40
00
pa
tie
nt
pa
tie
nt
oth
er
tha
n
(op
tho
mo
log
y cl
inic
)
loca
tio
na
ssig
ne
d E
D b
ed
ldquoTra
nsp
ort
Xra
yrdquoP
lan
P
rog
ress
th
rou
gh
C
T S
can
(wit
h a
1
09
42
31
96
41
76
09
41
87
pro
gre
sscl
inic
al w
ork
up
pla
nh
an
d-d
raw
n c
he
ckb
ox)
ldquol
ab
s d
on
e a
t 7
30
rdquoP
lan
ne
d
Be
d n
um
be
r o
r a
rea
ldquoE
ast
21
rdquordquo1
2Lrdquo
90
64
10
01
50
15
10
0b
ed
p
ati
en
t is
ass
ign
ed
a
ssig
nm
en
tto
mo
ve
to
wit
hin
ED
Se
rvic
eD
eta
ils o
n h
osp
ita
l ldquoa
dm
it O
BS
rdquo ldquo
ad
mit
pcp
rdquo1
40
03
30
23
00
45
75
gro
up
th
at
will
ca
re
for
pa
tie
nt
up
on
a
dm
issi
on
Te
am
De
tails
fo
r ca
reg
ive
r ldquoN
P 1
69
2 6
-14
NP
rdquo (n
urs
e
10
50
50
02
00
70
29
tea
m c
oo
rdin
ati
on
pra
ctit
ion
er
tea
m
fro
m u
nit
6-1
4 a
va
ilab
le
via
pa
ge
r n
um
be
r 1
69
2)
Te
st r
esu
lts
Lab
an
d t
est
re
sult
s ldquoI
NR
gt 1
25
K 2
9rdquo
40
01
10
06
00
16
00
(blo
od
te
st r
esu
lts)
Tra
nsp
ort
P
ati
en
t is
re
ad
y to
be
ldquoT
ran
spo
rt C
Trdquo
00
03
03
00
00
04
40
00
req
ue
sts
tra
nsp
ort
ed
to
a
(pa
tie
nt
tra
nsp
ort
ed
te
st o
r p
roce
du
re
to C
T)
Cu
sto
m D
isp
osi
tio
n a
nd
Co
mm
en
ts e
ntr
ies
are
to
tale
d in
th
e T
ota
l Ele
ctro
nic
co
lum
n
Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

Discussion
These analyses demonstrate the changes in information content and usage thatcan occur as information systems shift in formmdashin this case from a manual pri-marily handwritten system to an electronic system with some automated capabili-ties We found that the set of categories and functions of information content weregenerally similar across the two technologies This was true in both the comprehen-sive analysis and the more detailed analysis of the chief complaint and dispositioncomments areas
There was an attempt to mimic the matrix form of the manual board in thedesign of the electronic display as well as to include similar fields or categories ofinformation However despite the attempt to mimic the surface feature of themanual system the nature of the two technologies differed The use of font (hand-written to typographic) color and symbols changed and there were additionalcolumns and the introduction of icons codes and color indicators that mightmake it more difficult for clinicians to find or understand the information presentAnnotations were also restricted to be entered in particular cells and in somecases they were limited to a set of prespecified options These changes reducedthe flexibility with which the system could be adapted to situational demandsAdditionally the means of interaction was fundamentally different Instead ofdirect freehand input with a marker clinicians had to find an unused terminallog in and type or select inputs
Thus despite the similarities in the surface form of the two technologies therewere differences in their underlying capabilities These differences were reflectedin the analyses performed which revealed important changes in the use of the sys-tem that have the potential to affect work in the emergency department In partic-ular the electronic system did not on the primary and most directly accessibledisplay provide a resource for clinicians to track their individual workflowPhysicians could no longer use symbols to serve as reminders to themselves and oth-ers of the status of the standard sequence of patient interactions (eg hearing abouta case from a trainee meeting and evaluating a patient and completing the patientrsquoschart) In fact as noted during an observational phase of our research (Pennathuret al 2007) some physicians started making notes to track their patient tasksafter the manual system was replaced by the electronic system Because these werepersonal notes often carried in the physiciansrsquo pockets they were not visible to otherstaff This ldquotask-tailoringrdquo (Cook amp Woods 1996) essentially reduced the poten-tial for implicit communication and task coordination among care providers becausepreviously public information was now private The use of manual ED statusboards to document this process has been noted in multiple ED settings (Wears ampPerry 2007) so this absence in the electronic system is likely to have an effect onwork across a range of EDs
Additionally we found that ED staff had exploited the flexibility inherent inthe manual whiteboard to add information outside the structured row-columnformat There were notations in the margins phantom columns added to the left
Emergency Department Status Boards in Transition 61
of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

of the first column and symbols drawn across multiple rows or columns Theseannotations represent adaptations of the technology to meet demands that werenot anticipated at the time the original display was constructed
The shift to electronic technology has fundamentally limited practitionersrsquo abil-ity to change the functionality of the information system in response to moment-to-moment or more general shifts in circumstances The electronic system did allowsome customization Providers could sort rows or individually shuffle hide or dis-play columns however desires for new columns could be met only through oftencostly and time-consuming software changes (if approved at all) and ad hoc nota-tions outside of the matrix format were impossible
