Embed Size (px)
Citation preview
Elizabeth Docteur
European Health Forum Gastein
7 October 2004
Towards High-Performing Health Systems: Challenges and Opportunities for Reform
2
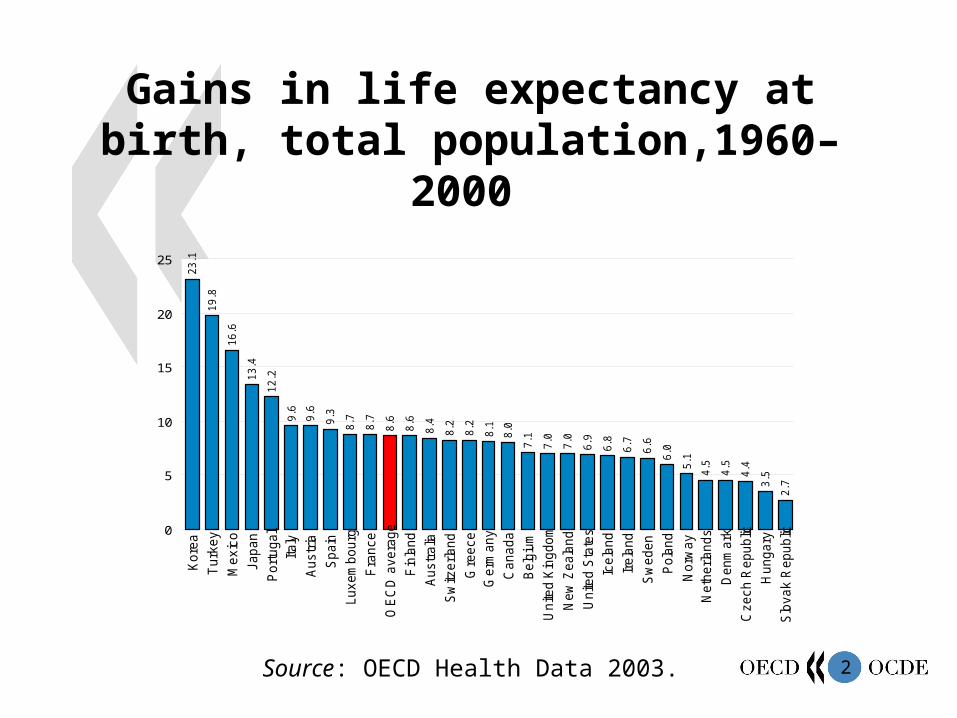
Gains in life expectancy at birth, total population,1960–2000
2.73
.54.44.5
4.55
.16.06
.66.76.86.97.0
7.07.18
.08.18.2
8.28.48.6
8.68.7
8.79.39.6
9.6
12
.213
.4
16
.6
19
.8
23
.1
0
5
10
15
20
25
Slo
vak R
epublic
Hungary
Czech R
epublic
Denm
ark
Neth
erlands
Norw
ay
Pola
nd
Sw
eden
Irela
nd
Icela
nd
Unite
d S
tate
s
New
Zeala
nd
Unite
d K
ingdom
Belg
ium
Canada
Germ
any
Gre
ece
Sw
itzerland
Austr
alia
Fin
land
OE
CD
avera
ge
Fra
nce
Luxem
bourg
Spain
Austr
ia
Italy
Port
ugal
Japan
Mexic
o
Turk
ey
Kore
a
years
Source: OECD Health Data 2003.
