Embed Size (px)
Citation preview

Author: Guy Jackson, Patrick Bose Date: November 2018
Job Title: Consultant anaesthetist, Consultant obstetrician Review Date: September 2019
Policy Lead: Group Director Urgent Care Version: V4.2 November 2018 V4.0 ratified 1/9/17
Location: Policy hub/ Clinical/ Maternity/ Intrapartum/ GL832
This document is valid only on the date last printed Page 1 of 9
Emergency Caesarean sections guideline
(GL832)
Approval and Authorisation
Approved by Job Title or Chair of Committee Date
Maternity & Children’s Services
Clinical Governance Committee
Chair, Maternity Clinical
Governance Committee
1st September
2017
Change History
Version Date Author Reason
3.0 Oct 2014 P Street, Consultant Obstetrician Reviewed
3.1 July 2015 A Mansfield, Mat Info Officer VTE risk assessment & Emergency CS roles & responsibilities updated (pg. 10-12)
3.2 Aug 2015 G Jackson, Consultant
Anaesthetist
Addition of appendix B categorising degree of urgency for CS
4.0 July 2017 P Bose (Consultant Obstetrician),
G Jackson (Consultant
Anaesthetist)
Reviewed – changes made throughout to make more concise and reflect current practice
4.1 Nov 2017 A Mansfield (Mat Info Officer) Appendix C updated
4.2 Nov 2018 A Mansfield (Mat Info Officer) Appendix C updated

Author: Guy Jackson, Patrick Bose Date: November 2018
Job Title: Consultant anaesthetist, Consultant obstetrician Review Date: September 2019
Policy Lead: Group Director Urgent Care Version: V4.2 November 2018 V4.0 ratified 1/9/17
Location: Policy hub/ Clinical/ Maternity/ Intrapartum/ GL832
This document is valid only on the date last printed Page 2 of 9
Emergency caesarean sections (GL832) November 2018
Overview: An emergency caesarean section (category 1-3) is usually performed in labour
(but may be required antenatally) if complications develop in pregnancy or labour that
increase the risk to the mother’s or babies health or life.
Preparation for Caesarean Section1, 2:
COMMENCE EMERGENCY OBSTETRIC CARE PATHWAY
Establish Intravenous access if time
Ensure appropriate blood samples taken: FBC, clotting (if needed), group & save
samples for all (2 samples needed – one historical and one within last 72 hours) or
cross-match (if suspected haemorrhage or difficult operation anticipated.
Ranitidine 150mgs orally
Obtain consent and provide mother with maternity information leaflet on Unplanned
(emergency) Caesarean Section
Contact:
o Anaesthetist, obstetrician, theatre team, delivery suite co-ordinator
o If category 1 Call 2222 stating Category 1 CS
o See appendix A ‘Emergency caesarean section staff responsibilities’ (2015)
o Clearly state urgency to ALL members of the team
o See appendix B Classification of urgency
Women whose situation is classified as category 2 or 3 will require regular review
whilst awaiting transfer to theatre as the situation is dynamic and may deteriorate. If
for any reason there is a delay this must be clearly documented in the mother’s
electronic records.
In the event of unavailability of a theatre or to achieve delivery within the timeframe set the
Second Emergency Theatre flowchart (EMA084) should be followed
Undertake WHO (World Health Organisation) checklist before commencing surgery
Prophylactic antibiotics
Women having a CS should have prophylactic antibiotics to reduce the risk of
postoperative infections which occurs in about 8% of women who have had a CS1.
See also ‘Antibiotic & prophylaxis guideline for Obstetrics (GL787).

Author: Guy Jackson, Patrick Bose Date: November 2018
Job Title: Consultant anaesthetist, Consultant obstetrician Review Date: September 2019
Policy Lead: Group Director Urgent Care Version: V4.2 November 2018 V4.0 ratified 1/9/17
Location: Policy hub/ Clinical/ Maternity/ Intrapartum/ GL832
This document is valid only on the date last printed Page 3 of 9
Emergency caesarean sections (GL832) November 2018
Paired Cord Samples
ALL cases of emergency caesarean section will have paired cord samples taken to allow
review of fetal wellbeing and guide ongoing care of the baby1. See guideline FBS/paired
cord sampling (GL839).
DOCUMENTATION
Make comprehensive notes of the delivery in the electronic maternity health record (K2)
including any problems or concerns as soon as practical.
The minimum data required are:
Indication for caesarean section (there may be more than one)
Surgical incision and ease of access (or not) to peritoneal cavity
Lie of fetus
Condition of the liquor (meconium, odour etc)
Engagement or not of the presenting part
Condition of neonate at delivery
Whether paired cord samples were obtained or not
Delivery of the placenta and membranes
Checking of uterine anatomy, fallopian tubes and ovaries. Recording of any
deviation from normality
Estimated blood loss
Thoughts for mode of delivery in subsequent pregnancy
Any additional instructions for post operative care, particularly if the procedure has
been in any way complicated.
Care of mother in first 24 hours1:
Following surgery the woman should remain either in recovery or on the
Delivery Suite for a minimum of two hours
Follow post anaesthetic care guideline for recovery on Delivery Suite (GL767)
Analgesia - Follow Puerperal Analgesia guideline GL768
Oral intake
Women who are recovering well after CS and who do not have complications can eat and
drink when they feel hungry or thirsty.

