Elliott K. Lee MD, FRCP(C) Christopher R. Skinner MD, FRCP(C)
SLEEP MEDICINE: An Overview
Slide 2
Objectives Describe the stages of normal sleep and describe how
normal sleep is regulated by the brain Discuss the usual
classification of sleep disorders Briefly describe the technique of
polysomnography and list the electrical and physiological variables
monitored List and describe the cardinal manifestations of
narcolepsy Define and give examples of parasomnias
Slide 3
Sleep Definition A reversible behavioral state of perceptual
disengagement from and unresponsiveness to the environment, is
restorative and important for the proper functioning of an
organism.
Slide 4
Why Study Sleep? We spend 1/3 of our lives sleeping We spend
1/3 of our lives sleeping 1 in 7 Canadians are not getting enough
sleep (Statistics Canada, 2002) 1 in 7 Canadians are not getting
enough sleep (Statistics Canada, 2002) Severe health consequences -
DEATH! Severe health consequences - DEATH! Sleep deprivation costs
Sleep deprivation costs $150 BILLION/yr in lost $150 BILLION/yr in
lost productivity productivity (Natl Commission on Sleep Disorders,
2003) (Natl Commission on Sleep Disorders, 2003)
Slide 5
THE IMPACT OF SLEEP DEPRIVATION
Slide 6
Challenger Disaster Challenger Disaster 3 Mile Island 3 Mile
Island Chernobyl Chernobyl
Slide 7
Purpose of Sleep Regeneration of Physiological Systems NREM
physical REM - cognitive Activation of Genes in different
stages
Slide 8
Purpose of Sleep Restorative Function Restorative Function
Energy Conservation Energy Conservation Immune Function Regulation
Immune Function Regulation Ontogenetic Hypothesis Ontogenetic
Hypothesis Memory Consolidation Memory Consolidation Protective
Mechanism Protective Mechanism
Slide 9
Gene Activation in Sleep 15,000 transcripts expressed in the
cerebral cortex, about 5% change their expression levels depending
on behavioural state but independently of time of day Half of the
modulated genes increase in wakefulness and half in sleep.
Slide 10
Waking-related transcripts Energy metabolism Excitatory
neurotransmission, transcriptional activation Synaptic potentiation
Memory acquisition Response to cellular stress..
Slide 11
Sleep-related transcripts Brain protein synthesis Synaptic
consolidation/depression Membrane trafficking and maintenance,
including cholesterol metabolism, myelin formation, and synaptic
vesicle turnover
Slide 12
Major Classification Dyssomnias Sleep disorders associated with
mental, neurologic, or other medical disorders Parasomnias Proposed
sleep disorders
Slide 13
ICSD - International Classification of Sleep Disorders
CATEGORIES: INSOMNIAS INSOMNIAS SLEEP RELATED BREATHING DISORDERS
SLEEP RELATED BREATHING DISORDERS HYPERSOMNIAS OF CENTRAL ORIGIN
HYPERSOMNIAS OF CENTRAL ORIGIN CIRCADIAN RHYTHM DISORDERS CIRCADIAN
RHYTHM DISORDERS PARASOMNIAS PARASOMNIAS SLEEP RELATED MOVEMENT
DISORDERS SLEEP RELATED MOVEMENT DISORDERS ISOLATED SYMPTOMS
ISOLATED SYMPTOMS
SLEEP DISORDERS ASSOCIATED WITH MENTAL, NEUROLOGIC, OR OTHER
MEDICAL DISORDERS Psychoses Mood Disorders Anxiety Disorders Panic
Disorders Alcoholism Associated with Neurologic Disorders Cerebral
Degenerative Disorders Dementia Parkinsonism Fatal Familial
Insomnia Sleep-Related Epilepsy Electrical Status Epilepticus of
Sleep Sleep-Related Headaches Associated with Other Medical
Disorders Sleeping Sickness Nocturnal Cardiac Ischemia Chronic
Obstructive Pulmonary Disease Sleep-Related Asthma Sleep-Related
Gastroesophageal Reflux Peptic Ulcer Disease Fibromyalgia
Slide 18
Circadian rhythm sleep disorders Time zone change (jet lag)
syndrome Shift work sleep disorder Irregular sleep-wake pattern
Delayed sleep phase syndrome Advanced sleep phase syndrome
Non24-hour sleepwake disorder Circadian rhythm sleep disorder
NOS
Slide 19
Circadian System
Slide 20
Slide 21
Slide 22
Fellowship training, workload, fatigue and physical stress: a
prospective observational study CMAJ 2004;170(6):965-70 Although
within current PAIROOCOTH and ACGME regulations, the workload of
senior fellows in the Hospital for Sick Childrens PCCU is
physically demanding, allows limited rest and is associated with
sleep deprivation and objective markers of physiologic stress.
