Embed Size (px)
Citation preview

EKG Interpretation

Objectives• Review approach for reading EKGs
• Keep it simple
• Impress preceptors on rounds

Resources

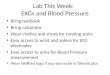
Interpretation• Rate• Rhythm• Axis• Hypertrophy• Ischemia, Injury, Infarction

Rate
• Count # of large boxes between 2 successive R-waves:
• 1 box = 300 bpm• 2 boxes = 150 bpm• 3 boxes = 100 bpm• 4 boxes = 75 bpm• 5 boxes = 60 bpm• 6 boxes = 50 bpm• 7 boxes = 43 bpm• 8 boxes = 37 bpm


Irregular rhythms
• If the R-R Interval is irregular:
• Count the number of QRS complexes in a 10 sec span (that is on the entire EKG) and multiply it by 6! {or no. of QRS complexes in a 6 sec span multiplied by 10}


Rhythm• Determine whether sinus or non-sinus

Sinus Rhythm• Every QRS preceded by P-wave• P-wave has normal morphology
• Duration <0.12 sec (<3 boxes)• Height <2.5 mm
• P-wave has normal axis• Upright in lead II
• Sinus “arrhythmia”• Rate varies with respiration

Arrhythmias• Irregular rhythms• Escape rhythms• Premature beats• Tachy-arrhythmias• Heart blocks

Irregular rhythms
• Wandering atrial pacemaker• P wave shape varies• Atrial rate <100• Irregular ventricular rhythm
• Multifocal atrial tachycardia• Same as above, but rate>100
• Atrial fibrillation / flutter

Escape rhythm• Junctional escape
• Originates in AV junction• Narrow QRS (<0.10ms)• Rate 40-60
• Ventricular escape• Originates in ventricles• Wide QRS (not normal depolarization)• Rate 20-40

Junctional escape

Premature beats• Irritable focus spontaneously fires a single stimulus
• Atrial (PAC)
• Ventricular (PVC)

Paroxysmal tachycardia• A very irritable focus suddenly paces rapidly
• Paroxysmal atrial tachycardia• Paroxysmal junctional tachycardia• Paroxysmal ventricular tachycardia
• Look for presence/absence of P waves and ventricular appearance to determine type


Supraventricular tachycardia• Often can’t tell between PAT and PJT (both originate above
ventricles & produce narrow QRS)• Rapid PAT can be so rapid that P waves not visible• Supraventricular tachycardia (SVT) is umbrella term for both

Flutter vs fibrillation• Flutter caused by single ventricular focus firing rapidly (250-
350x/min)
• Fibrillation caused by multiple foci firing rapidly (350-450x/min)

Atrial flutter & fibrillation
• Atrial flutter• Atrial fire so rapidly not every impuse triggers
ventricular contraction• 2:1, 3:1, 4:1 block, etc
• Atrial fibrillation• Irregularly irregular

Ventricular flutter & fibrillation• Ventricular flutter has smooth sine-wave appearance
with no jagged waves
• Often degenerates into ventricular fibrillation

Heart blocks• AV block
• Bundle branch block

AV block• 1st degree: delay in normal AV conduction
• PR >0.20 sec• 2nd degree: interruption in normal AV condution• 3rd degree: complete dissocation in AV conduction

1st degree AV block
• PR >0.20 sec

2nd degree AV block• Type I (Mobitz I) aka Wenckebach
• PR progressively gets longer with each beat• QRS complex is dropped• Cycle repeats
• Type II (Mobitz II)• PR stays constant, then one beat isn’t conducted


2:1 AV block• Sometimes hard to tell Wenckebach vs Mobitz II apart if both
have 2:1 conduction (2 P waves then QRS)• Wenckebach
• Likely if PR interval lengthened and QRS normal• Mobitz II
• Likely if PR interval normal and QRS widened

3rd degree AV block• Complete dissocation between atria & ventricles• Atria fire regularly• Ventricles contract independently at either junctional escape
(40-60) or ventricular escape (20-40)• If above AV nodal junction, then junctional escape rhythm
occurs


Bundle branch block• Wide QRS (<0.12 sec)• Left
• RR’ in V5 & V6• Right
• RR’ in V1 & V2• Incomplete
• QRS 0.10-0.12 sec

