Embed Size (px)
Citation preview

Introduction
Sudden cardiac death (SCD) is a major cause of deathin patients with nonischemic cardiomyopathy (DCM).The Implantable Cardioverter Defibrillator (ICD)prevents sudden cardiac death in patients who have
had an episode of ventricular tachycardia or cardiacarrest. In contrast studies failed to demonstratereduction of all cause mortality in patients withnonischemic cardiomyopathy receiving an ICD forprimary prevention [1, 8]. Identification of clinicalparameters predicting SCD would possibly improve
Tobias SimonRuediger BeckerFrederik VossOlympia BikouMelanie HauckManuela LickaHugo A. KatusAlexander Bauer
Elevated B-type natriuretic peptide levelsin patients with nonischemiccardiomyopathy predict occurrence ofarrhythmic events
Received: 9 August 2007Accepted: 20 November 2007Published online: 14 January 2008
j Abstract Background: Patients with nonischemic cardiomyopathy(DCM) are at high risk for sudden cardiac death (SCD). However, thepredictive value of prophylactic implantation of implantable cardioverterdefibrillators (ICD) in this patient cohort is yet unclear. Methods andResults: Whether NT pro BNP levels and/or reproducible non sustainedventricular tachycardias (NSVTs) are predictive for SCD was prospectivelytested in 30 patients with DCM and LVEF £ 40%. All patients receivedHolter-recordings (HR) on three consecutive days and baseline NT-proBNP levels were determined. Patients were followed for occurrence ofventricular tachyarrhythmias or unexplained syncope. A great degree ofvariability was found regarding the occurrence of NSVTs (10% had NSVTsin two consecutive HR, 10% in three consecutive HR, 30% in one HR and50% had no NSVTs). Patients with NSVTs in more than one HR hadsignificantly higher NT-pro BNP levels (first quartile: 715 pg/ml, median2,176 pg/ml, third quartile 5,755 pg/ml vs. first quartile 273 pg/ml, median566 pg/ml, third quartile 1,350 pg/ml, P = 0.0388). During a mean follow-up of 21.6 ± 1.2 months patients with an arrhythmic event had signifi-cantly higher NT-pro BNP levels than patients without event (first quartile:1,002 pg/ml, median 4,075 pg/ml, third quartile 7,777 pg/ml vs. firstquartile 173 pg/ml, median 267 pg/ml, third quartile 1,220 pg/ml,P = 0.0135). NT-pro BNP levels of 2,259 pg/ml were identified as optimalcut-off value for the prediction of arrhythmic events (P = 0.0313). Incontrast reproducible NSVTs were not predictive for arrhythmic events(P = 0.0960). Conclusion: The present study demonstrates that in patientswith DCM the value of reproducible NSVTs in predicting arrhythmic eventsis low. In contrast raised NT-pro BNP levels significantly correlated withoccurrence of symptomatic ventricular arrhythmias. Larger prospectivetrials are required to confirm these results.
j Key words nonischemic cardiomyopathy – risk stratification – nonsustained ventricular tachycardias – NT-pro BNP – sudden cardiac death
ORIGINAL PAPERClin Res Cardiol 97:306–309 (2008)DOI 10.1007/s00392-007-0629-2
CR
C62
9
Tobias Simon and Ruediger Becker con-tributed equally to this work.
T. Simon Æ R. Becker Æ F. VossO. Bikou Æ M. Hauck Æ M. LickaH.A. Katus Æ A. Bauer (&)Dept. of CardiologyUniversity Hospital HeidelbergIm Neuenheimer Feld 41069120 Heidelberg, GermanyTel.: +49-6221/56-8855Fax: +49-6221/56-5514E-Mail:[email protected]

effectiveness of ICD-therapy in this population. Insmaller studies nonsustained ventricular tachycardias(NSVTs) hold prognostic significance regardingarrhythmic events in patients with DCM [3, 7].However, in a larger and multicentric study ICDtherapy failed to reduce all cause mortality in thosepatients [2].
