Embed Size (px)
Citation preview

J Am Acad Audiol 17:45–68 (2006)
45
*Hearing and Speech Department, University of Kansas Medical Center; †Department of Communication Science andDisorders, University of Pittsburgh
John A. Ferraro, Ph.D., Hearing and Speech Department, University of Kansas Medical Center, 39th and Rainbow Blvd.,Kansas City, KS 66160-7605; Phone: 913-588-5937; Fax: 913-588-5923; E-mail: [email protected]
Electrocochleography in the Evaluation ofPatients with Ménière’s Disease/Endolymphatic Hydrops
John A. Ferraro*John D. Durrant†
Abstract
Electrocochleography (ECochG) has evolved as an important tool in thediagnosis/assessment/monitoring of Ménière’s disease/endolymphatic hydrops(MD/ELH).This manuscript provides an update on the use of ECochG for thesepurposes.The material presented includes descriptions of the components ofthe electrocochleogram; ECochG recording approaches and parameters; howto prepare for an exam, including subject/patient considerations; constructionand placement of a tympanic membrane recording electrode; and interpretationthe electrocochleogram. Various approaches aimed at improving ECochG’ssensitivity and specificity to MD/ELH also are described. These approachesgo beyond simple measurement of the now-conventional summating potential(SP)/action potential (AP) magnitude ratio to include the SP magnitude totonebursts, the SP/AP area ratio, and the AP latency difference to clicks ofopposing polarity.
Key Words: Action potential, auditory brainstem response, auditory evokedpotentials, broadband click, cochlear microphonic, electrocochleography,extratympanic, Ménière’s disease/endolymphatic hydrops, summating potential,toneburst, transtympanic, tympanic membrane, tymptrode
Abbreviations: ABR = auditory brainstem response; AC = alternating current;AP = action potential; AEP = auditory evoked potential; BBC = broadband click;CM = cochlear microphonic; ECochG = electrocochleography; ET =extratympanic; MD/ELH = Ménière’s disease/endolymphatic hydrops; SP =summating potential; TM = tympanic membrane; TT = transtympanic
Sumario
La electrococleografía (ECochG) ha evolucionado como una importante her-ramienta en el diagnóstico, evaluación y monitoreo de la enfermedad deMénière-hydrops endolinfático (MD/HEL). Este manuscrito aporta una actu-alización en el uso de la ECochG para estos propósitos. El material presentadoincluye descripción de los componentes del electrococleograma; parámetrosy enfoques de registro del ECochG; cómo prepararse para un examen,incluyendo consideraciones para el sujeto/paciente; construcción y colocaciónde un electrodo de registro en la membrana timpánica, e interpretación delelectrococleograma. Se describen también varios enfoques orientados a mejo-rar la sensibilidad y la especificidad de la ECochG en la MD/HEL. Estosenfoques van más allá de la simple medición de la convencional tasa de mag-nitud del potencia de suma (SP)/potencial de acción (AP), e incluyen la magnituddel SP para bursts tonales, la tasa de área de SP/AP y la diferencia de laten-cia del AP a clics de polaridad opuesta.

Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
46
As the term implies,“Electrocochleography”(ECochG) is a technique for recordingthe electrical events of the cochlea.
The clinical application of ECochG, however,is confined to the stimulus-related cochlearpotentials and often includes measurementof the whole nerve or compound actionpotential (AP) of the auditory nerve.As shown
in Figure 1, an “electrocochleogram” maycomprise the cochlear microphonic (CM),cochlear summating potential (SP), and AP,recorded independently or in variouscombinations. Although the tracings in thisfigure were recorded in response to broadbandclicks, tonal stimuli also are commonly usedto evoke the components of interest.
ECochG emerged as a clinical tool in the1970s, even though attempts to record the CMfrom humans date back almost to the time ofits discovery in the cat by Wever and Bray(1930) (e.g., Fromm et al, 1935;Andreev et al,1939; Perlman and Case, 1941; Lempert et al,1947; Lempert et al, 1950). The SP wasdescribed in animals in 1950 (Davis et al,1950; von Bekesy, 1950) but received little tono attention in humans until much later(e.g., Eggermont, 1976; Gibson et al, 1977;Gibson, 1978). The first recordings of humanauditory nerve APs are credited to Rubenand his colleagues (1960), who performedtheir measurements on patients undergoingotologic surgery.
Increased attention to all auditory evokedpotentials (AEPs) began to occur in the early1970s, following the discovery and clinicalapplication of the auditory brainstemresponse (ABR). The development andrefinement of noninvasive recordingtechniques also facilitated the clinicalapplication of AEPs, including ECochG.
The technical capability to record cochlearand auditory nerve potentials in humans hasled to a variety of clinical applications forECochG, chief among them being a tool inthe diagnosis/assessment/ monitoring ofMénière’s disease/ endolymphatic hydrops
Palabras Clave: Potencial de acción, respuesta del tallo cerebral, potencialesevocados audit ivos, cl ic de banda ancha, microfónica coclear,electrococleografía, extra-timpánico, enfermedad de Ménière/hydropsendolinfático, potencial de suma, burst tonal, trans-timpánico, membranatimpánica, electrodo para-timpánico
Abreviaturas: ABR = respuesta auditiva del tallo cerebral; AC = corriente alterna;AP = potencial de acción; AEP = potencial evocado auditivo; BBC = clic de bandaancha, CM = microfónica coclear; ECochG = electrococleografía; ET = extra-timpánico; MD/ELH = enfermedad de Ménière/hydrops endolinfático; SP =potencial de suma; TM = membrana timpánica; TT = trans-timpánico
Figure 1. Electrocochleograms evoked by broad-band click stimuli.Top tracings show responses to rar-efaction (R) and condensation (C) polarity clicks.Adding R and C responses (middle tracing) enhancesthe Summating Potential (SP) and auditory nerveAction Potential (AP), which are not phase-locked tothe stimulus. Subtracting R and C responses (bottomtracing) enhances the Cochlear Microphonic (CM)(from American Speech-Language-Hearing Associa-tion, 1988, p. 9, based on data from Coats, 1981).

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
47
(MD/ELH) and the assessment/monitoringof treatment strategies for these disorders.Thematerial for this article has been organized toinclude brief descriptions of the salientfeatures of the components of anelectrocochleogram, and how ECochG isrecorded, interpreted and used clinically,especially with reference to the aboveapplication. Much of this information isderived from recent chapters by the authorson ECochG (Ferraro, 2000; Ferraro andDurrant, 2002), and the reader is referred tothese chapters for supplemental reading inthis area.
ECOCHG COMPONENTS
Detailed descriptions of the CM, SP, andAP are abundant in the hearing science
literature and beyond the scope of this article.However, be assured that the practice ofperforming ECochG should not be attemptedwithout a thorough and working knowledgeof auditory electrophysiology. The followingsection summarizes the salient features of theCM, SP, and AP, especially as related toclinical ECochG.
CM
The CM is an alternating current (AC)voltage that reflects the instantaneousdisplacement of the basilar membrane alongsome distance within the cochlea (Ferraroand Durrant, 2002). This distance is definedby the effective site and method of therecording, and the conditions of the stimulus.As reflected by the CM, the organ of Corti acts(in a limited way) as a microphone, but herethe tranducers are numerous as each hair cellproduces a receptor potential that issubstantially AC (but not exclusively; seesection on SP below). In animals, the CM isperhaps the most thoroughly investigatedelectrical potential of the inner ear, but itcertainly remains to be fully understood. Thehistorical popularity of the CM in thelaboratory derives from its link to cochleartransduction, from well-demonstratedsensitivity to the health of the cochlearpartition, and, certainly, because it can berecorded from within or near the cochlea.This latter factor is facilitated by the CM’sconsiderable magnitude compared to otherelectrical phenomena associated with theauditory periphery. One would think that
such features would render the CM an idealtool for human clinical applications. In reality,however, the utility of the CM in differentialdiagnosis of inner ear versus auditory nervedisorders has yet to be established. Althoughreductions in CM magnitude have beenreported for various disorders such asMD/ELH (Gibson and Beagley, 1976), thesefeatures tend to reflect general rather thanspecific cochlear pathology. Furthermore,examination of the CM with confidence thatthe recording represents the true potentialremains challenging in the clinical setting.Since the CM mimics the waveform of theevoking signal (just as the voltage output ofa microphone), it is difficult to separate fromstimulus artifact.
SP
The SP is a complex response comprisingseveral components. Like the CM, the SP isstimulus related, generated by the hair cellsof the organ of Corti, and a reflection of thedisplacement-time pattern of the cochlearpartition. However, whereas the CM mirrorsthe stimulus waveform (i.e., time history),the SP displays a rectified, direct current(DC) version of this pattern morerepresentative of the stimulus envelope(Dallos, 1973). The SP appears as aunidirectional shift in the CM baseline, thepolarity of which is dictated by an interactiveeffect between stimulus parameters (i.e.,frequency and intensity) and the location ofthe recording electrode. When recorded fromthe tympanic membrane (TM) or ear canal,the SP is often seen as a downward (negative)deflection persisting for the duration of theacoustic stimulus (see Figure 1).
Because of its complexity, the role of theSP in hearing function remains unclear. AsDC responses to AC stimuli, however, at leastsome of its components are thought torepresent nonlinearities associated with thetransduction processes in the cochlea (Tasakiet al, 1954; Whitfield and Ross, 1965; Davis,1968; Engebretson and Eldridge, 1968; Dalloset al, 1972; Gulick et al, 1989; Ruth, 1994).Whether or not the SP actually reflectedintracellular receptor potentials wasuncertain for a period of time following itsdiscovery. However, SP-like potentials havesince been observed inside hair cells, and itis now clear and that the SP is not anepiphenomenon (e.g., Dallos, 1973). It also