A third overall change was the ability of the electronic system to automaticallyhighlight or fill in information Small colored bars cell color and font were usedto indicate or call attention to a variety of situations including prolonged lengthof stay or high-risk chief complaints Providing automatic alerts or indicators canimprove workload and safety if the indicators are meaningful and are carefullychosen to correspond to critical situations However the ease with which colorcoding symbols and font changes can be added to software may result in a prolif-eration of these alerts screen clutter and confusion
For instance on the studied displays a small vertical green bar on the edge of acell could indicate that a comment regarding patient transport is the most recentlyadded comment that the chief complaint requires special attention because aspectsare tracked to measure quality or that a specific detail screen has been accesseddepending on the column Note also that in addition to the one-to-many mappingof color to meaning the color coding did not correspond to known populationstereotypes (eg green to indicate ldquostartrdquo ldquosaferdquo or ldquoacceptable valuerdquo) Additionallycolor was not consistently used to indicate critical information or events (egcolor bars indicating a patient transport comment)
The analysis of chief complaint entry syntax indicated that there was not agreat deal of difference in the variability with which chief complaints were repre-sented in both systems variability was driven both by the presenting conditionsof the patients and differences in how those conditions were entered This issomewhat surprising because the electronic system included an autocompletefeature for the chief complaint field but only 45 of entries could have resultedfrom use of this feature Although standardizing entries may be an administrativegoal (eg to measure time for certain conditions to be treated) the staff did notuse the system in this way perhaps because they needed more flexibility than theautocomplete provided because of the cognitive effort to switch from typing tomonitoring and selecting the autocomplete entry (Higginbotham Bisantz SunmAdams amp Yik 2009 Koester amp Levine 1998) or because completion of auto-complete required using the mouse
For both areas we studied similar information categories were represented inboth technologies but with different frequencies For the chief complaint fieldthere was less variety in entry types in the electronic system For example entriesin the electronic system focused more on patient-reported symptoms (perhaps
62 Journal of Cognitive Engineering and Decision Making Spring 2010
because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

because autoentry data are almost exclusively symptoms) and less on other cate-gories of information such as potential diagnoses or mechanisms of injury Someimportant information was missing on the electronic displays For instance in themanual system nurses would signify allergies (particularly those that wouldlikely affect care for the condition being treated) in the chief complaint columnAllergy alerts were not shown on the primary electronic display but instead werelisted as part of a different patient information screen Thus critical informationrelevant to the patient condition at hand was no longer presented
Additionally we noted that the chief complaint information was changed moreoften in the manual compared with the electronic system Perhaps this was because itwas straightforward for staff to add or change information about the patientrsquos statuson the manual board as their understanding of the problem evolved whereas thefunction to change this field in the electronic system is easily accessed only during thetriage phase These results point to a reduction in the ability of the new system torepresent a range of informationmdashincluding critical safety informationmdashregardingpatient states including situations when more information is obtained
The differences in the dispositioncomments category frequencies as well asthe change to how physicians tracked their own work point to a dramatic changein the nature of the use of the status board In particular our results suggest thatthere was a shift from the board serving as a primary tool for clinical staff to com-municate coordinate and track aspects of medical care (eg the care plan planstatus admission status) to a tool used by other staff to communicate and tracksupport functions (eg transporting patients or delivering meals)
Importantly these changes were not driven by a wholesale change in the func-tions that were available in the new technology as we documented generally simi-lar capabilities in the two technologies Instead the changes in use seem to haveresulted from a combination of more subtle factors including the means of inter-action level of flexibility changes in information display format and loss of a fewkey functions For instance limited space was available for free-text entry in theelectronic system (only the three most recent comments could be displayed on themain display older comments had to be accessed on a different view) Entries onthe electronic system were restricted to text and keyboard symbols compared withthe ability to create customized lists figures and check boxes on the manualboard These changes combined with the loss of provider workflow-tracking capa-bility and the time it took to log in and enter text compared with freehand writingcould have shifted the use away from clinical planning and communication
