Embed Size (px)
DESCRIPTION
Escleorosis bilateral amiotroficaterapias
Citation preview

7/18/2019 ELA Blatzheim 2009
http://slidepdf.com/reader/full/ela-blatzheim-2009 1/8
PALLIATIVE CARE REVIEW
Interdisciplinary palliative care, including massage,in treatment of amyotrophic lateral sclerosis
Kendra Blatzheim, CMT, NMT*
Meridiansd
A Center for the Healing Arts, 321 Main Street, Gaithersburg, MD 20878, USA
Received 25 May 2007; received in revised form 16 March 2008; accepted 29 April 2008
KEYWORDSAmyotrophic lateralsclerosis (ALS);Lou Gehrig;Massage;Palliative care;
Interdisciplinary;Treatment methods
Summary Amyotrophic lateral sclerosis (ALS) is a progressive fatal neurological disease that
affects approximately 20,000 Americans. Symptoms include muscle weakness, fatigue, twitch-
ing, atrophy, spasticity, pain, oropharyngeal dysfunction, pseudobulbar affect, weight loss,
and respiratory impairment. Death occurs within 3e5 yr after onset of symptoms, with diag-
nosis taking from 11 to 17.5 months. The only FDA-approved drug for ALS is Riluzole, which only
increases the life expectancy by a few months. All other treatments for ALS provide symptom
management to improve the patient’s quality of life. An interdisciplinary palliative care teamfor the ALS patient helps to reduce the stress that the illness places on families. Massage can
be a useful adjunctive treatment for spasticity and pain when medication side effects are
unwanted. A holistic interdisciplinary palliative care team supports both the patient and thefamily improving their quality of life.
ª 2008 Elsevier Ltd. All rights reserved.
Introduction
Amyotrophic lateral sclerosis (ALS), or Lou Gehrig’s disease,is idiopathic; gradual and progressive neuromotor disease
with no definitive cause. Jean-Marie Charcot named thedisease, amyotrophic lateral sclerosis, in 1874, after whathe found in patients with ALS. Amyotrophic describes theeffects on the muscular system and is from the Greeklanguage. In medical terminology ‘‘a’’ means no, ‘‘myo’’means muscle, and ‘‘trophic’’ refers to nourishment;‘‘lateral’’ refers to the spinal tract that is involved; and
‘‘sclerosis’’ means scarring. ALS affects voluntary move-ments; symptoms include muscle weakness and atrophy;muscle spasticity in limbs and bulbar muscles, causing notonly the loss of movement but also oropharyngealdysfunction; weight loss; and, in end stage, loss of respi-
ration (Chio et al., 2006; Galbussera et al., 2006; Ganziniet al., 2002; Gomes et al., 2006). In up to 50% of ALSpatients, pseudobulbar affect is found (Rochs et al., 2005).Pseudobulbar affect is uncontrolled laughing or crying andis thought to be from damage to the frontal lobe of thebrain (Rochs et al., 2005). Neurons that control the eyesand bladder are killed in the later stages of the disease(Bruijn and Cudkowicz, 2006).
Approximately 20,000 Americans have ALS withapproximately 5000 more diagnosed every year (Gomes
* Tel.: þ13012751886.E-mail address: [email protected]
1360-8592/$ - see front matter ª 2008 Elsevier Ltd. All rights reserved.doi:10.1016/j.jbmt.2008.04.040
a v a i l a b l e a t w w w . s c i e n c e d i r e c t . c o m
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c om / j b m t
Journal of Bodywork & Movement Therapies (2009) 13, 328e335

7/18/2019 ELA Blatzheim 2009
http://slidepdf.com/reader/full/ela-blatzheim-2009 2/8
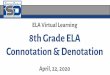
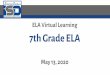
et al., 2006; NIH; accessed on October 8, 2006). ALS affectsall races with the typical age of infection being between 40and 60 yr, men being more prevalently affected (Czaplinskiet al., 2006; Ganzini et al., 2002; Gomes et al., 2006). ALSaffects the upper and lower motor neurons, destroying thebrain’s ability to send messages to the target muscle byway of the spinal cord (Figure 1aec). Because ALS isa gradual progressive disease, the symptoms may be mis-
diagnosed until they become more severe, with theaverage time to diagnosis being from 11 to 17.5 months(Bello-Haas et al., 1998; Gomes et al., 2006). There arethought to be two different causes of ALS: it could be anautoimmune illness or it could have a genetic association(Ganzini et al., 2002). The genetic link is seen in 5e10% ofpatients (Appel, 2006; Gomes et al., 2006). ALS is a fataldisease since there is no cure. The only drug treatment for ALS is Riluzole, which may slow down the naturalprogression of the illness, possibly prolonging life (Bruijnet al., 2006; Czaplinski et al., 2006). All other treatmentsfor ALS are to manage symptoms and improve the quality oflife (Galbussera et al., 2006). Therefore, a multi-teamapproach is beneficial to support patients and their families
(Bruijn and Cudkowicz, 2006; Galbussera et al., 2006;Jenkinson et al., 1999). While treating patients the benefitneeds to be assessed, not all healthcare professionals agree
that massage is useful for the ALS patient (Sancho andBoisson, 2006) The purpose of this paper is to explore theeffects of ALS on a patient, and the benefit of massagetherapy for the patient and their family.
