Embed Size (px)
Citation preview

�P
Embolization as First-Line Therapy forDiverticulosis-Related Massive LowerGastrointestinal Bleeding: EvidenceFrom a Meta-analysisAmit Khanna, M.D., M.P.H., Steven J. Ognibene, M.D., Leonidas G. Koniaris, M.D.
The study goal was to determine which etiologies of lower gastrointestinal bleeding (LGIB) may bestbe treated with superselective embolization. A meta-analysis was undertaken of 25 identified publicationsreporting the use of embolization and an unpublished series of 12 consecutive patients with LGIB fromthe authors’ institution. Six published series and the authors’ series met selection criteria for furtheranalysis. Multiple regression analysis demonstrated no significant difference in pooled outcomes whenvarying the included study, age, or embolization method on the outcome of rebleeding. The pooledodds ratio for arteriovenous dysplastic lesions and other diseases was 3.53 compared with rebleedingafter localization and embolization for diverticular disease (95% confidence interval odds ratio, 1.33,9.41; P � 0.01]. Embolization for diverticular bleeding was successful in 85% of patients. In contrast,rebleeding after embolization for nondiverticular bleeding occurred in greater than 40% of patients andover a more protracted period. Embolization for LGIB is most effective for the treatment of diverticularbleeding. Caution should be used when applying embolization therapy for nondiverticular causes due tothe considerably higher associated failure rate. An inpatient observation period of 2 days is suggestedfollowing embolization for diverticular bleeding. (J GASTROINTEST SURG 2005;9:343–352) � 2005 TheSociety for Surgery of the Alimentary Tract
KEY WORDS: Diverticulosis, colon, arteriovenous abnormality, lower gastrointestinal bleeding
Massive lower gastrointestinal bleeding (LGIB) asdefined as the requirement of greater than 6 units ofpacked red blood cells within a 24-hour period pres-ents a diagnostic and therapeutic challenge. LGIBhas an estimated annual incidence rate of 20.4 per100,000, with an overall mortality rate of about 10%.1In the majority of patients, the causes of LGIB areeither erosion of a vessel into a colonic diverticulumor an arteriovenous dysplastic lesion (AVD). Lesscommon etiologies of LGIB include inflammatorybowel disease, neoplasia, colitis, postprocedural com-plications, rectal trauma, and solitary rectal ulcer.2Localization of the bleeding source is difficult, largelydue to the intermittent nature of the hemorrhage.Multiple procedures over many days may be requiredto diagnose the site of bleeding, and failure rates areas high as 20% are encountered even in specializedcenters with high-volume admissions of LGIB.3Once localization of bleeding is accomplished, seg-
mental colectomy or subtotal colectomy has been
2005 The Society for Surgery of the Alimentary Tractublished by Elsevier Inc.
the standard therapy for both benign and malignantcauses of massive or chronic LGIB, even though suchprocedures are associated with a 4- to 6-week con-valescence period and substantial rates of severemorbidity and mortality.4,5 Increasingly, however,superselective angiographic embolization is beingused to treat LGIB from benign sources.6–29 To date,the body of literature of superselective embolizationfor LGIB has been composed of small retrospectiveinstitutional case series. Here, we report an analysisof individual case level data of both unpublishedseries from our institution and the published experi-ence, with the purpose of providing a more rigorousevaluation of its overall efficacy and to further defineindications for superselective embolization in thetreatment of LGIB. We present a systematic reviewof the published literature using the techniques ofmeta-analysis to determine the pooled odds of re-bleeding within 30 days in diverticular versus nondi-verticular sources of massive LGIB.
From the Department of Surgery (A.K., S.J.O.), University of Rochester School of Medicine, Rochester, New York; and The Dewitt DaughtryFamily Department of Surgery (L.G.K.), University of Miami School of Medicine, Miami, Florida.Reprint requests: Leonidas G. Koniaris, M.D., F.A.C.S., The Alan Livingstone Chair in Surgical Oncology, 3550 Sylvester ComprehensiveCancer Center (310T), 1475 NW 12th Avenue, Miami, FL 33136. e-mail: [email protected]
1091-255X/05/$—see front matterdoi:10.1016/j.gassur.2004.09.039 343

Journal ofGastrointestinal Surgery344 Khanna et al.
MATERIAL AND METHODSInstitutional Series
All patients at the Strong Memorial Hospital(Rochester, NY) undergoing attempted embolizationfor lower gastrointestinal (GI) hemorrhage fromNovember 1999 throughDecember 2001 were retro-spectively reviewed. Institutional review board ap-proval and human subject training was completed.
Literature Review
The Ovid (Ovid Technologies, New York, NY)andMEDLINE search engines were used to examineboth PubMed and The Cochrane Library. The fol-lowing phrases were used for the search: embolization,angiography directed, catheter directed embolization, selec-tive embolization, super-selective angiography, LGIB, andinterventional management of LGIB. The bibliogra-phies of the identified papers were examined to iden-tify any additional trials. Finally, academic surgeonsin Rochester, NY, were queried for other trials thatmay have been omitted.
