Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Electrocardiographic Screening for HypertrophicCardiomyopathy and Long QT Syndrome: The Driversof Cost-Effectiveness for the Prevention of Sudden Cardiac Death
Brett R. Anderson • Sean McElligott •
Daniel Polsky • Victoria L. Vetter
Received: 6 May 2013 / Accepted: 14 August 2013 / Published online: 5 September 2013
� Springer Science+Business Media New York 2013
Abstract It is universally recognized that the prevention of
sudden cardiac death (SCD) in youth is an important public
health initiative. The best approach remains uncertain. Many
European and Asian countries support the use of electro-
cardiograms (ECGs). In the United States, this is highly
controversial. Many debate its cost-effectiveness. We
designed a comprehensive economic model of two of the
most prevalent causes of SCD identifiable by ECG, hyper-
trophic cardiomyopathy (HCM) and long QT syndrome
(LQTS), to determine the drivers of uncertainty in the esti-
mate of cost-effectiveness. We compared the cost-effec-
tiveness of screening with history and physical examination
(H&P) plus ECG to the current United States standard, H&P
alone, for the detection and treatment of HCM and LQTS.
We used a Markov model on a theoretical cohort of healthy
12-year-olds over a 70-year time horizon from a societal
perspective, employing extensive univariable and probabi-
listic sensitivity analyses, to determine drivers of costs and
effectiveness. The incremental cost-effectiveness of adding
ECGs to H&Ps was $41,400/life-year saved. The model was
highly sensitive to the effect of identification and treatment
of previously undiagnosed individuals with HCM; however,
it was insensitive to many variables commonly assumed to
be significant, including the costs of ECGs, echocardio-
grams, and genetic testing, as well as the sensitivity and
specificity of ECGs. No LQTS-related parameters were
significant. This study suggests that the key to determining
the cost-effectiveness of ECG screening in the United States
lies in developing a better understanding of disease pro-
gression in the previously undiagnosed HCM population.
Keywords Cost-effectiveness � ECG screening �Sudden death � Hypertrophic cardiomyopathy � Long
QT syndrome
Introduction
It is estimated that[1,000 children and adolescents die each
year in the United States from sudden cardiac arrest [21, 28].
The prevention of these deaths is universally recognized as
an important public health goal, yet the best screening
method remains controversial [4, 29]. Many European and
Asian countries and organizations recommend screening
Electronic supplementary material The online version of thisarticle (doi:10.1007/s00246-013-0779-0) contains supplementarymaterial, which is available to authorized users.
B. R. Anderson
The Children’s Hospital of Philadelphia, Philadelphia, PA, USA
B. R. Anderson (&)
Division of Pediatric Cardiology, NewYork-Presbyterian/
Morgan Stanley Children’s Hospital, 3959 Broadway,
CH-2N, New York, NY 10032-3784, USA
e-mail: [email protected]
B. R. Anderson
Columbia Presbyterian Medical Center, New York, NY, USA
S. McElligott
Department of Healthcare Management and Economics, The
Wharton School, University of Pennsylvania,
Philadelphia, PA, USA
D. Polsky
Division of General Internal Medicine, Perelman
School of Medicine, University of Pennsylvania,
Philadelphia, PA, USA
V. L. Vetter
Division of Pediatric Cardiology, The Children’s
Hospital of Philadelphia, Perelman School of Medicine,
University of Pennsylvania, Philadelphia, PA, USA
123
Pediatr Cardiol (2014) 35:323–331
DOI 10.1007/s00246-013-0779-0

electrocardiograms (ECGs) given (1) that many deaths occur
in asymptomatic children with undiagnosed conditions and
(2) that conditions, such as hypertrophic cardiomyopathy
(HCM) and long QT syndrome (LQTS), can be identified on
ECG even in asymptomatic children with negative family
histories [5, 18, 28]. Proponents of ECG screening further
emphasize the fact that inexpensive treatments, including
lifestyle modification, are commonly thought to decrease
mortality [6]. In the United States, in contrast, many have
raised concerns regarding the logistics, feasibility, and costs
of ECG screening and have suggested that low disease
prevalence, imperfect ECG sensitivity or specificity, and
costs of ECGs/follow-up diagnostics or treatments might
limit the cost-effectiveness of this strategy [15, 27, 37]. The
American Heart Association’s scientific statement on pre-
participation cardiovascular screening currently recom-
mends screening only for children involved in competitive
sports with history and physical examination (H&P), without
inclusion of ECG, because these children are presumed to be
at highest risk of sudden unexpected death [4, 27, 29].