Stages of ALS
The importance of knowing the stages of ALS helps pre-plan
for the patient’s increasing needs. There are six stages thatare based on the ALS patient’s abilities outlined by Bello-Haas et al. (1998) study. See Table 1 for Stages of ALS.
Issues facing the ALS patient and family
Once diagnosed, the medical community wants the ALSpatient to focus on his death, considering advanceddirectives, living wills, and quality of life issues (Ganziniet al., 2002). While these issues are important to theautonomy of the patient, so is the need to live life in theface of a terminal illness. Continuity of care is alsoimportant in a complex, life-threatening illness. Receivingsupport from a palliative care medical team can makea difference in the life of the patient and the family. Theautonomy of the patient may be affected by the wishes of
Figure 1 (a) The brain and the lateral cortical spinal track within the spinal cord, leading to the muscles. (b) Shows where the
upper motor neurons interdigitate with the lower motor neurons. It is the lower motor neurons that send the signal to the muscles.
(c) Shows the location of the lateral cortical spinal track in the spinal cord.
Interdisciplinary palliative care, including massage, in treatment of amyotrophic lateral sclerosis 329

7/18/2019 ELA Blatzheim 2009
http://slidepdf.com/reader/full/ela-blatzheim-2009 3/8
the family. Since both the patient and the family membersmay have different views on treatment and quality of life,communication is extremely important (Trail et al., 2003,2004). The patient and the caregivers must both beeducated in treatment options to limit disagreements (Trailet al., 2003).
The dying person finds time important and wants to usehis time in a productive manner. Because ALS affects
movement and speech, the ability to maximize autonomyholds greater meaning than in other illnesses that do notaffect these skills. Within 3e5 yr from first symptoms, theperson may lose his ability to move, swallow, eat, talk, andbreathe, giving the patient a very limited time to say anddo all activities he has postponed (Ganzini et al., 2002).
In the critically ill person, continuity of care can meana major difference in the quality of life. Continuity of carecan also save time and energy for the patient and thefamily, decreasing stress levels as the treatment teamworks together. The family is busy taking care of thepatient; this time increases, as the patient gets sicker (Cannaets et al., 2004). The family should not be expected
to relay important health information from healthcareprovider to healthcare provider.A palliative care unit that has an interdisciplinary focus,
including massage, to care for the ALS patient will supportpatients and their families. The focus on life in a palliativecare unit changes the outlook for the patient and the familyto one of living instead of an outlook of dying. The outlookon life helps the patient and their family live life to thefullest. Since the palliative care unit’s goal is to maximizepatient’s care and quality of life, the patient maintainsautonomy. Cannaets et al. (2004) shows that a palliativecare unit improves the quality of life for both the caregiversand the patient with ALS. Rochs et al. (2005) found that 90%of 171 ALS patients died peacefully.
The stress associated with ALS is multilayered. What thepatient feels is stressful may not be what the caregiver feels is stressful.
The physiological effects of stress decrease theimmune response for both the caregiver and the patientswith ALS (Trail et al., 2004). In a number of studies,massage has been shown to decrease hormones that areassociated with stress, anxiety, depression and pain(Field et al., 2007, 2005; Lund et al., 2006). Cortisol hasbeen blamed for adversely affecting cells of the immunesystem; by decreasing the levels of cortisol the immunesystem is better able to mount an immune response ( Fieldet al., 2007). Studies have shown that 15e20 min massage
can have an effect on physical and psychological stress bydecreasing anxiety, and increasing mental relaxation(Bost and Wallis, 2006; Ouchi et al., 2006).
With the progression of the symptoms, patients and their families face new and difficult issues. Coping mechanismsthat help patients and their families accomplish activitiesof daily living; bathing, dressing, toilet use, transferring,difficulty in using hands and arms, turning and moving in
bed, picking objects up, holding and turning pages in books,writing clearly, doing jobs around the house, talking,walking, and eating, need to be revised frequently (Bello-Haas et al., 1998; Jenkinson et al., 1999). Issues facing thecaregivers are numerous and can be overwhelmingly timeconsuming. Not having enough personal time or being over burdened with responsibility can have a direct effect on thecaregivers’ feelings toward and relationships with the ALSpatient. The caregivers may also have issues about the carethey are giving to the ALS patient, such as what to do, or whether they should do more. The increased responsibilityissues that the caregivers feel places stress on the care-givers and the patients and may have a psychosocial effect
on the caregivers. The complex issues facing the patientand the caregivers have negative effects on the quality oflife and possibly the caregivers’ health (Trail et al., 2004).
Symptoms
Symptoms of ALS include muscle weakness, fatigue,twitching, atrophy, spasticity, muscular pain, constipation,oropharyngeal dysfunction, pseudobulbar affect, weightloss, and breathing issues. All the voluntary muscles in thebody can be affected based on what area of neurons aredying. Many of the symptoms are interrelated. There arealso case reports of ALS patients developing complex
regional pain syndrome from the immobility caused by thisillness (Shibata et al., 2003).