Inclusion and Exclusion Criteria
All case series of patients presenting with massiveLGIB (�6 units packed red blood cells in 24 hoursor transfusion-dependent hypotension with a systolicblood pressure �90 mm Hg) treated with both angi-ography and attempted embolization were evaluated
for subsequent analysis. Case series for further evalua-tion were limited to those reports where 10 or morepatients were included and greater than 6 units ofblood was required to replace that lost on bleeding ortransfusion-dependent hypotension was noted. Eachstudy was then independently evaluated by two re-viewers for data quality and to determine whetherindividual case data could be extracted from themanuscript. Individual case data extracted included:age (age�60 versus�60 years), disease process (AVDand other versus diverticulosis), rebleeding within 30days of treatment, type of embolic agents used (micro-coil use versus no microcoil use), repeat operation,postembolization ischemia, and duration of follow-up. Individual patients were excluded from furtheranalysis if either a malignancy was identified as theetiology of bleeding before attempted embolizationor vasopressin without vessel embolization was at-tempted. If multiple sites of bleeding were embolizedand rebleeding occurred, it was assumed to be fromthe LGIB source. Twelve articles were identified forfurther analysis and reviewed for data quality andextractability. Of these 12 studies, 6 studies were ex-cluded due to an inability to extract individual patientoutcomes, leaving a total of 6 series (plus our unpub-lished series) that fulfilled selection criteria (Fig. 1).
Data Extraction
Two reviewers blinded to journal, authors, andpublication dates performed independent extraction
N=26 (25 Published reports and unpublished institutional series
N=1 (Excludedvasopressin alone)
N=12 (Studies with samplesize greater of equal to 10)
N=13 (Excluded studies withsample size less than 10)
N=7 (Adequate data extractabilityand outcome reports)
N=5 (Excluded inadequate dataextractability and outcome reports)
N=25 (Embolizationused in therapy)
Fig. 1. Study flow and selection criteria. Twenty-five studies were identified in the published literatureafter systematic search. An additional unpublished series was also identified. One study was excluded onthe basis of use of vasopressin alone, 13 studies were excluded due to lack of sample size, and an additional7 studies were excluded based on inadequate individual data reporting. A total of seven studies fulfilledselection criteria for analysis (six published and one unpublished series).

Vol. 9, No. 32005 Embolization for Diverticulosis-related Lower GI Bleed 345
and assessment of study quality. Discrepancies wereresolved by consensus after discussion.
Statistical Analyses
Based on a priori criteria, the primary comparisonwas rebleeding rate at 30 days after successful emboli-zation in patients with diverticulosis-related bleedingversus AVD-related and other causes of LGIB, whichincluded ulcers of the lower GI tract and postpro-cedure bleeding. Studies were assessed for homoge-neity, both qualitatively and quantitatively. Giventhat the studies were nonrandomized trials, interstudyand intrastudy heterogeneity was anticipated. There-fore, both fixed- and random-effectsmodels were usedto evaluate the dichotomous outcomes (rebleedingwithin 30 days versus no rebleeding within 30 days)of the pooled studies. Multiple logistic regressionanalysis was first applied to explore heterogeneitypresent in the pooled analysis by evaluating potentialcovariates that were predictive of rebleeding within30 days of embolization (SAS; SAS Institute Inc.,Cary, NC), using combined data from the selectedstudies. The procedure PROC LOGISTIC (SAS In-stitute Inc.) was used. The examined covariatesincluded individual study (to determine interstudycorrelation), age (�60 versus�60 years), type of em-bolic agents employed (microcoil use or not), anddisease process (AVD and other causes versus diver-ticulosis). Odds ratios were calculated as the summarymeasures of effect for each study and the pooledanalysis.Meta-analysis using a random-effects model was
first conducted on the data set to estimate the effectof disease process on the outcome of rebleedingwithin 30 days of embolization given the anticipatedheterogeneity present in the pooled analysis. Afixed-effects model was also used to evaluate the ro-bustness of the pooled analysis. For each includedstudy, the odds ratio estimate and its standard errorwere calculated. A pooled odds ratio estimate wasthen calculated by combining individual odds ratiosusing the inverse variance-weighted method (RevMan4.2 orMetaview statistical package).30 Sensitivityanalyses were performed in jackknife fashion by seri-ally omitting each study and analyzing its effect onthe summary statistic. A funnel plot was alsoconstructed to determine the influence of possiblepublication bias.