48
Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
has long been known that the SP is alsosensitive to mechanical and electrical biasing(Durrant and Dallos, 1972; Durrant and Gans,1977). The nonlinear nature of the SP hasmade it useful for monitoring certain clinicalconditions such as MD/ELH, which mayaugment nonlinearities in the transductionprocess. This application will be discussedlater.
AP
The AP recorded via ECochG representsthe summed response of numerous, at timesthousands of, auditory nerve fibers firingsynchronously.When evoked by click stimuli,the term “whole nerve AP” is applied since,theoretically, the click has a nearly flatspectrum over the frequency range of interestand thus vibrates essentially the entirebasilar membrane. As recorded clinically,however, and regardless of the stimulus, theAP is clearly a compound action potential—-the response of a population of neuronsrather than a single unit. A stimulus with anarrower bandwidth, such as a toneburst,excites a more limited segment of themembrane and, consequently, a morerestricted population of nerve fibers. Here,then, the term “whole-nerve” can bemisleading. More important is the fact thatthese very different stimuli—clicks andtonebursts—fail to achieve their respectiveobjectives. That is, the spectrum of the clickthat actually reaches the cochlea generally isfar from flat, due to combined earphone, earcanal, and middle ear responsecharacteristics. Likewise, the cochlearresponse to tonebursts is far from discrete,due to their spectra and limited cochlearresolution (Durrant, 1986).Thus, clicks do notexcite the “whole” nerve, and even toneburstsexcite several points of vibration along thebasilar membrane.
A high degree of synchrony of neuralfirings is essential to producing a well-definedAP, which accounts for the popularity of clickand brief/abrupt-onset tonebursts as evokingstimuli. In either case, however, the responseto moderately intense stimulation (i.e., 70dB nHL or more) tends to be dominated byneural contributions from the basal or high-frequency end of the cochlea (Kiang, 1965),at least in normal ears and pathological earswith no worse than moderate hearing loss.Since the velocity of the traveling wave is the
highest in this region, phase shifts caused bycochlear mechanics are minimal.
The AP, like the CM, is an AC voltage.However, unlike either of the cochlearpotentials whose waveforms reflect thedisplacement-time pattern of the cochlearpartition (i.e., the CM and SP), the APwaveform is characterized by a series of brief,predominantly negative peaks representativeof the distribution of underlying neuralfirings. At suprathreshold stimulus levels,the first and largest of these peaks is referredto as N1. N1 is virtually the same componentas wave I of the ABR and, as such, arises fromthe distal portion of the auditory nerve(Moller and Janetta, 1983). AP peaks beyondN1 (such as N2 and N3) are analogous tocorresponding ABR components (i.e., wavesII and III) but have received little if anyclinical attention in ECochG.
For clinical purposes, AP magnitude andlatency appear to be the most useful features.The former is a reflection of the number ofnerve fibers firing. Since the afferent fibersof the auditory nerve primarily innervatethe inner hair cells (Spoendlin, 1966), APmagnitude also can be viewed as a reflectionof inner hair cell output. AP latency , whichis analogous to the “absolute latency” forABR components, represents the timebetween stimulus onset and the peak of N1.This value incorporates stimulus travel timefrom the output of the transducer to the innerear, traveling wave propagation time alongthe basilar membrane and time consumedactivating synaptic transmission betweenhair cells and first order neurons. As with allwaves of the ABR, reductions in signalintensity at suprathreshold levels for the APare accompanied by absolute latencyprolongations and reductions in N1magnitude leading to eventual disappearanceinto the electrical noise floor.
Since its initial recording in humans in1960, the AP has been the most widelystudied product of ECochG. Early interestin the AP, however, was directed toward thedevelopment of an electrophysiological indexof hearing status in children (Cullen et al.,1972). This effort was overshadowed by theABR for such purposes, primarily becausewave V of the ABR appeared to be moresensitive and easier to measure than the AP-N1.As AEP applications and technology haveevolved over the years, the use of the AP toassess and monitor cochlear and auditory

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
49
nerve function has received renewedattention, especially in surgical settings. Inaddition, the use of a combined AP-ABRapproach for assessing retrocochlear statusin hard-of-hearing subjects is gainingpopularity. Finally, an important applicationof the AP that will be discussed in more detaillater in this paper involves the measurementof its magnitude in comparison to that of theSP in patients suspected of having MD/ELH.
ECOCHG RECORDING APPROACHES
Transtympanic versus ExtratympanicECochG
The terms “transtympanic” (TT) and“extratympanic” (ET) refer to the two generalapproaches for recording ECochG.TT ECochGis an invasive procedure that involves passinga needle electrode through the TM to rest onthe cochlear promontory. A ball electrode onthe round window can also be used when themiddle ear space is exposed during surgery.TT approaches to ECochG were introduced inthe late 1960s (e.g., Yoshie et al, 1967; Aranand LeBert, 1968) and are still used widelyin countries other than the United States.
ET recordings are performed with anelectrode resting against the skin of the earcanal or surface of the TM. For the lattersite, the procedure may be referred to as“tympanic (or TM) ECochG” (Ferraro andFerguson, 1989), even though this approachis still considered to be ET. Pioneering workin ET recordings was performed by Sohmerand Feinmesser (1967), Coats and Dickey(1970), and Cullen et al (1972), among others.Although ET ECochG can be performed usinga needle electrode in the skin of the ear canal,this option is rarely chosen. Therefore,virtually all ET recordings are noninvasiveand, by virtue of this feature, have been betteraccepted in the United States than TTtechniques. Examples of currently popular ETelectrodes are shown in Figure 2.
Both TT and ET approaches to ECochGhave advantages and disadvantages. Theprimary advantage of the TT approach is theclose proximity of the recording electrode tothe response generators, which producescomponents of large magnitude withrelatively little signal averaging. The majorlimitations of TT ECochG relate to itsinvasiveness. Such procedures must beperformed by or require the assistance of aphysician and are therefore limited to amedical setting. In addition, penetrating theTM with a needle is painful to the patient,even when local anesthetics are used. Thesedisadvantages certainly have limited the useof TT ECochG in the United States.
By comparison, ECochG responsesrecorded from ET sites require more signalaveraging and tend to yield smallercomponent magnitudes than TT recordings.The biggest advantage of ET approaches,thus, is that they can be performed innonmedical settings with minimal discomfortto the patient, obviating the need forsedation/local anesthesia—and a physician.Another factor that has facilitated the use ofET ECochG relates to advances in electrodedesign (discussed in following section) and thepractice of using the TM as a recording site.The TM offers a good and practicalcompromise between ear canal and TTplacements with respect to componentmagnitudes and, consequently, signalaveraging time (Ruth and Lambert, 1989;Ferraro, Thedinger, et al, 1994; Ferraro,Blackwell, et al, 1994; Schoonhoven et al,1995). Perhaps most importantly for clinicalpurposes, however, the waveform patterns
Figure 2. Photographs of extratympanic ECochGelectrodes. Tymptrode (modified version of electrodedescribed by Stypulkoswski and Staller [1987]) (topleft), Lilly wick electrode (top right), and Bio-LogicECochGtrode (middle) are placed at the surface of thetympanic membrane. Gold-foil TIPtrode (bottom)rests in the ear canal. From Ferraro (2000, p. 429).

Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
50
that lead to the interpretation of the TTelectrocochleogram tend to be preserved inTM recordings (Ferraro, Thedinger, et al,1994).When performed correctly,TM ECochGshould cause minimal-to-no discomfort to thepatient. However, the technique of placing anelectrode on the highly sensitive TM cansometimes result in more patient discomfortthan is customary for other, noninvasive ETapproaches (but certainly not as much as isusually associated with TT ECochG).
Given the advantages and disadvantagesof both approaches, the decision to performET or TT ECochG often depends on thetraditional practices, personnel, and attitudesof the clinic. Obviously, TT recordings aredependent on the availability of a physicianwho has the time and interest to performthe examination. While a physician is notneeded for ET ECochG, placing an electrodeon the TM is certainly a more delicatemaneuver than attaching surface electrodesto the scalp or resting them in the ear canal.With proper instruction and materials,however, this procedure is relatively easy tolearn and well within the scope of professionalpractice for audiologists (American Speech-Language-Hearing Association, 1990).
Unfortunately, one factor that is virtuallyoverlooked in the decision to perform TT orET ECochG is the attitude/preference of thepatient. Given the choice with anunderstanding of the benefits and limitationsof each approach, which one would you choose
if you were the patient?
ECOCHG RECORDING PARAMETERS
Selection of recording parameters forECochG varies according to the
components of interest. Since thesecomponents generally occur within a latencyepoch of 5 msec following stimulus onset,they can be considered to be in the family of“early-latency” or “short-latency”AEPs (Pictonet al, 1974). As members of the same family,ECochG components and the ABR can berecorded using similar parameters.A notableexception occurs in the selection of thebandpass of the preamplifier for ECochGwhen the SP is of interest. That is, the filtersetting must be wide enough to accommodateboth a quasi-steady-state DC component (theSP) and an AC component with afundamental frequency of approximately 1kHz (the AP). Other differences betweenECochG and ABR recording parametersinvolve the electrode array and the numberof samples to be averaged. For ECochG, thelatter is dependent on the choice of recordingapproaches, with TT requiring considerablyfewer repetitions than ET. Table 1 illustratessuitable ET (TM) protocol for recording theSP and AP together, which often is done whenECochG is used in the diagnosis of MD/ELH.A description of these parameters is providedbelow.
Table 1. Extratympanic (Tympanic) ECochG Recording Protocol
Electrode Array
Primary (+) Tympanic MembraneSecondary (-) Contralateral Mastoid or EarlobeCommon Nasion
Recording Parameters
Timebase 10 millisecondsAmplification 50,000 XAnalog Filter Bandpass 5 Hz--3000 HzRepetitions 750--1000
Stimuli
Type Broadband Clicks (BBC), Tonebursts (TB)Duration of Electrical Pulse(BBC) 100 microsecondsFrequency (TB) 1000 Hz, 2000 HzEnvelope (TB) 2 millisecond linear rise/fall, 10 millisecond plateauPolarity Rarefaction, Condensation (BBC); Alternating (TB)Repetition Rate 11.3/secondBeginning Level 80 dB nHL