Skeletal muscle dysfunction
Skeletal muscle dysfunction includes muscle weakness,fatigue, twitching, atrophy, spasticity, and pain. Again,many of these symptoms are interrelated. Because of thelower motor neuron death, the muscles are not gettingthe nerve’s impulse (Kent-Braun and Miller, 2000). Motor units cannot be recruited causing a decrease in force for that muscle movement (Kent-Braun and Miller, 2000).Muscle fatigue has been found to be caused by upper
Table 1 Stages of ALS adapted by Bello-Haas et al. (1998).
Stages of ALS
Stage 1 The first stage of ALS is marked by limited muscle weakness, causing poor endurance. The patient is still
independent.
Stage 2 The patient shows moderate weakness and cardiovascular deconditioning.
Stage 3 The ALS patient has severe weakness but is still ambulatory. The patient may need help standing up from
a seated position. This is the stage when adaptive equipment is needed because of mild to moderate limitation.
Stage 4 In this stage the legs have severe weakness while the arms show mild weakness.Stage 5 The patient’s mobility and endurance have deteriorated and the patient experiences progressive weakness.
Stage 6 Here the patient requires the maximum assistance with activities of daily living. The patient is now bedridden.
330 K. Blatzheim

7/18/2019 ELA Blatzheim 2009
http://slidepdf.com/reader/full/ela-blatzheim-2009 4/8
motor neuron death, according to a study by Kent-Braun(Kent-Braun and Miller, 2000). There are many differentcauses for muscle atrophy, and it is not well understood(Lecker et al., 2004; Leger et al., 2006). ALS affects theneuronal pathways that carry the signal to the muscle.Since the signal is not reaching the muscle, it is notrecruited, causing disuse of the muscle. Given the Law ofReversibility, if a muscle is not used, that muscle will
atrophy which may explain some of the atrophy found inthe ALS patient. Muscle twitching and spasticity of ALSpatients reflects damage to the corticospinal tract(Figure 1b) and the suprasegmental control of the spinalcord segmental reflexes (Ashworth et al., 2006). Spas-ticity affects the ease of movement and the activity ofdaily living for the ALS patient. Spasticity also increasesjoint contracture that can cause pain and increasemovement issues. As ALS progresses, physical pain, frommuscle contraction and spasticity, becomes an issue for the patient. Pain can also be caused by disuse and fromprevious musculoskeletal issues. If the pain is leftuntreated, it decreases the quality of life. Several studieshave explored the effects of massage on healthy indi-
viduals. The studies have found massage to be effectivefor muscle recovery for grip strength after fatigue butresults were not statistically significant for improvementin sports performance (Brooks et al., 2005; Harmer, 1991;Hemmings et al., 2003; Robertson et al., 2004). While thiswas studied on healthy people one could expect to findthe same with the ALS patient population aiding in thesymptom of fatigue the patient experiences from thedisease (Ernst, 1998).
Oral-motor dysfunction
Oropharngeal dysfunction, bulbar palsy, is common in ALS.
This dysfunction leads to problems involving talking, swal-lowing and salivating, and possibly aspiration pneumonia asthe disease progresses. The symptom of weight loss may besecondary to the constellation of symptoms associated withbulbar palsy, where the muscles of the mouth are affected,as well as upper limb control issues. Weight loss issues havebeen thought of as secondary issues linked with breathingissues (Desport et al., 2005). As the ALS patient has a harder time breathing, therespiratorymuscles need to work harder,using more calories (Desport et al., 2005).A study by Desportet al. (2005) found that breathing issues measured by vitalcapacity were not associated with weight loss. The samestudy found that there is a hypermetabolism componentassociated with an average of 10% of ALS patients (Desport
et al., 2005). Weight loss may be associated with muscleweakness of the neck. The patient is no longer able to holdhis head up to eat or drink (Bello-Haas et al., 1998). Weightloss may also be associated with constipation. Medications,poor hydration, or the muscles of the gut not working prop-erly due to motor neuron death may cause constipation withthe ALS patient (Francis et al., 1999). Dehydration is anunder-recognized issue with the ALS patient (Francis et al.,1999). Some of the causes of dehydration are difficultiesswallowing, thickened secretion, fatigue, movement issues,and malaise (Francis et al., 1999). Several studies haveinvestigated the effects of massage on weight gain in pre-term, full-term newborn infants and rats, showing that
massage increases weight gain and also increases gastroin-testinal hormones that aid in the absorption of nutrients(Field, 2001, 2004, 2006; Holst et al., 2005). One couldexpect to see the same in the ALS patient population.Massage may be helpful for the ALS patients that exhibitsdecreased control with bowl function. A study on spinal cordinjury patients with neurogenic bowl dysfunction found thatdecreased abdominal distention and fecal incontinence
while increasing defecation frequency occurred after abdominal massage (Ayas et al., 2006).
