Embed Size (px)
Citation preview

[CANCERRESEARCH 47, 896-901, February l, 1987]
Elevation of Transforming Growth Factor a and Its Relationship to the EpidermalGrowth Factor and a-Fetoprotein Levels in Patients with HepatocellularCarcinoma1
Yun-Chi Yeh,2 Jung-Fa Tsai, Lea-Yea Chuang, Hsing-Wu Yeh, Juei-Hsiung Tsai, Dagne L. Fiorine, and
James P. TarnDepartment of Biochemistry, University of Arkansas for Medical Sciences. Little Rock, Arkansas 72205 [Y-C. Y., H-W. Y.J; Kaoshiung Medical College, Taiwan,Republic of China [J-F.T., L-Y.C., J-H.T.J; Triton Biosciences, Inc., Alameda, California 94501 [D.L.F.I; and The Rockefeller UniversityNew York, New York 10021 fj. P. T.J
ABSTRACT
A radioimmunoassay for transforming growth factor a (TGF-a) usingsynthetic rat sarcoma transforming growth factor and its rabbit polyclonalantibody has been developed. Using radioimmunoassays, the urinaryTGF-a and epidermal growth factor (EGF) concentrations in 31 patientswith hepatocellular carcinoma (11( < I. 15 probable HCC, four metastaticliver cancer, and 33 age, sex-matched healthy controls were determined.For the first time, we have shown that the average TGF-a concentrationfor HCC patients was 21.5 ±20.3 UKper g ere-alininc. significantly higherthan that of healthy subjects, 4.9 ±2.8 Mgper g creatinine (/' < 0.001).
There was no statistical difference in the level of EGF between HCCpatients and controls (40.9 ±29.3 versus 46.2 ±16.6 /ig per g creatinine;P > 0.05). The ratio of EGF/TGF-a between HCC patients (3.37 ±4.42)and controls (15.5 ±13.0) was significantly different (/' < 0.001). Among
patients, 65% (20 of 31) of HCC cases and 87% (13 of 15) of probableHCC cases showed a marked elevation of TGF-a levels. We found only16% (five of 31) of HCC cases with increased EGF level. EGF excretionwas inversely age related. Serum total protein concentration and alkalinephosphatase activity were positively correlated to EGF concentration (r= 0.522, P < 0.01 and r = OJ93, P < 0.05, respectively). There was nocorrelation between biochemical functions of liver and TGF-a concentration in HCC patients.
Our results also suggested that TGF-a may be a useful complementarytumor marker for management of patients with clinical manifestation ofHCC who have low a-fetoprotein levels.
INTRODUCTION
HCC3 is one of the most malignant and prevalent cancers in
humans. The estimated annual incidence of HCC in the worldis 0.3 to 1.2 million, with an apparent increase in its frequencyin many parts of the world (1,2).
Among several important factors in the etiology of HCC,persistent infection with HBV is considered to be a primarycause of this disease (3, 4). There is evidence that aflatoxin andother environmental, chemical, hormonal, and immunologicalagents are also causally associated with the development of thiscancer (5-7). Although the relationship between HBV and HCChas been studied extensively, the link between HBV infectionand neoplastic transformation of HCC remains undefined at abiochemical and genetic level (8).
Clinically, HCC progresses so rapidly that most patientssurvive less than 6 mo after symptoms develop (9, 10). This is
Received 4/7/86, revised 9/11/86; accepted 11/3/86.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1This work was supported in part by grants awarded by Triton Biosciences.Inc. (to Y. C. Y.) and the Chinese National Science Council (to J. H. T.) and byNIH Grant CA36544 (to J. P. T.).
2To whom requests for reprints should be addressed.3The abbreviations used are: HCC, hepatocellular carcinoma; TGF, transform
ing growth factor; EGF, epidermal growth factor; AFP, a-fetoprotein; LFT, liverfunction test; RIA. radioimmunoassay; PB, potassium phosphate buffer (20 m\iKHjPO4:80 min K2HPO4, pH 7.40); HBV, hepatitis B virus; PDGF. platelet-derived growth factor; FGF, fibroblast growth factor.
largely due to the fact that there is as yet no sensitive biochemical diagnostic method for early detection or effective therapeutic agents for treatment of the disease (11-13). Thus, to solvethe world health problem of HCC, biochemical studies ofgrowth control in HCC and identification of tumor markers inHCC patients for early detection become critically important.
More than 20 oncogenes that can transform normal cells intocancer cells in vitro have been identified (14). Some of theseoncogene products are structurally homologous to eithergrowth factors or receptors of growth factors (15-18). In addition, many cancer cells grow autonomously; they are capable ofpromoting their own growth by special growth factors, i.e.,TGFs (19, 20). These growth factors are implicated in theprogression and maintenance of tumor cells (21-26).
EGF is a polypeptide with a molecular weight of approximately 6 x IO3 (27). It was originally isolated from the sub-
maxillary gland of adult mice by Cohen (28) and from humanurine by Gregory (29). EGF promotes the growth of cells ofectodermal and mesodermal origins (30). Recently, genes homologous to a set of mammalian proteins that includes EGFhave been reported to be involved in neural development andhomeostatic controls (31,32). Hepatocytes growth and functionin culture are mutually regulated by EGF and other growthfactors (33, 34).
Two functional classes of TGFs are commonly described inthe literature (35, 36): (a) EGF-related TGFs (originated inembryonic and tumor cells), such as TGF-a, which competeswith EGF for binding to EGF receptors (37-40), and (b) TGF-ß(produced by normal and tumor cells) which does not bind toEGF receptors, but which potentiates the ability of TGF-a topromote colony formation by nontransformed normal rat kidney cells in soft agar (41-44). The biological activity of TGF-ßhas been shown to be nearly identical to that of the growthinhibitor isolated by Holley et al. (45) in that it either stimulatesor inhibits proliferation depending on the experimental conditions (46). There is also a TGF--y class of TGFs that does not
compete with EGF for binding to the EGF receptor but thatdoes promote formation of colonies in the absence of TGF-a(47). TGF-a has been purified and sequenced by Marquardt etal. (48) from a rat cell line transformed by a feline sarcomavirus oncogene (fes), and synthetic rat TGF-a has been preparedby Tarn et al. (49) by the solid-phase synthetic method. Ahuman TGF-a cDNA clone has been isolated and expressed,and anti-humnn TGF-a monoclonal antibodies have beenshown to prevent TGF-a producing rat fibroblast cells fromforming colonies in soft agar (50). TGF-«shave been shown tobe present in normal and pregnant urines and in the urine ofpatients with lung and breast cancer (51-53); however, noquantitative data were available because of lack of a sensitiveand specific assay.
