Embed Size (px)
Citation preview
Emergencies in Hematology
Zwi Berneman
BHS Educational Course
Seminar 4: Supportive Care in Hematology
15 February 2014
Emergencies in Hematology (I)
• Severe anemia: due to bleeding or
hemolysis
• Febrile neutropenia
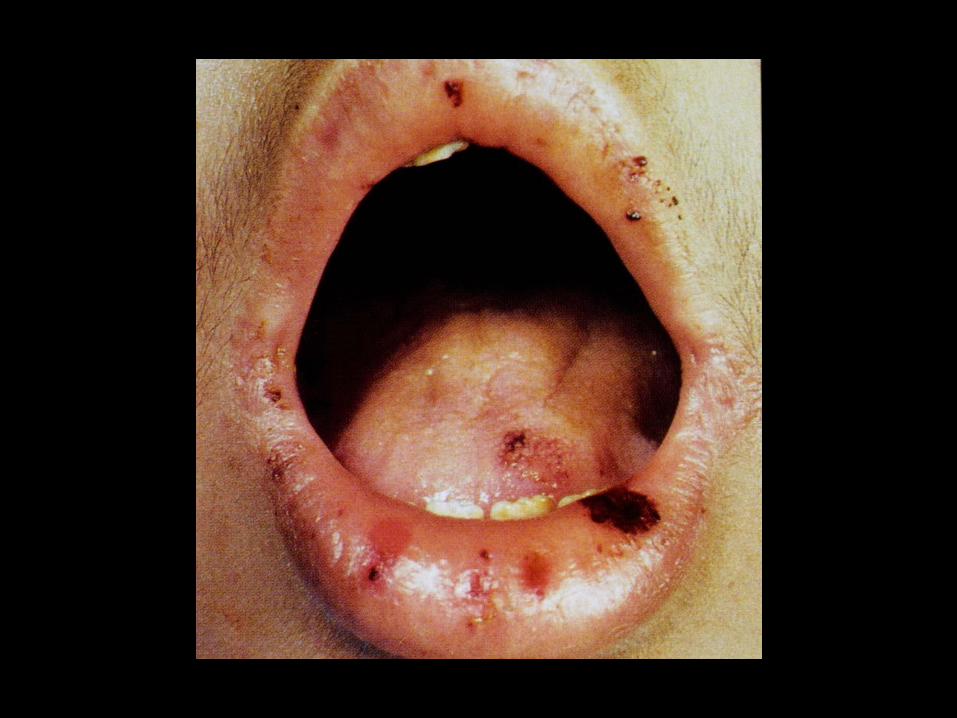
• (Bleeding due to) severe thrombocytopenia
• (Bleeding due to) clotting disorders


Thrombocytopenia
TRC < 140 x 109/l; danger if < 10 (-20) x 109/l TRC transfusion (also TRC transfusion if trombocytopenia > 10 x 109/l and overt bleeding).
Diagnosis:
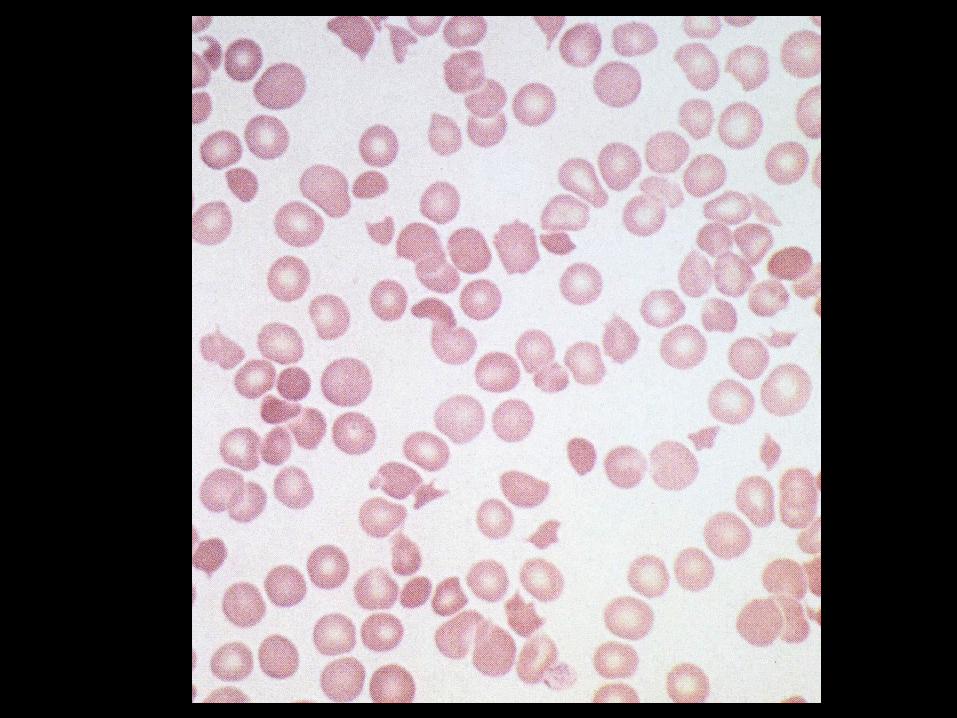
• Peripheral blood: MPV ? Other anomalies? (RBC, WBC?); schistocytes (≥0.5-1%): TTP/HUS or DIC?