Treatment
There are many studies looking at curative treatments for ALS. Currently treatment for ALS is treating the symptoms,thus improving the quality of life for the ALS patient (Trailet al., 2004). The only FDA-approved treatment for ALS isRiluzole (Bruijn and Cudkowicz, 2006). Riluzole has beenshown to moderately increase the quantity of life (Bruijnand Cudkowicz, 2006). Many studies are looking for other treatment methods. The US Food and Drug Administration,as an investigational drug, have approved Myotrophin (IGIF-I). This has shown promise in promoting regeneration ofmotor neurons and the survival of motor nerves (Bello-Haaset al., 1998).
Currently, the goals of treatment should be to help thepatient maintain mobility and function, optimize currentfunction, and help the patient manage symptoms to improvethe patient’s quality of life (Ashworth et al., 2006; Bello-Haaset al., 1998). Since ALS causes muscle weakness it would makesense to start an exercise program to assist in strength main-tenance. However, studies have shown that there is onlya short term, 3e6 month, benefit for exercise (Drory et al.,2001). The use of creatine supplementation for ALS patientshasshownsome temporary improvementfor specific situations
as a symptomatic treatment (Mazzini et al., 2001).
Muscular skeletal mobility concerns
Pain
The ALS patient may have had muscular pain before theonset of symptoms that were attributed to commoneveryday life. Muscle pain can be aggravated by the loss ofmovement as the disease progresses (Shibata et al., 2003).ALS causes spasticity that increases muscle pain as well asjoint pain. The first line of treatment for pain includesmassage, physical therapy, non-narcotic analgesics, anti-
inflammatory, and antispasticity medications (Miller et al.,1999). Opioids are used when the pain is not controlled withthe above list.
In the later stages of ALS the inability to move andchange positions can cause pain. To address this issue,special mattresses can be used to rotate the patient fromone side to another. During the day assistive range-of-motion (ROM) and exercise may be helpful.
Activities of daily living
Because of muscle weakness, the ALS patient may findorthosis to be helpful in completing tasks of daily living.
Interdisciplinary palliative care, including massage, in treatment of amyotrophic lateral sclerosis 331

7/18/2019 ELA Blatzheim 2009
http://slidepdf.com/reader/full/ela-blatzheim-2009 5/8
Occupational therapists are responsible for helping the ALSpatient maintain independence safely as the symptomsprogress. As muscle weakness and joint instability prog-resses, adaptive equipment such as slings for shoulder discomfort and foot and ankle bracing to improve gait anddecrease risks of falling may be needed. Environmentalmodifications to maintain independence consist of raisedtoilet seats, grab bars, wheelchairs, reaching and grabbing
devices, and tub seats (Rochs et al., 2005). Energy conser-vation tools can be taught to the ALS patients. Occupationaland physical therapist would help the ALS patient. Occupa-tional therapist will assist the patient and family by imple-mentation of adaptive equipment and education on energyconservation. Range of motion (ROM) and bracing, for example the lower extremity, will be the task of the physicaltherapy team leading to better gait and function.
Muscle
ROM exercise is important for the ALS patient. Decreasedmotion of any joint may decrease the ability for the patientto interact with his environment. Exercising that includes
cardiovascular and muscle strength should be encouraged,with caution not to over exercise, if the patient over exercises, spasticity and cramping can increase. As thepatient becomes weaker, bracing of muscles may beneeded to improve gait or grasping strength. By improvingthe patient’s gait, there is a decreased risk for falling, andby improving grasping strength ADLs (activities of dailyliving) are accomplished with less energy. As the patientbecomes more affected by ALS, there will be a decrease inmovement. This decrease may lead to spasticity andcramping. Spasticity can cause decreased ROM in any joint.This decreased ROM can cause joint changes and lead topain and movement issues. Decreased ROM leads to spas-
ticity that leads to decreased movement that leads todecreased ROM, a vicious cycle. Medications used todecrease spasticity in other conditions have unwanted sideeffect for the ALS patient: muscle weakness and fatigue.Medications that are used include quinine sulfate, diaz-epam, carbamazepine, phenytoin, baclofin, and tizanidine.The physical therapists can work with the ALS patient tomaintain or increase the joint’s ROM either actively or passively. Massage therapists can also address spasticity,cramping, and ROM of joints by soft-tissue manipulation,stretching and passive range of motion (Bello-Haas et al.,1998; Diego et al., 2002; Hernandez-Reif et al., 2001; Moriet al., 2004; Morl et al., 2005; Preyde, 2000; Rochs et al.,2005). A number of soft-tissue manipulation modalities can
release trigger point and other tissue to promote circula-tion and reduce spasm, contraction and increase function(Preyde, 2000). Keep in mind that ALS is a degenerativedisease so musculoskeletal benefits may be temporary sincethe cause of spasticity is neurological (Cherkin et al., 2001;Delaney et al., 2002).
Oral-motor concerns
Sialorrhea
This symptom has a social issue that can cause problems for the ALS patient. Since ALS affects the muscles of the mouthcausing poor management for the saliva, the patient drools.