In summary, we have quantitatively studied EGF and TGF-a in the urine of HCC patients using RIAs specific for EGF
896
on June 3, 2020. © 1987 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
TGF-a AND AFP LEVELS IN HCC
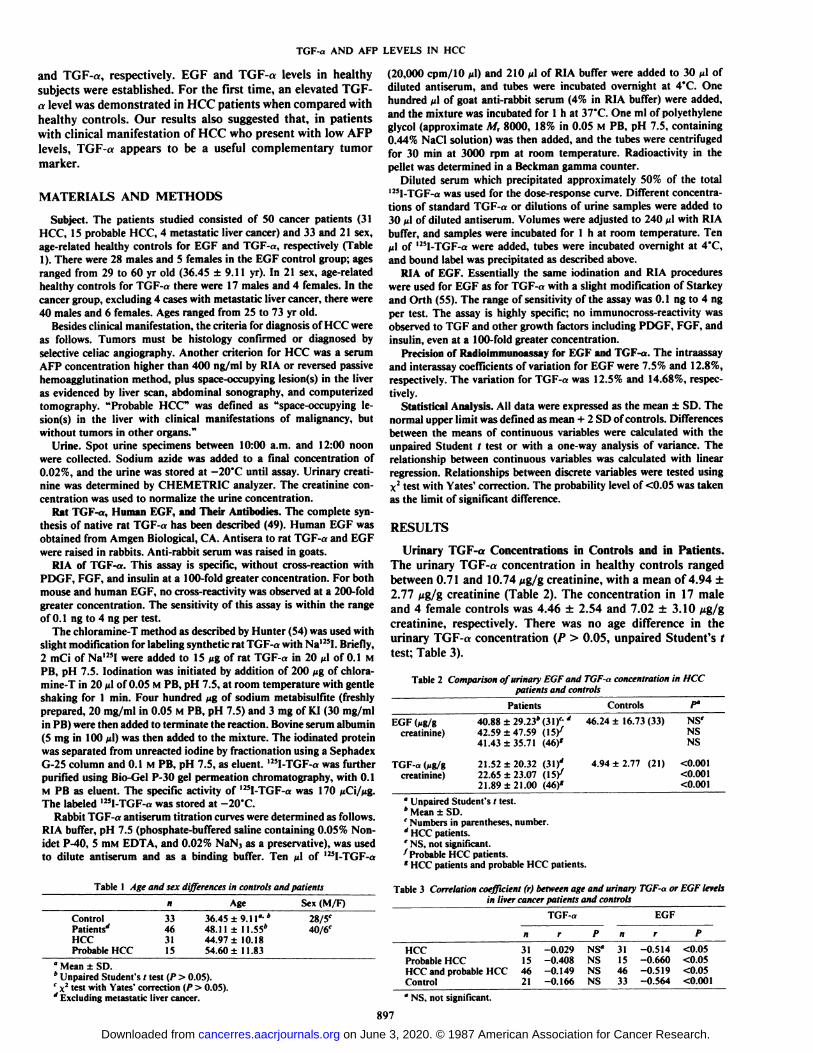
and TGF-«, respectively. EGF and TGF-a levels in healthysubjects were established. For the first time, an elevated TGF-
a level was demonstrated in HCC patients when compared withhealthy controls. Our results also suggested that, in patientswith clinical manifestation of HCC who present with low AFPlevels, TGF-a appears to be a useful complementary tumormarker.
MATERIALS AND METHODS
Subject. The patients studied consisted of SO cancer patients (31HCC, 15 probable HCC, 4 metastatic liver cancer) and 33 and 21 sex,age-related healthy controls for EGF and TGF-a, respectively (Table1). There were 28 males and 5 females in the EGF control group; agesranged from 29 to 60 yr old (36.45 ±9.11 yr). In 21 sex, age-relatedhealthy controls for TGF-a there were 17 males and 4 females. In thecancer group, excluding 4 cases with metastatic liver cancer, there were40 males and 6 females. Ages ranged from 25 to 73 yr old.
Besides clinical manifestation, the criteria for diagnosis of HCC wereas follows. Tumors must be histology confirmed or diagnosed byselective celiac angiography. Another criterion for HCC was a serumAFP concentration higher than 400 ng/ml by RIA or reversed passivehemoagglutination method, plus space-occupying lesion(s) in the liveras evidenced by liver scan, abdominal sonography, and computerizedtomography. "Probable HCC" was defined as "space-occupying le-
sion(s) in the liver with clinical manifestations of malignancy, butwithout tumors in other organs."
Urine. Spot urine specimens between 10:00 a.m. and 12:00 noonwere collected. Sodium azide was added to a final concentration of0.02%, and the urine was stored at -20°C until assay. Urinary creati-
nine was determined by CHEMETRIC analyzer. The creatinine concentration was used to normalize the urine concentration.
Rat TGF-a, Human EGF, and Their Antibodies. The complete synthesis of native rat TGF-a has been described (49). Human EGF wasobtained from Amgen Biological, CA. Antisera to rat TGF-a and EGFwere raised in rabbits. Anti-rabbit serum was raised in goats.
RIA of TGF-a. This assay is specific, without cross-reaction withPDGF, FGF, and insulin at a 100-fold greater concentration. For bothmouse and human EGF, no cross-reactivity was observed at a 200-foldgreater concentration. The sensitivity of this assay is within the rangeof 0.1 ng to 4 ng per test.
The chloramine-T method as described by Hunter (54) was used withslight modification for labeling synthetic rat TGF-a with Na' "I. Briefly,2 mCi of Na'25I were added to 15 ng of rat TGF-«in 20 a\ of 0.1 M
PB, pH 7.5. lodination was initiated by addition of 200 Mgof chloramine-T in 20 n\ of 0.05 M PB, pH 7.5, at room temperature with gentleshaking for 1 min. Four hundred /jg of sodium metabisulfite (freshlyprepared, 20 mg/ml in 0.05 M PB, pH 7.5) and 3 mg of KI (30 mg/mlin PB) were then added to terminate the reaction. Bovine serum albumin(5 mg in 100 nl) was then added to the mixture. The iodinated proteinwas separated from unreacted iodine by fractionation using a SephadexG-25 column and 0.1 M PB, pH 7.5, as eluent. 125I-TGF-a was furtherpurified using Bio-Gel P-30 gel permeation chromatography, with 0.1M PB as eluent. The specific activity of l25I-TGF-a was 170 /iCi/^g.The labeled l25I-TGF-a was stored at -20°C.
Rabbit TGF-a antiserum titration curves were determined as follows.RIA buffer, pH 7.5 (phosphate-buffered saline containing 0.05% Non-idet P-40, 5 mM EDTA, and 0.02% NaN3 as a preservative), was usedto dilute antiserum and as a binding buffer. Ten jil of l25I-TGF-a
Table 1 Age and sex differences in controls and patients
ControlPatients'*
HCCProbable HCCH33
4631ISAge36.45
±9.11°-'48.11 ±11.55*
44.97 ±10.1854.60 ±11.83Sex(M/F)28/5c
40/6C
" Mean ±SD.* Unpaired Student's t test (P > 0.05).' x2 test with Yates' correction (P > 0.05).'' Excluding metastatic liver cancer.
(20.000 cpm/10 ti\) and 210 ^1 of RIA buffer were added to 30 M!ofdiluted antiserum, and tubes were incubated overnight at 4°C.One
hundred n\ of goat anti-rabbit serum (4% in RIA buffer) were added,and the mixture was incubated for l h at 37°C.One ml of polyethylene
glycol (approximate M, 8000, 18% in 0.05 M PB, pH 7.5, containing0.44% NaCl solution) was then added, and the tubes were centrifugedfor 30 min at 3000 rpm at room temperature. Radioactivity in thepellet was determined in a Beckman gamma counter.