RESULTSUnpublished Series
All patients at the Strong Memorial Hospital(Rochester, NY) undergoing attempted embolization
for lower GI hemorrhage from November 1999through December 2001 were retrospectively re-viewed. Twelve patients (6 men and 6 women; agerange, 38-81 years; average age, 67 years) were stud-ied. Causes of bleeding were diverticular bleeding(n � 6), rectal ulcer (n � 2), cecal ulcer (n � 1),jejunal ulcer (n � 1), and postpolypectomy bleeding(n � 1). The average follow-up period was 5.4months.In this patient series, angiographic localization and
superselective embolization of bleeding resulted inimmediate control and cessation of hemorrhage in 11of 12 patients (92%). In one patient, embolizationwas unsuccessful and emergent sigmoid resection wasrequired for continued diverticular bleeding. In fourpatients with various underlying pathologies, therewas short-term success only; these patients re-bledand three (75%) eventually required surgery. Thefourth patient underwent a second embolization withgood result. Long-term success was defined as theabsence of surgical intervention for at least 30 days.No recurrent bleeders after 30 days were identified inthis cohort. In this series, 7 of 12 patients achievedgreater than 1-year median follow-up without evi-dence of rebleeding. Of note, no clinically significantinstances of postembolization ischemia occurred. Inaddition, no postprocedural instances of acute renalfailure were observed. Table 1 summarizes this insti-tutional experience.
Published Series
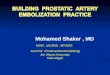
A systematic review of the literature was under-taken to identify the published experience using em-bolization in the treatment of LGIB as described inMaterial and Methods. Overall, 25 studies publishedfrom 1977 to 2002 were identified.4–29 These aresummarized in Table 2. The mean patient numberin these series was 12, with a range of 2–35. Themedian rebleeding rate for LGIB at 30 days postem-bolization was 14%, with a range from 0% to 75%.The most commonly observed complications afterrebleeding were intestinal ischemia, in a reportedrange from 0% to 33%, and reoperation, with a re-ported range from 0% to 50%. The time to rebleed-ing after successful embolization varied widely acrossstudies, with a range of 1–300 days postembolization.In reviewing case series after 1980, the averagenumber of days to rebleeding was 4.0 � 6.1, with75% of rebleeding occurring within 3.5 days of suc-cessful localization and embolization.Tests for heterogeneity of the pooled analysis were
significant (P � 0.01) and therefore the followingcovariates were examined using multiple regression:age, use of microcoils, and disease type on the re-maining six studies. No significant difference was

Journal ofGastrointestinal Surgery346 Khanna et al.
Table 1. Unpublished institutional series showing outcomes of superselective embolization for lowergastrointestinal bleeding
Patient Past medical Microcoils Rebleeding Type ofage/gender history Disease Site used within 30 days resection Follow-up
54/M Patient Cecal ulcer Right colon Yes No 6 moanticoagulated
76/F Patient Rectal ulcer Rectal Yes No 9 moanticoagulated
65/M No Diverticulosis Right colon No Yes Segmental R Surgery(9 days later) 9 days later
72/M Patient Cecum, Right colon Yes Yes (3 days) Segmental R Surgeryanticoagulated postpolypectomy 3 days later
bleeding61/M Renal disease Jejunum Jejunal Yes Yes 3 mo,
reembolized66/F No Rectum Rectal Yes No 4 mo53/F No Rectal ulcer Rectal No Yes Unknown Surgery
(10 days later) 2 wk later81/F No Diverticulosis Left colon No Yes Segmental Surgery
(within 1 day) sigmoid81/F Patient Diverticulosis Left colon Yes No 8 mo
anticoagulated77/M No Diverticulosis Right colon Yes No 6 mo77/F No Diverticulosis Left colon Yes No NA38/M No Diverticulosis Right colon Yes No 2 mo
identified when varying either age or embolizationtechnique on the outcome of rebleeding. Disease typewas significant (P� 0.01), predicting rebleeding ratesat 30 days postembolization (Table 3).The primary outcome variable rebleeding at 30
days postembolization forAVDandother diseaseswasevaluated using a random-effects model. This yieldeda pooled odds ratio for rebleeding at 30 days aftersuccessful localization and embolization for AVDsand other diseases of 3.53 (95% confidence interval,1.33–9.41; P � 0.01) compared with bleeding dueto diverticular disease. When using the fixed-effectsmodel, the pooled odds ratio was calculated on sixavailable studies and yielded a pooled odds ratio of3.52 (95% confidence interval, 1.35–9.16; P � 0.01],suggesting an absolute risk reduction of 62% for di-verticulosis-associated bleeding (Fig. 2).
Sensitivity Analyses
Further analyses of the trials by serially omittingeach trial did not substantially alter the summarystatistic. Each study was analyzed against the studyby Uflacker et al.23 to determine if any one study in-fluenced the data significantly. No individual studywhen compared to the reference study by Uflackeret al.23 achieved significance. In addition, employingstudy used as a covariate in the regression model alsofailed to achieve significance (Table 3).
In addition, pooled analysis of the seven studiesusing a fixed-effects model did not differ significantlyin outcome compared with the random-effects model(Fig. 3). A funnel plot was next constructed with thepooled data to examine for possible publication bias(Fig. 4). The plot failed to reveal major asymmetry, butpublication bias cannot be ruled out completely fromthis test alone.