Sialorrhea symptoms can be confused with symptoms thatare caused by thick mucus. The treatments are not alike sodiagnosis is important. Sialorrhea could be treated withmedications such as glycopyrrolate, benztropind, trans-dermal hyoscine, atropine, trihphenide hydrocholoride or amitripty (Miller et al., 1999). The treatment for thickenedmucus is propranolol or metoprolol (Milleret al., 1999).Inthelater stages of ALS, or when the patient is ill, manual cough
assistance may be needed (Miller et al., 1999).
Dysarthria and communication
Approximately 80% of all ALS patients develop communi-cation issues resulting from both upper and lower neuronimpairment (Francis et al., 1999). Early symptoms may bea nasal sound to the patient’s voice (Francis et al., 1999). Asmall percentage (30%) has problems abducting their vocalcords (Francis et al., 1999). As the muscles of respirationare affected, then the vital capacity is decreased, limitingthe patient’s breath. Insufficient breath affects the volumeof the ALS patient’s voice and proper phrasing of sentences.A speech therapist can support the patients and their families. The patient can start exercises to strengthen the
tongue and diaphragm. The speech therapist can help thepatient with phrasing so the speech is better understood. Apotential fix for the family may be fitting the primarycaregiver with a hearing aid, if the caregiver is diagnosedwith a hearing loss. The caregiver to aid in communication,leading to an economic effective solution, can use ampli-fication devices. If communication is severely affected, theaid of augmentative devices, such as a simple paper andpencil or a computer with a high tech keyboard base, willassist in communication (Francis et al., 1999).
Nutrition
Nutrition is affected by many different issues for the ALS
patient. Symptoms such as oral-motor weakness, musclefatigue, choking risks, upper limb control, and head controlcan cause self-feeding to be challenging (Miller et al.,1999). Poor nutrition can cause a worsening of muscleatrophy, and other symptoms such as weakness and fatigue(Miller et al., 1999). As swallowing becomes harder, thepatient is at increased risk for dehydration and aspirationpneumonia. In the beginning stages a speech pathologistcan assist with modifications of food consistency. Thespeech pathologist will also evaluate the patient to deter-mine if the patient is at an increased risk for aspiration. Apercutaneous endoscopic gastrostomy (PEG) is indicated ifthe patient cannot maintain his own weight or hydrationstatus or is at risk for aspiration pneumonia. The placement
of a PEG is also dependant on respiratory issues. Thepatient must be able to maintain his own airway after theprocedures so if his vital capacity is below 50% the surgerycannot be performed. The ALS patient who has a PEG maystill eat.
The physical issues that surround eating may need onlyslight modifications to resolve. The ALS patient may havebetter control of his eating utensils with simple modifica-tions. Adding foam around the handle of the utensil makesgrasping the tool easier for weakened or fatigued muscles.Neck supports to hold the head inan uprightposition can alsobe very helpful in self-feeding. As the neck muscle becomesmore affected, a stronger neck collar may be needed.
332 K. Blatzheim

7/18/2019 ELA Blatzheim 2009
http://slidepdf.com/reader/full/ela-blatzheim-2009 6/8
Respiratory concerns
Respiratory issues greatly affect the life expectancy of theALS patient. Symptoms of respiratory insufficiency includedyspnea that may be associated with exercise or position,marked fatigue that may or may not be associated withnocturnal waking or hypoventilation, morning headachesfrom hypoventilations, and insomnia from hypoventilation,anxiety or physical discomfort. With positional dyspnea thepatient may experience techypnea or tachycardia. Posturemisalignments of the spine that are found in patients whohave a history of neck and back, and/or rib misalignmentscan lead to a mechanical disadvantage for breathing (Yoz-
batiran et al., 2006). Nerve root irritation and musclespasm may also have an inhibitory effect on the patient’slung volume and chest expansion (Yozbatiran et al., 2006).Respiratory symptoms can also include tremors, cyanosis,and increased respiratory infections (Rochs et al., 2005).The ALS patient will need to decide on what respiratorysupport he wants before he needs a more invasive treat-ment. The simplest treatment for dyspnea is treatmentwith oxygen, as needed, and calming techniques.
Treatments that include postural drainage and manual-assisted coughing can be helpful in clearing the airway of itssecretions (Rochs et al., 2005). The use of external resis-tance inspiratory muscle training has shown promise in
improving lung functions (Rochs et al., 2005). The use of analternating pressure devise can also be helpful. As thedisease progresses, treatment for respiratory symptoms caninclude a bilevel positive pressure ventilation (BICAP) or nocturnal intermittent positive pressure ventilation(NIPPV), both treatments are the first level of mechanicalventilation used with ALS patients. An external nasal maskcan be worn to help with both non-invasive ventilators. For invasive ventilation a tracheotomy is needed. By adding thenon-invasive ventilation, respiratory symptoms, such asdyspnea, hypoxemia, atclectasis, and respiratory infection,may decrease. When respiratory symptoms are decreasedthe patient is healthier leading to a longer quantity and animproved quality of life (Chaisson et al., 2006). Treatment
with mechanical ventilation is voluntary. Francis et al.(1999) found that ALS patients who choose ventilator support may be ineligible for hospice care, since theventilator can be seen as a medical device used toimproved the quantity of life.