Diluted serum which precipitated approximately 50% of the totall25I-TGF-a was used for the dose-response curve. Different concentrations of standard TGF-«or dilutions of urine samples were added to30 iA of diluted antiserum. Volumes were adjusted to 240 n\ with RIAbuffer, and samples were incubated for l h at room temperature. Tenti\ of '"I-TGF-a were added, tubes were incubated overnight at 4'C,
and bound label was precipitated as described above.RIA of EGF. Essentially the same iodination and RIA procedures
were used for EGF as for TGF-a with a slight modification of Starkeyand Orth (55). The range of sensitivity of the assay was 0.1 ng to 4 ngper test. The assay is highly specific; no immunocross-reactivity wasobserved to TGF and other growth factors including PDGF, FGF, andinsulin, even at a 100-fold greater concentration.
Precision of Radioimmunoassay for EGF and TGF-a. The intraassayand interassay coefficients of variation for EGF were 7.5% and 12.8%,respectively. The variation for TGF-a was 12.5% and 14.68%, respec
tively.Statistical Analysis. All data were expressed as the mean ±SD. The
normal upper limit was defined as mean + 2 SD of controls. Differencesbetween the means of continuous variables were calculated with theunpaired Student t test or with a one-way analysis of variance. Therelationship between continuous variables was calculated with linearregression. Relationships between discrete variables were tested usingX2test with Yates' correction. The probability level of <0.05 was taken
as the limit of significant difference.
RESULTS
Urinary TGF-a Concentrations in Controls and in Patients.The urinary TGF-a concentration in healthy controls rangedbetween 0.71 and 10.74 pg/g creatinine, with a mean of 4.94 ±2.77 //g/g creatinine (Table 2). The concentration in 17 maleand 4 female controls was 4.46 ±2.54 and 7.02 ±3.10 ¿ig/gcreatinine, respectively. There was no age difference in theurinary TGF-a concentration (P > 0.05, unpaired Student's t
test; Table 3).
Table 2 Comparison of urinary EGF and TGF-a concentration in HCCpatients and controls
EGF (Mg/gcreatinine)TGF-a
(Mg/gcrealinine)Patients40.88
±29.23*(31)'-'42.59
±47.59 (IS/41.43 ±35.71(46)'21.52*20.32
(il)'
22.65 ±23.07 (IS/2 1.89 ±21.00 (46)'Controls46.24
±16.73(33)4.94
±2.77 (21)P°NS'
NSNS<0.001
<0.001<0.001
" Unpaired Student's t test.* Mean ±SD.' Numbers in parentheses, number.' HCC patients.' NS, not significant.7 Probable HCC patients.' HCC patients and probable HCC patients.
Table 3 Correlation coefficient (r) between age and urinary TGF-a or EGF levelsin liver cancer patients and controls
TGF-a EGF
HCC 31 -0.029 NS° 31 -0.514 <0.05Probable HCC 15 -0.408 NS 15 -0.660 <0.05HCC and probable HCC 46 -0.149 NS 46 -0.519 <0.05Control 21 -0.166 NS 33 -0.564 <0.001
•NS, not significant.
897
on June 3, 2020. © 1987 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
TGF-a AND AFP LEVELS IN HCC
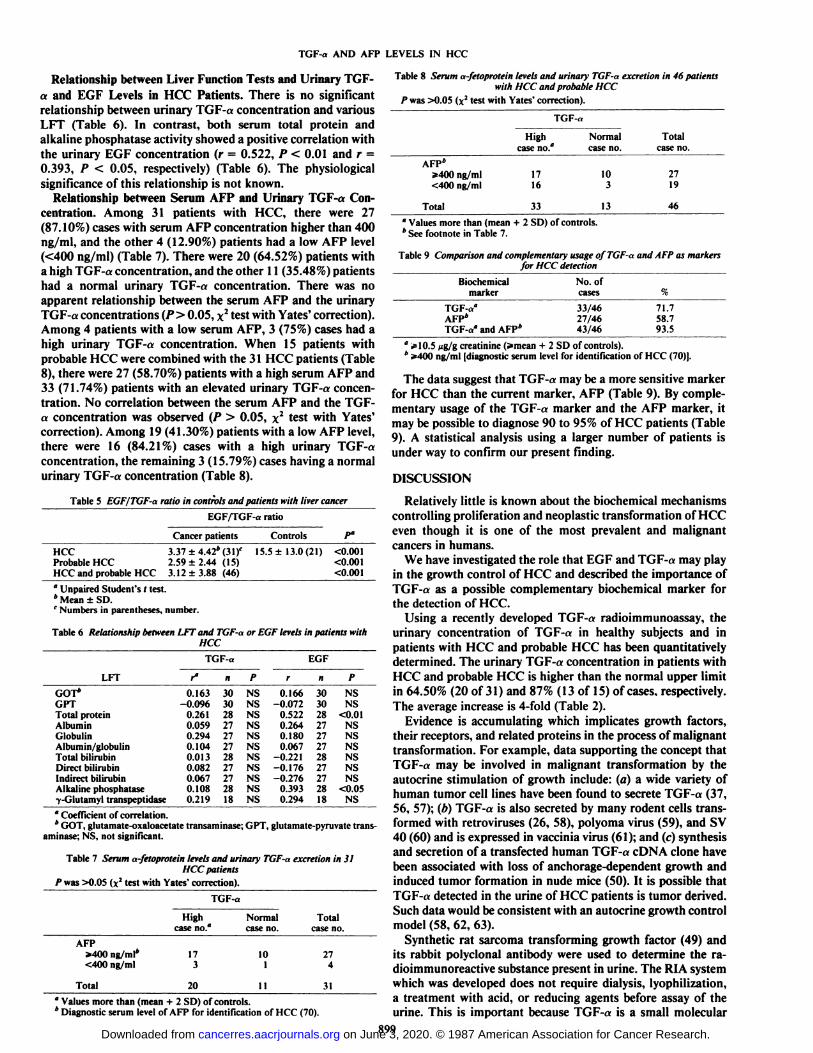
The range of urinary TGF-a concentration in cancer patientswas between 2.8 and 93.33 ßg/gcreatinine. The mean concentrations of TGF-a in patients with HCC, probable HCC, andboth groups combined were 21.52 ±20.32, 22.65 ±23.07, and21.89 ±21.00 ßg/gcreatinine, respectively. Each of these meanconcentrations showed a statistically significant difference ascompared to that of controls (Table 2; Fig. 1).
