Embed Size (px)
Citation preview

36 / / Veterinary Focus / / Vol 20 No 2 / / 2010
Introduction, initial assessmentand stabilizationRespiratory distress in small animal patients is atrue emergency which requires rapid stabilization,prompt recognition and treatment of the under-lying problem, determination of diagnostic andtherapeutic options, and an assessment of pro-gnosis. The first steps in the management of thedyspneic patient include recognizing that therespiratory system is compromised, performinga physical examination, providing supplementaloxygen, and obtaining a brief but focused historyfrom the owner.
Physical examination Animals that present in respiratory distress must behandled carefully to minimize stress and strugglingand the initial physical examination may be limited
Emergency care of the patient with acute
respiratory distress
Lesley King, MVB, Dipl.ACVECC, Dipl. ACVIM,Dipl. ECVIM (CA)Philadelphia School ofVeterinary Medicine, Universityof Pennsylvania, Philadelphia,USA
Dr Lesley King graduated from the Faculty of VeterinaryMedicine, University College Dublin, Ireland, in 1986. Aftera year as a House Surgeon in Dublin, she moved tothe School of Veterinary Medicine at the University ofPennsylvania and completed a residency in small animalinternal medicine in 1989. Following the residency, Dr Kingremained on staff in the Intensive Care Unit at theUniversity of Pennsylvania, and she is currently a Professorin the Section of Critical Care, and the Director of theIntensive Care Unit. Her research interests include allaspects of small animal intensive care medicine, withspecial emphasis on pulmonary medicine and outcomeprediction in the critical small animal patient.
KEY POINTS
Respiratory distress is a common presenting sign forsmall animals, especially in emergency clinics
Recognizing common respiratory patterns androutine breed- and age-related problems can help tonarrow the list of differential diagnoses
Emergency management is facilitated by identifyingthe anatomic location of the problem
Supplemental oxygen and efforts to minimizehandling and stress are imperative for these patients
Thoracic radiographs, pulse oximetry and blood gasanalysis are the most commonly utilized emergencydiagnostic tests for respiratory disease
Emergency clinicians should be familiar with life-saving interventions such as endotracheal intubation,thoracocentesis, and thoracostomy tube placement
Dana Clarke, VMD Philadelphia School ofVeterinary Medicine, Universityof Pennsylvania, Philadelphia,USA
Dana Clarke attended the School of Veterinary Medicine atthe University of Pennsylvania, graduating in 2006. Shecompleted a one-year rotating internship at Michigan StateUniversity then returned to the University of Pennsylvaniain 2007 to begin a three-year residency in Emergency &Critical Care. She is set to complete her residency this yearand would like to continue working in an academicintensive care unit. Her clinical and research interestsinclude respiratory disease, mechanical ventilation, care ofcritical post-operative patients, and microcirculation.

Vol 20 No 2 / / 2010 / / Veterinary Focus / / 37
to assessment of mucous membranes, capillary refill,and thoracic auscultation. Commonly the clinicianmay note increased respiratory rate and/or effort,shallow chest excursions, excessive respiratory noise,extension of the head and neck, nostril flare, mouthbreathing, elbow abduction, and an inability to liedown or be comfortable. Patients on the verge ofrespiratory arrest may have limited movement ofthe chest wall and a paradoxical respiratory patterndue to respiratory muscle fatigue (1-4).
It is imperative to assess airway patency at pre-sentation by observing that the patient is able tomove air during breathing; the animal should notbe stressed by attempting to open the mouth. Ifcomplete airway obstruction is diagnosed, rapidsequence sedation, intubation and possibly positivepressure ventilation are indicated. Cyanosis isnot a reliable indicator of hypoxemia, as it doesnot develop until the partial pressure of oxygen inarterial blood (PaO2) is <50mmHg, and cannotbe detected in severely anemic or hypoperfusedpatients. Therefore the presence of pink mucousmembranes should not be perceived as an indic-ation of adequate oxygenation (1,4). A brief periodof thoracic auscultation at this time should includeauscultation of the heart to detect arrhythmias ormurmurs, auscultation of the lungs with particularattention to areas of dullness or abnormal lungsounds such as crackles or wheezes, and auscult-ation of the cervical trachea to detect loud soundsindicating a possible airway obstruction.