3
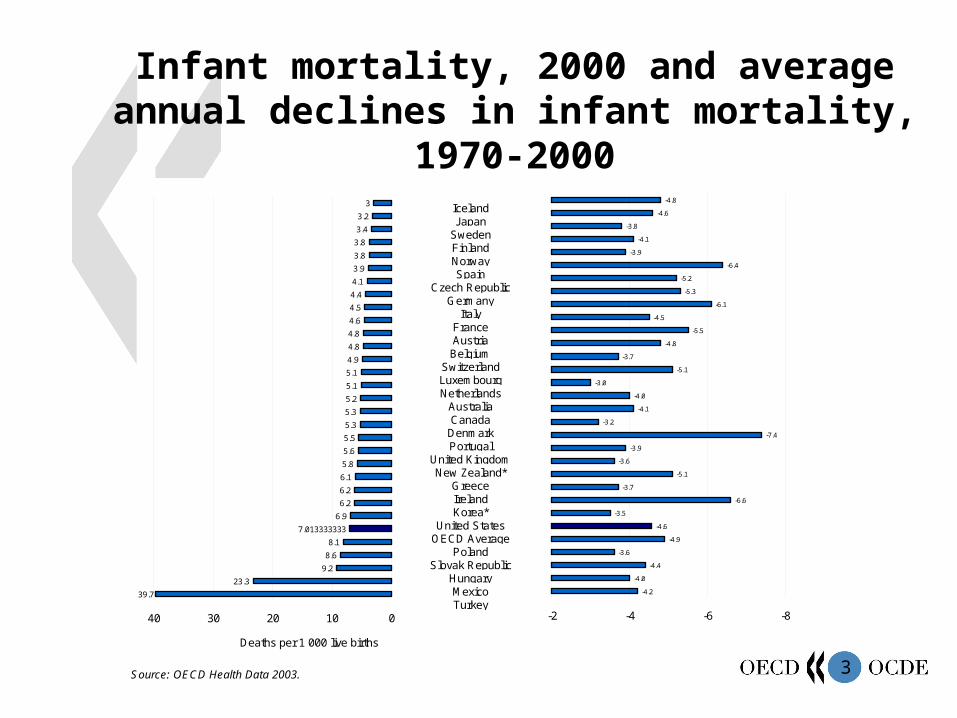
Infant mortality, 2000 and average annual declines in infant mortality, 1970-2000
IcelandJapan
SwedenFinlandNorwaySpain
Czech RepublicGermany
ItalyFranceAustriaBelgium
SwitzerlandLuxembourgNetherlands
AustraliaCanada
DenmarkPortugal
United KingdomNew Zealand*
GreeceIrelandKorea*
United StatesOECD Average
PolandSlovak Republic
HungaryMexicoTurkey
Source: OECD Health Data 2003.
3
3.2
3.4
3.8
3.8
3.9
4.1
4.4
4.5
4.6
4.8
4.8
4.9
5.1
5.1
5.2
5.3
5.3
5.5
5.6
5.8
6.1
6.2
6.2
6.9
7.013333333
8.1
8.6
9.2
23.3
39.7
010203040
-4.8
-4.6
-3.8
-4.1
-3.9
-6.4
-5.2
-5.3
-6.1
-4.5
-5.5
-4.8
-3.7
-5.1
-3.0
-4.0
-4.1
-3.2
-7.4
-3.9
-3.6
-5.1
-3.7
-6.6
-3.5
-4.6
-4.9
-3.6
-4.4
-4.0
-4.2
-8-6-4-2
Deaths per 1 000 live births % change*1999.
4
Factors driving health improvements
Economic expansion and related factors– e.g. increased educational attainment
Improvements in health care and health systems– Advances in medicine and technical capability– Improvements in access to care and health care systems
(e.g., universal coverage attained in most OECD countries)– Successful public health initiatives (vaccination, initiatives
and policies to reduce tobacco consumption)
5
“Health systems are victims of their own success.”