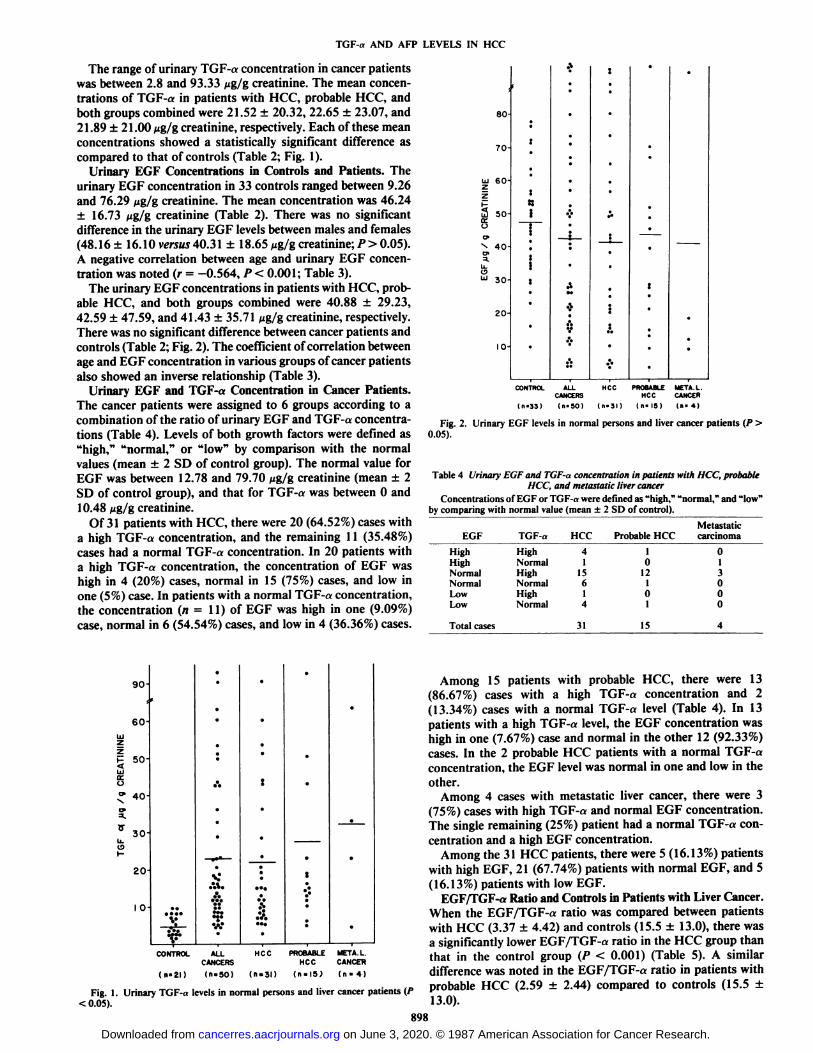
Urinary EGF Concentrations in Controls and Patients. Theurinary EGF concentration in 33 controls ranged between 9.26and 76.29 ßg/gcreatinine. The mean concentration was 46.24±16.73 ßg/gcreatinine (Table 2). There was no significantdifference in the urinary EGF levels between males and females(48.16 ±16.10 versus 40.31 ±18.65 ßg/gcreatinine; P > 0.05).A negative correlation between age and urinary EGF concentration was noted (r = -0.564, P < 0.001; Table 3).
The urinary EGF concentrations in patients with HCC, probable HCC, and both groups combined were 40.88 ±29.23,42.59 ±47.59, and 41.43 ±35.71 ßg/gcreatinine, respectively.There was no significant difference between cancer patients andcontrols (Table 2; Fig. 2). The coefficient of correlation betweenage and EGF concentration in various groups of cancer patientsalso showed an inverse relationship (Table 3).
Urinary EGF and TGF-a Concentration in Cancer Patients.The cancer patients were assigned to 6 groups according to acombination of the ratio of urinary EGF and TGF-a concentrations (Table 4). Levels of both growth factors were defined as"high," "normal," or "low" by comparison with the normal
values (mean ±2 SD of control group). The normal value forEGF was between 12.78 and 79.70 ßg/gcreatinine (mean ±2SD of control group), and that for TGF-a was between 0 and
10.48 ng/g creatinine.Of 31 patients with HCC, there were 20 (64.52%) cases with
a high TGF-a concentration, and the remaining 11 (35.48%)cases had a normal TGF-a concentration. In 20 patients witha high TGF-a concentration, the concentration of EGF washigh in 4 (20%) cases, normal in 15 (75%) cases, and low inone (5%) case. In patients with a normal TGF-a concentration,the concentration (n = 11) of EGF was high in one (9.09%)case, normal in 6 (54.54%) cases, and low in 4 (36.36%) cases.
so-ro-LU
60-ZH2
SO-iÃC71X
40-C7>a.
U.u
30-20-10-[.:*:ni!jt••.•ÎI•:.•§«*•|;A•MA0*A.I•,•;..•.•¿•*•:t—
—':•.•(.
CONTROL ALLCANCERS
U-33) (n-50)
HCC PROBABLE META.L.HCC CANCER
(n-31) (n- IS) (n- 4)
Fig. 2. Urinary EGF levels in normal persons and liver cancer patients (P >0.05).
Table 4 Urinary EGF and TGF-a concentration in patients with HCC, probableHCC, and metastatic liver cancer
Concentrations of EGF or TGF-a were defined as "high," "normal," and "low"
by comparing with normal value (mean ±2 SD of control).
EGFHigh
HighNormalNormalLowLowTGF-aHighNormal
HighNormalHighNormalHCC4
115614Probable
HCC1
012
101Metastatic
carcinoma01
3000
Total cases 31 15
90-60-?Z§
50-0^
40-o>
5.^
30-
u.131-20-10-..*\"•.:.%.u."t*•.9'••.:.:<:£••.S•*
•:'••CONTROL
ALL HCC PROBABLE META.L.CANCERS HCCCAMCER(n-2l)
(n. 50) (n. 3D (n-ISJ (n-4)
Fig. 1. Urinary TGF-a levels in normal persons and liver cancer patients (P< 0.05).
Among 15 patients with probable HCC, there were 13(86.67%) cases with a high TGF-a concentration and 2(13.34%) cases with a normal TGF-a level (Table 4). In 13patients with a high TGF-a level, the EGF concentration washigh in one (7.67%) case and normal in the other 12 (92.33%)cases. In the 2 probable HCC patients with a normal TGF-aconcentration, the EGF level was normal in one and low in theother.
Among 4 cases with metastatic liver cancer, there were 3(75%) cases with high TGF-a and normal EGF concentration.The single remaining (25%) patient had a normal TGF-a con
centration and a high EGF concentration.Among the 31 HCC patients, there were 5 (16.13%) patients
with high EGF, 21 (67.74%) patients with normal EGF, and 5(16.13%) patients with low EGF.
EGF/TGF-a Ratio and Controls in Patients with Liver Cancer.When the EGF/TGF-a ratio was compared between patientswith HCC (3.37 ±4.42) and controls (15.5 ±13.0), there wasa significantly lower EGF/TGF-a ratio in the HCC group thanthat ¡nthe control group (P < 0.001) (Table 5). A similardifference was noted in the EGF/TGF-a ratio in patients withprobable HCC (2.59 ±2.44) compared to controls (15.5 ±13.0).
898
on June 3, 2020. © 1987 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
TGF-a AND AFP LEVELS IN HCC
Relationship between Liver Function Tests and Urinary TGF-
a and EGF Levels in HCC Patients. There is no significantrelationship between urinary TGF-a concentration and variousLFT (Table 6). In contrast, both serum total protein andalkaline phosphatase activity showed a positive correlation withthe urinary EGF concentration (r = 0.522, P < 0.01 and r =0.393, P < 0.05, respectively) (Table 6). The physiologicalsignificance of this relationship is not known.
Relationship between Serum AFP and Urinary TGF-a Concentration. Among 31 patients with HCC, there were 27(87.10%) cases with serum AFP concentration higher than 400ng/ml, and the other 4 (12.90%) patients had a low AFP level(<400 ng/ml) (Table 7). There were 20 (64.52%) patients witha high TGF-a concentration, and the other 11 (35.48%) patientshad a normal urinary TGF-a concentration. There was noapparent relationship between the serum AFP and the urinaryTGF-a concentrations (P> 0.05, x2 test with Yates' correction).