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
51
Electrode Array
If your preference is an electrode arraythat displays the AP as a downward(negative) deflection. The primary electrode(i.e., the electrode connected to the+/noninverting input of the differentialpreamplifier) should rest on the TM. Sites forthe secondary (-/inverting) electrode includethe vertex of the scalp, high forehead,contralateral earlobe, or mastoid process. Weprefer the earlobe or mastoid for the locationof the secondary (-) electrode simply becauseelectrodes tend to be easier to attach andsecure to these sites. The nasion, ipsilateralearlobe, or ipsilateral mastoid may serve assites for the electrode connected to the“common” or “ground” input to thepreamplifier. If you prefer the AP to bedisplayed as an upward deflection (such as inthe way conventional ABR components aredisplayed), simply reverse the + and - inputsto the preamplifier.
Timebase
As indicated above, ECochG componentsgenerally occur within the first fewmilliseconds after stimulus onset. For brieftransient stimuli (such as clicks), we use atimebase (or signal averaging window) of 10msec, which also allows for visualization ofABR components that follow N1. For longerduration stimuli (such as tonebursts), thetimebase should extend beyond the durationof the stimulus envelope so that the entireresponse is observable within the averagingwindow (recalling that both the SP and CMpersist for the duration of the stimulus).
Amplification Factor
Amplification factor is selected tomaximize the signal-to-noise ratio for a givenrecording condition. The amount needed forsuitable recordings of the SP and/or AP forET measurements generally ranges between20,000 and 100,000X, whereas the factor forTT recordings can be much lower (by 5 to 10times). In part, selection of this parameter isbased on the level of the electrical noise floor,which comprises several elements (i.e.,myogenic and electroencephalographicactivity, electrical artifact from the equipmentand/or testing environment). The sensitivitysetting of the computer’s analog-to-digital
converter also must be taken into account.Thus, amplification/sensitivity settings mayvary from laboratory to laboratory and alsoamong evoked potential units from differentmanufacturers. However, the manipulation ofthese variables to provide settingsappropriate to recording conditions generallyis easily accomplished. The goal here is toamplify enough to extract a good (and real)response without triggering the artifactrejection routine inordinately throughout therecording.
Analog Filter Settings
Adaptation notwithstanding, the SP, asfundamentally a DC potential, could last aslong as the stimulus of any duration. Ideally,then, a DC recording amplifier is needed torecord this component. However, particularlyfor the amount of gain needed, such amplifiersare notoriously unstable forelectrophysiological recordings. Fortunately,the SP, as evoked for practical/clinicalpurposes, is only quasi-steady-state,permitting the use of the AC-coupledamplifiers typically found in commerciallymanufactured AEP units. Indeed, the clickevokes a rather brief transient DC componentthat is readily recorded with low-pass cutoffsin the vicinity of 5–100 Hz, depending uponfilter characteristics. Such recordings (i.e.,using familiar ABR settings) can beaccomplished without significant distortionof the SP-AP complex for purposes ofmeasuring the SP/AP magnitude ratio(Durrant and Ferraro, 1991). However, whenrecording the SP to tonebursts, this approachcreates a DC-step-like waveform, and, evenif only quasi-steady-state, the waveform islikely to be significantly distorted unless thelow-frequency cutoff of the amplifier is low(generally 10 Hz or below, depending onduration of the sound and the filtercharacteristics).
The low-pass (or high-frequency cutoff)setting of the filter should be set to allowtransmission of the AC components ofinterest. In the case of the AP-N1, 3000 Hzis a suitable setting as the fundamentalfrequency of this component is approximately1000 Hz. Filter settings for CM recordingswould depend on the frequencies of theevoking stimuli (and thus the resultantresponses).

Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
52
Repetitions
The number of individual responsesneeded to extract a well-definedelectrocochleogram from the backgroundnoise generally varies with recordingconditions, and also the subject’s degree ofhearing loss. The former depends on therecording approach. That is, TT recordingsrequire considerably fewer repetitions thanET approaches. More repetitions may benecessary for subjects with hearing loss thannormally hearing subjects, especially if theloss is in the 1–4 kHz range. In ourexperience, when sensorineural hearing lossin these frequencies exceeds 50–60 dB HL, theuse of ET ECochG in MD/ELH populationsis questionable. The basis for this statementis that losses of this magnitude reduce theoutput of the population of hair cellscontributing to the responses of interest andrender them too small for reliable ETrecordings. On the other hand, when hearingloss precludes the identification of wave I inthe presence of wave V in the conventionallyrecorded ABR, ECochG can be very useful(Ferraro and Ferguson, 1989).
Stimuli
As mentioned earlier, the broadband click(BBC) is a popular stimulus for short-latencyAEPs because it excites synchronousdischarges from a large population of neuronsto produce well-defined peaks in the response.In addition, 100 msec is a popular choice forthe duration of the electrical pulse driving thetransducer because the first spectral null fora click of this duration occurs at 10,000 Hz(i.e., 1/100 msec). In reality, the frequencyrange of the transducer is usually lower than10,000 Hz and the acoustic signal receivesadditional filtering by the outer and middleears. Thus, the spectrum of the stimulusreaching the cochlea is far from flat, andconsiderably narrower than 10,000 Hz.
Since the duration of both the CM and SPare stimulus dependent, the brevity of theclick makes it a less-than-ideal stimulus forstudying either of these potentials. Despitethis limitation, the use of clicks has proveneffective in evoking the SP-AP complex forECochG applications related to MD/ELH,even though the duration of the SP isabbreviated under these conditions (Durrantand Ferraro, 1991). This feature will receive
more attention later.Although the click continues to remain
popular, toneburst stimuli also have beenused in several ECochG studies involvingMD/ELH populations (e.g., Levine et al, 1992;Orchik et al, 1993; Ferraro, Blackwell, et al,1994; Ferraro,Thedinger, et al, 1994; Koyuncuet al, 1994; Margolis et al, 1995). Tone burstsprovide a higher degree of responsefrequency-specificity than clicks (dependingon stimulus envelope and duration), whichcan be useful for monitoring cochlear statusin progressive disorders where hearing maynot be affected at all frequencies. In addition,the use of longer stimuli allows for bettervisualization of the SP and CM (Durrant andFerraro, 1991).
A lack of standardization regardingstimulus parameters presents a problemwhen using tonebursts to record ECochGcomponents and other AEPs. Most studiesemploy signals of only one or two frequencies;stimulus envelopes are different, and thereis no standardized approach to definingstimulus intensity. These inconsistenciesmake it difficult to compare data fromdifferent studies/clinics. For tone bursts, weuse an envelope with a linear rise-fall timeof 1–2 msec and a plateau of 10 msec orlonger. Shorter plateaus (e.g., 5 msec) cansometimes be used to inhibit (but generallynot eliminate) interference by ABRcomponents (Levine et al, 1992).
Stimulus polarity depends on the initialdeflection of the transducer diaphragm andis an important factor for ECochG. Presentingclicks or tonebursts in alternating polarityinhibits the presence of stimulus artifact andCM, as their phases are locked to the signal.Stimulus artifact can sometimes be largeenough to obscure early ECochG components,and CM generally overshadows both the SPand AP features that are problematic whenthese latter two components potentials are thecomponents of interest.Alternating stimuluspolarity can be applied to help overcome thisproblem. However, recording separateresponses to condensation and rarefactionclicks then adding them together off-line maybe a more preferable solution, since certainsubjects with MD/ELH display abnormallatency differences between AP-N1 latenciesto condensation versus rarefaction clicks(Margolis and Lilly, 1989; Levine et al, 1992;Margolis et al, 1992; Margolis et al, 1995;Orchik et al, 1997; Sass et al, 1997).

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
53
As with the majority of signal-averagedAEPs, it is important for ECochG that thecochlear/neural responses to one stimulus becomplete before the next stimulus isintroduced. This requirement allows forconsiderable latitude in the selection ofstimulus repetition rate for click-evoked AEPs.For ECochG, however, increasing this ratebeyond 10–30/second may cause unacceptableadaptation of the AP (Suzuki and Yamane,1982). Click repetition rates on the order of100/second cause extensive (nearly total)adaptation of the AP while leaving the SPrelatively unaffected (Gibson et al, 1977;Coats, 1981). Unfortunately, the use of suchfast rates has not proven to be very successfulin the clinic, in part because the APcontribution is not completely eliminated andthe SP may also be reduced under extremeconditions (e.g., click rates greater than 90/sec)(Harris and Dallos, 1979; Durrant, 1986). Inaddition, rapid clicks presented at loud levelstend to be very annoying for patients.
When ECochG is performed to helpdiagnose MD/ELH, the stimulus should beintense enough to evoke a well-defined SP-AP complex. Thus, stimulus presentationtypically begins at a level near the maximumoutput of the stimulus generator.Unfortunately, as mentioned earlier, the lackof standardization for AEP stimuli regardingsignal calibration and dB reference is true forboth tonebursts and BBCs. Commonreferences include dB hearing level (HL, orhearing threshold level [HTL]), dB normalhearing level (nHL), dB sensation level (SL),and dB peak equivalent sound pressure level(pe SPL). Since the latter one is determinedby matching the SPL of a transient signal tothat of a continuous sinusoid, it represents theonly physical measure of intensity of thethree common references. It may be necessaryto calibrate ECochG signals in both nHL andpe SPL. As with conventional audiometry,nHL values are referenced against normalsubjects. For dB pe SPL, an oscilloscope isused to match the level of the click to that ofa continuous sinusoid (e.g., a 1000 Hz signal).Consistent with the findings of Stapells et al(1982), 0 dB nHL for clicks corresponds toapproximately 30 dB pe SPL.
The use of high stimulus levels raises thequestion of the need for masking to assureunilateral stimulation of the intended ear.This concern is irrelevant for ECochG,however, since the magnitude of any
electrophysiological response from the nontestear is very small. In addition, ECochGcomponents are generated prior to crossoverof the auditory pathway. Finally, the potentialfor crossover stimulation can be furtherminimized by the use of tubal insertearphones.
A final note regarding stimuli relates tostimulus artifact, which can be quite large forECochG. The nature of ET (especially TM)electrodes is that they tend to have highimpedance and are vulnerable to radiationfrom the transducer and other electricalsources in the environment. The followingfactors can help to inhibit such artifact: usinga tubal insert transducer; separating thetransducer from the electrode cables as muchas possible; braiding the electrode cables;testing subjects in a shielded sound boothwith the examiner and AEP unit locatedoutside of the booth; plugging the AEP unitinto an isolated socket equipped with a true-earth ground; using a grounded cable for theprimary electrode (such cables arecommercially available); turning off the lightsin the testing room and unpluggingunnecessary electronic equipment (it alsomay be necessary to turn off the lights inthe examiner room); encasing the transducerin grounded Mu metal shielding.
PREPARING FOR AN EXAMINATION
Recording Approach
Virtually all ECochG recordingsperformed in the authors’ clinics/laboratoriesare ET and made from the TM because of theadvantages this site offers over other locationsalong the ear canal (i.e., increased componentmagnitudes, more stable/repeatableresponses, and reduced testing time becauseless signal averaging is needed)(Stypulkowski and Staller, 1987; Ruth et al.,1988; Ruth and Lambert, 1989; Ferraro andFerguson, 1989; Ruth, 1990; Arsenault andBenitez, 1991). Given our preference for TMECochG, the following informationemphasizes this particular approach.
Subject/Patient Considerations
Most patients are unfamiliar withECochG and therefore confused as to what itis, why they need it, how it will be performed,

Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
54
and whether or not it will be painful. For thelay person (i.e., most patients) the lengthyterm “electrocochleography” adds to thisconfusion. Instructions to the patient canbegin on the way to the testing room with anassurance that the examination isnoninvasive and painless, that the test willtake approximately one hour, and they cansleep through it if they wish. The patientalso is informed as to why their physician hasrequested this examination (e.g., to helpdetermine if there is too much fluid in theinner ear). Engaging patients in conversationat this point and watching them walk alsoprovides some insight regarding the status oftheir hearing and balance, although theresults of other auditory and vestibulartesting should be available in their files. Oncein the sound booth, the patient is placed ina supine position on an examining bed orsemireclined in an examination chair orrecliner. Good and comfortable head and necksupport is particularly important. Eyeglassesand/or earrings are removed (usually by thepatient), and food/chewing gum/candy/etc.must be swallowed or discarded. When thepatient is comfortable and attentive, he or sheis informed that devices called electrodeswill be attached to the scalp, a small, sponge-or cotton-tipped electrode will be insertedalong the ear canal to rest on the TM, and anearplug will be used to hold the electrode inplace and deliver click and beeping-typesounds to the ear. The patient should bealerted that the TM electrode might feelstrange and maybe a little uncomfortable,but that it should not be particularly painful.If pain should occur, repositioning theelectrode usually helps. In very rare instances(i.e., less than 0.5% in the first author’sexperience), the exam may have to beterminated, or an ear canal electrode usedinstead of the tymptrode. The procedures forpreparing the skin and placing the surfaceelectrodes are identical to those used forconventional ABR examinations. Prior toinserting the tymptrode, otoscopy isperformed to assess the patency of the earcanal and normalcy of the TM. Cerumenremoval may be necessary to visualize the TMand clear a pathway along the ear canal largeenough for the electrode. If either the earcanal or TM appear abnormal or damaged,ECochG is not advisable in general, andcertainly not without consulting the patient’sphysician.
As with most audiometric examinations,both ears should be tested, even if unilateraldisease is suspected. Comparison betweenaffected and unaffected sides in particular canprovide important diagnostic information.We always test the affected side first in casethe patient becomes restless as theexamination progresses.
Construction and Placement of theTM Electrode (Tymptrode)
The photograph of ET electrodes inFigure 2 includes the tymptrode (originallydescribed by Stypulkowski and Staller, 1987,and modified by Ferraro and Ferguson, 1989),the Lilly wick electrode (Lilly and Black,1989), the TM-ECochGtrode manufactured byBio-Logic, and the gold-foil TIPtrode, whichhas long been available for ear canalrecordings. The latter three electrodes arecommercially available.The tymptrode can befabricated using the “store bought” materialslisted below (see Durrant, 1990; Ferraro,1992; and Ferraro, 1997):
• medical grade silicon (SilasticTM)tubing (0.058” inner diameter, 0.077”outer diameter;
• TeflonTM-insulated silver wire(0.008” bare diameter, 0.011”insulated diameter);
• a wad of cotton;• electrode gel (not paste or cream);• fine, needle-nosed forceps;• 1 cc disposable tuberculin syringe
with needle;• copper microalligator clip soldered to
the end of an electrode cable.Briefly, the procedure for constructing
the tymptrode involves cutting the wire andtubing into segments a few centimeters longerthan the ear canal, threading the wirethrough the tubing, scraping the Tefloninsulation off of both ends of the wire, hookingone of the bared ends into the cotton wad, andstuffing the hooked portion of the cotton backinto the tubing with fine forceps. A smallportion of the cotton extends beyond thetubing to serve as the electrode tip. Figure 3is a drawing of the tymptrode constructed asdescribed above. Tymptrodes, at this stage,can be made and stockpiled for indefiniteperiods of time. Immediately prior to use,the cotton tip of the tymptrode is impregnatedwith electrode gel using the tuberculinsyringe. We attach the microalligator clip of

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
55
the electrode cable to the other, bared end ofthe wire, before inserting the tymptrode.
With the test ear is facing up, thetymptrode is inserted into the entrance ofthe ear canal and gently advanced (by handor using the fine forceps) until the tip touchesthe TM. Contact is confirmed via otoscopy and
electrophysiological monitoring. It also helpsto ask the patient when they feel that theelectrode is touching the TM. Even with anotoscope, it is difficult to actually see thepoint of contact between the tymptrode tipand TM in most cases. However, monitoringthe electrophysiological noise floor duringelectrode placement helps to achieve propercontact. The noise floor, peak-clipping, andcyclic activity associated with an “open-line”condition drop dramatically, and the baselineEEG becomes more stable when the TM iscontacted. Repositioning and sometimesreinsertion of the tymptrode may be necessaryto achieve proper contact. However, usingboth visual and electrophysiologicalmonitoring provides the best opportunity forsuccess on the “first try.”
Once the tymptrode is in place, the foamtip of the sound delivery tube is compressedand inserted into the ear canal alongside theelectrode tubing. Care must be taken to notpush the electrode further against the TMwhen inserting the earplug. Although thematerials that comprise the tymptrode arerelatively soft and flexible (which allows thetip to compress or bend at the TM ratherthan penetrate the membrane), such acondition usually causes discomfort to thepatient. Only a portion of the transducerearplug needs to be inserted into the canal tohold the tymptrode in place and deliver thesignal for ECochG applications. Figure 4 is aschematic representation of the tymptrodeand sound delivery tube in place. Even withthe most delicate contact, the TM does reactsomewhat in most cases by displaying a slightblushing spot at the point of contact withthe tymptrode. In hundreds of subjects andpatients examined by the authors, thiscondition has never proven to be an untowardreaction, clears up within minutes or hours,and may even be a useful indicator of exactlywhere the electrode was situated.
INTERPRETATION OF THEELECTROCOCHLEOGRAM
As with most AEPs, component magnitudeand temporal features form the bases
for interpreting the electrocochleogram.Figure 5 depicts normal TM recordings toalternating polarity clicks (which enhancesthe SP and AP at the expense of the CM).Component magnitudes can be measured asabsolute values (defined by single points)
Figure 3. Components of the “tymptrode” electrodeused for surface recordings from the tympanic mem-brane.
Figure 4. Schematic illustration of the tymptrode inplace. Modified from Ferraro (1992, p. 28).

Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
56
(left panel) or using a baseline reference(right panel). The authors are split on whichof these two approaches is best, showing thateven authorities of similar background andgenerally similar views can still have differingopinions on how to interpret anelectrocochleogram. In this instance, rightsand wrongs are difficult to define, particularlyunder the electrically “noisy” circumstancesof minimally/non-invasive recordingconditions in awake patients.The first authorfinds the single-point calculations to be themore useful and potentially reliable as itminimizes the judgmental factor of definingan unstable or electrically skewed baselinecommon to ET recordings in general.Theoretically, this approach is subject to nomore or no less noise than single pointschosen to represent the SP and APmagnitudes. However, the second authorprefers using a value representing theaverage through a millisecond or two ofbaseline before the response. At least for oneof the measurements, the noise can bereduced (the average being inherently a“variance reducer”). This method is equallyuseful in determining the SP magnitude fortonebursts, for the same reason in bothcases—minimizing bias by some noise peak.In the final analysis, individual circumstances
may favor one approach over the other, butit probably is the best idea, above all else, totry to be as consistent as possible acrossmeasures in the normative sample andclinical patients. Here, for simplicity, thesingle-point approach is adopted, in whichcase, the normal SP measured from the TMin response to 80 dB nHL clicks may beexpected to range from 0.1–1.0 microvolts,with a mean of 0.4 microvolts.AP magnitudescan be as large as 5.0 microvolts, although ourmean value is approximately 2.0 microvolts.AP-N1 latency is measured from stimulusonset to the peak of N1 and, as mentionedearlier in this manuscript, should be identicalto the absolute latency of ABR wave I. At 80dB nHL, normal N1 latencies generally rangefrom 1.3–1.7 msec with a mean ofapproximately 1.5 msec. Since a tubal insertearphone was used to deliver the stimulus,the above latency values have been correctedfor the 0.9 msec delay attributable to thesound tube. Although labeled in Figure 5,N2 has received little interest for ECochGapplications.
Also as shown in Figure 5, we measureSP and AP magnitudes from the leading edgeof both components. The resultant values arethen used to derive the SP/AP magnituderatio, which is a key measure when ECochG
Figure 5. ECochG recordings from the tympanic membrane to clicks presented in alternating polarity at 80dB nHL.The magnitudes of the Summating Potential (SP) and Action Potential (AP) can be measured from peak-to-trough (left panel), or with reference to a baseline value (right panel). Magnitude/time scale is 1.25 micro-volts/1 millisecond per gradation. Insert phone delay is 0.90 milliseconds. From Ferraro (2000, p. 435).