Comprehensive economic analyses of ECG screening in
the United States are limited. Most either artificially decrease
estimates of costs by ignoring lifetime costs of treatment or
decrease estimates of life-years saved (LYS) by restricting
the number of years for which the models are run (for
example, to only years while playing sports). Other analyses
assume that all individuals will come to diagnosis before
adulthood, even without screening, or they overestimate
effectiveness and underestimate costs by focusing on limited
populations or by including the costs of H&P in calculations
of ECG costs [8, 10, 15, 20, 30, 33, 34, 38, 40, 41].
We sought to determine the key drivers of uncertainty in
an estimate of the comparative cost-effectiveness of
screening with ECG plus H&P, compared with H&P alone,
to identify potential barriers to the cost-effectiveness of
ECG screening.
Methods
Model Overview
We used a state transition Markov model to compare the
costs and benefits of two types of screening programs for a
hypothetical cohort of healthy children in the United States.
Unlike some previous studies, we included all children in the
model, not just athletes, because both ethical and practical
concerns have been raised regarding the implementation of
targeted ECG screening in the United States; given the dif-
ficulty in defining ‘‘athlete’’ and ‘‘activity level’’ in most
children, we did not want to overestimate the cost-effec-
tiveness of applying ECG screening to the general popula-
tion by limiting our study population. We focused on the
detection and treatment of two of the most common causes of
SCD that can be identified by ECG: HCM and LQTS [28].
We excluded conditions such as anomalous coronary arter-
ies, because they typically are not identifiable in asymp-
tomatic children in this age group either by H&P or ECG and
therefore do not impact incremental cost-effectiveness.
Wolff–Parkinson–White (WPW) syndrome was also exclu-
ded because it was assumed that the lower incidence of SCD
in this population and the high effectiveness of catheter
ablation would result in either a negligible or beneficial
effect on overall cost-effectiveness of an ECG screening
program and would be of limited utility in determining the
drivers of cost-effectiveness.
The two screening arms in our economic model were: (1)
H&P, screening with history and physical examination alone,
and (2) ECG/H&P, screening with ECG in addition to history
and physical examination. All children were assumed to enter
the model at 12 years of age (range 8–25 years). All children
entering the model were characterized as having HCM, hav-
ing LQTS, or having no underlying condition, based on esti-
mates of prevalence in the general United States population
(i.e., 1:500 for HCM [range 1:1,000–1:250]; 1:2,500 for
LQTS [range 1:5,000–1:1,250]). Wide ranges were used to
account for controversy in the literature regarding a variety of
factors for both diseases that influence estimates of prevalence
(e.g. definitions of athlete’s heart versus HCM and selection of
QTc cut-offs used in defining LQTS). Children were further
subdivided into true and false positives or true and
false negatives based on estimates of screening sensitivity and
specificity derived from the United States literature; wide
ranges were used to account for the variable sensitivity and
specificity of current ECG standards, recommended ‘‘mod-
ern’’ standards, and other future standards. True negatives
(i.e., healthy children) transitioned to death according to the
2007 United States Life Table [2]. False negatives initially
received no treatment, and diseases progressed according to
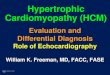
estimates of their natural histories (Fig. 1). Follow-up diag-
nostics, disease progressions, and treatments in true and
false positives were modeled separately and in detail for both
HCM and LQTS to represent the natural history of affected or
healthy children. Costs of follow-up evaluation and testing
were included in the model.
The model was run for 70 one-year cycles until each
theoretical subject either died or reached the age of
82 years. During each cycle, affected individuals transi-
tioned between health states based on estimates of proba-
bilities derived from the literature as shown in Figs. 2 and
3. The primary benefit was LYS. Screening, follow-up
diagnostic, and direct treatment costs were assigned to each
state and used to calculate total costs for each strategy. An
incremental cost-effectiveness ratio (ICER) was calculated
by dividing the difference in cumulative costs in the ECG/
H&P and H&P arms by the difference in LYS.
324 Pediatr Cardiol (2014) 35:323–331
123

Disease Progression and Treatment for HCM
True and false positives for HCM in both screening arms
were referred to cardiologists for ECGs, if not previously
obtained, and/or echocardiograms (ECHOs). After
accumulating costs of follow-up, false positives transi-
tioned to the true negative state. Initial health states for
individuals with HCM were ‘‘undiagnosed’’ (false nega-
tive), ‘‘diagnosed lower risk,’’ or ‘‘diagnosed higher risk.’’
Given that the exact criteria for risk stratification for
patients with HCM remain controversial, especially in
children, wide ranges were used around the probabilities of
being lower or higher risk. In defining point estimates,
preference was given to the probabilities cited in the 2003
ACC/ESC Expert Consensus Document on HCM and in
the ACCF/AHA Guideline for the Diagnosis and Treatment
of Hypertrophic Cardiomyopathy, which generally defined
lower risk patients as those individuals with no or mild
symptoms. The annual incidence of diagnosis and rates of
transitions between health states were also derived from the
literature [1, 9, 11, 22, 26].