Design ImplicationsThe results from this analysis point to a number of implications for the design of
information systems particularly those which are replacing existing technologiesFirst it is not sufficient to simply match the information fields available or the
overall format of the existing technology Having similar columns to or the samematrix formats as in the manual board was not sufficient to sustain current workpractices or to prevent unanticipated shifts in use
Emergency Department Status Boards in Transition 63
Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

Additionally support for tailorable andor flexible use that allows users toadapt the system as needs change in response to moment-by-moment demands orlonger-term changes is necessary In the case of the manual status boards the factthat information could be developed on the fly directly entered and flexibly dis-played supported the work Continued redesign of the manual artifact by theusers was supported by the fact that the manual whiteboard like the paper docu-ments described by Sellen and Harper (2003) afforded annotation and ldquotailorabil-ityrdquo Staff could write wherever they chose annotate the margins write acrosscolumns or rows or create new matrix elements (eg new columns) (For exam-ple in other observations of manual status board use we noted the invention andwidespread adoption of a new symbol indicating orders had been entered over arelatively short period)
Careful analyses are also required to identify all the important functions anddisplay features that must be supported as well as the effect of changing themethod of interaction with a system As noted earlier the loss or change of a fewkey functions (eg easy support of physician work flow customized lists andtracking of care plans) seemed to have shifted the use of the status board awayfrom clinical planning and communication The proliferation of automated col-ored alerts and codes also may have led to an information display that thoughdata dense did not clearly convey information supporting overall awareness ofthe ED or support planning and tracking activities related to a specific patientChanging the method of interaction from direct access to keyboard and terminal(combined with log-in requirements) also may have affected use by increasing thecost (in terms of time and effort) to enter annotate or change information
Limitations and Future ResearchAlthough the data analyzed in this study were drawn from one hospital
(potentially limiting the generalizability of the findings) the overall format infor-mation fields and typical uses of the status boards that we observed are consistentwith those documented in other EDs (Wears amp Perry 2007 Wears et al 2007)and other medical settings (Xiao 2005) To enhance generalizability data werecaptured in two different ED areas (running separate status boards) within thehospital Also the electronic status board we studied is the product of a nationalvendor of ED information systems with a large market share and is therefore rep-resentative of at least one type of commonly implemented system
In part to focus on the dynamic nature of information on the status boards(eg as seen in the changes to chief complaints) we collected data from 8-hr peri-ods rather than sampling across a longer time span It is possible that these peri-ods were idiosyncratic and thus not representative of the use of the status boardsgenerally Additionally we did not capture information about every patient treatedin the ED only those in the two largest adult treatment areas Also our data col-lection captured different numbers of patients across the two systems Howeverdata were not collected for either system during times of the year that were proneto known peak loads (eg summer trauma season or flu season) Finally data
64 Journal of Cognitive Engineering and Decision Making Spring 2010
were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

were collected on so-called typical days those with no unusual events (such as amass casualty incident) or unusual level of patient traffic either of which mighthave affected use of the boards
By focusing on only four periods we may have missed some instances ofinformation category use on one or the other of the systems because of the patientor care providers present Our analysis however did not indicate dramaticallydifferent uses between the two areas sampled for either the manual or the elec-tronic boards which would have indicated something out of the ordinary for oneof the periods or (given that the areas were staffed by different people) if differentstaff used the boards very differently
The analysis covered 185 patients across the two systems Future researchcould focus on changes in use of the status boards during critical incidents orcomparisons in usage of similar systems across different EDs
This analysis was limited to documenting aspects of the primary (patient list)view of the electronic status board This was chosen because it was the main overviewscreen displayed (on both desktop and large-screen monitors) and because it pro-vided the closest analogue to the manual status board Although this limited theextent to which we could evaluate all the implemented (and potential) functional-ity of the electronic system it is true that with both systems staff had access toinformation about patients through additional means such as paper charts andother hospital IT systems (eg radiology) An analysis of all these sources wasbeyond the scope of our study