Among 4 patients with a low serum AFP, 3 (75%) cases had ahigh urinary TGF-a concentration. When 15 patients withprobable HCC were combined with the 31 HCC patients (Table8), there were 27 (58.70%) patients with a high serum AFP and33 (71.74%) patients with an elevated urinary TGF-a concentration. No correlation between the serum AFP and the TGF-a concentration was observed (P > 0.05, x2 test with Yates'
correction). Among 19 (41.30%) patients with a low AFP level,there were 16 (84.21%) cases with a high urinary TGF-aconcentration, the remaining 3 (15.79%) cases having a normalurinary TGF-a concentration (Table 8).
Table 5 EGF/TGF-a ratio in controlsana patients withlivercancerEGF/TGF-a ratio
Cancer patients Controls
HCCProbable HCCHCC and probable HCC
3.37 ±4.42*(
2.59 ±2.44 (15)3.12 ±3.88 (46)
15.5 ±13.0(21) <0.001<0.001<0.001
" Unpaired Student's / test.4 Mean ±SD.c Numbers in parentheses, number.
Table 6 RelationshipbetweenLFTand TGF-aor EGF levelsin patients withHCC
TGF-aLFTGOT*GPTTotal
proteinAlbuminGlobulinAlbumin/globulinTotal
bilirubinDirectbilirubinIndirectbilirubinAlkalinephosphatase•y-Glutamyl
transpeptidaset*0.163-0.0960.2610.0590.2940.1040.0130.0820.0670.1080.219R3030282727272827272818PNSNSNSNSNSNSNSNSNSNSNSEGFr0.166-0.0720.5220.2640.1800.067-0.221-0.176-0.2760.3930.294n3030282727272827272818PNSNS<0.01NSNSNSNSNSNS<0.05NS
' Coefficient of correlation.* GOT, glutamate-oxaloacetate transaminase; GPT, glutamate-pyruvate trans
aminase; NS, not significant.
Table 7 Serum a-fetoproteinlevelsand urinary TGF-aexcretionin 31HCC patients
/"was >0.05 (x2 test with Yates' correction).
TGF-aAFP»400
ng/ml*
<400ng/mlTotalHigh
caseno."17
320Normal
caseno.10
111Total
caseno.27431
* Values more than (mean + 2 SD) of controls.* Diagnostic serum level of AFP for identification of HCC (70).
Table 8 Serum a-fetoproteinlevelsand urinary TGF-aexcretionin 46 patientswith HCC and probable HCC
P was >0.05 (x2 test with Yates' correction).
AFP*3*400ng/ml
<400ng/mlTotalTGF-«High
caseno."17
1633Normal
caseno.10313Totalcaseno.27
1946
°Values more than (mean + 2 SD) of controls.* See footnote in Table 7.
Table9 Comparisonand complementaryusageof TGF-aand AFPas markersfor HCC detection
Biochemicalmarker
No. ofcases
TGF-a"AFP*TGF-a°and AFP*
33/4627/4643/46
71.758.793.5
" *10.5 ng/g creatinine (»mean+ 2 SD of controls).* 2*400 ng/ml [diagnostic serum level for identification of HCC (70)).
The data suggest that TGF-a may be a more sensitive markerfor HCC than the current marker, AFP (Table 9). By complementary usage of the TGF-a marker and the AFP marker, itmay be possible to diagnose 90 to 95% of HCC patients (Table9). A statistical analysis using a larger number of patients isunder way to confirm our present finding.
DISCUSSION
Relatively little is known about the biochemical mechanismscontrolling proliferation and neoplastic transformation of HCCeven though it is one of the most prevalent and malignantcancers in humans.
We have investigated the role that EGF and TGF-a may playin the growth control of HCC and described the importance ofTGF-a as a possible complementary biochemical marker forthe detection of HCC.
Using a recently developed TGF-a radioimmunoassay, theurinary concentration of TGF-a in healthy subjects and inpatients with HCC and probable HCC has been quantitativelydetermined. The urinary TGF-a concentration in patients withHCC and probable HCC is higher than the normal upper limitin 64.50% (20 of 31) and 87% (13 of 15) of cases, respectively.The average increase is 4-fold (Table 2).
Evidence is accumulating which implicates growth factors,their receptors, and related proteins in the process of malignanttransformation. For example, data supporting the concept thatTGF-a may be involved in malignant transformation by theautocrine stimulation of growth include: (a) a wide variety ofhuman tumor cell lines have been found to secrete TGF-a (37,56, 57); (b) TGF-a is also secreted by many rodent cells transformed with retroviruses (26, 58), polyoma virus (59), and SV40 (60) and is expressed in vaccinia virus (61); and (c) synthesisand secretion of a transfected human TGF-a cDNA clone havebeen associated with loss of anchorage-dependent growth andinduced tumor formation in nude mice (50). It is possible thatTGF-a detected in the urine of HCC patients is tumor derived.Such data would be consistent with an autocrine growth controlmodel (58, 62, 63).
Synthetic rat sarcoma transforming growth factor (49) andits rabbit polyclonal antibody were used to determine the ra-dioimmunoreactive substance present in urine. The RIA systemwhich was developed does not require dialysis, lyophilization,a treatment with acid, or reducing agents before assay of theurine. This is important because TGF-a is a small molecular
899on June 3, 2020. © 1987 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
TGF-a AND AFP LEVELS IN HCC
weight polypeptide found in relatively low concentration in thebody fluid, and it exhibits a nonspecific affinity to varioussurfaces during pretreatment processes. Therefore, this procedure is rapid and quantitative for determining the total ¡miminoreactive TGF-a substances. A RIA which uses a \l-merfragment of rat TGF-a (residues 34 to 50) and its rabbitpolyclonal antibody instead of the whole rat TGF-a moleculehas been described (65).
The role of AFP in the diagnosis of advanced HCC is wellrecognized (66-70). The disadvantage of this test is a highincidence of false negatives. For instance, at least 35% of small-sized HCC and 10% of advanced HCC will be missed unlessanother diagnostic tool is used (71). In the present study, 4(12.9%) of 31 advanced HCC patients had AFP lower than 400ng/ml, but 3 (75%) of the 4 showed an elevated urinary TGF-n concentration (Table 7). If 15 cases with probable HCC areadded to the analysis, the proportion of patients with a lowAFP increased to 41.3% (19 of 46); thus, only 59% (27 of 46)of patients with HCC and probable HCC is detected by usingthe current AFP marker (Table 8). However, 84.2% (16 of 19)of the AFP false negatives exhibit an elevated urinary TGF-alevel, and thus those patients can be properly diagnosed by theTGF-a marker.
In this study, urinary EGF showed no sexual variation. Thisis consistent with previous reports (55), but in contrast to otherreports which demonstrated significantly higher excretion ofEGF in females than in males (72, 73). We observed an inverserelationship between age and the urinary EGF concentration(Table 3). Our result appears to be consistent with the reportby Uchihashi et al. (72), although Gregory et al. (73) did notobserve any obvious change of urinary excretion of EGF inrelation to age. Decreased urinary EGF excretion with increasedage in normal individuals may be due to reduced cellular synthesis or secretion of EGF.