Author: Guy Jackson, Patrick Bose Date: November 2018
Job Title: Consultant anaesthetist, Consultant obstetrician Review Date: September 2019
Policy Lead: Group Director Urgent Care Version: V4.2 November 2018 V4.0 ratified 1/9/17
Location: Policy hub/ Clinical/ Maternity/ Intrapartum/ GL832
This document is valid only on the date last printed Page 4 of 9
Emergency caesarean sections (GL832) November 2018
Diabetic mothers should be managed as per guideline Diabetes in pregnancy (GL983),
Appendix 2 (pg. 9).
If the mother is unable to tolerate food or drink and when there are absent bowel sounds
there may be a paralytic ileus which should be managed according the paralytic ileus
guideline. See guideline ‘Bowel complications after CS including Paralytic Ileus (GL796)’
Removal of the urinary bladder catheter
Once a woman is mobile after a regional anaesthetic
Not sooner than 12 hours after the last epidural ‘top up’ dose or spinal
See guidelines for ‘Bladder care post-partum including women with epidural analgesia
(GL792)’.
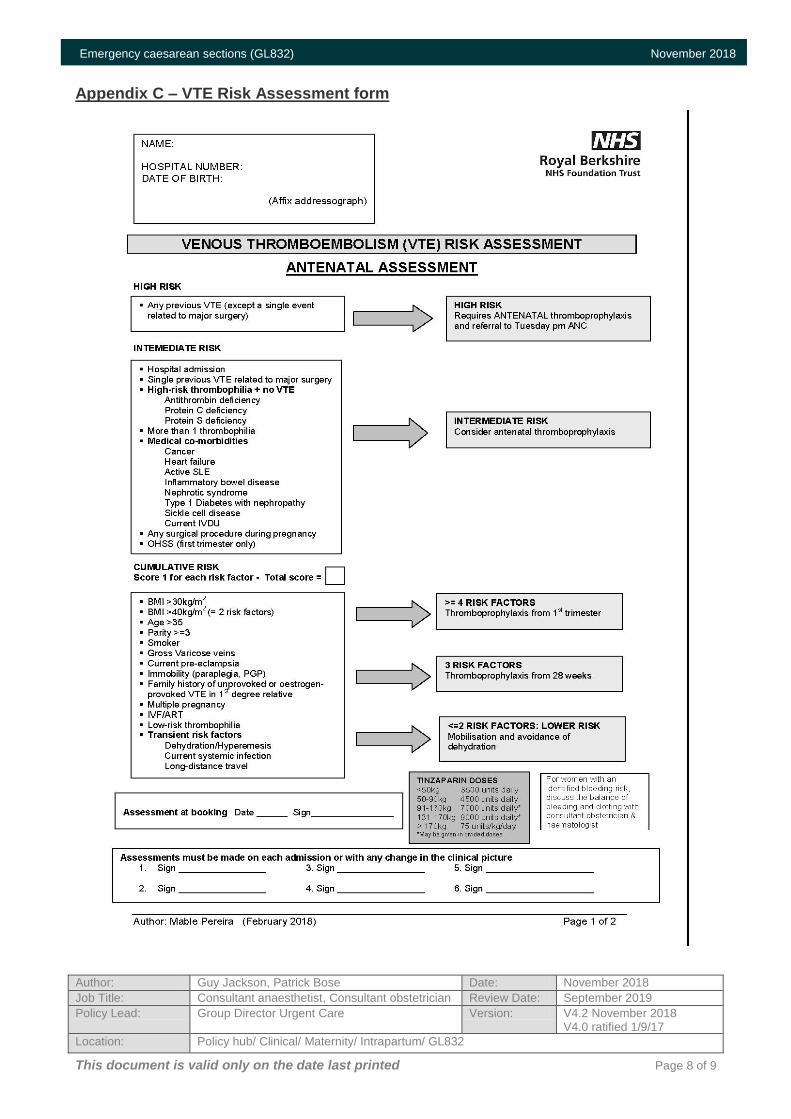
Thromboprophylaxis
A VTE risk assessment should be performed on all cases of emergency caesarean
section
Follow “postnatal prophylaxis against thromboembolism guidance (GL891)”
See Appendix C - VTE risk assessment and management
On admission to the post-natal ward a repeat VTE assessment is done
Postoperative ongoing care
Should include:
MOWS should be performed and recorded 4 hourly for first 24 hours then twice
daily up to 48 hours
The woman should be advised to wear loose, comfortable clothes and cotton
underwear
All dressings to be left on for five days unless obvious leaking or signs of infection
of the wound, such as increasing pain/redness /discharge, separation or
dehiscence
Most wounds are closed using monocryl. If used, non-absorbable sutures (such as
prolene) are usually removed in community on day 5 unless otherwise stated
ALL caesarean sections must be reviewed within 48 hours by the obstetric SHO

