Embed Size (px)
Citation preview

Elder Mistreatment in Long Term Care
Laura Mosqueda, M.D.
Director of Geriatrics
Professor of Family MedicineUniversity of California, Irvine School of Medicine

AbuseAbuse is the willful infliction of
injury, unreasonable confinement,
intimidation, or punishment with
resulting physical harm, pain, or
mental anguish.
…. Or the potential for harm.
Comparisons with Child Abuse
• Many have compared the current state of medical knowledge about elder mistreatment with the state of knowledge about child abuse and neglect 30 years ago

Difficulty with Detection/Diagnosis
• Medical picture of the elderly much more complex than that of a child
• Bad outcomes and death are more likely for the elderly than for children
• Abuse and neglect are rarely observed
• Difficult to link physical signs with diagnoses
Types of Abuse
• Physical
• Psychological/Emotional
• Neglect
• Abduction
• Sexual
• Financial

Types of Abuse
• Physical
• Psychological/Emotional
• Neglect
• Abduction
• Sexual
• Financial

Examples of Physical Abuse
• Pulling a patient’s hair
• Slapping/hitting/punching
• Throwing food or water on a patient
• Tightening a restraint to cause pain

Examples of Psychological Abuse
• Terrorizing and/or threatening a patient
with a word or gesture
• Inappropriate isolation of a patient
• Yelling at a patient in anger
• Denying food or privileges

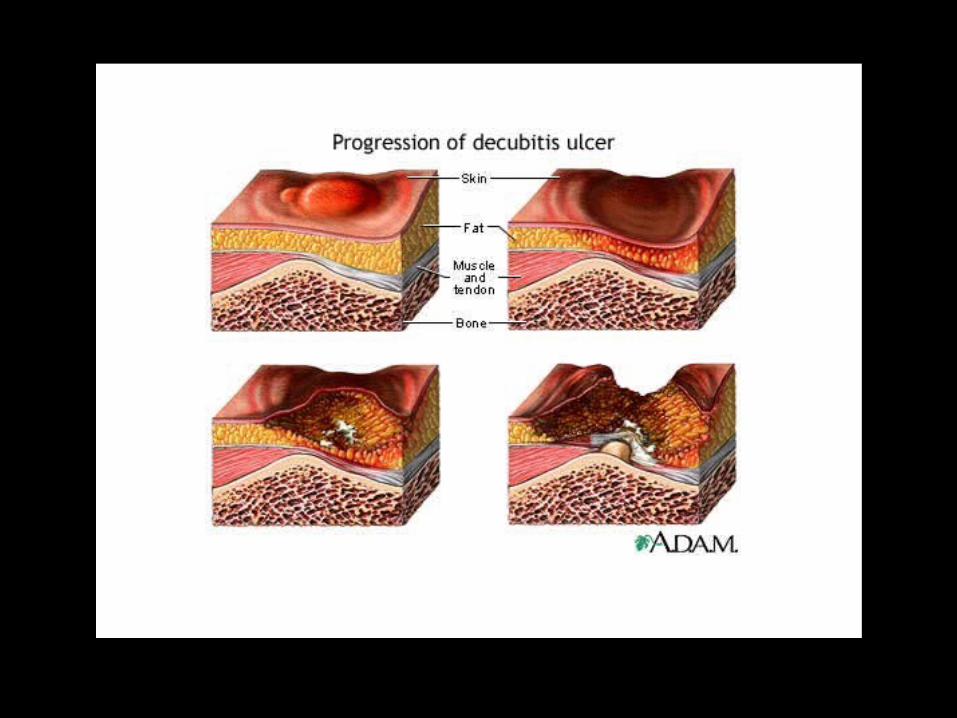
Examples of Neglect
• Person is lying in urine and feces for extended periods of time
• Person develops malnutrition and/or dehydration and/or pressure sores due to lack of appropriate care
• Person is dirty, has elongated nails, is living in filthy environment

Abuse Occurs in a Variety of Patterns
• Perpetrator works at the facility
• Perpetrator is another resident
• Good facilities
• Bad facilities

Abuse at the Person Level
• Resident to resident• Resident to staff• Family member to resident• Staff to resident
– CNAs– nurses– doctors– outside/paid help– janitors– etc.
Abuse among CNAs
• 10% committed physically abusive act(s)– excessive restraint 6%– pushing/grabbing/shoving/pinching 3%– hitting/slapping 3%
• 40% committed psychologically abusive act(s)– yelling 33%– insulting/swearing 9%– denying food/privileges as punishment 2%– threatening physical violence 2%
Pillemer 1991
Predictors of Abuse among CNAs
• High level of job stress/burnout
• Aggressive patient
• Frequent verbal conflict with patients

Great Facility/One Bad Egg
• Reasonable staffing ratio
• Good administration
• High quality care
• Sociopath gets hired
Great Facility/Unusual Circumstance
• High quality care
• Difficult resident– physically dependent– verbally abusive
• Stressed CNA– usually great with residents– trouble at home, stress at work– pushed “over the edge”

Abuse at the Facility Level
• Neglect
• Poor care
• Atmosphere of threats/reprisal