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
57
is used to help diagnose and monitorMD/ELH. This value tends to occur within arelatively small range (i.e., 0.1–0.5), especiallyin comparison to the individual magnitudesof both the SP and AP (Ferraro and Krishnan,1997).
Figure 6 depicts a normal waveformevoked by an 80 dB nHL, 2000 Hz toneburst(2 msec rise/fall, 10 msec plateau, alternatingpolarity). Recall that for tonebursts the SPpersists as long as the stimulus and thereforeis not seen as a small shoulder preceding theAP (which is still seen near the onset of theresponse). To minimize the influence of theAP, SP magnitude is measured at themidpoint of the waveform with reference tobaseline magnitude. The polarity of the SPdepends on whether this voltage is above(positive SP) or below (negative SP) thebaseline voltage. Figure 7 illustratestoneburst SPs at several frequencies recordedfrom both the TM and promontory (TT) of thesame normally hearing subject. Threeimportant features should be noted fromthese tracings: (1) The polarities of the SPsmay vary slightly across frequencies. (2)Despite these slight variations, themagnitudes of toneburst-SPs in normal earsare very small, which renders the actualpolarity of the SP in this populationsomewhat inconsequential. (3) Although themagnitudes of the TM responses areapproximately one-quarter that of the
promontory responses (note magnitudescales), the corresponding patterns of the TMand TT recordings at each frequency arevirtually identical (as indicated earlier inthis manuscript).
Although clicks and tonebursts are thestimuli of choice for ECochG, it is importantto note that comparisons among studies fromdifferent laboratories/clinics remain difficultat best. This problem persists because of alack of consistency and standardizationregarding such aspects as choice of recordingapproach, recording and stimulus parameters,stimulus calibration, and measurementpreferences. All of these conditions continueto necessitate the establishment of laboratory-/clinic-specific norms for ECochG.
ECOCHG’S ROLE IN THEEVALUATION OF MD/ELH
Although much has been learned aboutMD (or idiopathic ELH) since its initial
description in the literature over 140 yearsago (Ménière, 1861), the true pathophysiologyof this disorder(s) continues to be elusive. Asa result, neither a cure nor an effectivetreatment strategy that works for all patientshas been developed. The symptoms uponwhich diagnosis of MD/ELH is based includerecurrent, spontaneous vertigo, hearing loss,aural fullness, and tinnitus (AmericanAcademy of Otolaryngology—Head and Neck
Figure 6. ECochG recording from the tympanic membrane to a 2,000 Hz toneburst (alternating polarity, 80dB nHL, 2 msec rise/fall, 10 msec plateau). Action Potential (AP) and its first negative peak (N1) are seen atthe onset of the response. Summating Potential (SP) persists as long as the stimulus. SP magnitude is meas-ured at midpoint of response (point B), with reference to a baseline value (point A). From Ferraro, Blackwell,et al. (1994, p. 19).

Surgery Committee on Hearing andEquilibrium, 1995). However, the presenceand severity of these symptoms tend to varyover time both among and within patients.The capricious nature of this disorder makesit difficult to diagnose and evaluate with ahigh degree of specificity and/or sensitivity.
As mentioned throughout this paper,ECochG has emerged as one of the morepowerful tools in the diagnosis, assessment,and monitoring of MD/ELH, primarilythrough the measurement of the SP and AP.In particular, it is now well documented thatthe electrocochleograms of patients withMD/ELH often display abnormally enlargedSP magnitudes (e.g., Schmidt et al, 1974;Gibson et al, 1977; Gibson, 1978; Moriuchi andKumagami, 1979; Morrison et al, 1980; Coats,1981, 1986; Kitahara et al, 1981; Goin et al.,1982; Kumagami et al, 1982; Ferraro et al,1983; Ferraro et al, 1985; Staller, 1986;Dauman et al, 1988; Ruth et al, 1988; Ferraroand Krishnan, 1997). The conventionalrationale for this finding is that an increasein endolymph volume creates mechanicalbiasing of vibration of the organ of Corti towhich, again, the SP is sensitive.Whether thenature of this increased distortion is
mechanical (Gibson et al, 1977) and/orelectrical (Durrant and Dallos, 1972, 1974;Durrant and Gans, 1977) has not beenresolved, and other factors such asbiochemical and/or vascular changes mayalso be responsible (Eggermont, 1976; Goinet al; 1982; Staller, 1986). Regardless of thespecific pathophysiology, measurement of theSP to help diagnose, assess, and monitorMD/ELH has emerged as a primary, andprobably the most popular, application forECochG.
Although it is the enlargement of the SPmagnitude that often characterizes theelectrocochleograms of patients withMD/ELH, the consistency of this finding whenusing click stimuli improves when this valueis compared to the magnitude of AP-N1 toform the SP/AP magnitude ratio (Eggermont,1976; Coats, 1981; Coats, 1986). An enlargedSP/AP magnitude ratio to click stimuli,therefore, would be considered a positivefinding for ELH.This feature is illustrated inFig. 8, which displays the click-evokedelectrocochleogram of a patient with MD/ELHon the left side. As can be seen from thesetracings, the left SP/AP magnitude ratio(when measured using the “single point”
Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
58
Figure 7. Transtympanic (TT) and Tympanic Membrane (TM) electrocochleograms evoked by tonebursts of dif-ferent frequencies presented at 80 dB nHL (2 msec rise fall, 10 msec plateau). Stimulus frequency in kHz indi-cated at the right of each waveform. Despite differences in magnitudes (see magnitude scale),TT and TM responsepatterns are virtually identical. From Ferraro, Blackwell, et al, (1994, p. 20).

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
59
method), is approximately 21/2 times largerthan the normal right ratio. Figure 9 displaysnormal and abnormal toneburst-evokedelectrocochleograms (2000 Hz, 2 msec r/f, 10msec plateau) from another MD/ELH patient.For these measurements, SP magnituderepresents the difference between baseline andmidpoint voltages (recalling that the SP persistsfor the duration of the stimulus).The left paneldisplays an enlarged, negative SP from theaffected left ear, whereas the right response isbarely measurable and well within normallimits. It also should be noted for toneburstresponses that the measurement of interest isthe magnitude of the SP trough rather than theSP/AP magnitude ratio. Indeed, it often is thecase that the AP to tonebursts may not even bevisible in the face of an abnormally enlarged SP.
Although the specificity of ECochG inthe diagnosis of MD/ELH has been reportedto be higher than 90% (Ferraro et al, 1983; Pouet al, 1996; Murphy et al, 1997), the incidenceof an enlarged SP and SP/AP magnitude ratio
in the general Ménière’s population is onlyapproximately 55%–65% and has beenreported to be as low as 20% (Gibson et al,1977; Coats, 1981; Kitahara et al, 1981;Kumagami et al, 1982; Margolis et al, 1995;Pou et al, 1996; Ferraro and Tibbils, 1999).These statistics demand a continuing searchfor ways to make ECochG more sensitive,particularly for patients whose symptoms arenot “classic” and for whom the clinical profileis unclear (Campbell et al, 1992).
The episodic nature of MD/ELH certainlyplays a role in the sensitivity of any diagnostictool used for this disorder. In addition,MD/ELH is characterized by various stages during its evolution within a givenpatient, which manifest differentlyelectrophysiologically (Aran et al, 1984;Horner and Cazals, 1988). Thus, one mightexpect the sensitivity of ECochG to varyaccording to when the test was administeredin the course of the disease. In support ofthis notion, Ferraro et al (1985) found positive
Figure 8. ECochG tracings to broadband clicks (alternating polarity, 80 dB nHL) from a patient with endolym-phatic hydrops. Affected side (left) shows a magnitude-enlarged summating potential (SP), and SP/actionpotential (AP) magnitude ratio. SP-AP relationship on the unaffected side (right) is within normal limits.

electrocochleograms in over 90% of patientswho had active symptoms at the time oftesting that included aural fullness andhearing loss. Pou et al (1996) observedchanges in the SP-AP relationship as afunction of degree of hearing loss. Such lossmay be initially episodic but also tends toprogress with duration of disease. Given theseassociations, one way to make ECochG moresensitive is to test patients when they areexperiencing symptoms. Unfortunately, thepracticality of this idea is questionable giventhe fluctuating nature of the disorder(especially in its early stages), the generaloperating hours of most clinics, and theinability and/or unwillingness of patients tocomplete an examination during an “attack.”Nonetheless, testing patients during or assoon as possible after an episode willsignificantly improve the chances of obtaininga positive electrocochleogram if indeed thepatient has MD/ELH. We also have found ithelpful, especially in the early stages of thedisorder, to test patients when they are
asymptomatic and then retest them whensymptoms are present. Comparingelectrocochleograms under these conditionsoften reveals differences that arediagnostically significant.
Additional evidence for the closerelationship between ECochG and the acutestatus of the inner ear can be seen in casesinvolving intraoperative ECochG monitoringin patients undergoing endolymphaticdecompression/shunt surgery for treatmentof MD/ELH. Although still controversial,decompression or shunting of theendolymphatic sac is an option for patientswho fail nonsurgical treatments. During suchsurgeries, instantaneous measurements ofthe mechanoelectrical processes of the innerear can be achieved via ECochG (Gibson etal, 1988; Gibson and Arenberg, 1991;Arenberget al, 1993; Wazen, 1994; Mishler et al, 1994).Figure 10 exemplifies intraoperative changesin the electrocochleogram induced by probingfor the endolymphatic duct in a patient withMD/ELH. The uppermost tracings display
Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
60
Figure 9. ECochG tracings to a 2,000 Hz toneburst (alternating polarity, 80 dB nHL, 2 msec rise/fall, 10 msecplateau) from another patient with endolymphatic hydrops. Affected side (left panel) displays an enlarged SPtrough, while SP magnitude on unaffected side (right panel) is very small and within normal limits. AP-N1 com-ponent is seen at the onset of the response to toneburst stimuli.