It is important to note that treatment for other ALSsymptoms may affect respiratory drive. The physical painan ALS patient experiences is treated with opiates, whilespasticity is treated with muscle relaxors; both treatmentsdecrease the respiratory drive. Physical modalities used inthe non-ALS including hot packs, physical therapy andmassage has shown a significant decrease in pain scores andin peak expiratory flow rate with neck pain, and an overall
increase in thoracic expansion (Yozbatiran et al., 2006).This finding should also hold true for the ALS patient sincethe mechanical advantage would be the same. Since theALS patient develops decreased respiratory function,treating pain or spasticity can decrease the patient’squantity of life.
One of the side effects of compromised breathing isanxiety. In the last phase of respiratory insufficiency thetreatment of anxiety is needed to improve the quality oflife for the ALS patient. As the anxiety progresses in theterminal stages, treatment includes morphine, diazepam,midazolam, and chlorpromazine (Miller et al., 1999). The
treatment for anxiety can also treat other issues in theterminal patient, such as pain and hunger (Howard andOrrell, 2002).
Psychological concerns
Depression, anxiety, and pseudobulbar affects are commonin the ALS patient. Treatment includes counseling, relaxa-tion techniques, ALS symptom management, and medica-tion for depression and anxiety. Pseudobulbar affectsimprove with the medications used to treat depression.Medications used for psychological symptoms includeserotonin reuptake inhibitors such as citalopram, fluoxe-tine, or paroxetine for depression; benzodiazepines and
amitriptyline for anxiety; and a combination of depressionand anxiety medication for the pseudobulbar symptoms.Several studies have examined the hormones that areassociated with stress, anxiety, depression and pain. Thestudies have shown that massage can reduce thesehormones in the blood and urine as well as the patientsreporting a better mood, reduced anxiety and pain ( Fieldet al., 2005, 2007; Lund et al., 2006). Studies on elderlyinstitutionalize patients found that low back massagewould not have statistical significance but have clinicalsignification on depression and anxiety (Fraser, 1993; Moyer et al., 2004).
Conclusion
ALS is a fatal, progressive neurological disease thatthreatens the autonomy of the patient. As the diseaseprogresses, the patients need increasing support from their families and health care providers. The goal of the healthcare team is to manage the symptoms of the ALS patient.Many studies support an interdisciplinary approach to thecare of the ALS patient to improve their quality of life(Bruijn and Cudkowicz, 2006; Cannaets et al., 2004; Franciset al., 1999; Howard and Orrell, 2002; Jenkinson et al.,1999). The goal of a multidisciplinary team is to educatethe patient and family, provide psychological support, help
Table 2 Main stress from ALS adapted from Trail et al. (2003, 2004).
Main stress from ALS
Patient’s Caregivers
Worries about illness progression and dependency issues Worries about the patient’s illness progression,Problems speaking Concerns about patient’s swallowing and eating difficulties,
Muscle weakness Worries about loved ones’ emotional and physical well-being
Interdisciplinary palliative care, including massage, in treatment of amyotrophic lateral sclerosis 333

7/18/2019 ELA Blatzheim 2009
http://slidepdf.com/reader/full/ela-blatzheim-2009 7/8
with the ever-changing requirements for rehabilitation andappropriate equipment, and provide access to communityresources. Pautex et al. (2005) went so far as to recom-mend an interdisciplinary team even in hospitals that donot have an ALS clinic.
Treatment with speech therapists, physical therapists,occupational therapists, massage therapists, and mentalhealth care providers can be helpful in improving the
quality of life for the ALS patient (Francis et al., 1999;Howard and Orrell, 2002). While the benefits of massagehave been shown for all people (Field et al., 2007, 2005;Lund et al., 2006). Medical interventions to the body needto be weighted on the benefits to the patient against therisk to the patient. While treating ALS patients, the benefitneeds to be assessed by the patient and the patient’streatment. Not all healthcare professionals agree thatmassage is useful for the ALS patient (Sancho and Boisson,2006). It is also important to note that in a number ofstudies that look at the amount of pressure needed for massage to be effective and have found that moderatepressure more effective than any other pressure (Fieldet al., 2007, 2006, 2004). Healthcare professional can also
help the family with education. An interdisciplinary palli-ative care unit that includes a massage therapist to supportthe whole patient and, indirectly, supports the family,improving the quality of life for both (Tables 1 and 2).
Acknowledgments
The author thanks Susan Keleher, Instructor at the Univer-sity of Maryland and Sue Bennett for their critical review ofthe manuscript.
References
Appel, S., 2006. Is ALS a systemic disorder? Evidence from MuscleMitochondria Experimental Neurology 198, 1e3.
Ashworth, N., Satkunam, L., Deforge, D., 2006. Treatment for spasticity in amyotrophic lateral sclerosis/motor neuron disease(review). The Cochrane Library 3.
Ayas, S., Leblebici, B., Sozay, S., Bayramoglu, M., Niron, E.A.,2006. The effect of abdominal massage on bowel function inpatients with spinal cord injury. American Journal of PhysicalMedicine and Rehabilitation 85 (12), 951e955.