Julio Frenk
Health Minister, MexicoOECD Health Ministerial Meeting, May 2004
6
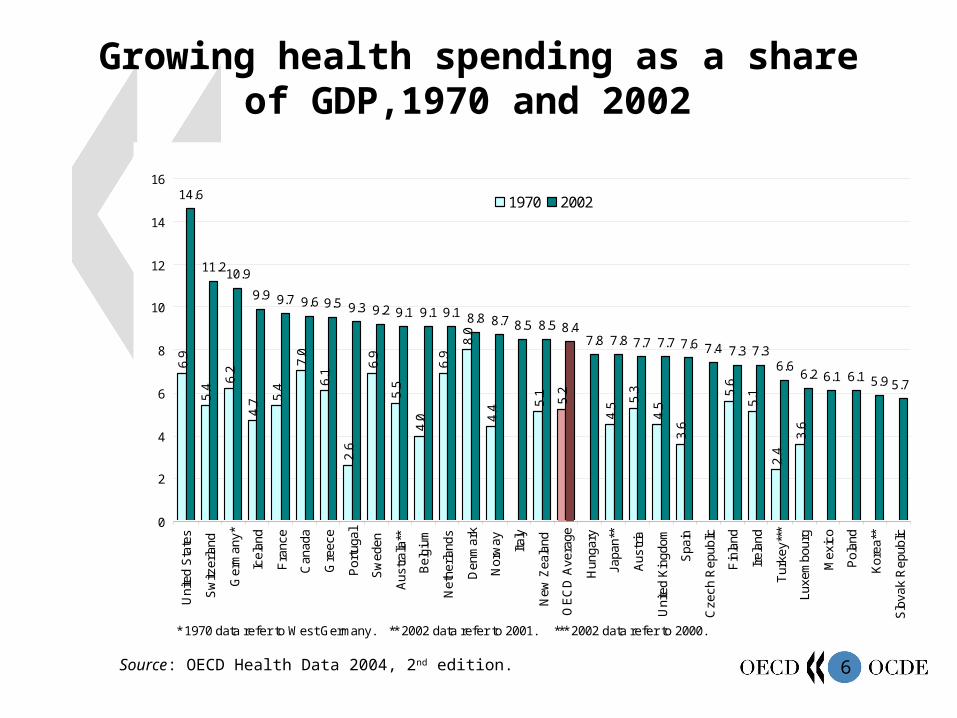
Growing health spending as a share of GDP,1970 and 2002
Source: OECD Health Data 2004, 2nd edition.
6.9
5.4
6.2
4.7 5.
4
7.0
6.1
2.6
6.9
5.5
4.0
6.9
8.0
4.4 5.
1
5.2
4.5 5.
3
4.5
3.6
5.6
5.1
2.4
3.6
14.6
11.210.9
9.9 9.7 9.6 9.5 9.3 9.2 9.1 9.1 9.1 8.8 8.7 8.5 8.5 8.47.8 7.8 7.7 7.7 7.6 7.4 7.3 7.3
6.66.2 6.1 6.1 5.9 5.7
0
2
4
6
8
10
12
14
16U
nite
d S
tate
s
Sw
itzer
land
Ger
man
y*
Icel
and
Fra
nce
Can
ada
Gre
ece
Por
tuga
l
Sw
eden
Aus
tral
ia**
Bel
gium
Net
herla
nds
Den
mar
k
Nor
way Ita
ly
New
Zea
land
OE
CD
Ave
rage
Hun
gary
Japa
n**
Aus
tria
Uni
ted
Kin
gdom
Spa
in
Cze
ch R
epub
lic
Fin
land
Irel
and
Tur
key*
**
Luxe
mbo
urg
Mex
ico
Pol
and
Kor
ea**
Slo
vak
Rep
ublic
1970 2002
% of GDP
* 1970 data refer to West Germany. ** 2002 data refer to 2001. *** 2002 data refer to 2000.
7
Is spending growth a problem?
Some evidence to suggest that benefits from medical advances exceed costs, at least for some conditions (e.g. Cutler and McClellan 2001)
Health is a vibrant economic sector providing good employment, high-tech industry
But…spending must be financed!