Many dyspneic patients, especially cats, are intol-erant of handling. Therefore supplemental oxygen,regardless of the cause of respiratory distress,is imperative for all patients with respiratorycompromise. If possible, a peripheral intravenouscatheter should also be placed at presentation toprovide vascular access.
Methods of oxygensupplementationMethods of oxygen support include flow-by, mask,hood delivery, nasal oxygen catheters, oxygencage, and positive pressure ventilation (3-7).
Flow-by oxygen is the provision of oxygen through atube held in front of the patient’s face. Inexpensiveand uncomplicated, it does require some patientrestraint and someone to hold the line to the
patient’s mouth and nose. It is most useful forshort-term provision of supplemental oxygenduring the initial assessment of the animal andduring brief procedures such as radiographs andcatheter placement (4-7) but may be insufficient forpatients that are panting or moving. Flow ratesshould be between 100-200 mL/kg/min, but highflow rates may not be well tolerated and arecomparatively wasteful. The effectiveness of flow-by oxygen can be improved via an oxygen mask: aplastic cone that attaches to the oxygen line. Withsimilar flow rates to those given above, thistechnique provides higher percentages of inspiredoxygen (especially with a well-fitted mask and arecumbent patient). Mobile patients will requirerestraint to keep the mask in place, and manydistressed animals resist placement of the maskover their face. An oxygen hood can be fashionedfrom an Elizabethan collar partially covered withplastic wrap. An oxygen line is inserted inside thecollar, with the plastic cover vented to allow expiredheat and gases to escape. Commercially availablehoods, with an adjustable collar and perforatedholes for expired gas release, also exist. Hoodsare generally well tolerated, can achieve highpercentages of inspired oxygen and allow forpatient monitoring and procedures withoutinterrupting oxygen delivery. However, there is nocontrol over the amount of inspired oxygen andsome patients, especially those that are panting,may overheat. Humidification should be used forlong term oxygen hood therapy (3-6). Nasalcatheters can provide high percentages ofinspired oxygen via an indwelling catheter (seeTable 1) or human nasal oxygen prongs (whichare less invasive and useful in quiet or recumbentpatients - Figure 1), using flow rates of 0.5-3 L/min.This technique is useful in patients that are restlessor panting, or too large or intolerant of an oxygencage, and is less wasteful than other methods. Itallows patient monitoring and further procedureswithout interruption of oxygen therapy, but giventhe time needed for catheter placement thismethod is usually reserved for more long-termtreatment (rather than initial stabilization) andhumidification should be added in this situation(3,4,6,7). Oxygen cages are extremely useful asthey provide accurate and (if indicated) highconcentrations of humidified oxygen, allowingpatient observation without restraint. Howevercages are expensive and can be wasteful as

38 / / Veterinary Focus / / Vol 20 No 2 / / 2010
© D
ana
Cla
rke
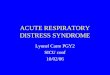
Figure 1. The use of human nasal oxygen prongs in a dog with respiratorydisease.
To place indwelling nasal oxygen catheters, one or both nostrils should first be infused with lidocaine. Asuitable catheter should be selected, measured to the medial canthus of the eye, and marked at that depthprior to insertion. With an assistant restraining the dog’s head, the catheter should be advanced into thenasal passage gently but quickly, as the initial sensation of passing through the rostral part of the ventralmeatus is the most uncomfortable part for the patient. Once inserted to the mark, the catheter should besecured using tissue glue or sutured with a tape butterfly or a Chinese finger-trap suture pattern. Anyremaining length of catheter should be secured to the top of the patient’s head to avoid irritating the ears orwhiskers. Most patients will also require an Elizabethan collar to prevent them from scratching or dislodgingthe catheter.