Although within current PAIROOCOTH and ACGME regulations, the
workload of senior fellows in the Hospital for Sick Childrens PCCU
is physically demanding, allows limited rest and is associated with
sleep deprivation and objective markers of physiologic stress.
Judged by the number and destinations of its trainees, this is a
highly successful program; however, trainees are unlikely to be
performing optimally. This style of health care delivery is almost
certainly associated with the production of error and adverse
patient outcomes. Judged by the number and destinations of its
trainees, this is a highly successful program; however, trainees
are unlikely to be performing optimally. This style of health care
delivery is almost certainly associated with the production of
error and adverse patient outcomes. Current guidelines and work
practices do not mitigate significant fatigue and physical stress.
Guideline revision and evaluation of other means to reduce the
physical demands on trainees are required if the health care system
wishes to address these challenging issues. Current guidelines and
work practices do not mitigate significant fatigue and physical
stress. Guideline revision and evaluation of other means to reduce
the physical demands on trainees are required if the health care
system wishes to address these challenging issues.
Slide 23
Med Educ. 1994;28:566-572 Lingenfelser et al The effect of
training experience (first- and second-year residents vs third- and
fourth-year) The effect of training experience (first- and
second-year residents vs third- and fourth-year) Examined the
performance on a number of psychomotor tasks of 40 residents in the
off-duty state (6 hours of reported sleep the previous night) and
after 24 hours on call Examined the performance on a number of
psychomotor tasks of 40 residents in the off-duty state (6 hours of
reported sleep the previous night) and after 24 hours on call
Performances on a simulated electrocardiogram, short- term recall
of a list of things to do, and reaction times all deteriorated
after being on call Performances on a simulated electrocardiogram,
short- term recall of a list of things to do, and reaction times
all deteriorated after being on call These post call performance
deficits were similar for junior and senior residents These post
call performance deficits were similar for junior and senior
residents suggesting a lack of adaptation over time to the sleep-
deprived state suggesting a lack of adaptation over time to the
sleep- deprived state
Slide 24
Ann Emerg Med. 1994;24:928-934 Smith-Coggins R ER physicians
found that both completion time in a simulated intubation task and
clinical accuracy in a triage task were worse for night-shift
physicians than for dayshift ER physicians found that both
completion time in a simulated intubation task and clinical
accuracy in a triage task were worse for night-shift physicians
than for dayshift physicians and that performance deteriorated
across night shifts but not across day shifts. physicians and that
performance deteriorated across night shifts but not across day
shifts. Performance deterioration across the night shift likely
results from both insufficient sleep and circadian rhythm
differences. circadian rhythm differences. Performance
deterioration across the night shift likely results from both
insufficient sleep and circadian rhythm differences. circadian
rhythm differences.