8
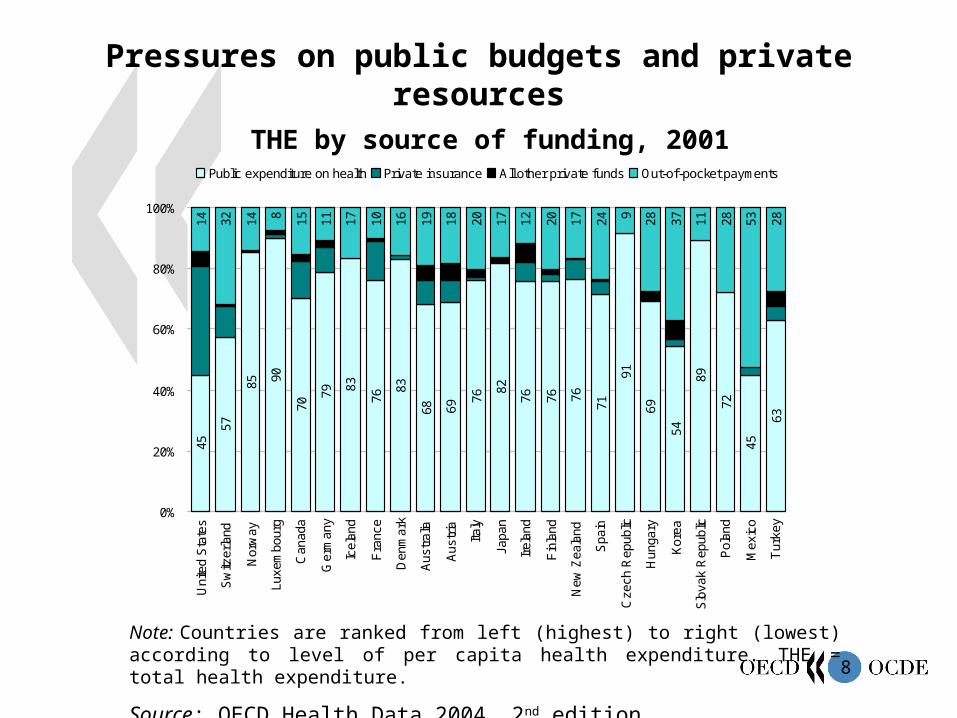
Pressures on public budgets and private
resources THE by source of funding, 2001
Note: Countries are ranked from left (highest) to right (lowest) according to level of per capita health expenditure. THE = total health expenditure.
Source: OECD Health Data 2004, 2nd edition.
63
45
72
89
54
69
91
71
767676
82
76
6968
83
76
8379
70
9085
57
45
2853281137289241720121720181916101711158143214
0%
20%
40%
60%
80%
100%
Tur
key
Mex
ico
Pol
and
Slo
vak
Rep
ublic
Kor
ea
Hun
gary
Cze
ch R
epub
lic
Spa
in
New
Zea
land
Fin
land
Irel
and
Japa
n
Italy
Aus
tria
Aus
tral
ia
Den
mar
k
Fra
nce
Icel
and
Ger
man
y
Can
ada
Luxe
mbo
urg
Nor
way
Sw
itzer
land
Uni
ted
Sta
tes
Public expenditure on health Private insurance All other private funds Out-of-pocket payments

9
Countries should expect continued cost and financing pressure in the health sector.
10
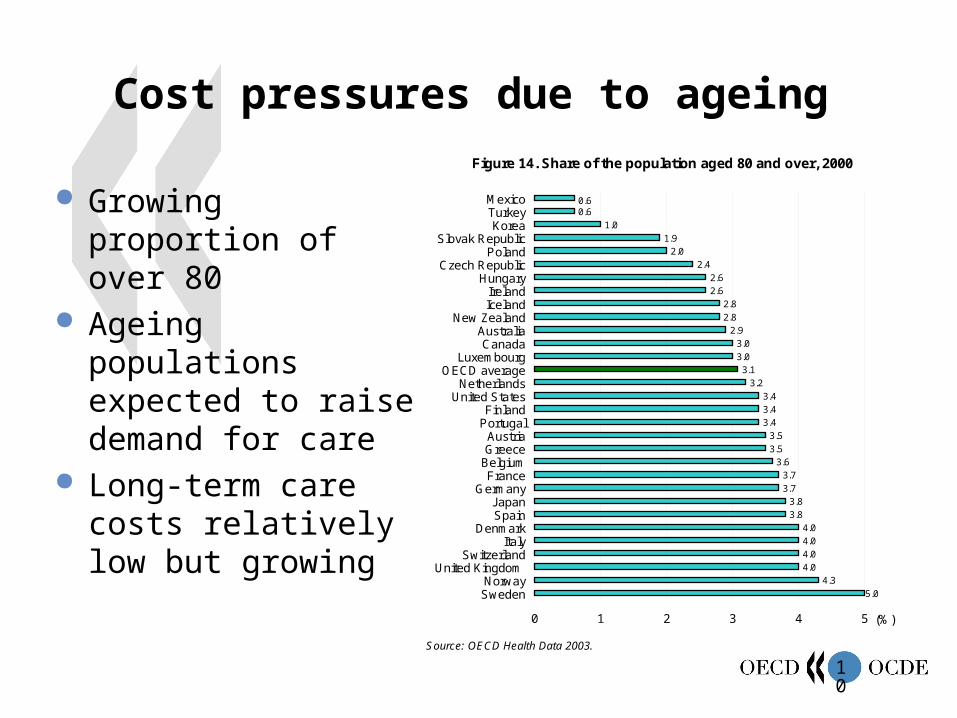
Cost pressures due to ageing
Growing proportion of over 80
Ageing populations expected to raise demand for care
Long-term care costs relatively low but growing
Source: OECD Health Data 2003.