Table 1. Nasal oxygen catheter placement
oxygen concentration decreases rapidly whenthe door is open. If severe respiratory distresscannot be relieved using other techniques,intubation and positive pressure ventilation isthe best way to control the airway, deliver oxygenor positive end-expiratory pressure, to relievethe patient’s anxiety and discomfort. Heavysedation or light anesthesia, constant intensivemonitoring, specialized equipment and trainingare required for this technique (4-7).
Regardless of the method of oxygen supplem-entation chosen, it is important to remember thatprolonged periods (>24 hours) of high oxygenconcentrations (>60%) should ideally be avoidedto reduce the risk of oxygen toxicity due to freeradical formation (4,6,7).
Obtaining a historyAfter the patient has been stabilized with supple-mental oxygen, a preliminary history can beobtained from the owner. Important information
includes the duration and nature of respiratorysigns, the presence of coughing, gagging, orexercise intolerance, possibility of toxin or foreignbody ingestion, voice changes, history of heart orpulmonary disease, use of heartworm prevent-ative, and the presence of concurrent systemicillness, such as vomiting, anorexia, and endocrinediseases. A current medication list should also beobtained. Once a physical examination has helpeddetermine the anatomic origin of the respiratorydistress and the animal has been stabilized, a morecomplete history can be obtained and a definitivediagnostic and therapeutic plan reviewed with theowners.
Localization of respiratorycompromise, diagnostics, andtherapeuticsA more complete physical examination can beperformed to localize the origin of respiratorydistress. Based on this examination, the causesof respiratory distress can be assigned to one offive categories: airway obstruction, pulmonaryparenchymal disease, pleural space disease,thoracic wall abnormalities, and “look-alikes”.Identification of the probable site of the problem,combined with the signalment and history, allowsthe determination of a list of likely differentialdiagnoses, necessary diagnostics and immediatetherapeutic options.
Airway obstructionThese patients may have inspiratory and/orexpiratory stridor or stertor, head and neckextension, heat and exercise intolerance, pro-longed inspiration, cyanosis, a honking or dry

Vol 20 No 2 / / 2010 / / Veterinary Focus / / 39
a b
c d © D
ana
Cla
rke
EMERGENCY CARE OF THE PATIENT WITH ACUTE RESPIRATORY DISTRESS
Figure 2. Common sites of pulse oximetry probe placement (2a: the tongue, 2b: lip, 2c: pinna) and an example of a reliable pulse oximetrywave (2d). A uniform waveform, which matches the patient’s heart rate, must be present in order to accept the pulse oximetryreading as reliable. Excessive patient movement, poor contact due to fur, and pigmentation can interfere with the generation of areliable pulse oximetry value.
cough, respiratory distress, retching, and collapse.Dogs may be hyperthermic and cats may haveintermittent open mouth breathing. A prolongedinspiratory phase of respiration (because theupper airway is sucked closed on inspiration) maybe noted and wheezes may be heard, particularlyon expiration. Coughing is commonly seen incats with asthma, and lower airway obstructivedisease is associated with increased expiratoryeffort. Referred upper airway noise may bedifferentiated from pulmonary parenchymalsounds as the sound intensity and pitch islouder on auscultation of the larynx and trachea(1,2,4,8,9).
Common causes of airway obstruction in dogsinclude: brachycephalic airway syndrome, laryngealparalysis, inflammation or edema of the pharynxor larynx, airway infections and/or abscessation,foreign body, coagulopathy induced hemorrhage,neoplasia, tracheal and mainstem bronchialcollapse, and bronchitis (1,4,8,9). In cats, the most
common causes of airway obstruction are felineasthma, nasopharyngeal polyps, pharyngeal andlaryngeal neoplasia, inflammatory and granulo-matous laryngeal disease, and viral nasal infections(2,4,8,9).