Bello-Haas, V., Kloos, A., Mitsumoto, H., 1998. Physical therapy for a patient through six stages of amyotrophic lateral sclerosis.Physical Therapy 78 (12), 1313e1324.
Bost, N., Wallis, M., 2006. The effectiveness of a 15 min weeklymassage in reducing physical and psychological stress in nurses.Australian Journal of Advanced Nursing 23 (4), 28e33.
Brooks, C., Woodruff, L., Wright, L., et al., 2005. The immediateeffects of manual massage on power-grip performance after maximal exercise in health adults. The Journal of Alternativeand Complementary Medicine 11, 1093e1101.
Bruijn, L., Cudkowicz, M., 2006. Therapeutic targets for amyo-trophic lateral sclerosis current treatments and prospects for more effective therapies. Neurotherapeutics 6 (3), 417e428.
Cannaets, N., Dierckx de Casterle, B., Grypdonck, M., 2004. Palli-ative care, care for life: a study of the specificity of residentialpalliative care. Qualitative Health Research 14 (6), 816e835.
Chaisson, K., Walsh, S., Simmons, Z., et al., 2006. A clinical pilotstudy: high frequency chest wall oscillation airway clearance inpatients with amyotrophic lateral sclerosis. AmyotrophicLateral Sclerosis 7, 107e111.
Cherkin, D.C., Eisenberg, D., Sherman, K.J., Barlow, W.,Kaptchuk, T.J., Street, J., et al., 2001. Randomized trialcomparing traditional Chinese medical acupuncture, thera-peutic massage, and self-care education for chronic low backpain. Archives of Internal Medicine 161 (8), 1081e1088.
Chio, A., Gauthier, A., Vignola, A., et al., 2006. Caregiver time usein ALS. Neurology 67 (5), 902e904.
Czaplinski, A., Yen, A., Simpson, E., et al., 2006. Slower diseaseprogression and prolonged survival in contemporary patients
with amyotrophic lateral sclerosisd
is the natural history ofamyotrophic lateral sclerosis changing? Archives of Neurology63, 1139e1143.
Delaney, J.P., Leong, K.S., Watkins, A., Brodie, D., 2002. The short-term effects of myofascial trigger point massage therapy oncardiac autonomic tone in healthy subjects. Journal ofAdvanced Nursing 37 (4), 364e371.
Desport, J., Torny, F., Lacoste, M., et al., 2005. Hypermetabolismin ALS: correlations with clinical and paraclinical parameters.Neur-degenerative diseases 2, 202e207.
Diego, M., Field, T., Hernandez-Reif, M., et al., 2002. Spinal cordpatients benefit from massage therapy. International Journal ofNeuroscience 112, 133e142.
Drory, V., Goltsman, E., Reznik, J., et al., 2001. The value ofmuscle exercise in patients with amyotrophic lateral sclerosis.
Journal of the Neurological Sciences 191, 133e
137.Ernst, E., 1998. Does post-exercise massage treatment reduce
delayed onset muscle soreness? A systematic review. BritishJournal of Sports Medicine 32, 212e214.
Field, T., 2001. Massage therapy facilitates weight gain in preterminfants. American Psychological Society 10 (2), 51e54.
Field, T., Hernandez-Reif, M., Diego, M., et al., 2004. Massagetherapy by parents improves early growth and development.Infant Behavior and Development 03 (04), 435e442.
Field, T., Hernandez-Reif, M., Diego, M., 2005. Cortisol decreasesand serotonin and dopamine increase following massagetherapy. International Journal of Neuroscience 115, 1397e1412.
Field, T., Diego, M., Hernandez-Reif, M., et al., 2006. Moderateversus light pressure massage therapy leads to greater weightgain in preterm infants. Infant Behavior and Development 7
(11), 574e
578.Field, T., Diego, M., Hernandez-Reif, M., et al., 2007. Massage
therapy research. Developmental Review 27/, 75e89.Francis, K., Bach, J., DeLisa, J., 1999. Evaluation and rehabilita-
tion of patients with adult motor neuron disease. Archives ofPhysical Medicine and Rehabilitation 80, 951e963.
Fraser, J., 1993. Psychophysicological effects of back massage onelderly institutionalized patients. Journal of Advanced Nursing18 (2), 238e245.
Galbussera, A., Tremolizzo, L., Brighina, L., et al., 2006. Vitamin Eintake and quality of life in amyolrophic lateral sclerosispatients: a follow-up case series study. Neurological Science 27,190e193.
Ganzini, L., Johnston, S., Silveira, M., 2002. The final month of lifein patients with ALS. Neurology 59, 428e431.
Gomes, A., Soares, A., Peviani, S., et al., 2006. The effect of 30 minof passive stretch of the rat soleus muscle on the myogenicdifferentiation, myostatin, and atrogin-1 gene expressions.Archives of Physical Medicine and Rehabilitation 87, 241e246.
Harmer, P., 1991. The effect of pre-performance massage on stridefrequency in sprinters. Athletic Training 26, 55e59.