At least in postinfarction patients, the risk factorNSVT exhibits marked spontaneous variability [12].In patients with DCM variability of NSVTs has notbeen systematically elucidated. However, if a highvariability of NSVTs would be present, the clinicalvalue of this selection criterion for implantation ofan ICD would be low and could possibly be onecause for the disappointing results of a recent pri-mary prophylactic ICD-trial [8]. On the other handserial Holter-recordings might overcome this prob-lem.
Currently biomarkers are emerging as an impor-tant tool for the diagnosis and treatment of congestiveheart failure [5, 13]. The prognostic significance ofNT-pro BNP levels in predicting ventricular arrhyth-mias has already been shown in patients with ische-mic cardiomyopathy [9] or in unselected patients withheart failure [4]. In patients with nonischemic car-diomyopathy the predictive value of NT-pro BNPlevels is still unknown. The goal of the present studywas to test whether reproducibility of NSVTs and/orraised NT-pro BNP levels are predictors of arrhythmicevents in patients with DCM.
Methods
In the present study, we enrolled 30 patients withDCM, LVEF £ 40% and without a history of symp-tomatic ventricular arrhythmias. Presence of anischemic cardiomyopathy was excluded by heartcatheterization. Further, an exclusion criterion wasNT-pro BNP levels unavailable at baseline. Holter-recordings were performed on three consecutive days(minimum 3 · 17 h) using a CardioRec Event Re-corder (AD Elektronik, Wetzlar, Germany). NSVTswere defined as ventricular salvos of at least threebeats at a rate of at least 120 beats/min and with aduration <30 s. Reproducibility of NSVTs was definedas presence of NSVTs on more than one day. NT-proBNP levels (Roche, Diagnostics, Mannheim, Ger-many) were determined at baseline (inclusion of thestudy) and on the day of an arrhythmic event. Pa-tients were followed for the occurrence of arrhythmicevents defined as sustained ventricular tachyarrhyth-mias, cardiac arrest and/or unexplained syncopes.Syncopes were defined as unexplained, if the etiologyremained undetermined after thorough evaluation[10].
Statistical analysis
A ROC-curve was computed to identify the optimalcut-off level for differentiation of patients with orwithout arrhythmic event. The Fishers-exact test andthe Wilcoxon/Kruskal–Wallis test were used to eval-uate a significant difference between clinical baselinecharacteristics regarding occurrence of NSVTs/arrhythmic events. Logistic regression analysis wasperformed to test a correlation between multiplevariables and the occurrence of NSVTs/arrhythmicevents. The data are presented as mean ± SEM.
Results
Baseline characteristics of the patients are shown inTable 1. Of the 30 patients 15 (50%) had no NSVTsduring the three consecutive ECG recordings, 9 (30%)had NSVT during one Holter-recording, 3 (10%) hadNSVTs during two Holter-recordings and 3 (10%) hadNSVTs during all three Holter-recordings. Patientswith reproducible NSVTs (presence of NSVTs onmore than one day) had significantly higher NT-proBNP level (first quartile: 715 pg/ml, median 2,176 pg/ml, third quartile 5,755 pg/ml) than patients withoutor NSVTs during one Holter-recording (first quartile273 pg/ml, median 566 pg/ml, third quartile1,350 pg/ml, P = 0.0388, P = 0.0388).
There was no statistically significant correlationbetween sex, age, LVEF, NYHA-class, medication,presence of arterial hypertension at baseline and thefrequency of NSVTs. In a multivariate analysis anelevated NT-pro BNP level was found to be the onlyfactor that correlated with occurrence of frequentNSVTs (P = 0.0049).
During a mean follow-up of 21.6 ± 1.2 months threepatients developed a sustained ventricular tachycardiaand one patient suffered from an unexplained syncopemost likely due to an arrhythmic event. One patient hada monomorphic ventricular tachycardia (Cycle length260 ms) requiring electrical defibrillation. Anotherpatient developed a monomorphic ventricular tachy-cardia (Cycle length 280 ms), which was also success-fully terminated by electrical defibrillation. In a thirdpatient a self-limiting symptomatic polymorphic ven-tricular tachycardia (mean cycle length 290 ms) oc-curred. All four patients received an implantablecardioverter defibrillator.