Since airway obstructions may impede oxygenation,ventilation, or both, useful diagnostics include pulseoximetry (Figure 2) and arterial or venous bloodgas analysis. Hypoventilation is defined as arterialcarbon dioxide partial pressure (PaCO2) >43 mmHgin dogs and >36 mmHg in cats, resulting in primaryrespiratory acidosis. PaCO2 >60 mmHg is consistentwith significant hypoventilation and warrantsdefinitive therapy to relieve the airway obstruction.When arterial blood gas sampling is not possible,venous carbon dioxide partial pressure (PvCO2) canbe used. Hypoxemia is defined as arterial partialpressure of oxygen (PaO2)<80 mmHg and a valueof PaO2 <60 mmHg (which corresponds to <90%pulse oximetry) is consistent with severe hypo-xemia and requires therapeutic intervention.

40 / / Veterinary Focus / / Vol 20 No 2 / / 2010
In these patients initial stabilization should be aimedat provision of supplemental oxygen, establishingvascular access, and applying cooling measures.Sedative and/or anxiolytic therapies can relieverespiratory distress and decrease respiratory drive,thus decreasing the degree of airway collapse.Intravenous fluid therapy, wetting of the fur andthe use of a fan will aid cooling. Anti-inflammatorydoses of corticosteroid may also be considered; thiscan be life-saving in patients with severe airwayedema or inflammation but should be usedselectively as it may impede a definitive diagnosisof lymphoma (1,8). Cats with feline asthma maybenefit from parenteral bronchodilators such asterbutaline if they have no evidence of heartdisease. Inhaled drugs (e.g. albuterol, fluticasone)may be substituted if complicating systemicdisease is present. In the majority of patients,sedation, cooling and head/neck positioningto optimize airway patency are sufficient forstabilization.
For those with complete airway obstruction, orwhen cooling and sedative efforts are ineffective,induction of anesthesia and intubation is required.If endotracheal intubation cannot be achieved,an emergency tracheostomy must be performed.
The cause of an upper airway obstruction canusually be diagnosed by a sedated upper airway/laryngeal examination, cervical and thoracic radio-graphs, fluoroscopy, rhinoscopy/laryngoscopy/tracheoscopy/bronchoscopy, and/or computedtomography (CT). If a hematoma caused by acoagulopathy (e.g. secondary to rodenticide) issuspected, prothrombin time (PT) and partialthromboplastin time (PTT) should be performed.Transtracheal lavage, endotracheal lavage,or bronchoalveolar lavage should be consideredin patients suspected to have lower airway(bronchial) or concurrent pulmonary parenchymaldisease.
Pulmonary parenchymal diseaseDogs with pulmonary parenchymal diseaseare often depressed; signs may include: pantingor breathing open-mouthed, with nostril flare,coughing, head and neck extension, and anxiety.Cats only breathe through an open mouth whenthey have severe respiratory compromise and (in
contrast to dogs) rarely cough. Physical examin-ation findings may include weakness, tachypnea,tachycardia, fever, mucopurulent nasal discharge,harsh lung sounds, and/or crackles. A heart murmurand/or arrhythmias are usually heard in dogsthat have respiratory signs due to congestive heartfailure. The same is not always true of cats withcongestive heart failure, when cardiac auscult-ation may be normal. Pulse quality may bediminished whilst cyanosis may be seen in severelyhypoxemic patients although hypoperfusionmay produce pallor of the mucous membranes(1,2,4).
Common causes of pulmonary parenchymaldisease include parasitic or bacterial pneumonia,pulmonary edema (cardiogenic or non-cardio-genic), pulmonary contusions, smoke inhalation,pneumonitis (chemical and uremic), aspirationpneumonia, fungal or viral infection, pulmonarythromboembolism, neoplasia, pulmonary fibrosis,and acute respiratory distress syndrome (ARDS).Cardiogenic edema occurs frequently in cats,whereas aspiration pneumonia is uncommon inthis species (1-4,10).
Thoracic radiographs are particularly importantin this situation. For example, classic radiographicchanges associated with pneumonia include acranio-ventral alveolar pattern (Figure 3), whereascardiogenic pulmonary edema in dogs is generallyassociated with a heavy perihilar interstitial toalveolar pattern (Figure 4). In contrast, non-cardiogenic pulmonary edema is associated witha caudo-dorsal interstitial to alveolar pattern(Figure 5).
