-
8/7/2019 Emergency Airway Access
1/28
-
8/7/2019 Emergency Airway Access
2/28
Ensuring an adequate airway is the firstpriority in the primary
survey.In general
patients who are conscious and have anormal voice do not require
early attentionto their airway.Patients who have anabnormal voice
or altered mental status
require further airway evaluation. Options for airway access
include
nasotracheal,orotracheal and surgical.
-
8/7/2019 Emergency Airway Access
3/28
The most widely used route is orotracheal, in which an
endotrachealtube is passed through oral cavity.In a nasotracheal
procedure, anendotracheal tube is passed through thenose.
Other methods of intubation involvesurgery and include theI.
cricothyroidotomyII. tracheostomy
-
8/7/2019 Emergency Airway Access
4/28
T
racheal intubation is indicated in patients with:
Actual or impending airway obstruction due to Foreign body
common in infants and toddlers. Severe blunt orpenetrating injury
to the face
or neck may be accompanied by swellingand an expanding hematoma,
or
Injury to the larynx, trachea or bronchi. It is also common in
people who have suffered
smoke inhalation or burns within or near theairway.
Sustained generalized seizure activity and angioedema
-
8/7/2019 Emergency Airway Access
5/28
Defined as decreased oxygen content and oxygen saturation of the
bloodcaused due to hypoventilation) suspended (apnea), or when the
lungsare unable to sufficiently transfer gasses to the blood.
Examples of such conditions include
cervical spine injury,
multiple rib fractures,
severe pneumonia,
acute respiratory distress syndrome (ARDS), or
near-drowning.
Specifically, intubation is considered if the arterial partial
pressure of
oxygen (PaO2) is less than 60 millimeters of mercury (mm Hg)
whilebreathing an inspired O2 concentration (FIO2) of 50% or
greater. Inpatients with elevated arterial carbon dioxid
e, an arterial partialpressure of CO2 (PaCO2) greater than 45 mm
Hg in the setting ofacidemia would prompt intubation, especially if
a series ofmeasurements demonstrate a worsening respiratory
acidosis.
-
8/7/2019 Emergency Airway Access
6/28
Depressed level of consciousness due toa) Administration of
general anaesthesiab) Strokec) Non-penetrating head injuriesd)
Poisoning
e) Intoxication
f) when depressed level of consciousnessbecomes severe to the
point of stupororcoma (defined as a score on the GlasgowComa Scale
of less than 8)
-
8/7/2019 Emergency Airway Access
7/28
Diagnostic or therapeutic manipulation of the
airway (such as bronchoscopy, lasertherapy orstenting of the
bronchi) mayintermittently interfere with the ability
tobreathe.
-
8/7/2019 Emergency Airway Access
8/28
Relative contraindications include
maxillo facial trauma
laryngeal injury
cervical spine injuries
-
8/7/2019 Emergency Airway Access
9/28
PRE REQUISITESPre oxygenation with a bag valve mask apparatus
and100%oxygen,suction,adequate sedation and muscle relaxationan
appropriately sized ETT tube and a functional laryngoscope
are required
With the physician at the patients head,the head is so
positionedthat the pharyngeal and laryngeal axes are in
alignment.
The patients head and neck are fully extended. With the non
dominant hand,the physician opens the mouth
with the thumb and index finger on pts lower and upper
teeth.
The oropharynx is inspected and foreign bodies or secretions
areremoved,blade of the laryngoscope is introduced andadvanced with
gentle traction upward and towards the patientsfeet.
-
8/7/2019 Emergency Airway Access
10/28
oOnce the epiglottis is visualized the tipof the blade is
positioned in thevaleculla.the glottic opening and
vocal cords are visualized, the ET tubeis advanced under direct
vision until
the cuff passes through the vocalcords.
oCuff is inserted roughly 2cm past the
vocal cords and the patients incisorsshould rest between the 19
and 23 cm
markings on the tube.
oThe cuff is inflated and proper positionis confirmed by
auscultating bilateral
breath sounds.An anteroposterior chestx ray is obtained to
confirm
position.Ideallly the tip of the ET tubeshould be 2 to 4 cm
above the carina.
-
8/7/2019 Emergency Airway Access
11/28
-
8/7/2019 Emergency Airway Access
12/28
Chipped teeth
Emesis and aspiration
Vocal cord injury
Laryngospasm
Soft tissue injury to the oropharynx
-
8/7/2019 Emergency Airway Access
13/28
Advantages include
Direct visualization of the vocal cords
Ability to use larger diameter
endotracheal tubes
Applicability to apneic patients
Familiarity to most physicians Demerits
require neuromuscular blockade or
deep sedation
-
8/7/2019 Emergency Airway Access
14/28
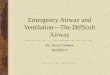
A cricothyrotomy is an incision made through the skin
andcricothyroid membrane to establish a patent airway
INDICATIONS include
Life-threatening situations, such as airway obstruction by
aforeign body, angioedema, or massive facial trauma.