There is no significant difference in the urinary EGF concentration in patients with HCC and normal controls (Table 2). Inour study, among 31 patients with HCC, there are 5 (16%)cases with a high urinary EGF concentration. Wong et al. (74)have also reported an elevation of multiple forms of EGF andTGF-like substances during pregnancy. It is possible that someHCC may, like pregnancy, excrete EGF-like substances orproduce an as yet unspecified stimulatory factor for synthesisand excretion of EGF.
According to our results, serum total protein concentrationand alkaline phosphatase activity were positively correlatedwith EGF concentration (r = 0.522, P < 0.01 and r = 0.393, P< 0.05, respectively). One possible interpretation is that EGFmay play a significant role in the metabolism of these proteinsin HCC patients (Table 6). In contrast, no correlation wasfound between biochemical functions of the liver and TGF-aconcentration in HCC patients.
Functional and structural relationships of various TGF-asremain unclear. Sherwin et al. (52) reported an EGF-related,high-molecular-weight (M, = 30,000 to -35,000) TGF activityand a low-molecular-weight TGF activity (M, = 6,000 to~8,000) in the urine of patients with solid disseminated tumors.Kimball et al. (53) also demonstrated existence of a high-molecular-weight (M, = 30,000) TGF activity in the urine oftumor patients. This high-molecular-weight tumor-associatedTGF gradually underwent conversion to M, 6,000 TGF. Multiple TGFs of different molecular mass have also been detectedin human placenta (75) and in supernatants and extracts oftumor cells (21, 37, 76, 77). Recently TGFs with differentisoelectric points then previously reported have also been reported in human milk (78). Amino acid composition of a human
melanoma-derived urinary TGF-a has recently been reported(64). Data suggested that the urinary TGF-a of melanomapatients is different from the TGF-a of human and rat cell lines(48, 64, 79). It is important to ascertain whether the TGF-adescribed in this paper is unique to HCC or is representative ofa class of peptides with similar properties in other tumors. Thepurification of TGF-a from the urine of patients with HCC andestablishment of the amino acid sequence may provide furtherunderstanding of the tumorigenesis of HCC.
REFERENCES
1. World Health Organization. Advances in viral hepatitis. Report of the WHOExpert Committee on Viral Hepatitis. WHO Tech. Rep. Ser., 602: 7-47,1977.
2. World Health Organization. Prevention of primary' liver cancer: report of aWHO meeting. WHO Tech. Rep. Ser., 691: 7-11, 1983.
3. Szmuness. W. Hepatocellular carcinoma and the hepatitis B virus: evidencefor a casual association. Prog. Med. Virol., 24:40-69, 1978.
4. Beasley, R. P., Hwang, L. Y., Lin, C. C, and Chien, C. S. Hepatocellularcarcinoma and hepatitis B virus. A prospective study of 22.707 men inTaiwan. Lancet, 2:1129-1133. 1981.
5. Linsell, C. A., and Peers, F. G. Aflatoxin and liver cell cancer. In: H. H.Hiatt, J. D. Watson, and J. A. Winsten (eds.), Origins of Human Cancer,pp. 549-556. Cold Spring Harbor, NY: Cold Spring Harbor Laboratory,1977.
6. Cook-Mozaffari, P.. and Van Renburg, S. Cancer of the liver. Br. Med. Bull.,40:342-345, 1984.
7. Webber, M. M. Carcinoma of the liver. In: M. M. Webber and L. I. Sekely(eds.). In Vitro Models for Cancer Research, Vol. 2, pp. 4-7. Boca Raton,FL: CRC Press, 1985.
8. Shaul, Y., Ziemer, M., Gacia, P. D., Crawford, R., Hsu, R., Valenzuela, P.,and Rutter, W. J. Cloning and analysis of integrated hepatitis virus sequencesfrom a human hepatoma cell line. J. Virol., 51: 776-787, 1984.
9. Berman, C. Primary carcinoma of the liver. A study incidence, clinicalmanifestations, pathology, and aetiology. London: Lewis & Company, 1951.
10. Lin, T. Y., Hsieh, C. M., Tsai, T. C., and Lin, T. K. Study on primarycarcinoma of the liver. Clinical observation of 63 cases with 18 hepatoecto-mies. J. Formosan Med. Assoc., 61: 323-344, 1962.
11. Okuda. K., and Nakashima, T. Primary carcinoma of the liver. In: J. E. Berk,W. S. Haubrick, M. H. Kaiser, J. L. A. Roth, and F. Shaffner (eds.). BackusGastroenterology. Vol. 5. pp. 3315-3387. Philadelphia. PA: W. B. SaundersCo., 1985.
12. Sheen, M. C., Huang, T. J., Sheen, P. C., Ho, Y. H., Chang, W. Y., andChen, C. Y. Intraarterial infusion chemotherapy of primary liver cancer. J.Formosan Med. Assoc.. 83: 800-806. 1984.
13. Edmondson, H. A., and Peter. R. L. Neoplasms of the liver. In: L. Shiff andE. R. Shiff (eds.), Disease of the liver, pp. 1101-1151. Philadelphia, PA: J.B. Lippincott Co., 1982.
14. Bishop, J. M. Viral oncogenes. Cell, 42: 23-38, 1985.15. Downward. J.. Yarden, Y., Mayes. E., Scarce, G., Totty, N., Stockwell, P.,
Ullrich, A., Schlessinger. J., and Waterfield. M. D. Close similarity ofepidermal growth factor receptor and \-erb B oncogene protein sequences.Nature (Lond.), 307: 521-527, 1984.
16. Ullrich, A., Coussens, L., Hayflick, J. S., Dull, T. J., Gray. A., Tarn, A. W.,Lee, J., Yarden, Y., Libermann. T. A., Schlessinger. J., Downward. J., Mayes,E. L. V., Whittle, N.. Waterfield. M. D., and Seeburg, P. H. Humanepidermal growth factor receptor cDNA sequence and aberrant expressionof the amplified gene in A431 epidermoid carcinoma cells. Nature (Lond.),309:418-425, 1984.
17. Doolittle, R. F., Hunkapiller, M. W., Hood, L. E., Devare, S. G., Robbins.K. C.. Aaronson, S. A., and Antoniades, H. N. Simian sarcoma virusoncogene, v-ji'j, is derived from the gene (or genes) encoding a platelet-
derived growth factor. Science (Wash. DC), 221: 275-277, 1983.18. Waterfield, M. D., Scarce, G. T., Whittle, N., Stroobant, P., Johnson, A.,
Wasteson, A., Westmark, B., Heldin, C. H.. Huang. J. S., and Deuel, T. F.Platelet-derived growth factor is structurally related to the putative transforming protein p28'" of simian sarcoma virus. Nature (Lond.). 304: 35-39,
1983.19. Growth factors and transformation. In: J. Feramisco, B. Ozanne, and C.
Stiles (eds.). Cancer Cells, Vol. 3. Cold Spring Harbor, NY: Cold SpringHarbor Laboratory, 1985.
20. Anzano, M. A., Roberts, A. B., Meyers, C. A., Komoriya, A., Lamb, L. C.,Smith, J. M.. and Sporn, M. B. Synergistic interaction of two classes oftransforming growth factors from murine sarcoma cells. Cancer Res., 42:4776-4778, 1982.
21. De Larco, J. E., and Todaro, G. J. Growth factors from murine sarcomavirus transformed cells. Proc. Nati. Acad. Sci. USA, 75: 4001-4005, 1978.