Figure 14. Share of the population aged 80 and over, 2000
0.60.6
1.0
1.9
2.0
2.4
2.6
2.6
2.8
2.8
2.9
3.0
3.0
3.1
3.2
3.4
3.4
3.4
3.5
3.5
3.6
3.7
3.7
3.8
3.8
4.0
4.0
4.0
4.0
4.3
5.0
0 1 2 3 4 5
MexicoTurkeyKorea
Slovak RepublicPoland
Czech RepublicHungary
IrelandIceland
New ZealandAustraliaCanada
LuxembourgOECD average
NetherlandsUnited States
FinlandPortugal
AustriaGreece
BelgiumFrance
GermanyJapanSpain
DenmarkItaly
SwitzerlandUnited Kingdom
NorwaySweden
(%)
11
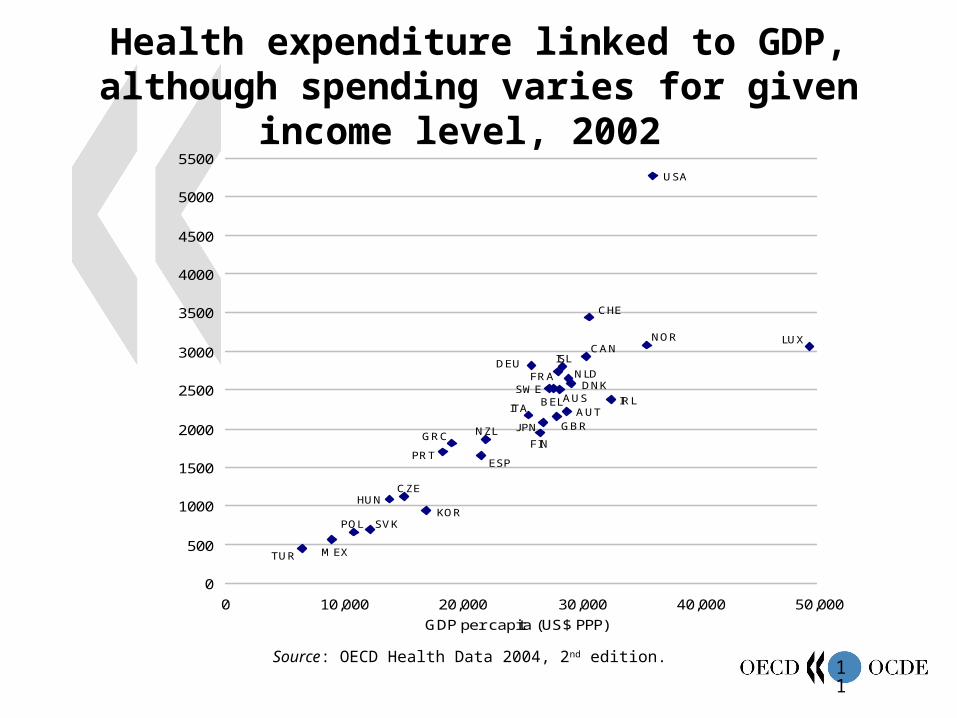
Health expenditure linked to GDP, although spending varies for given income level, 2002
Source: OECD Health Data 2004, 2nd edition.