We did not perform a usability evaluation of the electronic system (thoughsome of our findings are clearly related to issues that could be identified throughsuch an analysis such as the inconsistent use of color) A usability analysis of theelectronic system has been performed as part of a separate research effort (FairbanksGuarrera et al 2008 Fairbanks Karn et al 2008)
Conclusions
In conclusion this study examined in detail the type and frequency of infor-mation presented on two types on patient-tracking displays a manual whiteboardimplementation and a computerized implementation Although the format of theprimary electronic display was designed to be similar to the manual whiteboardand the categories of information that appeared in both systems were similar thefrequency with which types of information was present differed These changesrepresent a shift in use that was not explicitly anticipated or intended but thatreflects the underlying affordances of the two technologies
Designing supportive information technology goes beyond mimicking the sur-face features of current systems particularly when the affordances of those currentsystems differ substantially from those of the replacement technology (Sellen ampHarper 2003) The analysis performed here provides additional evidence thatmerely identifying the form and information fields present in a manual technologyis not sufficient input for design Cognitive engineering analyses (Bisantz amp Burns
Emergency Department Status Boards in Transition 65
2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

2008 Bisantz amp Roth 2008 Roth Patterson amp Mumaw 2002)mdashwhich focus onthe purposes processes and constraints of the ED work environment as well asthe goals activities and strategies of the various clinicians and staffmdashshould beperformed in order to identify the information and interactivity necessary to sup-port ED work
Acknowledgments
This study was supported in part by a grant from the Emergency MedicineFoundation of the American College of Emergency Physicians At the time of thestudy Rollin J Fairbanks was supported by a research training grant from theEmergency Medicine Patient Safety Foundation through the Society for AcademicEmergency Medicine
References
Aronsky D Jones I Lanaghan K amp Slovis C M (2008) Supporting patient care in theemergency department with a computerized whiteboard system Journal of the AmericanMedical Informatics Association 15 184ndash194
Aspden P Corrigan J M Wolcott J amp Erickson S M (Eds) (2004) Patient safety Achievinga new standard for care Washington DC National Academy Press
Berg M (1997) Rationalizing medical work Cambridge MIT PressBerg M (2004) Health information management Integrating information technology in health care
work London RoutledgeBisantz A M amp Burns C M (Eds) (2008) Applications of cognitive work analysis Boca Raton
FL CRC PressBisantz A M amp Ockerman J J (2002) Informing the evaluation and design of technology in
intentional work environments through a focus on artifacts and implicit theoriesInternational Journal of Human-Computer Studies 56 247ndash265
Bisantz A M amp Roth E M (2008) Analysis of cognitive work In D A Boehm-Davis (Ed)Reviews of human factors and ergonomics (Vol 3 pp 1ndash43) Santa Monica CA HumanFactors and Ergonomics Society
Button G amp Harper R H (1993) Taking the organization into account In G Button (Ed)Technology in working order Studies of work interaction and technology (pp 98ndash107) LondonRoutledge
Committee on Quality of Health Care in America (2001) Crossing the quality chasm A newhealth system for the 21st century Washington DC National Academy Press
Cook R I amp Woods D D (1996) Adapting to new technology in the operating room HumanFactors 38 593ndash613
Fairbanks R J Guarrera T K Karn K S Caplan S H Shah M N amp Wears R L (2008)Interface design characteristics of a popular emergency department information system InProceedings of the Human Factors and Ergonomics Society 52nd Annual Meeting (pp 778ndash782)Santa Monica CA Human Factors and Ergonomics Society
Fairbanks R J Karn K S Caplan S H Guarrera T K Shah M N amp Wears R L (2008)Use error hazards from a popular emergency department information system InProceedings of the Usability Professionalsrsquo Association 2008 International Conference [CD-ROM] Bloomingdale IL Usability Professionalsrsquo Association (UPA) Available fromhttpwwwupassocorgupa_storeconference_proceedings
66 Journal of Cognitive Engineering and Decision Making Spring 2010
Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

Glaser B amp Strauss A L (1967) The discovery of grounded theory Strategies for qualitativeresearch Chicago Aldine
Higginbotham D J Bisantz A M Sunm M Adams K amp Yik F (2009) The effect of con-text priming and task type on augmentative communication performance Augmentativeand Alternative Communication 25 19ndash31
Hutchins E (1997) Cognition in the wild Cambridge MIT PressKoester H H amp Levine S P (1998) Model simulations of user performance with word pre-
diction Augmentative and Alternative Communication 14 25ndash36Kohn L T Corrigan J M amp Donaldson M S (Eds) (1999) To err is human Building a safer