Poor Quality Facility
• Many residents receive poor care (i.e. pattern of poor care)– pressure sores: common and improperly treated
– malnutrition: common and improperly treated
• Lack of leadership/administrative support
• Employee morale is poor
• Absentee medical director

High risk caregiver
Vulnerable person
Context/Right circumstance
Recipe for Abuse

The Problem with the Problem
Complexity • Age-related changes • When does it cross the line?• Impaired Capacity• Mandated roles of multiple agencies• Lack of coordinated, comprehensive
system

Normal & Common Changes
• Integument– thinner epidermis– capillary fragility
• Renal: decrease in creatinine clearance• Sensory system
– slower reaction time– presbycussis– macular degeneration, cataracts

Normal & Common Changes
• Musculoskeletal– sarcopenia– osteopenia/osteoporosis
• Cardiovascular– orthostatic hypotension– congestive heart failure
• Function– gait/falls– ADLs
When does bad care cross the line to become neglect?
greatacceptablepoorneglect
Dementia is a disease process
which causes loss of intellectual
abilities and inability to perform
one’s usual activities.
Types of Dementia
• Alzheimer’s Disease
• Vascular Dementia
• Frontal Temporal Lobe Dementia
• Primary Progressive Aphasia
• Dementia with Lewy Bodies
Dementia and Abuse
• Provocative behaviors
• May be unable to recognize abuse
• May be unable to report abuse
• May be the perpetrator of abuse
• May not be believed
Interviewing People with Dementia
• Understand the type of dementia
• Know the pattern of cognitive loss
• When do you “take it seriously”?

Types of Memory
• Verbal
• Visual
• Emotional
Delirium
• Problems with attention
• Fluctuation in cognition
• Reversible (e.g. infections, medications,
dehydration)
• Cannot make a diagnosis of dementia if
delirium is present

Delirium and Abuse
• Delirium may be a marker of abuse– Neglect – Over-medication– Delay in seeking care
• Delirium will interfere with victim’s ability
to explain what happened

When Abuse is Suspected...
• Context
• History
• Physical Examination
• Mental Status examination
• Laboratory testing
• Cognitive/behavioral changes

Context
• Circumstances/Events leading up to the alleged abuse
• Personality and behavioral characteristics– victim
– perpetrator
• Medical history
• Cognitive capacity

Red Flags: History
• Implausible/vague explanations
• Delay in notification
• Unexplained injuries - past or present
• Inconsistent stories
• Change in behavior
Interviewing Issues
• Establish cognitive ability level
• Vision
• Hearing
• Comfort
• Best time of day

Observations
• Observe the alleged victim and the perpetrator
– Interaction
– Behavioral indicators of state of mind
• Depression
• Fear
• Confusion

Physical Exam
• Injury assessment
• Functional status
• Skin examination
• Pelvic examination

Clues on Physical Exam
• Sores, bruises, other wounds
• Unkempt appearance
• Poor hygiene
• Malnutrition
• Dehydration
Functional Assessment
• Range of motion
• Pain
• Gait and balance
• Sensory

Injury Assessment:The Challenge in Elders
• Normal changes
• Medication effects
• Common changes
• Dementia
Injury Assessment
Types of InjuriesTypes of Injuries
• Bruises• Pressure sores• Fractures• Burns
What to look forWhat to look for
• Hx consistent with exam?
• Old injuries
• Delay in seeking care
• Location

Bruising
• Age-related changes
• Medications
• Dating by color
• Multiple stages of healing
• History consistent with injury?
• Location

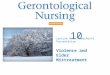
Summary of Results
Nearly 90% of the bruises were on the extremities.
No bruises on the neck, ears, genitalia, buttocks, or soles of the feet.
Subjects were more likely to know the cause of the bruise if the bruise was on the trunk.
16 bruises were predominately yellow within the first 24 hours of onset.
Those people on medications known to impact coagulation pathways and those with compromised function were more likely to have multiple bruises.