Author: Guy Jackson, Patrick Bose Date: November 2018
Job Title: Consultant anaesthetist, Consultant obstetrician Review Date: September 2019
Policy Lead: Group Director Urgent Care Version: V4.2 November 2018 V4.0 ratified 1/9/17
Location: Policy hub/ Clinical/ Maternity/ Intrapartum/ GL832
This document is valid only on the date last printed Page 5 of 9
Emergency caesarean sections (GL832) November 2018
If no problems identified the woman should be formally transferred to Midwife Care
after 48 hours
Prescriptions for low molecular weight heparin (LMWH, such as Clexane) have to
be obtained from the RBFT pharmacy
If any postoperative complications/concerns are identified the duty consultant
obstetrician should be informed.
There is no evidence that ‘routine’ chest physiotherapy improves respiratory outcome for
most women. However, an obstetric physiotherapist is available for women who need to
be seen and out of hours, the on-call physiotherapist can be requested to see the patient.
Discuss implications for future deliveries
After the operation there should be a discussion with the patient regarding the reasons for
the caesarean and implications for the child or future pregnancies1, 3. This discussion
should be documented in the woman’s health care record covering the following:
The events surrounding the birth
Recommendations for future pregnancy – i.e. elective CS or VBAC confirmed early
in pregnancy
Likely success at future VBAC
Information copied to GP
Women who have had a previous CS should be booked under consultant care in their next
pregnancy. The mother should be given the completed caesarean section letter of why
the caesarean was performed for their information and a copy sent to the GP.
References
1. National Institute for Clinical Excellence (2011). Caesarean Section CG132.
London.
2. Royal College of Obstetricians and Gynaecologists (2001). The National Sentinel
Caesarean Section Audit Report. London.
3. NHS Institute for Innovation and Improvement. (2007). Focus on: Caesarean
section. London.

Author: Guy Jackson, Patrick Bose Date: November 2018
Job Title: Consultant anaesthetist, Consultant obstetrician Review Date: September 2019
Policy Lead: Group Director Urgent Care Version: V4.2 November 2018 V4.0 ratified 1/9/17
Location: Policy hub/ Clinical/ Maternity/ Intrapartum/ GL832
This document is valid only on the date last printed Page 6 of 9
Emergency caesarean sections (GL832) September 2017
Appendix A – Emergency C-section roles & responsibilities

Author: Guy Jackson, Patrick Bose Date: November 2018
Job Title: Consultant anaesthetist, Consultant obstetrician Review Date: September 2019
Policy Lead: Group Director Urgent Care Version: V4.2 November 2018 V4.0 ratified 1/9/17
Location: Policy hub/ Clinical/ Maternity/ Intrapartum/ GL832
This document is valid only on the date last printed Page 7 of 9
Emergency caesarean sections (GL832) November 2018
Appendix B – Categorising the degree of urgency for CS
Author: Guy Jackson, Patrick Bose Date: November 2018
Job Title: Consultant anaesthetist, Consultant obstetrician Review Date: September 2019
Policy Lead: Group Director Urgent Care Version: V4.2 November 2018 V4.0 ratified 1/9/17
Location: Policy hub/ Clinical/ Maternity/ Intrapartum/ GL832
This document is valid only on the date last printed Page 8 of 9
Emergency caesarean sections (GL832) November 2018
Appendix C – VTE Risk Assessment form

Author: Guy Jackson, Patrick Bose Date: November 2018
Job Title: Consultant anaesthetist, Consultant obstetrician Review Date: September 2019
Policy Lead: Group Director Urgent Care Version: V4.2 November 2018 V4.0 ratified 1/9/17
Location: Policy hub/ Clinical/ Maternity/ Intrapartum/ GL832
This document is valid only on the date last printed Page 9 of 9
Emergency caesarean sections (GL832) September 2017