What Happens at the Sleep Lab ROMHC: 5 bed clinical lab, 4 bed
research lab ROMHC: 5 bed clinical lab, 4 bed research lab TOH: 15
bed clinical lab, MSLT, MWT TOH: 15 bed clinical lab, MSLT, MWT
STEPS: STEPS: 1) Referral 1) Referral 2) Consultation with a Sleep
Specialist 2) Consultation with a Sleep Specialist 3) Overnight
Sleep Study 3) Overnight Sleep Study 4) Data is Analyzed by RPSGTs
4) Data is Analyzed by RPSGTs 5) Results Appt with a Sleep
Specialist 5) Results Appt with a Sleep Specialist
Slide 33
How Do We Measure Sleep in the Laboratory? EEG brainwaves
(Central & Occipital Leads) EEG brainwaves (Central &
Occipital Leads) EOG eye movements EOG eye movements EMG muscle
tone EMG muscle tone EKG/ECG heart EKG/ECG heart Breathing:
Breathing: 1)Airflow 1)Airflow & 2) Effort: Thoracic &
Abdominal & 2) Effort: Thoracic & Abdominal Blood oxygen
saturation (SaO 2 ) Blood oxygen saturation (SaO 2 ) Snore mic.
Snore mic. Digital AV recording Digital AV recording
Slide 34
Slide 35
Slide 36
Slide 37
Diagnostic Tools Overnight Polysomnogram Multiple Sleep Latency
Test Maintenance of Wakefulness Test Actigraphy Sleep Diaries Sleep
Surveys Epworth Sleep Scale Stanford Sleepiness Rating
Slide 38
Overnight Sleep Study Sleep Architecture Sleep Disordered
Breathing Oxygen Desaturation Periodic Limb Movements Restless
Legs
Slide 39
Multiple Sleep Latency Test MSLT Repeated naps at 2 hour
intervals during the day Measures Normal > 12 minutes
Pathological Sleepiness < 6 minutes Sleep Latency REM Onset
Slide 40
Slide 41
Maintenance of Wakefulness Test MWT Subjects lie in darkened
room in daytime Try to remain awake 40 min version Some use
performance tests Validation and sensitivity not established
Slide 42
Epworth Sleepiness Scale SITUATION CHANCE OF DOZING Sitting and
reading3 Watching TV3 Sitting inactive in a public place (e.g. a
theater or a meeting)3 As a passenger in a car for an hour without
a break3 Lying down to rest in the afternoon when circumstances
permit3 Sitting and taking to someone3 Sitting quietly after a
lunch without alcohol3 In a car, while stopped for a few minutes in
traffic3
Slide 43
Slide 44
STAGES OF SLEEP NREM & REM NREM & REM NREM = N1, N2, N3
NREM = N1, N2, N3 Sleep Cycle Sleep Cycle REM increases as the
night progresses REM increases as the night progresses Changes
across the lifespan Changes across the lifespan
Slide 45
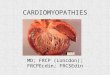
Sleep Histogram RL
Slide 46
Slide 47
Arousal System
Slide 48
NREM SLEEP N1: lightest stage of sleep N1: lightest stage of
sleep (hypnic jerks/sleep starts), dozing N2: Sleep spindles &
K complexes N2: Sleep spindles & K complexes N3 (formerly
stages 3 & 4): deepest most physically restorative stage of
sleep. More difficult to awaken from this stage. Decreases with
age. N3 (formerly stages 3 & 4): deepest most physically
restorative stage of sleep. More difficult to awaken from this
stage. Decreases with age. Breathing regular, heart rate decreases
Breathing regular, heart rate decreases
Slide 49
Non-REM Control
Slide 50
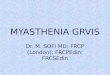
REM Sleep Giant Cells of Pontine Tegmentum (Brain Activation)
Laterodorsal Tegmental Nucleus Pediculopontine Tegmental Nucleus
Subcerulean Nuclei (Atonia and Paralysis) Medial and Descending
Vestibular Nuclei (Phasic Phenomena) Hypothalamic Component
(Autonomic, sexual, neuroendocrine) REM On Neurons REM Off
Neurons
Objectives Describe the stages of normal sleep and describe how
normal sleep is regulated by the brain Discuss the usual
classification of sleep disorders Briefly describe the technique of
polysomnography and list the electrical and physiological variables
monitored List and describe the cardinal manifestations of
narcolepsy Define and give examples of parasomnias