• Clotting: APTT, PT, fibrinogen, D-dimers (DIC?)
• Bleeding time not necessary.
• Bone marrow: peripheral or central origin of thrombocytopenia?
• (Auto-antibodies: ANF, anti-CCP, …; TRC antibodies not in current use anymore).
Thrombotic thrombocytopenic purpura (TTP)(/Hemolytic uremic syndrome (HUS))
Pathology (pentade): microangiopathic hemolytic anemia; thrombocytopenia; neurologic abnormalities; renal failure; fever.
TTP(/HUS): clinical diagnosis; requires only thrombocytopenia and microangiopathic hemolytic anemia.
Disseminated intravascular coagulation (DIC): usually not at start of TTP/HUS (APTT, PT, fibrinogen usually not disturbed in a major way at start of TTP/HUS).
Differential diagnosis of TTP/HUS, DIC, HELLP syndrome and postpartum renal failure difficult in obstetric circumstances.
TTP (/ HUS)Etiology:
• Severe (<10% activity) ADAMTS13 deficiency
• Typical or acute diarrheal HUS: associated with
enterotoxicogenic E. coli or Shiga toxin-producing E.
coli (STEC-HUS) – in children
• Atypical HUS: mutation in complement.
Therapy in the acute setting:
• Plasmapheresis: urgent, especially if neurological
symptoms; do not wait for the results of ADAMTS13
levels!
• According to some: preferably no thrombocyte
transfusions, unless bleeding or invasive procedure.
Disseminated intravascular coagulation (DIC)
No primary disease entity, with usually a
demonstrable etiology.
Clinical presentation (1):
• Bleeding: generalized, unexplained
• Renal failure
• Hypoxia
• Neurological features (CNS bleeding,
thrombosis).
DIC
Clinical presentation (2)
Variants with thrombosis:
• Trousseau syndrome: recurrent thrombosis
(venous and arterial) – (hidden)
malignancy?
• Purpura fulminans : (cutaneous) DIC +
necrosis.
DIC
Diagnosis
• APTT usually (can be normaal)
• PT usually disturbed (INR ) (can be normal)
• Fibrinogen or decreasing
• D-dimers +
• Thrombocytes
• RBC fragmentation – schistocytes (50-60% of
cases)
DIC
Etiology
• Septicemia (Gram- > Gram+)
• Neoplasia: procoagulant substance
• Obstetric complications (placenta previa, abruptio
placentae, mors in utero, amniotic fluid embolism,
abortus)
Differential diagnosis with HELLP syndrome:
hemolysis, elevated liver tests, low platelets ((pre)-
eclampsia).
• Other: trauma, peritoneovenous shunt, hemangioma,
pancreatitis, heat stroke, aneurisma, snake bites.
DIC – Treatment (1)
Treat the cause; treat also hypotension, hypoxia,
hypovolemia, acid-base and electrolyte
disturbances.