Pulmonary parenchymal disease causes hypo-xemia primarily by mismatch of ventilation andperfusion, but also due to diffusion impairment andintrapulmonary shunt. Pulse oximetry and bloodgas analysis are important in determining theseverity of disease, and hematology and bio-chemistry may assist diagnosis. Lower respiratorytract sampling via transtracheal, endotracheal, orbronchoalveolar lavage can be important diagnosticsto determine the origin of pulmonary parenchymaldisease, especially in patients with atypical radio-graphic changes or when multiple disease processesare suspected, and cytology, bacterial culture and

Vol 20 No 2 / / 2010 / / Veterinary Focus / / 41
© D
ana
Cla
rke
© Le
sley
Kin
g, D
ana
Cla
rke
© Le
sley
Kin
g, D
ana
Cla
rke
EMERGENCY CARE OF THE PATIENT WITH ACUTE RESPIRATORY DISTRESS
Figure 4.
Lateral thoracic radiograph in a dog with perihilar cardiogenicpulmonary edema, cardiomegaly, and pulmonary venousdistension.
Figure 5.
Lateral thoracic radiograph from a puppy after being strangled byhis collar, demonstrating the caudo-dorsal, heavy interstitial toalveolar pattern commonly seen in patients with non-cardiogenicpulmonary edema.
Figure 3. Lateral thoracic radiograph from a dog with aspiration pneumoniashowing the cranioventral alveolar pattern commonly seen inthis disease process.
sensitivity, and fungal culture are usually indicated.Emergency therapy for patients with pulmonaryparenchymal disease depends on the clinician’seducated guess about the most likely etiology.
Pleural space diseaseClinical signs in these patients may include ashort, shallow restrictive breathing pattern,increased respiratory rate, nostril flaring, ortho-pnea, an abdominal component to respiration,and a reluctance to lie down. Cats may haveopen mouth breathing. The degree of respiratorydistress depends on the rate of development ofthe pleural space-occupying lesion, especiallypleural effusion. Paradoxical respiration may benoted in patients with a diaphragmatic hernia.Thoracic auscultation may reveal decreased ordull lung sounds ventrally (pleural effusion) ordorsally (pneumothorax), an auscultable fluidline, muffled cardiac sounds, or borborygmiif stomach or intestines are in the chest. Thoracicauscultation changes may be unilateral or bilateraland are not always equal. Cats with a mediastinalmass have decreased chest wall compressibility(1,2,4,11,12).
Common causes of pleural space disease includepneumothorax and pleural effusions. Pleuraleffusions may be pure or modified transudates dueto congestive heart failure, vasculitis, and lung lobetorsion; pyothorax, chylothorax, hemothorax, felineinfectious peritonitis, and neoplastic effusions arealso common. Diaphragmatic hernia and pleuralspace masses also occur (1,2,4,11,12).
If pleural disease is suspected, it is imperative toevacuate the pleural space as quickly as possible(Table 2). Oxygen supplementation and vascularaccess is established if it can be done withoutstress. Thoracocentesis is both therapeutic anddiagnostic, and any fluid obtained submitted forcytology and culture. Thoracocentesis is not indic-ated for patients with pleural space masses,diaphragmatic hernias, or hemothorax secondaryto coagulopathy that is not causing significantrespiratory compromise. Other diagnostics (e.g.radiography or ultrasound) should be delayed untilafter the animal has been stabilized by thoraco-centesis, allowing the pulmonary parenchyma tobe visualized effectively.