In terms of non invasive risk predictors the valueof reproducible NSVT was low. There was only atendency towards an increased risk of arrhythmicevents in patients with reproducible NSVTs (presenceof NSVTs on more than one day) compared to pa-tients with NSVTs during one recording or withoutNSVTs (P = 0.0960).
T. Simon et al. 307Elevated B-type natriuretic peptide levels in patients with DCM

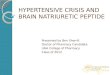
More importantly, raised NT-pro BNP levels werepredictive for arrhythmic events (first quartile:1,002 pg/ml, median 4,075 pg/ml, third quartile7,777 pg/ml vs. first quartile 173 pg/ml, median267 pg/ml, third quartile 1,220 pg/ml, P = 0.0135)(Fig. 1). NT-pro BNP levels of 2,259 pg/ml wereidentified as optimal cut-off value for the predictionof arrhythmic events, characterized by a sensitivity of75% and a specificity of 92.3%. Those patients withsymptomatic ventricular arrhythmias also had highNT-pro BNP levels on the day of the event (patient 1:5,755 pg/ml, patient 2: 4,378 pg/ml, patient 3:2,259 pg/ml, median 5,892 pg/ml).
Discussion
The present study identifies raised NT-pro BNP levelsas a predictor of arrhythmic events in patients with
nonischemic cardiomyopathy and EF < 40%. Incontrast, reproducible NSVTs are less reliable riskfactors predicting occurrence of sustained ventriculararrhythmias.
In patients with ischemic cardiomyopathy the valueof NSVTs for identification of those that will benefitfrom ICDs has already been shown [6, 11]. In contrast,in patients with DCM the predictive value of NSVTs wasrather low [8]. In the DEFINITE-study, patients withDCM, NSVTs and a low left ventricular ejection fractionwere enrolled. As a result, implantation of an ICD re-duced the rate of SCDs, but did not significantly de-crease all cause mortality. Therefore, routineimplantation of ICDs was not recommended by theauthors [8]. As shown in the present study, occurrenceof NSVTs underlies a great degree of variability. In 80%of our patients NSVTs were lacking or occurred only inone out of three consecutive Holter-recordings. Merelyin 10% of the patients NSVT were present in all threeconsecutive Holter-recordings. Therefore, the clinicalvalue of NSVTs as a selection criterion for implantationof an ICD is low. To increase the sensitivity of Holter-recordings, serial Holter-recordings could be per-formed. However, this procedure is not feasible in thedaily routine, since it is expensive, and it requires anexcellent patient’s compliance. More importantly, thepresent study failed to demonstrate a significant cor-relation between reproducibility of NSVTs and occur-rence of sustained ventricular arrhythmias.
In terms of risk stratification determination of NT-pro BNP levels seems to be more reliable. In two re-cent trials log BNP as well as NT-pro BNP levels wereidentified as strong predictors for arrhythmic events[4, 9]. However, those studies particularly enrolledpatients with ischemic cardiomyopathy [9] or anunselected population of patients with heart failure[4]. The present study is the first to demonstrate acorrelation of arrhythmic events and raised NT-proBNP levels in patients with nonischemic cardiomy-opathy. A parameter, as easily to obtain as the NT-proBNP levels, would simplify risk stratification for SCDand may improve candidate selection for ICDimplantation. Since we enrolled only 30 patients intothe present study, future prospective trials of a largerscale are required to confirm our results.
In the present study none of the patients died,which is in contrast to former studies (2.10). In theCAT-trial annual mortality rate was 3.7%, whereas inthe Definite-Trial 6.2% of the patients in the standardgroup died in the first year. These differences mightbe caused by a nearly optimal heart failure medicationof the patients in our study. All patients were on ß-blocker and ACE/ARB-blocker. Most of the patientsreceived spironolactone. Fortunately, those who havehad ventricular arrhythmias or unexplained syncopesuccessfully survived this event.