All individuals with HCM were assumed to be risk-
stratified. Although the guidelines are not universally
adhered to in clinical practice, for the purposes of our
model, we assumed that management of all patients with
HCM followed the published guidelines, using established
criteria [1, 9, 11, 26]. All higher risk patients (defined
based on estimates of prevalence cited in these same
Fig. 1 Abbreviated decision tree, showing sample of model branching
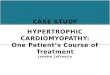
Fig. 2 Bubble diagram for HCM. Circles represent disease-specific
health states. Straight arrows represent possible transitions. Curved
arrows represent possible continuation in the same health state. HCM
hypertrophic cardiomyophathy
Pediatr Cardiol (2014) 35:323–331 325
123

guidelines) were assumed to receive implantable cardio-
verter defibrillators (ICDs). Transition to the death state for
HCM could occur through all-cause mortality or HCM-
specific mortality. Early HCM studies estimated annual
mortality of 3–6 %/year, before the widespread use of
high-dose beta-blockers, calcium-channel blockers, or
ICDs, and often in centers with higher risk profiles [9, 11].
In community-based studies, more recent estimates of
mortality are 1 %/year for adults [26, 35, 36], 2 %/year for
children [23, 31], and B1 %/year for higher risk children
and adults after ICD placement without heart failure or
atrial fibrillation [24, 26]. In this model, we assumed that
community-based studies reflected outcomes for lower risk
patients. We assumed that the lowest mortality would occur
after age 55 years (0.5 %/year [range 0.25–1 %]) [16, 25,
35] and highest mortality between ages 16 and 55 years
(2 %/year [range 1–4 %]) [26, 35, 36]. Mortality before
puberty was assumed to be 1 %/year (range 0.5–2 %) [23,
31]. Because our model began at 12 years of age, we did
not include the observed higher mortality in children
\1 year of age [31]. Mortality in diagnosed higher risk
individuals depended on treatment strategies and comor-
bidities. Compared with those diagnosed as lower risk of
the same age, undiagnosed individuals with HCM were
assumed to have, on average, a relative risk of dying of
0.67 (range 0.33–1). The Supplemental Table reports all
transition probabilities and sources.
Disease Progression and Treatment for Long QT
Syndrome
True and false positives for LQTS in both screening arms
were referred to cardiologists for risk stratification, Holter
monitors, exercise stress tests, and ECGs if not previously
obtained. Because prolonged QTc on ECG is a major cri-
terion for LQTS diagnosis, it was assumed that false pos-
itives for LQTS, as diagnosed by ECG, would remain
presumptively diagnosed in the lower risk arm for life, thus
accumulating costs without receiving benefits. Similar to
HCM, the initial states for individuals with LQTS were
‘‘undiagnosed,’’ ‘‘diagnosed lower risk,’’ or ‘‘diagnosed
higher risk’’ [32]. As with HCM, the incidence of diagnosis
and rates of transitions between health states were derived
from literature estimates, with wide ranges to account for,
among other factors, differential cut-off values for QTc
used in the definition of LQTS in the literature. Follow-up
testing and treatments were assumed to correspond with
current United States standards [1, 12, 13, 17, 32].
Because most patients with LQTS in the United
States are given beta-blockers and/or mexiletine, for the
base case model, it was assumed that all identified true or
false positives for LQTS would incur costs of one of these
medications. Higher risk individuals could receive an ICD
or undergo left cervical sympathetic denervation, with or
without continued beta-blocker treatment. Given that
guidelines are less prescriptive for higher risk patients with
LQTS than for those with HCM, it was assumed that not all
patients would receive the same treatments; relative pro-
portions receiving each therapy were based on published
estimates in the literature.
Mortality estimates for LQTS in this model were
extrapolated from published reports; mortality was set at
0.1 %/year for lower risk individuals (0.05–0.2 %), at 1 %/
year for treated higher risk individuals (0.12–2.0 %), and
at 1.3 %/year (0.7–5.0 %) for undiagnosed/untreated indi-
viduals [12, 13, 17]. Figure 3 models health-state transi-
tions for individuals with LQTS. The Supplemental Table
reports all transition probabilities and sources.
Clinical Assumptions
As detailed previously, disease-transition probabilities
were collected from the literature or based on expert
opinion if no published estimates existed. The validity of
all inputs was tested in extensive univariable and proba-
bilistic sensitivity analyses over broad ranges, to account
for differences in published data, clinical practice vari-
ability, or differences that might arise when applying
screening to diverse United States populations with dif-
fering ethnic, racial, sex, or age compositions. In deter-
mining point estimates for all LQTS-related parameters,
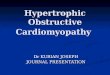
Fig. 3 Bubble diagram for LQTS. Circles represent disease-specific
health states. Straight arrows represent possible transitions. Curved
arrows represent possible continuation in the same health state. ICD
implantable cardioverter defibrillator, LCSD left cervical sympathetic
denervation, LQTS long QT syndrome
326 Pediatr Cardiol (2014) 35:323–331
123

studies were used that generally defined LQTS as C460 ms
(Supplemental Table) [1, 12, 13, 17, 32].