health system Washington DC National Academy PressLaxmisan A Hakimzada F Sayan O Green R amp Patel Z (2007) The multitasking clini-
cian Decision-making and cognitive demand during and after team handoffs in emergencycare International Journal of Medical Informatics 76 801ndash811
Mackay W E (1999) Is paper safer The role of paper flight strips in air traffic control ACMTransactions on Computer-Human Interaction 6 311ndash340
Nemeth C P OrsquoConnor M Nunnally M amp Cook R I (2007) Re-presenting reality Thehuman factors of heath care information In P Carayon (Ed) Handbook of human factorsand ergonomics in health care and patient safety (pp 439ndash455) Mahwah NJ Erlbaum
Pennathur P Bisantz A M Fairbanks R J Perry S Zwemer F amp Wears R L (2007)Assessing the impact of computerization on work practice Information technology in emer-gency departments In Proceedings of the Human Factors and Ergonomics Society 51st AnnualMeeting (pp 377ndash381) Santa Monica CA Human Factors and Ergonomics Society
Poon E Jha A Christino M Honour M Fernanopulle R Middleton B Newhouse JLeape L Bates D W Blumenthal D amp Kaushal R (2006) Assessing the level of healthcareinformation technology adoption in the United States A snapshot BMC Medical Informaticsand Decision Making 6 Retrieved December 23 2009 from httpwwwncbinlmnihgovpmcarticlesPMC1343543
Roth E M Patterson E S amp Mumaw R J (2002) Cognitive engineering Issues in user-centeredsystem design In J J Marciniak (Ed) Encyclopedia of software engineering (2nd ed pp163ndash179) New York Wiley
Sachs P (1995) Transforming work Collaboration learning and design Communications of theACM 38 37ndash44
Sellen A J amp Harper R H R (2003) The myth of the paperless office Cambridge MIT PressWears R L amp Perry S (2007) Status boards in accident and emergency departments Support
for shared cognition Theoretical Issues in Ergonomics Science 8 371ndash380Wears R L Perry S J Wilson S Galliers J amp Fone J (2007) Emergency department status
boards User-evolved artefacts for inter- and intra-group coordination Cognition Technologyand Work 9 163ndash170
Xiao Y (2005) Artifacts and collaborative work in healthcare Methodological theoretical andtechnological implications of the tangible Journal of Biomedical Informatics 38 26ndash33
Ann M Bisantz PhD is an associate professor of industrial and systems engineering at the
University at Buffalo The State University of New York Her research interests are in cognitive
engineering methods complex decision making and interface design in domains such as
health care and defense
Priyadarshini R Pennathur is a doctoral candidate in industrial and systems engineering at
the University at Buffalo She holds a bachelorrsquos and masterrsquos degree in computer science
and a masterrsquos in industrial engineering Her research interests are in understanding cogni-
tive artifacts and information transformation in work systems She has been involved in
Emergency Department Status Boards in Transition 67
projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010

projects for designing and testing emergency department interfaces through simulation
techniques
Theresa K Guarrera is a doctoral student in industrial and systems engineering at the
University at Buffalo and a health project coordinator for the University of Rochester
Emergency Department Theresa has a BS degree in biomedical engineering Her research
includes evaluating patient-tracking systems used in the emergency setting for design and
usability purposes as well as considering interfaces between emergency medicine and radi-
ology imaging
Rollin J (Terry) Fairbanks MD MS is assistant professor of emergency medicine and of
community and preventive medicine at the University of Rochester He is also adjunct assis-
tant professor of industrial and systems engineering at the University at Buffalo His research
focuses on applying human factors engineering research techniques to the health care
domain His clinical practice is in the adult and pediatric emergency departments at the
University of Rochester Medical CenterStrong Memorial Hospital in Rochester New York
Shawna J Perry MD is director for Patient Safety System Engineering at Virginia
Commonwealth University Health Systems in Richmond Virginia and associate professor
associate chair for the Department of Emergency Medicine Perryrsquos primary research interest
is patient safety with an emphasis in human factorsergonomics and system failure She has
published widely on topics related to these areas as well as transitions in care the impact of
IT on clinical care and naturalistic decision-making
Frank Zwemer MD is section chief of emergency medicine at McGuire VAMC in Richmond
Virginia as well as associate chair in the Department of Emergency Medicine at Virginia
Commonwealth University He has implemented whiteboard and ED information systems
both in the private sector and in the Veterans Health Administration
Robert L Wears MD is a professor in the Department of Emergency Medicine at the
University of Florida and a visiting professor in the Clinical Safety Research Unit at Imperial
College London His interests lie in technical work studies joint cognitive systems and par-
ticularly the impact of information technology on safety and resilient performance
68 Journal of Cognitive Engineering and Decision Making Spring 2010