• DIC with bleeding:
– Freshly frozen plasma (FFP)
– TRC transfusions (check increase in TRC count)
– (Antithrombin (III))
– Heparin: controversial; only as last resort if nothing
else helps.
DIC – Treatment (2)
DIC with thrombosis: heparin
Trousseau syndrome
Purpura fulminans
Mors in utero
Amniotic fuid embolism
Emergencies in Hematology (II)
• Hypercalcemia (myeloma, lymphoma)
• Spinal cord compression (myeloma,
lymphoma)
• Obstructive nephro-uropathy (lymphoma)
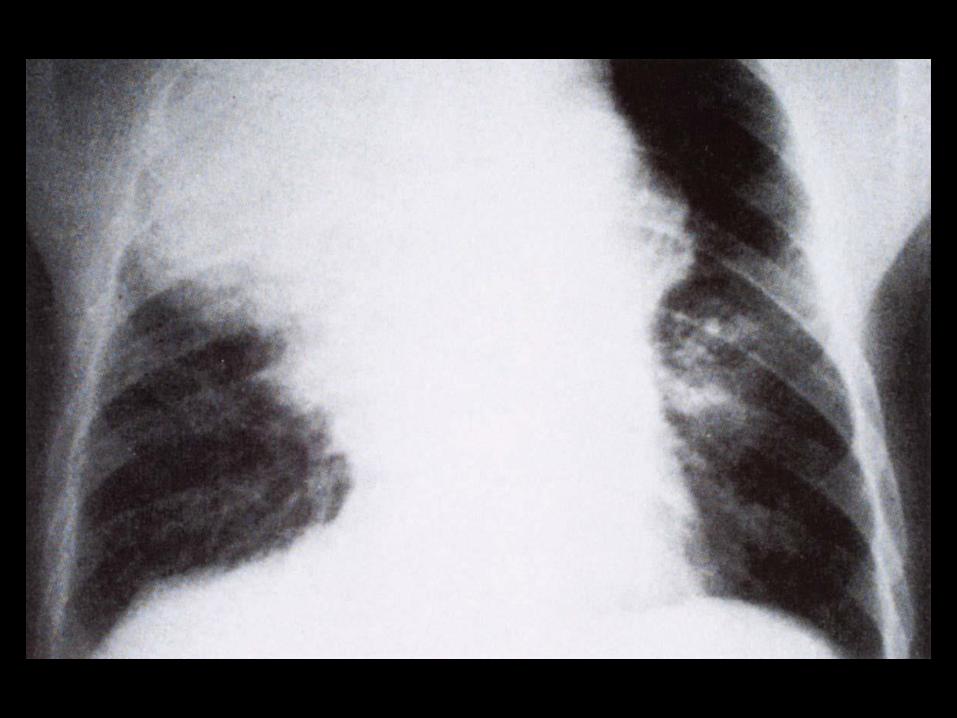
• Malignant pericardial effusion (lymphoma,
acute leukemia).
• Vena cava superior syndrome (lymphoma)

Emergencies in Hematology (III)
• Hyperviscosity syndrome:
– paraprotein (Waldenström’s macroglobulinemia, myeloma)
– RBC (polycythemia vera)
– WBC (leukostasis)
Hyperviscosity syndrome
• Waldenström’s macroglobulinemia
(lymphoplasmocytic lymphoma with IgM
hypersecretion) >> IgA myeloma > IgG myeloma
• Symptoms: visual, neurological, cardial, bleeding.
• Eye fundus examination: “linked sausage effect”of the retinal veins, retinal bleeding, exsudation.