Because individuals with undiagnosed HCM and LQTS
are unobserved, there are few to no data on disease pro-
gression before diagnosis. Some cost analyses have
focused only on athletes and/or used historic data from
Italy to calculate expected decreases in mortality with
screening and treatment [40]. Our model uses the follow-
ing, more conservative, assumptions:
1. Given that our model was applied to the general
United States population with screening at 12 years of
age, not just to competitive athletes, estimates of risk
reduction are lower than those reported in the Italian or
sports-related literatures.
2. Individuals with symptoms are more likely to be
diagnosed. Undiagnosed individuals are more likely
than diagnosed individuals to be lower risk.
3. For LQTS, ECGs identify more asymptomatic (and
lower risk) patients than H&P alone. Therefore, a
greater proportion of the patients identified as having
LQTS by ECG/H&P compared with H&P alone are
lower risk at diagnosis.
4. In patients with HCM, symptoms are relatively rare at
12 years of age. Therefore, we assume that the
overwhelming majority of HCM patients identified
by either screening method are lower risk (95 % [range
80–100 %]).
5. Lower risk individuals, for each disease, regardless of
diagnosis method, could progress to higher risk at the
same rate. Lower risk individuals, for each disease,
regardless of diagnosis method, respond similarly to
treatment.
6. Higher risk individuals, for each disease, regardless of
diagnosis method, also respond to treatment similarly.
Costs
The 2009 and 2010 Medicare Fee Schedules were used
to determine inpatient, outpatient technical, outpatient
procedural, physician, durable medical equipment, lab-
oratory, and diagnostic costs [3]; however, costs for
genetic testing, which have decreased due to rapid
recent changes in charges and availability, were esti-
mated from the recent reimbursement experience at The
Children’s Hospital of New York and The Children’s
Hospital of Philadelphia. Drug costs were estimated
using 2010 Costco prices [7]. The cost of initial H&P
was assumed to be equivalent in the two arms and
therefore was not included in the analysis. All costs and
LYS were discounted at 3 % (range 1–5 %). See Sup-
plemental Table.
Analysis
Analyses were performed from a societal perspective. The
incremental cost-effectiveness thresholds for ECG screening
were based on commonly accepted thresholds for willing-
ness to pay in the United States and set at B $50,000/LYS to
be highly cost-effective and B $100,000/LYS to be cost-
effective.
Uncertainty
To model the potential impact of uncertainty, we per-
formed both univariable and probabilistic (multivariable)
sensitivity analyses on all input variables. These analyses
allowed us to determine which inputs most influenced the
ICER and to test robustness of the model. We assumed a
beta distribution for all disease progression-, diagnostic-,
and treatment-related probabilities, with ranges based on
95 % confidence intervals from their estimates in the lit-
erature. Model inputs based on expert opinion were tested
over large but feasible ranges. Assumptions around age
were assumed to follow normal distributions. Uncertainty
around costs was modeled by setting tested ranges from 50
to 200 % of the base case estimates. Costs were assumed to
be gamma-distributed, with means set equal to the SD,
because of the long tails typically associated with health
care costs.
For univariable sensitivity analyses, the model was run
using low and high estimates for each variable, while
holding all other inputs at their base values. This allowed
us to estimate a range of ICERs for each variable and to
determine how much these ICERs deviated from the base
ICER estimate. Probabilistic sensitivity analyses were
performed using Monte Carlo simulation, whereby esti-
mated values for each variable were drawn from their
distributions and used to calculate ICER estimates. This
process was repeated 10,000 times to allow for model
uncertainty and to estimate confidence intervals.
All models around uncertainty were performed using
TreeAge Software (TreeAge, Williamstown, MA, USA)
with statistical analyses performed in STATA 11MP
(StataCorp LP, College Station, TX, USA) or EXCEL
(Microsoft, Richmond, WA, USA).
Results
The estimated ICER of ECG/H&P screening compared
with H&P alone for our base case model is $41,400/LYS at
an incremental cost of $140/child screened with an incre-
mental increase of 3.4 LYS/1,000 children screened
(Table 1). Compared with H&P alone, ECG/H&P averted
Pediatr Cardiol (2014) 35:323–331 327
123

360 deaths before age 21 and 760 deaths before age 40, at
an average lifetime cost of $0.8 M/death averted [39].