Hemmings, B., Smith, M., Gaydon, J., et al., 2003. Effects ofmassage on physiological restoration perceived recovery, andrepeated sports performance. British Journal of Sports Medicine34, 109e115.
Hernandez-Reif Field, T., Krasnegor, J., et al., 2001. Lower back pain is reduced and range of motion increased after massage therapy. International Journal of Neuroscience 106,131e145.
334 K. Blatzheim

7/18/2019 ELA Blatzheim 2009
http://slidepdf.com/reader/full/ela-blatzheim-2009 8/8
Holst, S., Lund, I., Petersson, M., 2005. Massage-like strokinginfluences plasma levels of gastrointestinal hormones, includinginsulin, and increases weight gain in mail rats. AutonomicNeuroscience Basic and Clinical 120 (1-2), 73e79.
Howard, R., Orrell, R., 2002. Management of motor neuronedisease. Postgraduate Medical Journal 78, 736e741.
Jenkinson, C., Fitzpatrick, R., Brennan, C., et al., 1999. Develop-ment and validation of a short measure of health status for individuals with amyotrophic lateral sclerosis/motor neurone
disease: ALSAQ-40. Journal of Neurology 264 (3), III16e
III21.Kent-Braun, J., Miller, R., 2000. Central fatigue during isometric
exercise in amyotrophic lateral sclerosis. Muscle and Nerve 23,909e914.
Lecker, S., Jagoe, R., Gilbert, A., et al., 2004. Multiple types ofskeletal muscle atrophy involve a common program of changesin gene expression. FASEB Journal 18, 39e51.
Leger, B., Vergani, L., Soraru, G., et al., 2006. Human Skeletalmuscle atrophy in amyotrophic lateral sclerosis revealsa reduction in Akt and an increase in atrogin-1. FASEB Journal 20(3), 583e585.
Lund, I., Lundeberg, T., Carleson, J., et al., 2006. Corticotropinreleasing factors in urine. A possible biochemical marker offibromyalgia response to massage and guided relaxation.Neuroscience Letters 403, 166e171.
Mazzini, L., Balzarini, C., Colombo, R., et al., 2001. Effects ofcreatine supplementation on exercise performance andmuscular strength in amyotrophic lateral sclerosis: preliminaryresults. Journal of Neurological Sciences 191, 139e144.
Miller, R., Rosenberg, J., Gelinas, D., et al., 1999. Practiceparameter: the care of the patient with amyotrophic lateralsclerosis (an evidence-based review): report of the quality ofstandards subcommittee of the American academy ofneurology. Neurology 52 (7), 1311e1329.
Mori, H., Ohsawa, H., Tanaka, H., et al., 2004. Effect of massage onblood flow and muscle fatigue following isometric lumbar exercise. Medical Science Monitor 10 (5), 173e178.
Moyer, C.A., Rounds, J., Hannum, J.W., 2004. A meta-analysis ofmassage therapy research. Psychological Bulletin 130 (1), 3e18.
Ouchi, Y., Kanno, T., Okada, H., Yoskikawa, E., Shinke, T.,Nagasawa, S., Minoda, K., Doi, H., 2006. Changes in cerebralblood flow under the prone condition with and withoutmassage. Neuroscience Letters 407, 131e135.
Pautex, S., Janssens, J., Vaugnar, H., et al., 2005. Management ofpatients with amyotrophic lateral sclerosis. Swiss MedicalWeekly 135, 626e629.
Preyde, M., 2000. Effectiveness of massage therapy for subacutelow-back pain; a randomized controlled trial. Canadian MedicalAssociation Journal 162 (12), 1815.
Robertson, A., Watt, J., Galloway, S., 2004. Effects of leg massageon recovery from high intensity cycling exercise. British Journalof Sports Medicine 38, 173e176.
Rochs, J., Reis, C., Simoes, R., et al., 2005. Diagnostic investigationand multidisciplinary management in motor neuron disease.Journal of Neurology 252, 1435e1447.
Sancho, P., Boisson, D., 2006. Physical therapy in ALS. RevueNeurologigue 162 (HS2) 4S253e4S255.
Shibata, M., Abe, K., Jimbo, A., et al., 2003. Complex regional painsyndrome type i associated with amyotrophic lateral sclerosis.The Clinical Journal of Pain 19 (1), 69e70.
Trail, M., Nelson, N., Van, J., et al., 2003. A study comparing
patients with amyotrophic lateral sclerosis and their caregiverson measures of quality of life, depression, and their attitudestoward treatment options. Journal of Neurological Science 209,79e85.
Trail, M., Nelson, N., Van, J., et al., 2004. Major stressors facingpatients with amyotrophic lateral sclerosis (ALS): a survey toidentify their concerns and compare with those of their care-givers. ALS and Other Motor Neuron Disorders 5, 40e45.
Yozbatiran, N., Gelecek, N., Karadibak, D., 2006. Influence ofphysiotherapy programme on peak expiratory flow rate (PEF)and chest expansion in patients with neck and low back pain.Journal of Back and Musculoskeletal Rehabilitation 19, 35e40.
Interdisciplinary palliative care, including massage, in treatment of amyotrophic lateral sclerosis 335