Left bundle branch block

Right bundle branch block

Axis• Measures overall electrical activity of heart• Limb leads (I, aVF) used to quickly determine axis• Lead I: 0 degrees• aVF: +90 degrees

Axis

0
-90
I
aVF
+_
Lead I If lead I is positive, the green zone reveals thearea of electrical activity

0
-90
I
aVF
If aVF is positive, the red zone reveals the areaof electrical activity
–
+
aVF

0
-90
I
aVF If we superimpose these onto one another we find the axis to be between 0° & +90°
+90

Left axis deviation• Usually caused by HTN, aortic valvular disease &
cardiomyopathies
• aVF: negative
• Lead I: positive

0
-90
I
aVF
+_
If lead I is positive then the blue zone is the area of electrical activity
+90
Lead I

0
-90
I
aVF
+
_If aVF is negative, the green zone is the area of electrical activity
+90
aVF

0
-90
I
aVF
If we superimpose these onto one another we find the axis to be between 0° & –90°
+90


Right axis deviation• Usually secondary to enlarged right ventricle or pulmonary
disease• Pulmonary HTN• COPD• Acute pulmonary embolism

0
-90
I
aVF
If lead I is negative thegreen zone encompassesthe area of electrical activity
+90
180
+_
Lead I

0
-90
I
aVF
If aVF is positive, the red zone reveals the areaof electrical activity
+90
180
+
_aVF

0
-90
I
aVFIf we superimpose these onto one another, we find the axis to be between 90° & 180°
+90
180


Right atrial enlargement


Left atrial enlargement


Left ventricular hypertrophy• Large S in V1• Large R in V5• S in V1 + R in V5 >35mm = LVH• aVL > 11-13mm = LVH


Right ventricular hypertrophy• Normally S > R in V1
• Large R in V1 = RVH
• Large R in V1 will get smaller V2V4


Ischemia, Injury, Infarction• Ischemia
• T wave inversions or ST depression• Injury
• ST segment elevation• >1mm in 2 or more contiguous leads
• Infarction• Q waves
• 1mm wide or 1/3 height of QRS

Ischemia

Injury

Infarction

Location• Anterior = V1-V4• Inferior = II, III, aVF• Lateral = I, aVL• Posterior = Large R wave, ST depression in V1 or V2

Anterior MI

Inferior MI

Anterolateral

Posterior MI

Tips for rounds
• Review EKG silently (don’t talk though method unless asked to)
• Ignore interpretation at top of 12-lead• Intervals usually ok
• Summarize findings• Rate• Rhythm• Axis• Hypertrophy• Ischemia, infarction

Example• This is a normal sinus rhythm, rate 60, normal intervals, no
hypertrophy, no ischemic or infarctive changes• This is normal sinus rhythm, rate 75, 1st degree AV block, left
ventricular hypertrophy, possible old inferior MI• This is atrial fibrillation with a rapid ventricular response


• NSR• Rate 80• Normal axis• Normal intervals, no block
• No hypertrophy• No ischemic or infarctive
changes


• NSR (sinus tachycardia)• Rate 111• Normal axis• Normal intervals
• One premature ventricular contraction
• No hypertrophy• No ischemic or infarctive
changes


• NSR, rate 100• 1st degree AV block• Normal axis
• Borderline LVH by voltage
• No ischemic or infarctive changes


• NSR, rate 100• LAD• Normal intervals
• No hypertrophy• Acute anterior wall MI with
reciprocal ST depression inferiorly


• NSR, rate ~60• Normal axis• Right bundle branch
block
• No hypertrophy• No ischemic or
infarctive changes


• NSR, rate ~90• Normal axis• Normal intervals
• No hypertrophy• Old inferior wall MI
with ?inferior ischemia


• Atrial flutter with variable block
• Normal QRS (no BBB)
• No hypertrophy• No ischemic or
infarctive changes


• NSR, rate 75• Left axis deviation• Left bundle branch
block
• Left ventricular hypertrophy
• Can’t tell infarction because of LBBB repolarization changes


• Ventricular tachcardia• Rate ~170• Don’t really care
about anything else


• Accelerated junctional
• Rate ~80• Normal axis
• LVH by voltage• No ischemic or
infarctive changes

Interpretation• Rate• Rhythm• Axis• Hypertrophy• Ischemia, Injury, Infarction