Cost-effectiveness analyses can be misleading if only the
base-case ICER is considered. The power of such analyses
lies in understanding sources of uncertainty. One-way sen-
sitivity analyses indicate that our model is largely insensitive
to variance in most input variables for both conditions,
including ECG false positive and negative rates, as well as
the costs of ECGs, echocardiograms, and other follow-up
testing. It is also insensitive to all LQTS disease and treat-
ment variables in this model, such as the prevalence of
LQTS (including the effects of variable QTc cut-offs used in
diagnosing LQTS), false positive and false negative rates
associated with screening, and rates of disease progression.
Conversely, it is highly sensitive to assumptions around the
effects of identifying and treating previously undiagnosed
youths with HCM (lower and higher risk) compared with
those diagnosed with lower risk HCM. Holding all other
variables constant and using the assumption that identifying
and treating previously undiagnosed HCM patients is simi-
lar to that in the currently diagnosed HCM population, the
estimated ICER for ECG/H&P screening versus H&P alone
is highly favorable at $16,500/LYS. However, using the
assumption that identification and treatment in this popula-
tion provides little benefit, the ICER becomes highly unfa-
vorable at $182,100/LYS. This one input accounts for
77.5 % of ICER variability. When all other inputs
parameters are allowed to vary across 95 % CIs, no other
variables caused ICER estimates to rise above the $100,000/
LYS threshold, such as the many variables commonly
assumed to be barriers to cost-effectiveness, including false
positive and negative rates for ECGs, the discount rate,
and the prevalence of HCM and LTQS in the general pop-
ulation. These variables each have B5.1 % effect on vari-
ability of the ICER (Fig. 4).
Probabilistic sensitivity analyses also demonstrate that
the incremental cost-effectiveness of ECG/H&P screening
compared with H&P alone is uncertain regarding just one
variable: the effect of identifying and treating previously
undiagnosed youths with HCM. As the result of the effect
of this one input on ICER variance, ECG/H&P remains
incrementally cost-effective 78 % of the time (Figs. 5, 6).
Discussion
We compared the United States cost-effectiveness of H&P/
ECG versus ECG alone by way of a theoretical economic
model of diagnosis, treatment, and disease progression for
HCM and LQTS, two of the most common causes of SCD
identifiable on ECG. We found an ICER of $41,400/LYS,
at an incremental cost of $140/child screened, with an
incremental increase of 3.4 LYS/1,000 children screened.
Although previous studies have offered similar point
Table 1 Estimated incremental cost-effectiveness of ECG/H&P screening compared with H&P alone
Screening Cost/child Incremental
costs/child
Effectiveness
(LYS/child)
Incremental effectiveness
(LYS/child)
ICER ($/LYS)
H&P $45.92 28.491
ECG/H&P $185.62 $139.70 28.494 0.0034 $41,400
ICER incremental cost-effectiveness ratio, LYS life-year saved
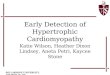
Fig. 4 Tornado graph, showing
results of univariable sensitivity
analyses for the 10 parameters
with the largest effects on cost
per LYS, comparing ECG/H&P
with H&P. Cumulative and
incremental percents of the total
variability in the incremental
cost-effectiveness ratio, as
explained by each parameter,
are denoted in the column on
the right. HCM hypertrophic
cardiomyopathy, H&P
screening arm with only history
and physical examination, ICER
incremental cost effectiveness
ratio, LYS life-year saved
328 Pediatr Cardiol (2014) 35:323–331
123

estimates for the incremental cost-effectiveness ratio, our
study focused on the variables that drive cost-effectiveness
or could act as barriers.
We performed extensive sensitivity analyses and deter-
mined that many factors previously assumed to be barriers to
cost-effectiveness do not appear to be actual obstacles. Many
have speculated that ECG screening in the United States
might or might not be cost-effective because of low preva-
lence of disease, high false positive rates associated with
screening (as the result of antiquated normal values), or costs
of ECGs, follow-up testing, or treatments. Sensitivity anal-
yses of the ICER to these inputs showed that only changes in
the prevalence of HCM, discount rate, and ECG false posi-
tive rate for HCM had just a mild (3.4, 4.4, and 5.1 %,
respectively) effect on the ICER. None moved the ICER
across the putative $100,000 threshold for cost-effective-
ness. The only variable that significantly impacted the cost-
effectiveness of ECG screening was related to the assumed
progression of disease in the undiagnosed HCM population.
An ICER point estimate is dependent on a number of
clinical assumptions, and these assumptions can make base
case estimates vary widely [8, 10, 15, 20, 33, 34, 38, 40,
41]. It is important, therefore, to focus on the results of the
sensitivity analyses rather than on point estimates alone.
Our model shows that a better understanding of disease
characteristics in the undiagnosed HCM population must
be determined to allow accurate assessment of the impact
of ECG screening in the United States.