USA
AUSAUT
BEL
CAN
CZE
DNK
FIN
FRADEU
GRC
HUN
ISL
IRLITA
J PN
KOR
LUX
MEX
NLD
NZL
NOR
POL
PRT
SVK
ESP
SWE
CHE
TUR
GBR
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
5500
0 10,000 20,000 30,000 40,000 50,000
GDP per capita (US$ PPP)
Health expenditure per capita (US$ PPP)
12
There are very great opportunitiesto further improve health and theperformance of health systems.
13
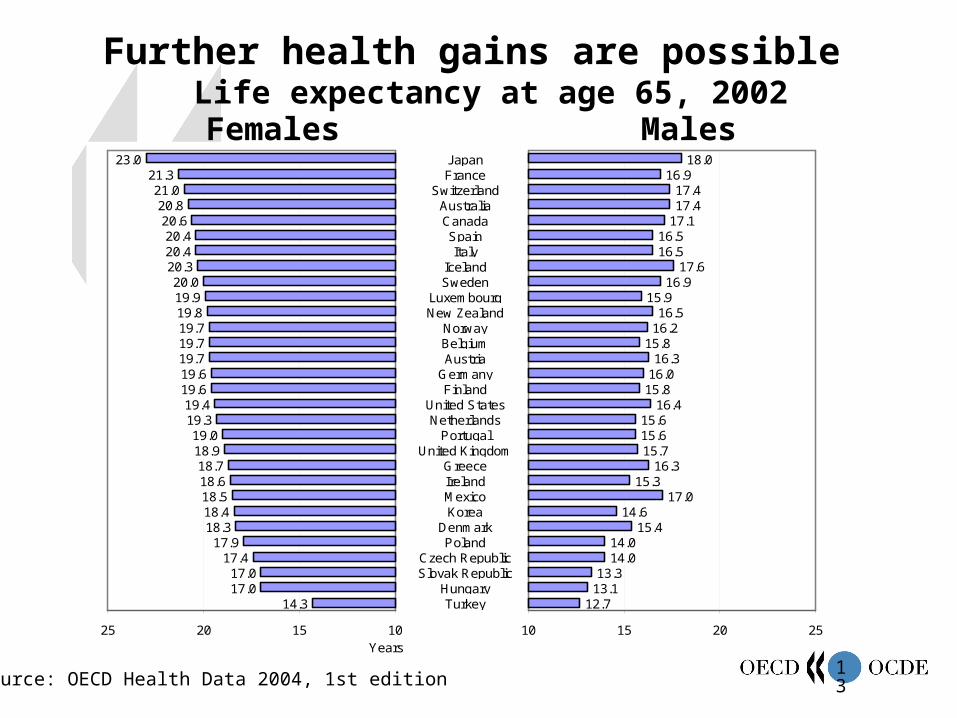
Further health gains are possible Life expectancy at age 65, 2002
JapanFrance
SwitzerlandAustraliaCanadaSpainItaly
IcelandSweden
LuxembourgNew Zealand
NorwayBelgiumAustria
GermanyFinland
United StatesNetherlands
PortugalUnited Kingdom
GreeceIrelandMexicoKorea
DenmarkPoland
Czech RepublicSlovak Republic
HungaryTurkey14.3
17.017.0
17.417.9
18.318.418.518.618.7
18.919.0
19.319.4
19.619.619.719.719.719.819.920.0
20.320.420.4
20.620.8
21.021.3
23.0
10152025
12.713.113.3
14.014.0
15.414.6
17.015.3
16.315.715.615.6
16.415.816.016.3
15.816.216.5
15.916.9
17.616.516.5
17.117.417.4
16.918.0
10 15 20 25Years Years
Females Males
Source: OECD Health Data 2004, 1st edition
14
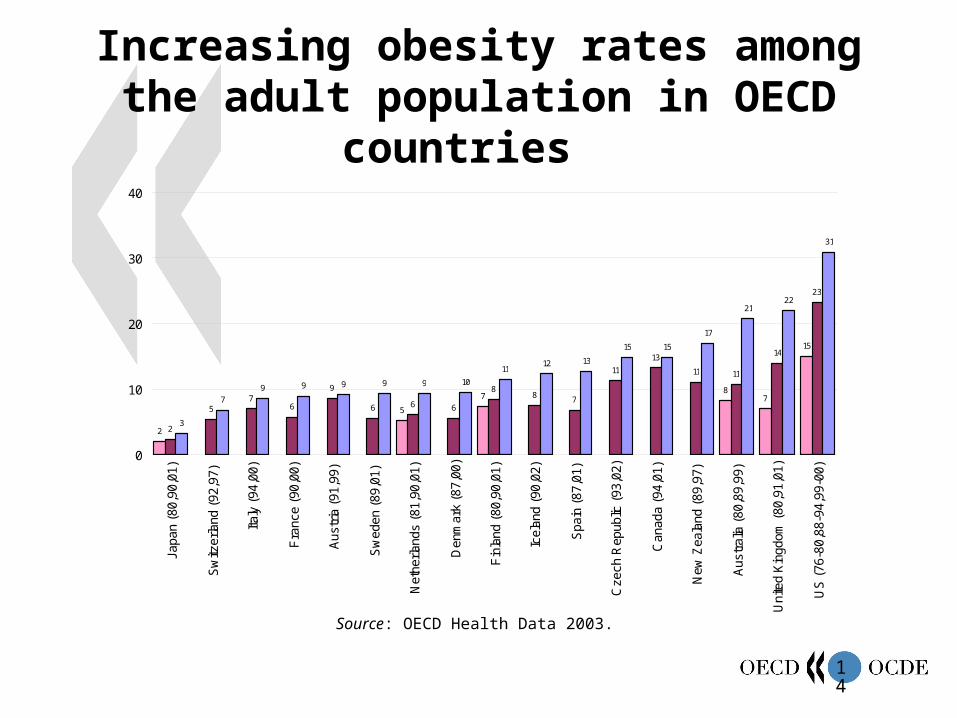
Increasing obesity rates among the adult population in OECD countries
Source: OECD Health Data 2003.
2
5
78
7
15
2
57
6
9
6 6 6
88 7
11
13
11 11
14
23
3
79 9 9 9 9 10
1112 13
15 15
17
2122
31
0
10
20
30
40
Japa
n (8
0,90
,01)
Sw
itzer
land
(92
,97)
Italy
(94
,00)
Fra
nce
(90,
00)
Aus
tria
(91
,99)
Sw
eden
(89
,01)
Net
herla
nds
(81,
90,0
1)
Den
mar
k (8
7,00
)
Fin
land
(80