A cricothyrotomy is nearly always performed as a lastresort in
cases where orotracheal and nasotrachealintubation are impossible
or contraindicated.
Advantages include Cricothyrotomy is easier and quicker to
perform than
tracheotomy, does not require manipulation of thecervical spine
and is associated with fewer complications.[
-
8/7/2019 Emergency Airway Access
15/28
The thyroid cartilage is easilyidentified in the midline of
theneck.The cricoid is the onlycomplete cartilaginous ring ,isthe
first ring inferior to thethyroid cartilage.Thecricothyroid
membrane joinsthese two cartilages and is anavascular
membrane.Inferiorto the cricoid and straddlingthe trachea is the
isthmus ofthe thyroid gland.The thyroidlobes lie lateral to the
tracheaand the superior poles canextend to the level of thethyroid
cartilage.
-
8/7/2019 Emergency Airway Access
16/28
If time permits the area is prepared,draped and anesthetized
with 1%lidocaine.
A vertical skin incision is made. The cricoid is identified and
held firmly and
circumferentially in the physicians non dominant hand until the
end of the
procedure.
With a no.11 or 15 blade, a small 3 to 5 cm transverse incision
is made over
the cricothyroid membrane.The incision is carried deep to the
until theairway is entered through the cricothyroid membrane.
The tract is widened using a clamp ,tracheal dilator or end of
the scalpelhandle.
The tracheostomy tube is inserted along its curve into the
trachea,the cuff is
inflated and bilateral breath sounds are confirmed.
If breath sounds are confirmed ,the tracheostomy is secured to
the skin by
suturing the tabs to the skin with heavy ,non
absorbable,monofilamentsuture.
A chest x ray is obtained to document the location of the
tracheostomytube.
Traditionally cricothyroidotomy was converted to formal
tracheostomy
.However it has been suggested that a cricothyroidotomy maybe
used long
term without an increase in acute complications.
-
8/7/2019 Emergency Airway Access
17/28
-
8/7/2019 Emergency Airway Access
18/28
Creation of a false passage when inserting tracheostomytube is
most common complications. Others include
Subcutaneous emphysema
Pneumothorax Injury to surrounding structures such as
thyroid,parathyroids,esophagus,anterior jugular
veins,andrecurrent laryngeal nerves can occur in situations of
urgency.
Subglottic stenosis and granuloma formation are potential
long term complications.
-
8/7/2019 Emergency Airway Access
19/28
-
8/7/2019 Emergency Airway Access
20/28
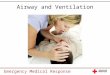
Tracheotomy consists of making an incisionon the front of the
neck and opening adirect airway through an incision in the
trachea. The resulting opening can serveindependently as an
airway or as a site fora tracheostomy tube to be inserted; thistube
allows a person to breathe without theuse of their nose or mouth.
The opening
may be made by a knife or a needle(referred to as surgical
andpercutaneous[72] techniques respectively)and both techniques are
widely used incurrent practice.
-
8/7/2019 Emergency Airway Access
21/28
In the acute setting, indications fortracheotomy are similar to
those for
cricothyrotomy. In the chronic setting, indications for
tracheotomy include the
o need for long-term mechanical
ventilation and removal of trachealsecretions (e.g., comatose
patients, or
o extensive surgery involving the headand neck).
-
8/7/2019 Emergency Airway Access
22/28
The patient is laid supine with padding placed under
theshoulders and neck extended.
A vertical midline incision is made from the inferior aspectof
the thyroid cartilage to the suprasternal notch and
continued down between the infrahyoid muscles. In extreme
urgency,a further vertical incision straight into
the trachea at the level of the second,third and fourth
ringshould be made immediately without regard to thepresence of
thyroid isthmus.
The knife blade is rotated through 90 ,thus opening the
trachea. Any form of available tube is inserted into the trachea
as
soon as possible and blood and secretion sucked out.
Once an airway is established hemostasis is thensecured.With the
emergency under control,thetracheostomy should be refashioned as
soon as possible.
-
8/7/2019 Emergency Airway Access
23/28
-
8/7/2019 Emergency Airway Access
24/28
-
8/7/2019 Emergency Airway Access
25/28
-
8/7/2019 Emergency Airway Access
26/28
INTRAOPERATIVE
Hemorrhage
Injury to para tracheal structures
injury to trachea
EARLY POST OP
Apnea caused by a fall in pCO2Hemorrhage
Subcutaneous emphysema,pneumomediastinum and pneumothorax
accidental extubation
anterior displacement of the tube
obstruction of the tube lumen
occlusion against tracheal wall
LATE POST OP
Difficult decannulation
Tracheocutaneous fistula
Tracheo-esophageal fistula
Trachea stenosis
-
8/7/2019 Emergency Airway Access
27/28
Although emergent tracheostomy has fallen into disfavor because
of itstechnical difficulties it may still be necessary in cases of
laryngotracheal
separation orlaryngeal fractures,where cricothyroidotomy may
cause further
damage or result in complete loss of the airway.
-
8/7/2019 Emergency Airway Access
28/28