Model Limitations
This model does not incorporate the psychosocial impact of
false positive screens or the false sense of security derived
from one-time negative screens by using quality-adjusted
life-years, because no verified data exist [14]. Although
improving ECG standards would lessen the effect, a sig-
nificant burden would fall on health care professionals to
counsel children and families, and the extent of that burden
is not captured here. Nevertheless, sensitivity analyses
suggest that even a modest effect on quality of life would
have a minimal effect on incremental cost-effectiveness.
Second, whereas maintenance costs are included in the
model, startup costs associated with the initiation of a
national screening program are not included. In theory,
one-time startup costs for a program that runs in perpetuity
represent only a fraction of the lifetime costs of such a
program. In the short-run, these costs, or other logistical
hurdles, might pose significant but not necessarily insur-
mountable barriers.
The greatest limitation of the model in this study, as is
true with any Markov simulation, is its basis on a theo-
retical cohort of patients and a number of assumptions. To
address this, we validated the sensitivity of our model to all
assumptions over wide ranges. This allowed us to account
for differences in published estimates of probabilities,
clinical practice variability, and differences that might arise
when applying screening to varied United States popula-
tions with variable ethnic, racial, sex, or age compositions.
We made assumptions to account for the predictable dif-
ferences between diagnosed and undiagnosed populations.
It is unknown whether disease progression in undiagnosed
individuals mirrors that in those currently diagnosed. It is
possible that ECG screening might identify a greater pro-
portion of exceptionally lower risk individuals, who might
never have presented but who would now be followed-up
for life, thus accumulating costs without accruing benefits.
In contrast, early implementation of low-cost (e.g. lifestyle
modification or beta-blockers and surveillance) or more
Fig. 5 Probabilistic sensitivity graph, showing the impact of uncer-
tainty in parameter inputs on the incremental costs and effectiveness
of ECG/H&P versus H&P screening as the result of 10,000 simulation
trials. Diagonal lines represent willingness to pay thresholds, and dots
to the right of these lines represent trials with lower ICERs
Fig. 6 Acceptability curve, showing the likelihood that ECG/H&P is
cost-effective, relative to H&P alone, for different willingness-to-pay
thresholds. P is the probability the ICER falls below the given
willingness-to-pay thresholds
Pediatr Cardiol (2014) 35:323–331 329
123

costly but highly effective (e.g. placement of ICDs) inter-
ventions in identified higher risk individuals might dra-
matically impact disease progression, thus improving
benefits and decreasing total costs.
In addition, this analysis only models two common
causes of SCD in youth. For other diseases, such as WPW
syndrome, it was assumed that the lower incidence of SCD
in this population and the high effectiveness of catheter
ablation would result in negligible or beneficial effect on
the ICER because the model would be dominated by the
effects of HCM and, to a lesser extent, LQTS. This is not to
say that the addition of WPW screening would not be cost-
effective. Rather, it is to say that the addition of WPW
screening would not significantly drive overall estimates of
the ICER.
Finally, our model does not capture the potential bene-
fits associated with the identification of family members
due to the genetic transmission of these conditions; this
approach was selected for modeling simplicity, but it
potentially underestimates LYS. Once a proband is iden-
tified, certainly it becomes more cost-effective to screen
family members because there is a higher probability of
identifying true positives. Therefore, screening family
members could decrease the ICER associated with a
screening program, thus making screening more cost-
effective; however, family screening is unlikely to alter the
drivers of cost-effectiveness.
Conclusion
In summary, ECG screening remains highly controversial
in the United States with limited data regarding potential
barriers to cost-effectiveness. We have shown that the
addition of ECG screening to history and physical exami-
nation could be cost-effective for the prevention of SCD in
youths in the United States and that many of the concerns
previously raised are not in fact valid barriers to cost-
effectiveness. We have shown that significant uncertainty
remains in the cost per potential LYS and that the key to
this uncertainty lies in developing a better understanding of
the disease profile and the impact of identification and
treatment in the currently undiagnosed HCM population.
Until this understanding is developed, one cannot defini-
tively conclude whether or not ECG screening in the
United States is cost-effective.
Therefore, we recommend that those considering ECG
screening make the objectives and scope of screening clear
to the participants and provide appropriate follow-up for
any presumed abnormal findings. Furthermore, it would be
beneficial for those conducting ECG screenings to pro-
spectively collect data on outcomes to allow for knowledge
improvement in this area so that future decisions on ECG
screening can be evidence-based. Similarly, those involved
in cardiac screening without ECGs also should collect
outcome data because a randomized clinical trial of H&P
plus ECG screening versus screening with H&P alone
appears to be prohibitive with regard to the numbers
required, time interval for follow-up, and overall costs, as
indicated by the National Institutes of Health Working
Group [19].
Conflict of interest None.