Time to Rebleeding
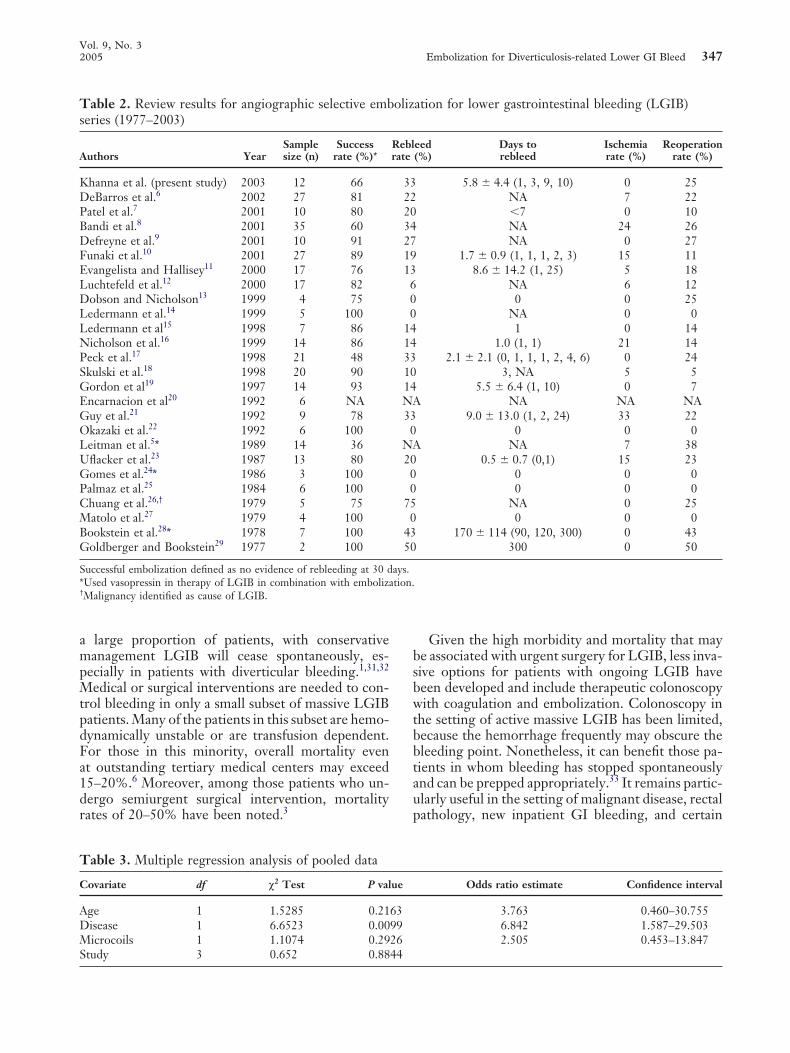
Given the dramatic difference between diverticularand nondiverticular sources of bleeding based on themeta-analysis, we next compared the time to rebleed-ing. Using Kaplan-Meier statistics, time-to-re-bleeding plots were generated using the available datafrom the six included studies and our own case series.As shown (Fig. 5), an overall failure rate of approxi-mately 15% was noted for diverticular bleeding com-paredwith an overall failure rate approaching 45% forthe non–diverticular-cause group. Of note, failuresin thediverticular groupalso appeared tooccur earlier,with infrequent failures being noted after 2 days. Incontrast, a high failure rate persisted in the nondi-verticular group even at 5 days after successfulembolization.
DISCUSSION
LGIB accounts for a substantial number of hospitaladmissions to both medical and surgical services. In
Vol. 9, No. 32005 Embolization for Diverticulosis-related Lower GI Bleed 347
Table 2. Review results for angiographic selective embolization for lower gastrointestinal bleeding (LGIB)series (1977–2003)
Sample Success Rebleed Days to Ischemia ReoperationAuthors Year size (n) rate (%)* rate (%) rebleed rate (%) rate (%)
Khanna et al. (present study) 2003 12 66 33 5.8 � 4.4 (1, 3, 9, 10) 0 25DeBarros et al.6 2002 27 81 22 NA 7 22Patel et al.7 2001 10 80 20 �7 0 10Bandi et al.8 2001 35 60 34 NA 24 26Defreyne et al.9 2001 10 91 27 NA 0 27Funaki et al.10 2001 27 89 19 1.7 � 0.9 (1, 1, 1, 2, 3) 15 11Evangelista and Hallisey11 2000 17 76 13 8.6 � 14.2 (1, 25) 5 18Luchtefeld et al.12 2000 17 82 6 NA 6 12Dobson and Nicholson13 1999 4 75 0 0 0 25Ledermann et al.14 1999 5 100 0 NA 0 0Ledermann et al15 1998 7 86 14 1 0 14Nicholson et al.16 1999 14 86 14 1.0 (1, 1) 21 14Peck et al.17 1998 21 48 33 2.1 � 2.1 (0, 1, 1, 1, 2, 4, 6) 0 24Skulski et al.18 1998 20 90 10 3, NA 5 5Gordon et al19 1997 14 93 14 5.5 � 6.4 (1, 10) 0 7Encarnacion et al20 1992 6 NA NA NA NA NAGuy et al.21 1992 9 78 33 9.0 � 13.0 (1, 2, 24) 33 22Okazaki et al.22 1992 6 100 0 0 0 0Leitman et al.5* 1989 14 36 NA NA 7 38Uflacker et al.23 1987 13 80 20 0.5 � 0.7 (0,1) 15 23Gomes et al.24* 1986 3 100 0 0 0 0Palmaz et al.25 1984 6 100 0 0 0 0Chuang et al.26,† 1979 5 75 75 NA 0 25Matolo et al.27 1979 4 100 0 0 0 0Bookstein et al.28* 1978 7 100 43 170 � 114 (90, 120, 300) 0 43Goldberger and Bookstein29 1977 2 100 50 300 0 50
Successful embolization defined as no evidence of rebleeding at 30 days.*Used vasopressin in therapy of LGIB in combination with embolization.†Malignancy identified as cause of LGIB.