22. Roberts, A. B., Anzano, M. A., Lamb, L. C., Smith, J. M., and Sporn, M.B. New class of transforming growth factors potentiated by epidermal growthfactor, isolation from non-neoplastic tissues. Proc. Nati. Acad. Sci. USA, 78:5339-5343. 1981.
23. Marquardt, H.. Hunkapillar, M. W., Hood, L. E., Twardzik. D. R., De Larco,J. E., Stephenson, J. R., and Todaro, G. J. Transforming growth factorsproduced by retrovirus-transformed rodent fibroblasts and human melanoma
900
on June 3, 2020. © 1987 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
TGF-a AND AFP LEVELS IN HCC
cells: amino acid sequence homology with epidermal growth factor. Proc.Nati. Acad. Sci. USA, SO:4684-4688, 1983. 51.
24. Kaplan, P. L.. Anderson, M., and Ozanne, B. Transforming growth factor(s)production enables cells to grow in the absence of serum: an autocrine system.Proc. Nati. Acad. Sci. USA, 79:485-489, 1982. 52.
25. Todaro, G. J. Autocrine secretion of peptide growth factors by tumor cells.Nail. Cancer Inst. Monogr., 60: 139-147, 1982.
26. Twardzik, D. R., Todaro, G. J.. Marquardt, H.. Reynolds. F. H., Jr., and 53.Stephenson, J. R. Transformation induced by Abelson murine leukemia virusinvolves production of a polypeptide growth factor. Science (Wash. DC),2/6:894-897. 1982.
27. Savage, C. R., Jr., Inagami, T., and Cohen, S. The primary structure of 54.epidermal growth factor. J. Biol. Chem., 247: 7612-7621, 1972.
28. Cohen, S. Isolation of a mouse submáxillarygland protein accelerating incisoreruption and eyelid opening in the newborn animal. J. Biochem.. 237:1555- 55.1562, 1962.
29. Gregory, H. Isolation and structure of urogastrone and its relationship toepidermal growth factor. Nature (Lond.), 257: 325-327, 1975. 56.
30. Carpenter, G., and Cohen, S. Epidermal growth factor. Annu. Rev. Biochem.,48:193-216, 1979.
31. Wharton, K. A., Johansen. K. M., Xu, T.. and Artavanis-Tsakonas, S. 57.Nucleotide sequence from the neurogenic locus notch implies a gene productthat shares homology with proteins containing EGF-like repeats. Cell. 43:567-581. 1985.
32. Greenwald, I. A nematode homeotic gene is homologous to a set of mammalian proteins that includes epidermal growth factor. Cell, 43: 583-590, 58.1985.
33. Bucher, N. L. Hormone interactions in primary cultures of adult rat hepa-tocytes. In: H. Murakami, I. Yamane, D. W. Barnes, J. P. Hayashi, and G. 59.H. Sato (eds.). Growth and Differentiation of Cells in Defined Environment,pp. 467-472. New York: Springer-Verlag, 1985.
34. Leffert, H. L., Koch, K. S., Lad, P. J., Skelley, H.. and Hemptinne, B. 60.Hepatocyte growth factors. In: D. Zakim and T. D. Boyer (eds.), Hepatology.p. 64. Philadelphia, PA: W. B. Saunders Co., 1982.
35. Roberts, A. B., Frolik, C. A., Anzano, M. A., and Sporn, M. B. Transforming 61.growth factors from neoplastic and non-neoplastic tissues. Fed. Proc., 42:2621-2625, 1983.
36. Moses, H. L. Growth factors and transforming growth factors: potential 62.roles in cancer. Proc. Am. Assoc. Cancer Res., 25: 412-413, 1984.
37. Todaro, G. J., Fryling, C., and De Larco, J. E. Transforming growth factors 63.produced by certain human tumor cells: polypeptides that interact withepidermal growth factor receptors. Proc. Nati. Acad. Sci. USA, 77: 5258- 64.5262, 1980.
38. Moses, H. L., Branum, E. L., Proper, J. A., and Robinson, R. A. Transforming growth factor production by chemically transformed cells. Cancer Res., 65.41: 2842-2848, 1981.
39. Roberts, A. B.. Lamb, L. C., Newton, D. L., Sporn, M. B., De Larco, J. E.,and Todaro, G. J. Transforming growth factors: isolation of polypeptidesfrom virally and chemically transformed cells by acid/ethanol extraction. 66.Proc. Nati. Acad. Sci. USA, 77:3494-3498, 1980.
40. Massague, J. Epidermal growth factor-like transforming growth factor. II.Interaction with epidermal growth factor receptors in human placenta mem- 67.brane and A431 cells. J. Biol. Chem., 25Ä:13614-13620. 1983.
41. Roberts, A. B., Anzano. M. A., Lamb, L. C., Smith, J. M., Frolik, C. A., 68.Marquardl, H., Todaro. G. J., and Sporn, M. B. Isolation from murinesarcoma cells of novel transforming growth factors potentiated by EGF.Nature (Lond.), 295:417-419, 1982. 69.
42. Roberts, A. B., Anazo. M. A., Meyers, C. A., Wideman, J.. Blacher, R., Pan,Y. E., Stein, S., Lehman, S. R., Smith, J. M.. Lamb, L. C, and Sporn, M. 70.B. Purification and properties of a type •'transforming growth factor frombovine kidney. Biochemistry, 22: 5692-5698, 1983. 71.
43. Assoian, R. K., Komoriya, A., Meyers, C. A., Miller, D. M., and Sporn, M.B. Transforming growth factor .; in human platelets: identification of a majorstorage site, purification, and characterization. J. Biol. Chem., 255: 7155- 72.7160, 1983.
44. Frolik, C. A., Dart, L. L., Meyers, C. A., Smith, D. M., and Sporn, M. B.Purification and initial characterization of a type ßtransforming growth 73.factor from human placenta. Proc. Nati. Acad. Sci. USA, 80: 3676-3680,1983.
45. 1Inlli-). R. W., Armour, R., and Baldwin, J. H. Density-dependent regulation 74.of growth of BSC-I cells in culture: growth inhibitors formed by the cells.Proc. Nati. Acad. Sci. USA, 75:1864-1866, 1978.
46. Tucker, R. F.. Shipley, G. D., Moses, H. L., and Holley, R. W. Growth 75.inhibitor from BSC-1 cells closely related to platelet type beta transforminggrowth factor. Science (Wash. DC), 226: 705-707, 1984.
47. Yamaoka, K., Hirai. R., and Mitsui, H. New class of transforming growth 76.factor, TGF gamma 2, isolated from avian sarcoma virus-transformed ratcells: purification and determination of ^-terminal amino acid sequences. In:H. Murakami. I. Yamane, D. W. Barnes, J. P. Hayashi, and G. H. Sato 77.(eds.). Growth and Differentiation of Cells in Defined Environment, pp.385-388. New York: Springer-Verlag, 1985.
48. Marquardt, H., Hunkapiller, M. W.. Hood, L. E., and Todaro, G. J. Rat 78.transforming growth factor type I : structure and relation to epidermal growthfactor. Science (Wash. DC), 22* 1079-1082, 1984.
49. Tam, J. P., Marquardt, H., Rosberger, D. F., Wong, T. W., and Todaro, G. 79.J. Synthesis of biologically active rat transforming growth factor I. Nature(Lond.), 309: 376-378, 1984.