References
1. Ackerman MJ, Priori SG, Willems S, Berul C, Brugada R, Cal-
kins H et al (2011) HRS/EHRA expert consensus statement on
the state of genetic testing for the channelopathies and cardio-
myopathies. This document was developed as a partnership
between the Heart Rhythm Society (HRS) and the European
Heart Rhythm Association (EHRA). Heart Rhythm 8:1308–1339
2. Arias E (2011) United States life tables, 2007. Natl Vital Stat Rep
59:1–60
3. Centers for Medicare and Medicaid Services (2010) Available at:
http://www.cms.gov/Medicare/Medicare.html. Accessed 15 June
2010
4. Chaitman BR (2007) An electrocardiogram should not be inclu-
ded in routine preparticipation screening of young athletes. Cir-
culation 116:2610–2615
5. Corrado D, Pelliccia A, Bjornstad HH, Vanhees L, Biffi A,
Borjesson M et al (2005) Cardiovascular pre-participation
screening of young competitive athletes for prevention of sudden
death: proposal for a common European protocol. Consensus
statement of the Study Group of Sport Cardiology of the Working
Group of Cardiac Rehabilitation and Exercise Physiology and the
Working Group of Myocardial and Pericardial Diseases of the
European Society of Cardiology. Eur Heart J 26:516–524
6. Corrado D, Basso C, Pavei A, Michieli P, Schiavon M, Thiene G
(2006) Trends in sudden cardiovascular death in young compet-
itive athletes after implementation of a preparticipation screening
program. JAMA 296:1593–1601
7. Costco (2010) Pharmacy drug information. Available at: http://
wwwcostcocom/Pharmacy/DrugInformationaspx?p=1. Accessed
15 June 2010
8. Denchev P, Kaltman JR, Schoenbaum M, Vitiello B (2010)
Modeled economic evaluation of alternative strategies to reduce
sudden cardiac death among children treated for attention deficit/
hyperactivity disorder. Circulation 121:1329–1337
9. Elliott P, Poloniecki J, Dickie S, Sharma S, Monserrat L, Varnava
AM et al (2000) Sudden death in hypertrophic cardiomyopathy
identification of high risk patients. J Am Coll Cardiol 36:
2212–2218
10. Fuller C (2000) Cost effectiveness analysis of screening of high
school athletes for risk of sudden cardiac death. Med Sci Sports
Exerc 32:887–890
11. Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link
MS et al (2011) 2011 ACCF/AHA guideline for the diagnosis and
treatment of hypertrophic cardiomyopathy. A Report of the
American College of Cardiology Foundation/American Heart
Association Task Force on Practice Guidelines Developed in
Collaboration With the American Association for Thoracic Sur-
gery, American Society of Echocardiography, American Society
330 Pediatr Cardiol (2014) 35:323–331
123
of Nuclear Cardiology, Heart Failure Society of America, Heart
Rhythm Society, Society for Cardiovascular Angiography and
Interventions, and Society of Thoracic Surgeons. J Am Coll
Cardiol 58:e212–e260
12. Goldenberg I, Moss AJ, Peterson DR, McNitt S, Zareba W,
Andrews ML et al (2008) Risk factors for aborted cardiac arrest
and sudden cardiac death in children with the congenital long-QT
syndrome. Circulation 117:2184–2191
13. Goldenberg I, Zareba W, Moss AJ (2008) Long QT syndrome.
Curr Probl Cardiol 33:629–694
14. Griebsch I (2005) Quality-adjusted life-years lack quality in
pediatric care: a critical review of published cost-utility studies in
child health. Pediatrics 115:e600–e614
15. Halkin A, Steinvil A, Rosso R, Adler A, Rozovski U, Viskin S
(2012) Preventing sudden death of athletes with electrocardio-
graphic screening: what is the absolute benefit and how much will
it cost? J Am Coll Cardiol 60:2271–2276
16. Harris KM (2006) Prevalence, clinical profile, and significance of
left ventricular remodeling in the end-stage phase of hypertrophic
cardiomyopathy. Circulation 114:216–225
17. Hobbs JB, Peterson DR, Moss AJ, McNitt S, Zareba W, Gold-
enberg I et al (2006) Risk of aborted cardiac arrest or sudden
cardiac death during adolescence in the long-QT syndrome.
JAMA 296:1249–1254
18. International Olympic Committee Medical Commission (2004)
Sudden cardiovascular death in sports. Lousanne recommenda-
tions. Available at: http://www.olympic.org/Documents/Reports/
EN/en_report_886.pdf.