a large proportion of patients, with conservativemanagement LGIB will cease spontaneously, es-pecially in patients with diverticular bleeding.1,31,32Medical or surgical interventions are needed to con-trol bleeding in only a small subset of massive LGIBpatients.Many of the patients in this subset are hemo-dynamically unstable or are transfusion dependent.For those in this minority, overall mortality evenat outstanding tertiary medical centers may exceed15–20%.6 Moreover, among those patients who un-dergo semiurgent surgical intervention, mortalityrates of 20–50% have been noted.3
Given the high morbidity and mortality that maybe associated with urgent surgery for LGIB, less inva-sive options for patients with ongoing LGIB havebeen developed and include therapeutic colonoscopywith coagulation and embolization. Colonoscopy inthe setting of active massive LGIB has been limited,because the hemorrhage frequently may obscure thebleeding point. Nonetheless, it can benefit those pa-tients in whom bleeding has stopped spontaneouslyand can be prepped appropriately.33 It remains partic-ularly useful in the setting of malignant disease, rectalpathology, new inpatient GI bleeding, and certain
Table 3. Multiple regression analysis of pooled data
Covariate df χ2 Test P value Odds ratio estimate Confidence interval
Age 1 1.5285 0.2163 3.763 0.460–30.755Disease 1 6.6523 0.0099 6.842 1.587–29.503Microcoils 1 1.1074 0.2926 2.505 0.453–13.847Study 3 0.652 0.8844

Journal ofGastrointestinal Surgery348 Khanna et al.
Review:Comparison:Outcome:
Study OR (random) Weight OR (random)or sub-category
New review01 Rebleeding Diverticular versus AVM01 Rebleeding Rates following Superselective Embolization
95% Cl % 95% Cl
DebarrosDufreyneEvangelistaNicholsonPeckUflackerUnpublished
Total (95% Cl)Total events: 20 (AVM), 9 (Diverticular)Test for heterogeneity: Chi2 = 2.19, df = 6 (P = 0.90), 2 = 0%Test for overall effect: Z = 2.52 (P = 0.01)
0.1 0.2 0.5 1 2 5 10
Favors treatment Favors control
20.498.14
13.809.66
18.2811.9917.64
100.00
9.50 [1.09, 82.72]3.67 [0.12, 113.73]3.60 [0.26, 50.33]9.00 [0.39, 210.39]2.50 [0.25, 24.72]2.67 [0.16, 45.14]1.13 [0.11, 11.60]
3.53 [1.33, 9.41]
Fig. 2. Forest plot and pooled results of random-effects model. Pooled analysis of the seven studiesusing a random-effects model to adjust for heterogeneity between studies demonstrates a significantdifference in rebleeding rate by etiology of lower gastrointestinal bleeding.
cases of slower but persistent LGIB such as may occurfrom ischemia or infectious colitis.2,31,32Angiographic diagnosis and treatment of LGIB
have evolved since the early 1970s, when the tech-nique was first described in the treatment of GIbleeding. Early attempts at angiographic control usedselective infusion of vasopressin. The use of selectivevasoconstrictive agent infusion was associated with
high recurrence rates and complications of isch-emia, particularly of the GI tract, however.34,35Subsequently, improved microcatheters that allowedselective cannulation of secondary vessels and emboli-zation agents such as PVA (polyvinyl alcohol) andmetal coils were used with much greater success totreat a wide variety of clinical scenarios. Such inter-ventions in LGIB were complicated by failure to
Review:Comparison:Outcome:
Study OR (fixed) Weight OR (fixed)or sub-category
New review01 Rebleeding Diverticular versus AVM01 Rebleeding Rates following Superselective Embolization
95% Cl % 95% Cl
DebarrosDufreyneEvangelistaNicholsonPeckUflackerUnpublished
Total (95% Cl)Total events: 20 (AVM/other), 9 (Diverticular)Test for heterogeneity: Chi2 = 2.19, df = 6 (P = 0.90), 2 = 0%Test for overall effect: Z = 2.58 (P = 0.010)
0.1 0.2 0.5 1 2 5 10
Favors treatment Favors control
9.658.14
12.777.46
20.0313.0228.94
100.00
9.50 [1.09, 82.72]3.67 [0.12, 113.73]3.60 [0.26, 50.33]9.00 [0.39, 210.39]2.50 [0.25, 24.72]2.67 [0.16, 45.14]1.13 [0.11, 11.60]
3.52 [1.35, 9.16]
Fig. 3. Forest plot and pooled results of fixed-effects model. Pooled analysis of the six studies using afixed-effects model did not differ significantly in outcome compared with the random-effects model.OR � odds ratio. P � 0.05 significance level.