50. Rosenthal. A., Lindquist. P. B.. Bringman, T. S.. Goeddel, D. V.. andDerynck, R. Expression in rat fibroblasts of a human transforming growth
901
factor «cDNA results in transformation. Cell, 46: 301-309, 1986.Twardzik, D. R., Sherwin, S. A., Ranchalis, J., and Todaro, G. J. Transforming growth factors in the urine of normal, pregnant, and tumor-bearinghumans. J. Nati. Cancer Inst., 69: 793-798. 1982.Sherwin. S. A., Twardzik. D. R., Bohn, W. H., Cookley. K. D.. and Todaro,G. J. High molecular weight transforming growth factor activity in the urineof patients with disseminated cancer. Cancer Res.. 43:403-407, 1983.Kimball, E. S., Bohn, W. H.. Cookley. K. D.. Warren, T. C., and Sherwin,S. A. Distinct high-performance liquid chromatography pattern of transforming growth factor activity in urine of cancer patients as compared with thatof normal individuals. Cancer Res.. 44: 3613-3619. 1984.Hunter, W. M., and Greenwood, F. C. Preparation of iodine-131 labelledhuman growth hormone of high specific activity. Nature (Lond.), 194: 495-496, 1962.Starkey, R. H., and Orth, D. N. Radioimmunoassay of human epidermalgrowth factor (urogastrone). J. Clin. Endocrino!. & Melab., 45: 1144-1153,1977.Marquardt, H., and Todaro, G. J. Human transforming growth factor.Production by a melanoma cell line, purification, and initial characterization.J. Biol. Chem., 257: 5220-5225, 1982.Marquardt, H.. Hunkapillar. M. W., Hood, L. E., Twardzik. D. R., De Larco,J. E., Stephenson, J. R., and Todaro. G. J. Transforming growth factorsproduced by retrovirus-transformed rodent fibroblasts and human melanomacells: amino acid sequence homology with epidermal growth factor. Proc.Nati. Acad. Sci. USA. 80:4684-4688, 1983.Todaro, G. J.. De Larco. J. E., Nissley, S. P.. and Rechler, M. M. MSA andEGF receptors on sarcoma virus-transformed cells and human fibrosarcomacells in culture. Nature (Lond.), 267: 526-528, 1977.Kaplan, P. L., and Ozanne, B. Polyoma virus-transformed cells producetransforming growth factor(s) and grow in serum-free medium. Virology.123: 372-380. 1982.Kaplan, P. L., Topp, W. C., and Ozanne, B. Simian Virus 40 induces theproduction of a polypeptide transforming factor(s). Virology, 108: 484-490,1981.Brown, J. P.. Twardzik, D. R., Marquardt, H., and Todaro, G. J. Vacciniavirus encodes a polypeptide homologous to epidermal growth factor and atransforming growth factor. Nature (Lond.), 313:491-492, 1985.Sporn. M. B.. and Todaro. G. J. Autocrine secretion and malignant transformation of cells. N. Engl. J. Med., 303:878-880. 1980.Sporn. M. B., and Roberts, A. B. Autocrine growth factors and cancer.Nature (Lond.). 313:745-747, 1985.Kim, M. K.. Warren, T. C., and Kimball, E. S. Purification and characterization of low-molecular-weight transforming growth-factor from the urine ofmelanoma patients. J. Biol. Chem., 260: 9237-9243, 1985.Linsley, P. S., Hargreaves, W. R.. Twardzik, D. R., and Todaro, G. J.Detection of larger polypeptides structurally and functionally related to typeI transforming growth factor. Proc. Nati. Acad. Sci. USA, «2:356-360,1985.Tatarinov, Y. S. Obnaruzheni embriospetsi ficheskogo alpha-globulina vsyvorotke Krovi bol'nogo pervichnym rakom pecheni. Vopr. Med. Mum..10:90-91, 1964.Alpert. M. E., Uriel, J., and de Nechand, B. Alpha-1 fetoglobulin in thediagnosis of human hepatoma. N. Engl. J. Med., 27«:984-986, 1968.O'Connor, G. T., Tatarinov, Y. S., Abelev, G. I., and Uriel, J. A collaborative
study for the evaluation of serologie test for primary liver cancer. Cancer(Phila.). 25:1091-1098, 1970.Kew, M. Progress report. Alpha-fetoprotein in primary liver cancer and otherdiseases. Gut, 15: 814-821, 1974.Chen, D. S., and Sung, J. L. Serum alpha-fetoprotein in hepatocellularcarcinoma. Cancer (Phila.). 40: 779-783, 1977.Chen, D. S., Sung, J. L., Sheu, J. C, Lai, M. Y., How, S. W., Hsu, H. C,Lee, C. S., and Wei, T. C. Serum alpha-fetoprotein in the early stage ofhuman hepatocellular carcinoma. Gastroenterology, 86: 1404-1409, 1984.Uchihashi, M.. Hirata, T., Fugita, T., and Matsukura, S. Age-related decreaseof urinary' excretion of human epidermal growth factor (h EGF). Life Sci.,31:679-683, 1982.Gregory. H., Holmes, J. E.. and Wiltshire, I. R. Urogastrone levels in theurine of normal adult humans. J. Clin. Endocrino!. & Metab., 45: 668-672,1977.Wong, T. C., Yeh, H. W., and Yeh, Y. C. A study on human epidermalgrowth factor (EGF) and transforming growth factor (TGF)-like substancesin the urine of pregnant females. Fed. Proc., 43: 1889, 1984.Stromberg, K., Pigott, D. A., Ranchalis, J. E., and Twardzik, D. R. Humanterm placenta contains transforming growth factors. Biochem. Biophys. Res.Commun.. 706: 354-361. 1982.Zwiebel, J. A., Davis, M. R., Kohn, E., Salomon. D. S., and Kidwell, W. R.Anchorage-independent growth-conferring factor production by rat mammary tumor cells. Cancer Res., 42: 5117-5125, 1982.De Larco. J. E., Pigott, D. A., and Lazarus, J. A. Ectopie peptides releasedby a human melanoma cell line that modulate the transformed phenotype.Proc. Nati. Acad. Sci. USA, «2:5015-5019, 1985.Zwiebel, J. A.. Baño,M., Nexo, E., Salomon, D. S., and Kidwell, W. R.Partial purification of transforming growth factors from human milk. CancerRes., 46: 933-939, 1986.Derynck. R., Roberts, A. B., Eaton, D. H.. Winkler. M. E., and Goeddel, D.V. Human transforming growth factor-alpha precursor sequence gene structure and heterologous expression. In: J. Feramisco. B. Ozanne, and C. Stiles(eds.). Cancer Cells: 3. Growth Factors and Transformation, pp. 79-86. ColdSpring Harbor, NY: Cold Spring Harbor Laboratory, 1985.
on June 3, 2020. © 1987 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1987;47:896-901. Cancer Res Yun-Chi Yeh, Jung-Fa Tsai, Lea-Yea Chuang, et al. Patients with Hepatocellular Carcinoma
-Fetoprotein Levels inαto the Epidermal Growth Factor and and Its RelationshipαElevation of Transforming Growth Factor
Updated version
http://cancerres.aacrjournals.org/content/47/3/896
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/47/3/896To request permission to re-use all or part of this article, use this link
on June 3, 2020. © 1987 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from