42 / / Veterinary Focus / / Vol 20 No 2 / / 2010
Table 2. Thoracocentesis
Sedation is often not necessary unless the patient is very distressed or agitated; most animals can be restrainedin sternal recumbence for the procedure. The patient’s chest wall should be prepared in the region where thelung sounds are most muffled. This is generally in the upper third of the caudodorsal thorax between the 8th
and 9th ribs for pneumothorax, and in the ventral two thirds of the thorax between the 6th and 8th intercostalspaces for pleural effusion. Alternatively, an ultrasound probe can be used to find pockets of fluid amenableto aspiration. When aspirating air, a 22 or 25 gauge straight needle or butterfly needle is preferred; larger gaugeneedles (18 or 20 g) are often needed for pleural fluid aspiration in dogs. The needle is attached to tubing, athree-way stopcock, and syringe. The cranial border of the rib is palpated, and the needle is advanced throughthe skin, bevel up, and slowly into the thoracic cavity on the cranial border of the rib. The needle should beslowly advanced while an assistant aspirates the system; the needle is then held still as soon as air or fluid isvisible in the tubing. Air and fluid should be aspirated until negative pressure is achieved, at which point theneedle may be advanced further into the thorax, redirected, or repositioned if additional air or fluid issuspected.
Normally blood aspirated during thoracocentesisshould clot quickly, unless a coagulopathy or ahemorrhagic effusion (e.g. due to neoplasia orlung lobe torsion) is present; if this occurs furthertesting to confirm these suspicions should beperformed. If unexpected air is aspirated, thecollection system should be checked for leaks.If no leaks are present, thoracoentesis shouldbe temporarily aborted as long as the animal isstill stable, because an iatragenic pneumothoraxmay have been created (3,4,12,13). If negativepressure is not achieved during thoracocentesis,if the patient re-accumulates a significant amountof air within a short period requiring multiplethoracocentesis events, or for the medicalmanagement of certain pleural effusions such aspyothorax, thoracostomy tubes (unilateral orbilateral) may be needed and are best placedusing general anesthesia (1,3,4,14).
Thoracic wall abnormalitiesAbnormalities of thoracic wall function mayoccur because of dysfunction at several levels. Insome cases, respiratory distress may be second-ary to thoracic wall injuries or trauma. Thosepatients often demonstrate pain on manipulationor palpation of the thorax, and may have a flailchest with paradoxical motion of a segment ofchest wall. Lacerations, bruising or concurrentpulmonary contusions may occur. Alternatively,abnormal thoracic wall and diaphragmatic funct-ion may result from defective neuromuscular
control of breathing, which may be caused bydisease in the brain, spinal cord, peripheral nervesor neuro-muscular junctions. Such patientstypically lack diaphragmatic and abdominalmuscle movement, and have clinical evidence ofhypoventilation with elevated PaCO2 levels onblood gas analysis (1,3,15).
Common causes of thoracic wall dysfunctioninclude traumatic injuries, anesthetics and centralrespiratory depressants, severe hypokalemia,myasthenia gravis, botulism, tick paralysis,polyradiculoneuritis, congenital abnormalities,some snake envenomation, thoracic wall neo-plasia, and spinal cord or phrenic nerve disease(1,3,15).
Diagnostics for these patients include bloodgas analysis, pulse oximetry, capnography, andthoracic radiographs. Neurologic examinationfindings consistent with cervical spinal cord orbrainstem dysfunction may support a neurologicorigin. Measurement of acetylcholine receptorantibody titers, edrophonium response testing,and electromyelography (EMG) can aid in thediagnosis of myasthenia gravis. EMG and theconfirmation of botulism toxin in serum, feces,or vomited material can support a diagnosis ofbotulism. There are no specific diagnostic testsfor tick paralysis, polyradiculoneuritis, and snakevenoms, though geographic location, signalment,and history may support a diagnosis (15).

Vol 20 No 2 / / 2010 / / Veterinary Focus / / 43
1. Lee JA, Drobatz KJ. Respiratory distress and cyanosis in dogs. In: KingLG. Textbook of respiratory disease in dogs and cats. Philadelphia: WBSaunders 2004; 1-12.
2. Mandell DC. Respiratory distress in cats. In: King LG. Textbook of respiratorydisease in dogs and cats. Philadelphia: WB Saunders 2004; 12-17.