Vol. 9, No. 32005 Embolization for Diverticulosis-related Lower GI Bleed 349
Review:Comparison:Outcome:
New review01 Rebleeding Diverticular versus AVM01 Rebleeding Rates following Superselective Embolization
0.0
0.4
0.8
1.2
1.6
0.1 0.2 0.5 1 2 5 10
SE(log OR)
OR (fixed)
Fig. 4. Funnel plot of pooled data.
control bleeding or associated intestinal ischemia.36Failure of bleeding control in many early reportswas ascribed to embolization proximal to themarginalartery, thus allowing bleeding to propagate via collat-
100
90
80
70
60
500 10 20 30
Days Post Embolization
Fig. 5. Kaplan-Meier analysis of lower gastrointestinal re-bleeding. Time to rebleeding within 30 days of successfulembolization by etiology of bleeding (mean � SE, diverticularversus arteriovenous dysplastic lesions [gray] and other etiolo-gies [black]). Data were derived from all studies that metselection criteria except DeBarros et al.,6 where days to re-bleeding was not reported.
eral intramural arteries. The incidence of ischemiarelated to selective embolization has ranged in thepast decade from 0% to 22%, with fewer than 10%of patients requiring surgical resection for ischemia(see Tables 1 and 2). In the most recent series, theincidence of ischemia has markedly decreased due tothe use of larger-particle PVA or metal coils andincreased experience.7 Notably, few reports of sig-nificant ischemia requiring exploration and resectionhave been reported in any of the included series since1997, suggesting a current rate of significant ischemiaof less than 5%.To date, the overall failure rate of embolization
remains high in some series, and its widespread appli-cation has not been universally achieved.We hypoth-esized that certain etiologies of bleeding would bemore effectively treated by the use of embolizationthan would others.We therefore set out to systemati-cally examine the published literature using the tech-niques of meta-analysis to identify those patients whomight benefit from the use of embolization in thetreatment of LGIB. A thorough review of the pub-lished literature identified 25 articles for subsequentanalysis. We applied selection criteria to these datasets to identify the highest quality studies with com-prehensive individual data reporting. Critical review

Journal ofGastrointestinal Surgery350 Khanna et al.
Massive Lower Gastrointestinal Bleed
Angiography
Diverticular Source Non-Diverticular Source
Amenable to Embolization?
YesNo
Surgery
Embolization
Success(85%)
Fail (15%)
Observe5 Days
Discharge
Consider Embolization*
Semi-electiveSurgery
Success(50%)
Amenable to Embolization?
Diverticular Source
YesNo
Non-Diverticular Source
Fail (50%)
Surgery
Observe2 Days
Fig. 6. Suggested treatment approach algorithm.
of the literature identified six published series and ourinstitutional data set thatwere amenable to subsequentstatistical analysis. Initial examination of these datasets involved exploration of sources of anticipatedheterogeneity between trials by using multiple logis-tic regression analysis and using each study’s data setas a variable. Importantly, no statistically significantdifference based on the covariates of age, microcoiluse, or individual study were found on the outcome ofrebleeding between these studies, strongly suggestingthat the difference in rebleeding rates in diverticularversus nondiverticular bleeding of each study wereconsistent and that subsequent pooled identified dif-ferences were, in fact, valid.The only statistically significant variable identified
by logistic regression was disease process. Emboliza-
tion is demonstrated more effective for diverticularbleeding than other less common pooled pathologies.Meta-analysis of the data set with both random andfixed-effects models demonstrated that diverticularbleeding was three to four times more likely to becontrolled with embolization than other causes ofbleeding. These data suggest, therefore, that emboli-zation is most effective for diverticular bleeding andthat this efficacy is not dependent on the patient’sage or the embolization technique used.Several limitations exist in this meta-analysis pri-
marily because the available data on this techniqueare from small retrospective case series, allowing atotal sample of 103 patients for meta-analysis. Selec-tion bias was possible based on the studies includedin the meta-analysis, particularly because the data

Vol. 9, No. 32005 Embolization for Diverticulosis-related Lower GI Bleed 351