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
61
an enlarged SP and SP/AP magnitude ratio.However, the SP becomes smaller andremains that way after a metal probe ispassed into (and therefore decompresses) theduct (bottom three tracings). Probing ofsurrounding tissue did not alter theelectrocochleogram. Figure 11 displaysselected tracings measured from anotherpatient undergoing endolymphatic sacdecompression surgery.A noticeable reductionin the SP/AP magnitude ratio to click stimuli,and the SP magnitude to tonebursts wereobserved when the sac was decompressed.Although not always the case, this particularpatient reported an improvement insymptoms following surgery.
Beyond the SP/AP Magnitude Ratio
Other approaches to increasing thesensitivity of ECochG have been directedtoward the parameters associated withrecording and interpreting theelectrocochleogram, and looking beyondcomparatively simple measures of SPmagnitude. An example of such a methodinvolves measuring the AP-N1 latency
difference between responses to condensationversus rarefaction clicks (as described earlierin this chapter). Figure 12 illustrates thisprocedure.The AP-N1 latency difference (LD)between clicks of opposite polarity for thisMD/ELH patient was 0.75 msec, which wasconsiderably above the upper limit 0.38 msecseen in normal ears. The basis for comparingAP-N1 latencies to clicks of opposite polarityrelates to changes in the velocity of thetraveling wave in an endolymph-loadedcochlea. That is, the vibratory cycle of thecochlear partition under such conditions maybe abnormally restricted (or enhanced) inone direction over the other. If this conditionoccurs, the velocity of the traveling wave (onwhich the AP-N1 latency is dependent) willdiffer if the initial movement of the cochlearpartition is upwards (as with rarefactionclicks) versus downwards (as withcondensation clicks).
Another interesting feature in Figure 12is that the AP-N1 latency difference is obscuredwhen responses to rarefaction and condensationclicks are combined (lowest tracing). Thisapproach is analogous to presenting clicks inalternating polarity. What appears instead is
Figure 10. ECochG recordings measured at various events during endolymphatic sac decompression surgery.Note the reduction in SP magnitude in the “Probe passed into duct” tracing, which illustrates the relationshipbetween the electrocochleogram and the acute status of the endolymphatic system. This feature is used to helpto differentiate the location of the endolymphatic duct from surrounding tissue during surgery. From Gibsonand Arenberg (1991, p. 300).

an abnormally widened SP-AP complex. It isinteresting to note that Morrison et al (1980)reported a widening of the SP-AP duration inMénière’s patients over 20 years ago. Thisfinding was attributed to an “after-ringing” ofthe CM caused by endolymphatic hydrops. Inlight of recent studies, it may be more likely thatdifferences in AP-N1 latency to condensationversus rarefaction clicks accounted for thewidened SP-AP complex observed by Morrisonet al (who used click stimuli presented inalternating polarity).
Even though the underlying mechanismsmay be unclear, the above studies suggest thatthe width (i.e., duration) of the SP-AP complexmay be important to consider in theinterpretation of the electrocochleogram.Ferraro and Tibbils (1999) explored thisnotion by combining both magnitude andduration features of the response to measurethe “areas” of the SP and AP. Areameasurements were accomplished using aspecial software routine that allowed us tomeasure the “area under the curve” definedby a straight line connecting two cursorpoints. Figure 13 displays representativetracings from this study.The waveforms in the
left panel are from a normal subject, whereasthe right tracings are from an MD/ELHpatient. The shaded portions of the toptracings in both panels represent the area ofSP, which was defined by the onset of the SP(baseline) and that point in the tracing wherethe waveform returned to the baselinemagnitude. Despite its label, thismeasurement also includes the areas ofcomponents other than the SP (such as theAP-N1, and often AP-N2). The shadedportions of the lower tracings represent theAP-N1 area. The results from this studyrevealed that virtually all MD/ELH patientswith enlarged SP/AP magnitude ratios alsohave enlarged SP/AP area ratios. However,enlarged area ratios also were seen in severalpatients suspected of having MD/ELH butwhose SP/AP magnitude ratios were withinnormal limits. Subsequent research in ourlaboratory using data from 138 patients withMD/ELH has shown that measurement ofthe SP/AP area ratio significantly improvesthe diagnostic sensitivity of ECochG incomparison to the SP/AP magnitude ratio(Devaiah et al, 2003).
Given the above findings, we routinely
Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
62
Figure 11. ECochG tracings recorded during endolymphatic shunt decompression surgery: baseline tracing (1),drilling on mastoid (2), probing for endolymphatic duct (3), inserting prosthesis (4), closing (5). Tracing 5 showsa reduction in the summating potential (SP)/action potential (AP) magnitude ratio compared to tracing 1. Trac-ings 1–5 are in response to clicks, whereas tracings 6–7 were recorded to tonebursts at the onset of surgery anddisplay an enlarged SP magnitude. From Ferraro (2000, p. 446).

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
63
Figure 13. Measurement of the areas of the summating potential (SP) and action potential (AP) to click stim-uli to derive the SP/AP area ratio. Area values are obtained using a software routine that allows for measure-ment of the “area under a curve” defined by a straight line that connects two cursor points. Shaded portionsrepresent these areas. Tracings in the top and bottom left panels are from the affected side of a subject withendolymphatic hydrops and display an enlarged SP/AP area ratio. Normal tracings on the right are from theunaffected side. From Ferraro and Tibbils (1999, p. 24).
Figure 12. ECochG tracings to broadband clicks presented in opposing polarity from a patient with Meniere’sdisease. Top tracing evoked with condensation-polarity clicks; middle tracing evoked with rarefaction-polarityclicks. The latency difference of 0.75 milliseconds between AP-N1 components to condensation versus rarefac-tion clicks is a positive finding for endolymphatic hydrops since it is greater than 0.38 milliseconds. This fea-ture is obscured if the condensation and rarefaction tracings are combined to derive the response to alternat-ing clicks (bottom tracing). From Margolis et al (1995, p. 52).

include measurement of the SP/AP area ratioin the interpretation of electrocochleograms.However, we continue to measure the SP/APmagnitude ratio to clicks, the SP magnitudeto tonebursts (1000 and 2000 Hz), and the N1latency difference to clicks of opposite polarity.The question as to which of thesemeasurements (or combination ofmeasurements) is most sensitive to MD/ELHremains to be answered. To address thisissue, we have begun an outcome studyinvolving several hundred patients seen forECochG examinations in our clinic during thepast five years.This project involves assessingthe relationship between the results of anECochG examination (i.e., the individualmeasurements described above) and thesubsequent diagnosis and treatment of thepatient. At this time, the jury is still outregarding the measurement(s) that is mostsensitive to MD/ELH.
A final note regarding the specificity ofECochG relates to enlarged SP/AP magnituderatios in conditions other than MD/ELH. Inparticular, this feature also has been reportedfor perilymphatic fistulae (Kobayashi et al,1993;Ackley et al, 1994; Campbell and Abbas,1993, 1994).Thus, it may be the case that anychange in cochlear fluid pressure that biasescochlear transduction, and therefore the SP,will affect the SP/AP relationship (Stormset al, 1996). However, as implied in earlierdiscussion, definitive proof of this mechanismremains to be seen. Eggermont (1976)questioned the hydromechanical rationaleover two decades ago, suggestingconsideration of possible biochemical changesunderlying or triggered by the fluid pressurechanges—ionic diffusion gradients can bealtered by osmosis and vice versa.
Yamasoba et al (1993) observed enlargedSPs in cases of idiopathic low-frequencyhearing losses, namely patients who have nobalance-related or other symptomscharacteristic of MD/ELH. This findingsuggests that a positive electrocochleogrammay be a manifestation of “cochlear hydrops.”Indeed, we have seen numerous patients whofit this profile. That is, a positiveelectrocochleogram in the face of hearingloss, aural fullness, and tinnitus, but notaccompanied by vertigo. Likewise, we alsohave observed negative electrocochleogramsin dizzy patients whose auditory symptomswere minimal at the time of testing but whowere eventually diagnosed with MD/ELH.
Obviously, more research in this area isneeded to ascertain ECochG’s sensitivity tocochlear versus vestibular hydrops, assumingthat these conditions can exist independently.
As we continue to learn more about theinfrastructure and physiology of the inner ear,it is likely that even more basic mechanismswill be revealed to account for normal andimpaired hair-cell transduction in general.Molecular biological bases, perhaps eveninvolving genetic coding or related processesmay play a role in altering these mechanismsin individuals with MD/ELH to produce thechanges in the SP and other features of theelectrocochleogram described above.
SUMMARY
ECochG has emerged as an important toolin the diagnosis, assessment, and
monitoring of MD/ELH despite continuingdebate on the best ways to record andinterpret responses. In this case, the “bestways” are those that optimize the sensitivityand specificity of ECochG in the evaluationof MD/ELH—while causing minimaldiscomfort to the patient. The following is asummary of the features described in thismanuscript that should be considered in theselection of ECochG parameters to achievethis goal.
• Although ECochG componentsinclude the CM, SP, and AP,measurement of the SP and APcontinues to offer the most usefulinformation in the evaluation ofMD/ELH. While the CM may indeedhave other valuable applications(e.g., in the diagnosis of auditoryneuropathy), its utility for MD/ELHpurposes has yet to be established.
• The authors prefer an ET recordingapproach for ECochG that involvesplacing the primary electrode on theexternal surface of the TM. This siteoffers a good compromise betweenTT and other ET sites regardingcomponent magnitudes, preservationof diagnostic patterns, and testingtime, and can be performed byaudiologists in a nonmedical settingwith minimal-to-no discomfort to thepatient.
• The stimulus and signal averagingparameters associated with ECochGshould be chosen to favor
Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
64