19. Kaltman JR, Thompson PD, Lantos J, Berul CI, Botkin J, Cohen
JT et al (2011) Screening for sudden cardiac death in the young:
report from a National Heart, Lung, and Blood Institute Working
Group. Circulation 123:1911–1918
20. Leslie LK, Cohen JT, Newburger JW, Alexander ME, Wong JB,
Sherwin ED et al (2012) The costs and benefits of targeted
screening for causes of sudden cardiac death in children and
adolescents. Circulation 125:2621–2629
21. Liberthson R (1996) Sudden death from cardiac causes in chil-
dren and young adults. N Engl J Med 334:1039–1044
22. Maron BJ (1999) Clinical course of hypertrophic cardiomyopathy
in a regional United States cohort. JAMA 281:650–655
23. Maron B, Roberts W, Epstein S (1982) Sudden death in hyper-
trophic cardiomyopathy a profile of 78 patients. Circulation
65:1388–1394
24. Maron B, Shen W, Link M, Epstein A, Almquist A, Daubert J
et al (2000) Efficacy of implantable cardioverter-defibrillators for
the prevention of sudden death in patients with hypertrophic
cardiomyopathy. N Engl J Med 342:365–373
25. Maron BJ, Olivotto I, Bellone P, Conte MR, Cecchi F, Flygenring
BP et al (2002) Clinical profile of stroke in 900 patients with
hypertrophic cardiomyopathy. J Am Coll Cardiol 39:301–307
26. Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn
HJ, Seidman CE et al (2003) American College of Cardiology/
European Society of Cardiology clinical expert consensus
document on hypertrophic cardiomyopathy. J Am Coll Cardiol
42:1687–1713
27. Maron BJ, Thompson PD, Ackerman MJ, Balady G, Berger S,
Cohen D et al (2007) Recommendations and considerations
related to preparticipation screening for cardiovascular abnor-
malities in competitive athletes: 2007 update: a scientific state-
ment from the American Heart Association Council on Nutrition,
Physical Activity, and Metabolism: Endorsed by the American
College of Cardiology Foundation. Circulation 115:1643–1655
28. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO (2009)
Sudden deaths in young competitive athletes: analysis of 1866 deaths
in the United States, 1980–2006. Circulation 119:1085–1092
29. Myerburg RJ, Vetter VL (2007) Electrocardiograms should be
included in preparticipation screening of athletes. Circulation
116:2616–2626
30. O’Connor DP, Knoblauch MA (2010) Electrocardiogram testing
during athletic preparticipation physical examinations. J Athl
Train 45:265–272
31. Ostman-Smith I, Wettrell G, Keeton B, Holmgren D, Ergander U,
Gould S et al (2008) Age- and gender-specific mortality rates in
childhood hypertrophic cardiomyopathy. Eur Heart J 29:1160–1167
32. Priori SG, Schwartz PJ, Napolitano C, Bloise R, Ronchetti E,
Grillo M et al (2003) Risk stratification in the long-QT syndrome.
N Engl J Med 348:1866–1874
33. Quaglini S, Ragnoni C, Spazzolini C, Priori S, Mannarino S,
Schwartz PJ (2006) Cost-effectiveness of neonatal ECG screen-
ing for the long QT syndrome. Eur Heart J 27:1824–1832
34. Schoenbaum M, Denchev P, Vitiello B, Kaltman JR (2012)
Economic evaluation of strategies to reduce sudden cardiac death
in young athletes. Pediatrics 130:e380–e389
35. Spirito P, Rapezzi C, Autore C, Bruzzi P, Bellone P, Ortolani P
et al (1994) Prognosis of asymptomatic patients with hypertro-
phic cardiomyopathy and nonsustained ventricular tachycardia.
Circulation 90:2743–2747
36. Spirito P, Seidman C, McKenna W, Maron B (1997) The management
of hypertrophic cardiomyopathy. N Engl J Med 336:775–785
37. Steinvil A, Chundadze T, Zeltser D, Rogowski O, Halkin A,
Galily Y et al (2011) Mandatory electrocardiographic screening
of athletes to reduce their risk for sudden death: proven fact or
wishful thinking? J Am Coll Cardiol 57:1291–1296
38. Tanaka Y, Yoshinaga M, Anan R, Tanaka Y, Nomura Y, Oku S
et al (2006) Usefulness and cost effectiveness of cardiovascular
screening of young adolescents. Med Sci Sports Exerc 38:2–6
39. United States Census (2010) Available at: http://www.census.
gov/population/age/. Accessed 2 Aug 2012
40. Wheeler M, Heidenreich P, Froelicher V, Hlatky M, Ashley E
(2010) Cost-effectiveness of preparticipation screening for pre-
vention of sudden cardiac death in young athletes. Ann Intern
Med 152:276–286
41. Zupancic J, Triedman J, Alexander M, Walsh E, Richardson D,
Berul C (2000) Cost-effectiveness and implications of newborn
screening for prolongation of QT interval for the prevention of
sudden infant death syndrome. J Pediatr 136:481–489
Pediatr Cardiol (2014) 35:323–331 331
123