10000
8000
6000
NT
- pro
BN
P (n
g/I)
4000
2000
00
arrhythmic event
1
Fig. 1 Box plot showing the NT-pro BNP levels in patients with (1) and without(0) arrhythmic event (P = 0.0135)
Table 1 Baseline characteristics of the patients
Clinical characteristicsSex (m/f) 22/8Age (y) 53 ± 2Left ventricular ejection fraction (%) 27.6 ± 1.3
NYHA class (in %)NYHA I 13NYHA II 60NYHA III 27NYHA IV 0Arterial Hypertension (%) 30NT-pro BNP (pg/ml) 1,328 ± 248
Medication at enrollmentDigitalis (%) 30ß-blocker (%) 100ACE-inhibitor/Angiotensin II-receptor blocker (%) 100Spironolactone (%) 80Loop diuretics (%) 80Serum creatinine 1.08 ± 0.28 mg/dlSerum potassium 4.16 ± 0.4 mmol/l
308 Clinical Research in Cardiology, Volume 97, Number 5 (2008)� Steinkopff Verlag 2008

Limitation: Since the number of patients includedin the present study is low, the implications must betreated with caution. A larger randomized study is
required to give general recommendations on riskstratification in patients with non ischemic cardio-myopathy and increased NT-pro BNP values.
References
1. Bardy GH, Lee KL, Mark DB et al forthe Sudden Cardiac Death in HeartFailure Trial (SCD-HeFT) Investigators(2005) Amiodarone or an implantablecardioverter defibrillator for congestiveheart failure. N Engl J Med 352:225–237
2. Bansch D, Antz M, Boczor S et al (2002)Primary prevention of sudden cardiacdeath in idiopathic dilated cardiomy-opathy: the cardiomyopathy trial(CAT). Circulation 105:1453–1458
3. Becker R, Haass M, Ick D et al (2003)Role of nonsustained ventriculartachycardia and programmed ventric-ular stimulation for risk stratificationin patients with idiopathic dilated car-diomyopathy. Basic Res Cardiol98:259–266
4. Berger R, Huelsman M, Strecker K et al(2002) B-type natriuretic peptide pre-dicts sudden death in patients withchronic heart failure. Circulation105:2392–2397
5. Bohm M, Werner N, Kindermann M(2006) Drug treatment of chronic heartfailure. Clin Res Cardiol 95:36–56
6. Buxton AE, Lee KL, Fisher JD et al(1999) A randomized study of theprevention of sudden death in patientswith coronary artery disease. Multi-center Unsustained Tachycardia TrialInvestigators. N Engl J Med 341:1882–1890
7. Grimm W, Glaveris C, Hoffmann J et al(2000) Arrhythmia risk stratification inidiopathic dilated cardiomyopathybased on echocardiography and 12-lead, signal-averaged, and 24-h Holterelectrocardiogarphy. Am Heart J140:43–51
8. Kadish AH, Dyer A, Daubert JP et al(2004) Prophylactic ICD-Implantationin patients with non-ischemic dilatedcardiomyopathy. N Engl J Med350:2151–2158
9. Klingenberg R, Zugck C, Becker R et al(2006) Raised B-type natriuretic pep-tide predicts implantable cardioverter–defibrillator therapy in patients withischemic cardiomyopathy. Heart92:1323–1324
10. Linzer M, Yang EH, Estes M for theClinical Efficacy Assessment Project ofthe American College of Physicians(1977) Clinical Guideline. Diagnosingsyncope. Part 2: Unexplained syncope.Ann Intern Med 127:76–86
11. Moss AJ, Hall WJ, Cannom DS et al forthe multicenter automatic defibrillatorimplantation trial investigators (1996)Improved survival with an implantabledefibrillator in patients with coronarydisease at high risk for ventriculararrhythmia. N Engl J Med 335:1933–1940
12. Senges JC, Becker R, Schreiner K et al(2002) Variability of holter electrocar-diographic findings in patients fulfill-ing the noninvasive MADIT criteria.Pacing Clin Electrophysiol 25:183–190
13. Weil J, Schunkert H (2006) Patho-physiology of chronic heart failure.Clin Res Cardiol 95:1–17
T. Simon et al. 309Elevated B-type natriuretic peptide levels in patients with DCM