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
65
measurement of the SP and AP,recorded together or separately, andin response to both BBCs andtonebursts.
• The lack of standardized stimuli andstimulus calibration approaches forECochG continues to necessitate theestablishment of laboratory-/clinic-specific normative data.
• Stimulus and other artifact can be abigger problem for TM-ECochG thanfor other AEPs because of thesensitivity/fragility of recording site,the construction, sensitivity, andstability of the recording electrode,and lowering the low-frequencycutoff of the analog filter to allowfor measurement of the SPcomponent. Several suggestions areoffered in this manuscript to helpinhibit such artifact.
• Although the SP/AP magnitude ratioto BBCs appears to be highly specificto MD/ELH (i.e., patients that displayan enlarged ratio are usuallydiagnosed with this disorder), thesensitivity of this measurement (i.e.,the likelihood of finding an enlargedSP/AP magnitude ratio in someonewho has MD/ELH) in the generalMD/ELH population is not as high.This finding demands a continuedsearch for other features of theelectrocochleogram that may improveECochG’s sensitivity.These featuresmay include the SP magnitude totonebursts, the SP/AP area ratio toBBCs, and the latency differencebetween the AP-N1 components toBBCs of opposing polarity. Althoughour data suggest that measurementof the SP/AP area ratio may offer themost sensitivity among the abovevalues, additional research is neededto verify this finding.
• There is a significant relationshipbetween ECochG results and thesymptoms the patient displays atthe time of testing. Thus, one way tomake ECochG more sensitive is totest patients when they aresymptomatic, even though thepracticality of this strategy often islimited.
• Although, as indicated above,ECochG is highly specific to
MD/ELH, enlarged SP/APmagnitude ratios also have beenreported in cases of perilymphaticfistulae and apparent cochlearhydrops. This finding suggests thatthe conditions to which ECochG maybe most specific are changes incochlear fluid pressure.
• The relationship between ECochGresults and symptoms and also tothe acute status of the ear (asobserved in intraoperative recordingsand conditions other than MD/ELHthat cause changes in cochlear fluidpressure), serves to underscore thegeneral truism of ECochG, and allAEP measures for that matter: theyare functional indicators and notpathognomonic of a particulardisorder/disease. Fortunately for thediagnostician, an increased SP/APmagnitude and/or area ratio, orabnormally prolonged AP-N1 latencydifference to BBCs of opposingpolarity are rare in retrocochlearcases and other disorders of hearing.Thus, a positive electrocochleogramcertainly points strongly to a cochleardisorder and most likely an etiologyof MD/ELH.
REFERENCES
Ackley RS, Ferraro JA,Arenberg IK. (1994) Diagnosisof patients with perilymphatic fistula. Semin Hear15:37–41.
American Academy of Otolaryngology–-Head andNeck Surgery. Committee on Hearing andEquilibrium. (1995) Guidelines for the diagnosis andevaluation of therapy in Meniere’s disease. OtolaryngolHead Neck Surg 113:181-185.
American Speech-Language-Hearing Association.(1988) The short latency auditory evoked potentials:a tutorial paper by the Working Group on AuditoryEvoked Potential Measurements of the Committeeon Audiologic Evaluation.
American Speech-Language-Hearing Association.(1990) Competencies in auditory evoked potentialmeasurement and clinical applications. WorkingGroup on Auditory Evoked Potential Measurementsof the Committee on Audiologic Evaluation. Suppl 2.
Andreev AM,Aropova AA, Gersuni SV. (1939) On elec-trical properties in the human cochlea. J PhysiolUSSR 22:206–212.
Aran JM, Lebert G. (1968) Les responses nerveusecochleaires chex l’homme, image du fonctionnementde l’oreille et nouveau test d’audiometrie objectif.Revue de Laryngologie, Otologie, Rhinologie (Bordeaux)89:361–365.

Aran J-M, Rarey KE, Hawkins JE Jr. (1984)Functional and morphological changes in experi-mental endolymphatic hydrops. Acta Otolaryngol97:547–557.
Arenberg IK. (1980) Abnormalities, congenital abnor-malities and unusual anatomic variations of theendolymphatic sac and vestibular aqueduct: clinical,surgical and radiographic correlations. Am J Otol2:118–149.
Arenberg IK, Gibson WPR, Bohlen HKH.(1993)Improvements in audiometric and electrophysiologicparameters following nondestructive inner ear sur-gery utilizing a valved shunt for hydrops andMeniere’s disease. Proceedings of the Sixth AnnualWorkhops on Electrocochleography & OtoacousticEmissions. Denver, CO: International Meniere’sDisease Research Institute, 545–561.
Arsenault MD, Benitez JT. (1991)Electrocochleography: a method for making theStypulkowski-Staller electrode and testing technique.Ear Hear 12:358–360.
Campbell KC, Abbas PJ. (1993) Electrocochleographywith postural changes in perilymphatic fistula andMeniere’s disease: case reports. J Am Acad Audiol4:376–383.
Campbell KC, Abbas PJ. (1994) Electrocochleographywith postural changes in perilymphatic fistula.Animalstudies. Ann Otol Rhinol Laryngol 103:474–482.
Campbell KC, Harker LA, Abbas PJ. (1992)Interpretation of electrocochleography in Meniere’sdisease and normal subjects. Ann Otol RhinolLaryngol 101:496–500.
Coats AC. (1981) The summating potential andMeniere’s disease. Arch Otolaryngol 104:199–208.
Coats AC. (1986) Electrocochleography: recordingtechnique and clinical applications. Semin Hear7:247–266.
Coats AC, Dickey JR. (1970) Non-surgical recordingof human auditory nerve action potentials andcochlear microphonics. Ann Otol Rhinol Laryngol29:844–851.
Cullen JK, Ellis MS, Berlin CI, Lousteau RJ. (1972)Human acoustic nerve action potential recordingsfrom the tympanic membrane without anesthesia.Acta Otolaryngologica 74:15–22.
Dallos P. (1973) The Auditory Periphery: Biophysicsand Physiology. New York: Academic Press.
Dallos P, Schoeny ZG, Cheatham MA. (1972) Cochlearsummating potentials: descriptive aspects. ActaOtolaryngologica 301(Suppl.):1–46.
Dauman R, Aran JM, Sauvage RC, Portmann M.(1988) Clinical significance of the summating poten-tial in Meniere’s disease. Am J Otol 9:31–38.
Davis H. (1968) Mechanisms of the inner ear. AnnOtol Rhinol Laryngol 77:644–656.
Davis H, Fernandez C, McAuliffe DR. (1950) The exci-tatory process in the cochlea. Proc Natl Acad Sci36:580–587.
Devaiah AK, Dawson KL, Ferraro JA, Ator G. (2003)Utility of area curve ratio: electrocochleography inearly Meniere’s Disease. Arch Otolaryngol Head NeckSurg 129:547–551.
Durrant JD. (1981) Auditory physiology and an audi-tory physiologist’s view of tinnitus. J Laryngol Otol4(Suppl.):21–28.
Durrant JD. (1986) Combined ECochG-ABR versusconventional ABR recordings. Semin Hear 7:289–305.
Durrant JD. (1990) Extratympanic electrode supportvia vented earmold. Ear Hear 11:468–469.
Durrant JD, Dallos P. (1972) Influence of direct cur-rent polarization of the cochlear partition on thesummating potential. J Acoust Soc Am 52:542–552.
Durrant JD, Ferraro JA. (1991) Analog model ofhuman click-elicited SP and effects of high-pass fil-tering. Ear Hear 12:144–148.
Durrant JD, Gans D. (1977) Biasing of the summat-ing potentials. Acta Otolaryngologica 80:13–18.
Eggermont JJ. (1976) Summating potentials in elec-trocochleography: relation to hearing disorders. In:Ruben RJ, Elberling C, Salomon G, eds.Electrocochleography. Baltimore:University ParkPress, 67–87.
Engebretson AM, Eldridge DH. (1968) Model for thenonlinear characteristics of cochlear potentials. JAcoust Soc Am 44:548–554.
Ferraro JA. (1992) Electrocochleography: how - partI. Audiol Today 4(6):26–28.
Ferraro JA. (1997) Laboratory Exercises in AuditoryEvoked Potentials. San Diego: Singular PublishingGroup.
Ferraro JA. (2000) Electrocochleography. In: RoesserRJ, Valente M, Hosford-Dunn H, eds. Audiology:Diagnosis. New York: Thieme, 425–450.
Ferraro JA, Arenberg IK, Hassanein RS. (1985)Electrocochleography and symptoms of inner ear dys-function. Arch Otolaryngol 111:71–74.
Ferraro JA, Best LG, Arenberg IK. (1983) The use ofelectrocochleography in the diagnosis, assessmentand monitoring of endolymphatic hydrops. OtolaryngolClin N Am 16:69–82.
Ferraro JA, Blackwell W, Mediavilla SJ, Thedinger B.(1994) Normal summating potential to toneburstsrecorded from the tympanic membrane in humans.J Am Acad Audiol 5:17–23.
Ferraro JA, Durrant JD. (2002) Electrocochleography.In: Katz J, ed. Handbook of Clinical Audiology. NewYork: Lippincott, Williams and Williams, 249–273.
Ferraro JA, Ferguson R. (1989) Tympanic ECochGand conventional ABR: a combined approach for theidentification of wave I and the I-V interwave inter-val. Ear Hear 3:161–166.
Ferraro JA, Krishnan G. (1997) Cochlear potentialsin clinical audiology. Audiol Neurootol 2:241–256.
Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
66