used were from higher-volume centers. Hence, theconclusions made for the success of embolization fordiverticular bleeding may not be those encounteredwhere less expertise exists. Moreover, the studies ex-amined were noncontrolled observational studies andtherefore may include other potential unknown con-founding variables. To address the potential of biasin some of the reported studies, a funnel plot wasconstructed and appeared symmetric, suggesting nosignificant evidence of publication bias. However,much debate has focused on the ability of funnelplots in excluding publication bias completely, and itis possible that publication bias was present in theanalysis (see Fig. 4). A sensitivity analysis was alsoundertaken but failed to demonstrate significant dif-ferences in outcomes measures either after serialstudy omission or compared with a single-referencestudy. Again, the techniques of meta-analysis areoften hypothesis generating but can be useful in plan-ning subsequent trials to further elucidate the optimalselection of patients for superselective embolization.Notwithstanding the above limitations of small
sample size and observational design, it is clear thatthe outcomes of our meta-analysis are internally con-sistent. In addition, by using the rigors of meta-analysis to the best available data on this topic, weconclude that superselective embolization has a highinitial success rate at controlling hemorrhage. Thebest available data suggest a control rate exceeding85% at 1 month for diverticular bleeding. The rateof control of bleeding for AVD and other rare causesof benign LGIB is lower, with an overall successrate of less than 55% at 30 days postembolization.These data suggest a controlled randomized studycomparing surgical resection and superselective em-bolization would require a sample size of at least 250patients in each treatment arm to achieve 80% powerwith a significance level of 5%.Based on the results of the meta-analysis, a treat-
ment algorithm is suggested (Fig. 6). All patients,regardless of age, who present with significant LGIBfrom diverticulosis should be considered for superse-lective embolization, if technically feasible. A subset ofthese patientsmay stop on their own, without embolictherapy, but its inclusion in the treatment algorithmfor these patients is associated with a very high overallcontrol rate. Surgery should be reserved for the fewfor whom embolization fails. Overall, 95% of patientswho do not rebleed within 2 days of embolization fordiverticular bleeding are most likely not to requirereintervention. Moreover, according to these data,at least a 2-day observation period for rebleedingfollowing embolization for diverticular bleeding ap-pears to be justified. Importantly, long-term follow-up of these patients has not identified a large late
recurrence rate after 30 days, but this possibilityshould still be entertained. Embolization for AVDand other nondiverticular LGIB may be consideredgiven the low risk of postembolization ischemia; how-ever, a failure rate of 45% may be encountered. Em-bolization in this subset of LGIB patients may bestbe used as a temporary measure to allow bowelpreparation and subsequent semielective alternateprocedure. Alternatively, early consideration for theuse of other therapies following localization maybe considered.
REFERENCES
1. Schuetz A, JauchKW.Lower gastrointestinal bleeding: Ther-apeutic strategies, surgical techniques and results. Langen-becks Arch Surg 2001;386:17–25.
2. Hendrickson RJ, Diaz AA, Salloum R, Koniaris LG. Benignrectal ulcer. Surg Endosc 2003.
3. Vernava AM 3rd,Moore BA, LongoWE, Johnson FE. Lowergastrointestinal bleeding. Dis Colon Rectum 1997;40:846–858.
4. Bokhari M, Vernava AM, Ure T, Longo WE. Diverticularhemorrhage in the elderly—is it well tolerated? Dis ColonRectum 1996;39:191–195.
5. Leitman IM, Paull DE, Shires GT 3rd. Evaluation and man-agement of massive lower gastrointestinal hemorrhage. AnnSurg 1989;209:175–180.
6. DeBarros J, Rosas L, Cohen J, Vignati P, Sardella W, Halli-sey M. The changing paradigm for the treatment of colonichemorrhage: Superselective angiographic embolization. DisColon Rectum 2002;45:802–808.
7. Patel TH, Cordts PR, Abcarian P, Sawyer MA. Will trans-catheter embolotherapy replace surgery in the treatment ofgastrointestinal bleeding? Curr Surg 2001;58:323–327.
8. Bandi R, Shetty PC, Sharma RP, Burke TH, Burke MW,Kastan D. Superselective arterial embolization for the treat-ment of lower gastrointestinal hemorrhage. J Vasc IntervRadiol 2001;12:1399–1405.
9. Defreyne L, Vanlangenhove P, De Vos M, et al. Emboliza-tion as a first approach with endoscopically unmanageableacute nonvariceal gastrointestinal hemorrhage. Radiology2001;218:739–748.
10. FunakiB,Kostelic JK, Lorenz J, et al. Superselectivemicrocoilembolization of colonic hemorrhage. AJR Am J Roentgenol2001;177:829–836.
11. Evangelista PT, Hallisey MJ. Transcatheter embolizationfor acute lower gastrointestinal hemorrhage. J Vasc IntervRadiol 2000;11:601–606.
12. Luchtefeld MA, Senagore AJ, Szomstein M, Fedeson B,Van Erp J, Rupp S. Evaluation of transarterial embolizationfor lower gastrointestinal bleeding. Dis Colon Rectum 2000;43:532–534.
13. Dobson CC, Nicholson AA. Treatment of rectal hemorrhageby coil embolization. Cardiovasc Intervent Radiol 1999;22:143–146.