,90,
01)
Icel
and
(90,
02)
Spa
in (
87,0
1)
Cze
ch R
epub
lic (
93,0
2)
Can
ada
(94,
01)
New
Zea
land
(89
,97)
Aus
tral
ia (
80,8
9,99
)
Uni
ted
Kin
gdom
(80
,91,
01)
US
(76
-80,
88-9
4,99
-00)
Percent
15
Increasing awareness of serious problems with health care quality
Needed services not always provided– Aspirin and beta blockers after a heart attack
Services are provided that are not clinically appropriate for a patient– Antibiotics for colds
Errors in health-care delivery are not uncommon– Wrong-site surgeries, wrong medicine or dosage
16
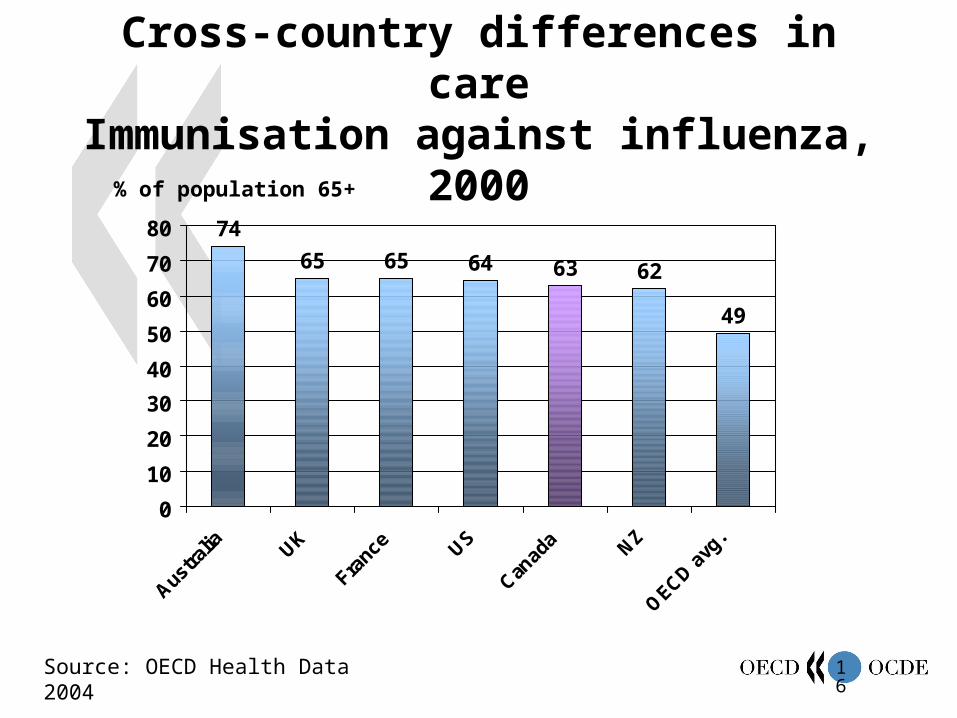
Cross-country differences in careImmunisation against influenza, 2000
Source: OECD Health Data 2004
74
65 65 64 63 62
49
0
10
20
30
40
50
60
70
80
Austra
lia UK
Franc
e US
Canad
a NZ
OECD a
vg.
% of population 65+
17
One-year case-fatality rates for ischaemic stroke, 1998
Note: Canadian data are from Alberta and Ontario, United Kingdom data are from the Oxford region, and United States data are from Medicare data only.
Source: OECD (2003), A Disease-Based Comparison of Health Systems.
% of patients who died within the first year following admission
0
10
20
30
40
50
60
Canada (Ont.) Canada (Alb.) Denmark Sweden UnitedKingdom (Oxf.)
USA (Med.)
M 40-64 F 40-64 M 65-74 F 65-74 M 75+ F 75+
18
Other pressures to improve health-system performance
Excessive waiting times for elective surgery are a policy issue in about ½ of OECD countries
Disparities in access to care, service use, or health status across population groups
19
Efficiency of OECD health systems: what do we know?
Complexity, market failures, extent of government intervention suggest potential for distortions that reduce efficiency
Very large cross-country variation in resources, activity and health system performance– Highest spending and activity levels do not always translate
into best results (e.g. health-care outcomes, waiting times, patient and consumer satisfaction, equitable access to care)
– This suggests that it is not just how much you spend, but how you spend it that matters
– Suggests that there is opportunity to learn from comparison
20
The Challenges
Improving performance without increasing cost pressure
Finding ways to reduce spending that do not hurt performance
Reducing financing pressure while maintaining equity
21
Some Lessons
International comparisons provide valuable guidance– Monitoring and benchmarking are essential
Even armed with knowledge, improving health-system performance is never easy
Trade-offs across policy goals are inevitable
Making real change can be difficult– Need to involve stakeholders– Reform is an iterative process
22
OECD Health Project products
Towards High-Performing Health Systems Final Report to Ministers Summary Report
Policy Studies compendium
Private Health Insurance in OECD Countries
Health Technologies and Decision Making
Long-Term Care for Older People
New OECD Health Working Papers series (16 releases to date)
23
For more information:
www.oecd.org/health
www.oecd.org/healthmin2004