Electrocochleography in the Evaluation of Patients/Ferraro and Durrant
67
Ferraro JA, Thedinger B, Mediavilla SJ, Blackwell W.(1994) Human summating potential to tonebursts:observations on TM versus promontory recordings inthe same patient. J Am Acad Audiol 6:217–224.
Ferraro JA, Tibbils R. (1999) SP/AP area ratio in thediagnosis of Meniere’s disease. Am J Audiol 8:21–28.
Fromm B, Bylen CO, Zotterman Y. (1935) Studies inthe mechanisms of Wever and Bray effect. ActaOtolaryngologica 22:477–483.
Gibson WPR. (1978) Essentials of Electric ResponseAudiometry. New York: Churchill and Livingstone.
Gibson WPR, Arenberg IK. (1991) The scope of intra-operative electrocochleography. In: Arenberg IK, ed.Proceedings of the Third International Symposiumand Workshops on the Surgery of the Inner Ear.Amsterdam: Kugler Publications, 295–303.
Gibson WPR, Arenberg IK, Best LG. (1988)Intraoperative electrocochleographic parameters fol-lowing nondestructive inner ear surgery utilizing avalved shunt for hydrops and Meniere’s disease. In:Nadol JG, ed. Proceedings of the Second InternationalSymposium on Meniere’s Disease.Amsterdam: Kuglerand Ghedini Publications, 170–171.
Gibson WPR, Beagley MA. (1976) Transtympanic elec-trocochleography in the investigation of retrocochleardisorders. Rev Laryngol 97(Suppl.):507–516.
Gibson WPR, Moffat DA, Ramsden RT. (1977) Clinicalelectrocochleography in the diagnosis and manage-ment of Meniere’s disorder. Audiology 16:389–401.
Goin DW, Staller SJ, Asher DL, Mischke RE. (1982)Summating potential in Meniere’s disease.Laryngoscope 92:1381–1389.
Gulick WL, Gescheider GA, Frisina RD. (1989)Hearing: Physiological Acoustics, Neural Coding, andPsychoacoustics. New York: Oxford University Press.
Harris D, Dallos P. (1979) Forward masking of audi-tory nerve fiber responses. J Neurophysiol42:1083–1107.
Horner KC, Cazals Y-S. (1988) Independent fluctua-tions of the round-window summating potential andcompound action potential following the surgicalinduction of endolymphatic hydrops in the guineapig. Audiology 27:147–155.
Kiang NS. (1965) Discharge Patterns of Single NerveFibers in the Cat’s Auditory Nerve. ResearchMonograph 35. Cambridge, MA: MIT Press.
Kitahara M, Takeda T, Yazama T. (1981)Electrocochleography in the diagnosis of Meniere’sdisease. In: Volsteen KH, ed. Meniere’s Disease,Pathogenesis, Diagnosis and Treatment. New York:Thieme-Stratton, 163–169.
Kobayashi H, Arenberg IK, Ferraro JA, Van der ArkG. (1993) Delayed endolymphatic hydrops followingacoustic tumor removal with intraoperative and post-operative Auditory Brainstem Responseimprovements. Acta Otolaryngol (Stockh)504(Suppl.):74–78.
Koyuncu M, Mason SM, Shinkwin C. (1994) Effect ofhearing loss in electrocochleographic investigation of
endolymphatic hydrops using tone-pip and click stim-uli. J Laryngol Otol 108:125–130.
Kumagami H, Nishida H, Masaaki B. (1982)Electrocochleographic study of Meniere’s disease.Arch Otol 108:284–288.
Lempert J, Meltzer PE,Wever EG, Lawrence M. (1950)The cochleogram and its clinical applications: con-cluding observations. Arch Otolaryngol 51:307–311.
Lempert J, Wever EG, Lawrence M. (1947) Thecochleogram and its clinical applications: a prelimi-nary report. Arch Otolaryngol 45:61–67.
Levine SM, Margolis RH, Fournier EM, WinzenburgSM. (1992) Tympanic electrocochleography for eval-uation of endolymphatic hydrops. Laryngoscope102:614–622.
Lilly DJ, Black FO. (1989) Electrocochleography inthe diagnosis of Meniere’s disease. In: Nadol JB, ed.Meniere’s Disease. Berkeley, CA: Kugler and Ghedini,369–373.
Margolis RH, Levine SM, Fournier MA, Hunter LL,Smith LL, Lilly DJ. (1992) Tympanic electro-cochleography: normal and abnormal patterns ofresponse. Audiology 31:18–24.
Margolis RH, Lilly DJ. (1989) Extratympanic elec-trocochleography: stimulus considerations. Asha31:183(A).
Margolis RH, Rieks D, Fournier M, Levine SM. (1995)Tympanic electrocochleography for diagnosis ofMeniere’s disease. Arch Otolaryngol Head Neck Surg121:44–55.
Meniere P. (1861) Pathologic auriculaire. Memoiresur les lesions de l’oreille interne donnant lieu a dessymptomes de congestion cerebrale applectiforme.Gaz Med Paris 16:88–89.
Moller A, Janetta P. (1983) Monitoring auditory func-tions during cranial nerve microvasculardecompression operations by direct monitoring fromthe eighth nerve. J Neurosurg 59:493–499.
Moriuchi H, Kumagami H. (1979) Changes of AP, SPand CM in experimental endolymphatic hydrops.Audiology 22:258–260.
Morrison AW, Moffat DA, O’Connor AF. (1980) Clinicalusefulness of electrocochleography in Meniere’s dis-ease: an analysis of dehydrating agents. OtolaryngolClin North Am 11:703–721.
Murphy LA, Ferraro JA, Chertoff M, McCall S, ParkD. (1997) Issues in auditory evoked potentials.Abstract.American Academy of Audiology ConventionProgram. McLean, VA: American Academy ofAudiology, 64.
Orchik DJ, Ge X, Shea JJ. (1997) Action potentiallatency shift by rarefaction and condensation clicksin Meniere’s disease. Am J Otol 14:290–294.
Orchik DJ, Shea JJ Jr, Ge X. (1993) Transtympanicelectrocochleography in Meniere’s disease using clicksand tone-bursts. Am J Otol 14:290–294.
Perlman MB, Case TJ. (1941) Electrical phenomenaof the cochlea in man. Arch Otolaryngol 34:710–718.

Picton TW, Hillyard SH, Frauz HJ, Galambos R. (1974)Human auditory evoked potentials. ElectroencephalogrClin Neurophysiol 36:191–200.
Pou AM, Hirsch BE, Durrant JD, Gold SR, KamererDB. (1996) Efficacy of tympanic electrocochleographyin the diagnosis of endolymphatic hydrops. Am J Otol17:607–611
Ruben R, Sekula J, Bordely JE. (1960) Human cochlearresponses to sound stimuli. Ann Otorhinolaryngol69:459–476.
Ruth RA. (1990) Trends in electrocochleography. JAm Acad Audiol 1:134–137.
Ruth RA. (1994). Electrocochleography. In: Katz J, ed.Handbook of Clinical Audiology. 4th ed. Baltimore:Williams and Wilkins, 339–350.
Ruth RA, Lambert PR. (1989) Comparison of tym-panic membrane to promontory electrode recordingsof electrocochleographic responses in Meniere’spatients. Otolaryngol Head Neck Surg 100:546–552.
Ruth RA, Lambert PR, Ferraro JA. (1988)Electrocochleography: methods and clinical applica-tions. Am J Otol 9:1–11.
Sass K, Densert B, Arlinger S. (1997) Recording tech-niques for transtympanic electrocochleography inclinical practice. Acta Otolaryngol (Stockh) 118:17–25.
Schmidt P, Eggermont J, Odenthal D. (1974) Studyof Meniere’s disease by electrocochleography. ActaOtolaryngologica 316(Suppl.):75–84.
Schoonhoven R, Fabius MAW, Grote JJ. (1995)Input/output curves to tonebursts and clicks inextratympanic and transtympanic electrocochleog-raphy. Ear Hear 16:619–630.
Sohmer H, Feinmesser M. (1967) Cochlear actionpotentials recorded from the external canal in man.Ann Otol Rhinol Otolaryngol 76:427–435.
Spoendlin H. (1966) Organization of the cochlearreceptor. Adv Otorhinolaryngol 13:1–227.
Staller SJ. (1986) Electrocochleography in the diag-nosis and management of Meniere’s disease. SeminHear 7:267–278.
Stapells D, Picton TW, Smith AD. (1982) Normal hear-ing thresholds for clicks. J Acoust Soc Am 72:74–79.
Storms RF, Ferraro JA, Thedinger B. (1996)Electrocochleographic effects of ear canal pressurechange in subjects with Meniere’s disease. Am J Otol17:874–882.
Stypulkowski PH, Staller SJ. (1987) Clinical evalua-tion of a new ECoG recording electrode. Ear Hear8:304–310.
Suzuki JL, Yamane H. (1982) The choice of stimulusin the auditory brainstem response test for neuro-logical and audiological examinations. Ann N Y AcadSci 388:731–736.
Tasaki I, Davis H, Eldridge DH. (1954) Explorationof cochlear potentials in guinea pig with a micro-electrode. J Acoust Soc Am 26:765–773.
von Bekesy G. (1950) DC potentials and energy bal-ance of the cochlear partition. J Acoust Soc Am22:576–582.
Wazen JJ. (1994) Intraoperative monitoring of audi-tory function: experimental observation, and newapplications. Laryngoscope 104:446–455.
Wever EG, Bray C. (1930) Action currents in the audi-tory nerve response to acoustic stimulation. Proc NatlAcad Sci 16:344–350.
Whitfield IC, Ross HF. (1965) Cochlear microphonicand summating potentials and the outputs of indi-vidual hair cell generators. J Acoust Soc Am38:126–131.
Yamasoba T, Sugasawa M, Kikuchi S,Yagi M, HaradaT. (1993) An electrocochleographic study of acute low-tone sensorineural hearing loss. Eur ArchOtorhinolaryngol 250:418–422.
Yoshie N, Ohashi T, Suzuki T. (1967) Non-surgicalrecording of auditory nerve action potentials in man.Laryngoscope 77:76–85.
Journal of the American Academy of Audiology/Volume 17, Number 1, 2006
68
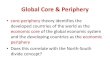



















![[ECFR] Periphery of the Periphery-Crisis and the Western-Balkans-Brief](https://img.pdfslide.us/doc/110x75/577cdcad1a28ab9e78ab1b9d/ecfr-periphery-of-the-periphery-crisis-and-the-western-balkans-brief.jpg)