14. Ledermann HP, Schoch E, Jost R, Zollikofer CL. Emboliza-tion of the vasa recta in acute lower gastrointestinal hemor-rhage: A report of five cases. Cardiovasc Intervent Radiol1999;22:315–320.
15. Ledermann HP, Schoch E, Jost R, Decurtins M, ZollikoferCL. Superselective coil embolization in acute gastrointestinalhemorrhage: Personal experience in 10 patients and reviewof the literature. J Vasc Interv Radiol 1998;9:753–760.

Journal ofGastrointestinal Surgery352 Khanna et al.
16. Nicholson AA, Ettles DF, Hartley JE, et al. Transcathetercoil embolotherapy: A safe and effective option for major col-onic haemorrhage. Gut 1998;43:79–84.
17. Peck DJ, McLoughlin RF, Hughson MN, Rankin RN.Percutaneous embolotherapy of lower gastrointestinal hem-orrhage. J Vasc Interv Radiol 1998;9:747–751.
18. Skulski R, Snider JM, Buzzard CJ, Ling FS, Mendelsohn AM.Transcatheter closure of a patent foramen ovale followingmitral valve replacement. Ann Thorac Surg 1999;68:582–583.
19. Gordon RL, Ahl KL, Kerlan RK, et al. Selective arterialembolization for the control of lower gastrointestinal bleed-ing. Am J Surg 1997;174:24–28.
20. EncarnacionCE,Kadir S, BeamCA,PayneCS.Gastrointesti-nal bleeding: Treatment with gastrointestinal arterial embo-lization. Radiology 1992;183:505–508.
21. Guy GE, Shetty PC, Sharma RP, Burke MW, Burke TH.Acute lower gastrointestinal hemorrhage: Treatment bysuperselective embolization with polyvinyl alcohol particles.AJR Am J Roentgenol 1992;159:521–526.
22. Okazaki M, Furui S, Higashihara H, Koganemaru F, Sato S,FujimitsuR. Emergent embolotherapy of small intestine hem-orrhage. Gastrointest Radiol 1992;17:223–228.
23. UflackerR.Transcatheter embolization for treatment of acutelower gastrointestinal bleeding. Acta Radiol 1987;28:425–430.
24. Gomes AS, Lois JF, McCoy RD. Angiographic treatmentof gastrointestinal hemorrhage: Comparison of vasopressininfusion and embolization. AJR Am J Roentgenol 1986;146:1031–1037.
25. Palmaz JC, Walter JF, Cho KJ. Therapeutic embolization ofthe small-bowel arteries. Radiology 1984;152:377–382.
26. Chuang VP, Wallace S, Zornoza J, Davis LJ. Transcatheterarterial occlusion in themanagement of rectosigmoidal bleed-ing. Radiology 1979;133:605–609.
27. Matolo NM, Link DP. Selective embolization for control ofgastrointestinal hemorrhage. Am J Surg 1979;138:840–844.
28. Bookstein JJ, Naderi MJ,Walter JF. Transcatheter emboliza-tion for lower gastrointestinal bleeding. Radiology 1978;127:345–349.
29. Goldberger LE, Bookstein JJ. Transcatheter embolization fortreatment of diverticular hemorrhage. Radiology 1977;122:613–617.
30. Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F.Methods for Meta-analysis in Medical Research. London:John Wiley and Sons, 2000.
31. Zuckerman GR, Prakash C. Acute lower intestinal bleeding.Part I: Clinical presentation and diagnosis. GastrointestEndosc 1998;48:606–617.
32. Zuckerman GR, Prakash C. Acute lower intestinal bleeding.Part II: Etiology, therapy, and outcomes. Gastrointest Endosc1999;49:228–238.
33. Jensen DM, Machicado GA, Jutabha R, Kovacs TO. Urgentcolonoscopy for the diagnosis and treatment of severe diverti-cular hemorrhage. N Engl J Med 2000;342:78–82.
34. Browder W, Cerise EJ, Litwin MS. Impact of emergencyangiography in massive lower gastrointestinal bleeding. AnnSurg 1986;204:530–536.
35. Sherman LM, Shenoy SS, Cerra FB. Selective intra-arterialvasopressin: Clinical efficacy and complications. Ann Surg1979;189:298–302.
36. Rosenkrantz H, Bookstein JJ, Rosen RJ, Goff WB 2nd,Healy JF. Postembolic colonic infarction. Radiology 1982;142:47–51.


![Case Report Angiographic Embolization of a Postpartum …downloads.hindawi.com/journals/criog/2013/323781.pdf · 2019-07-31 · cesarean section, or with postpartum bleeding [ ]](https://img.pdfslide.us/doc/110x75/5ed7536860a80d707700c2d6/case-report-angiographic-embolization-of-a-postpartum-2019-07-31-cesarean-section.jpg)















![Diverticulosis%5B1%5D %5BAutosaved%5D[1]](https://img.pdfslide.us/doc/110x75/577d38db1a28ab3a6b989f85/diverticulosis5b15d-5bautosaved5d1.jpg)