• Treatment: plasmapheresis in symptomatic
hyperviscosity; chemotherapy
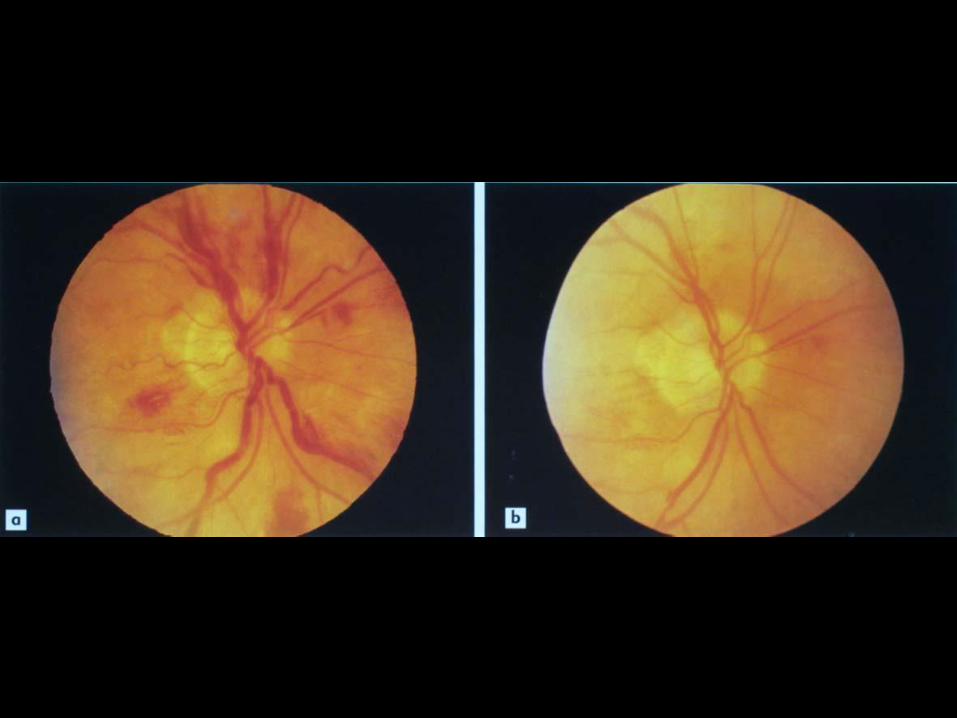
Leukostasis
(symptomatic hyperleukocytosis)
Hyperleukocytosis (WBC > 50-100x109/L) with
respiratory and/or neurological distress.
Covers 2 pathological processes:
• Organ dysfunction due to hyperviscosity and
tissue hypoxia caused by hyperleukocytosis
• Proliferation of leukemic cells through blood
vessel endothelium, formation of tumors and
secundary bleeding.
Frequency: AML, CML-BC > CML-CP, ALL>CLL
Leukostasis
Occurrence:
• Lungs > brain > liver, kidneys, genito-urinary tract
• In acute leukemia, CML-BC: WBC > (50) -100 x 109/L
• In CML-CP: > 300 x 109/L
• In CLL: > 400-800 x 109/L.
Diagnosis: eye fundus examination.
If left untreated: 1-wk mortality rate 20-40%
Leukostasis: Treatment
• Prompt institution of (induction) chemotherapy
• Patients who must have induction chemotherapy delayed:
– Asymptomatic hyperleukocytosis: hydroxyurea 50-100 mg/kg/day (eg. 2-4 g/12 hr) – reduces WBC by 50-80% within 24-48 hr
– Symptomatic hyperleukocytosis: hydroxyurea + leukapheresis ; per leukapheresis: reduction of WBC with @ 30%; NOT in acute promyelocytic leukemia. [Conflicting data of effect of leukapheresis on early mortality not recommended as routine treatment].
• Delaying RBC transfusions; TRC transfusions during leuphapheresis; prevention & treatment of tumor lysis syndrome, DIC and renal damage.
Emergencies in Hematology (IV)
Tumor lysis syndrome
Rapid lysis of tumoral cells with release of intracellular phosphate, potassium and uric acid.
Potential consequences:
• hyperuricemia (nephropathy, gout)
• hyperkaliemia (cardiac dysrythmia)
• hyperphosphatemia (hypocalcemia, progressive renal failure)
• hypocalcemia (muscle spasms, cardiac dysrythmia).
Tumor lysis syndrome
Treatment and prevention:
• rasburicase (Fasturtec): recombinant urate
oxidase
• allopurinol
• correction of electrolyte anomalies
• (Early dialysis, if needed).
Illustrations from:
AV Hoffbrand, JE Pettit. Color Atlas of
Hematology. London: Mosby, 3rd edition,
2000