Location of Bruises
(108 bruises at Day 1)
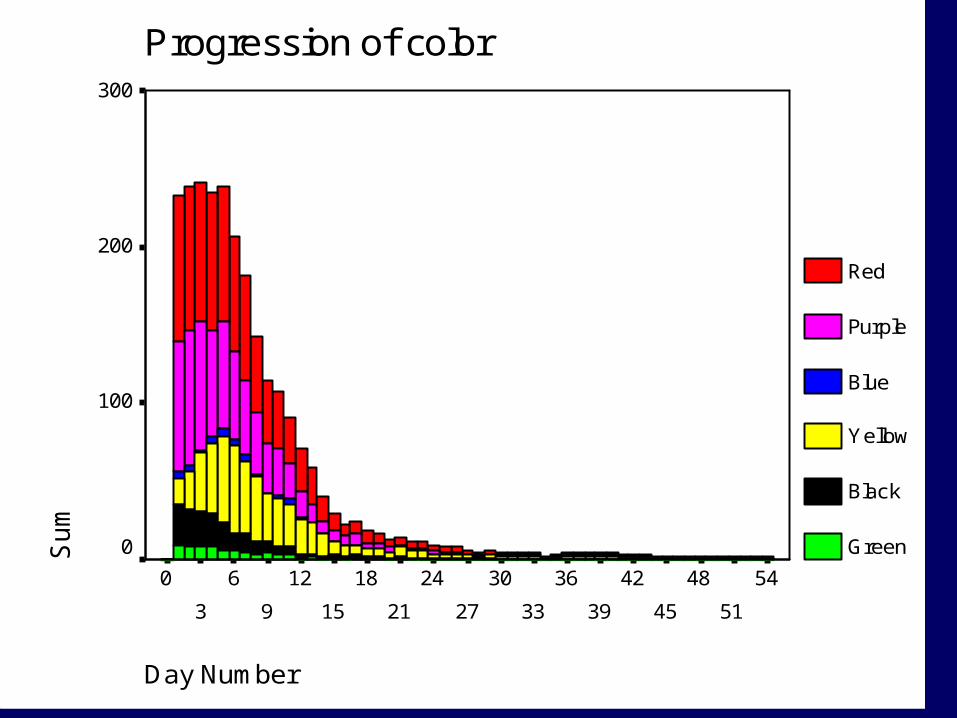
Progression of color
Day Number
54
51
48
45
42
39
36
33
30
27
24
21
18
15
12
9
6
3
0
Su
m300
200
100
0
Red
Purple
Blue
Yellow
Black
Green
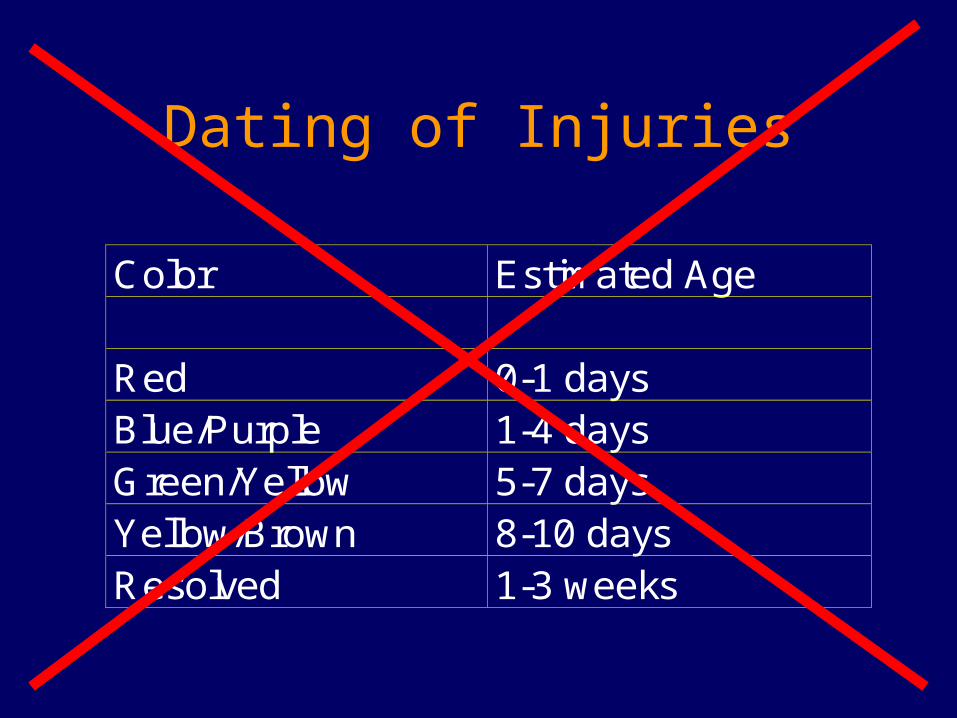
Dating of Injuries
Color Estimated Age
Red 0-1 daysBlue/Purple 1-4 daysGreen/Yellow 5-7 daysYellow/Brown 8-10 daysResolved 1-3 weeks
Laboratory Evidence
• Malnutrition
• Dehydration
• Coagulation studies
• Medication levels
• Radiographs
• Neuroimaging (MRI, CT)
Mental Status Exam
• Best to have a formal mental status exam
such as the Folstein Mini Mental State
exam (MMSE) documented
• At a minimum, get some observations and
statements about the victim’s cognitive
status
Look for…
• Residents in restraints
• Mood
• Medication errors
• Infection control
• Pressure sores
• Staffing levels
• Complaints







![Index of [tenosique.gob.mx]€¦ · norma alicia morales magaÑa jose-fa mosqueda morales maria sarabia ... rebeca balcazar perez romelia el-wan suchite etelvina mosqueda dominguez](https://img.pdfslide.us/doc/110x75/5fa30c09c8bd370bc5560080/index-of-norma-alicia-morales-magaa-jose-fa-mosqueda-morales-maria-sarabia.jpg)
















![[Dissertation 2003] Gilberto Mosqueda UC Berkeley](https://img.pdfslide.us/doc/110x75/549e2cc1ac795947768b467a/dissertation-2003-gilberto-mosqueda-uc-berkeley.jpg)