3. Tseng LW, Waddell LS. Approach to the patient in respiratory distress. ClinTech Small Anim Pract 2000; 15: 53-62.
4. Macintire DK, Drobatz KJ, Haskins SC, et al. Manual of small animalemergency and critical care medicine. Philadelphia: Lippencott, Williamsand Wilkins, 2005; 115-159.
5. Rozanski E, Chan DL. Approach to the patient with respiratory distress.Vet Clin Small Anim Pract 2005; 35: 307-317.
6. Tseng LW, Drobatz KJ. Oxygen supplementation and humidification.In: King LG. Textbook of respiratory disease in dogs and cats.Philadelphia: WB Saunders 2004; 205-213.
7. Mazzaferro EM. Oxygen therapy. In: Silverstein DC, Hopper K.Small Animal Critical Care Medicine. Philadelphia: WB Saunders 2009; 78-81.
8. Costello MF. Upper airway disease. In: Silverstein DC, Hopper K.Small Animal Critical Care Medicine. Philadelphia: WB Saunders 2009;67-72.
9. Holt DE. Upper airway obstruction, stertor, and stridor. In: King LG.Textbook of respiratory disease in dogs and cats. Philadelphia: WBSaunders 2004; 35-42.
10. De Clue AE, Cohn LA. Acute respiratory distress syndrome in dogsand cats: a review of clinical findings and pathophysiology.J Vet Emerg Crit Care 2007; 17: 340-347.
11. Suave V. Pleural space disease. In: Silverstein DC, Hopper K. Small AnimalCritical Care Medicine. Philadelphia: WB Saunders 2009; 125-130.
12. Silverstein DC. Pleural space disease. In: King LG. Textbook of respiratorydisease in dogs and cats. Philadelphia: WB Saunders 2004; 49-52.
13. Sigrist NE. Thoracocentesis. In: Silverstein DC, Hopper K. Small AnimalCritical Care Medicine. Philadelphia: WB Saunders 2009; 131-133.
14. Sigrist NE. Thoracostomy tube placement and drainage. In: SilversteinDC, Hopper K. Small Animal Critical Care Medicine. Philadelphia: WBSaunders 2009; 134-137.
15. Donahue S. Chest wall disease. In: Silverstein DC, Hopper K.Small Animal Critical Care Medicine. Philadelphia: WB Saunders 2009;138-140.
16. Hall K, Lee JA. Nonrespiratory look-alikes. In: Silverstein DC, Hopper K.Small Animal Critical Care Medicine. Philadelphia: WB Saunders 2009;141-144.
EMERGENCY CARE OF THE PATIENT WITH ACUTE RESPIRATORY DISTRESS
REFERENCES
“Look-alikes”Whilst rare, some non-respiratory conditionscan mimic respiratory disease. Examples includehyperthermia, compensation for metabolic acid-osis, anemia, pain, stress, anxiety, hypovolemia,abdominal distension (cranial organomegalyand abdominal effusion), hyperadrenocorticismor corticosteroid therapy, and certain opioidmedications (16). History, physical examination,thoracic radiographs, blood gas analysis andserum chemistry can be helpful to distinguishthese conditions from real respiratory disease.
ConclusionRespiratory distress is a common and seriousemergency encountered by veterinarians. Anunderstanding of the need for careful patienthandling and the provision of supplementaloxygen is vital. Veterinarians should recognize thesignalment, history, and physical examinationfindings seen with common respiratory diseases.An understanding of respiratory disease patho-physiology and localization as well as thediagnostic and therapeutic techniques essentialfor management of each category of dysfunctionis crucial for successful treatment.





![Chronic Pancreatitis Associated Acute Respiratory Failuremedcraveonline.com/MOJI/MOJI-05-00149.pdf · Chronic Pancreatitis Associated Acute Respiratory ... [1,2]. Acute respiratory](https://img.pdfslide.us/doc/110x75/5ca432de88c993ad338b9ab4/chronic-pancreatitis-associated-acute-respiratory-f-chronic-pancreatitis-associated.jpg)