Embed Size (px)
Citation preview

Evid Based Integrative Med 2004; 1 (3): 189-194REVIEW ARTICLE 1176-2330/04/0003-0189/$31.00/0
© 2004 Adis Data Information BV. All rights reserved.
Eicosapentaenoic AcidPromising Nutritional Supplement in the Treatment of Cancer Cachexia inElderly Patients
Nagi B. Kumar and Kyle Dalton
H. Lee Moffitt Cancer Center & Research Institute, University of South Florida, Tampa, Florida, USA
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 189
1. Cancer Cachexia and Implications of Malnutrition in the Elderly Cancer Patient . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 190
2. Cancer Cachexia: Potential Mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 190
3. Efficacy of Current Therapies for Cancer Cachexia in the Elderly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 190
4. Eicosapentaenoic Acid as an Anticachectic Agent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 191
5. Valid Intermediate Endpoint Biomarkers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 191
5.1 Morphological Markers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192
5.2 Biochemical Markers of Protein Status (Serum Albumin and Transferrin) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192
5.3 Molecular Targets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192
5.4 Immune and Inflammatory Markers (Interleukin-6 and Tumour Necrosis Factor-α) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192
5.5 Functional Markers (Karnofsky Performance Score) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 193
6. Future Directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 193
Cancer cachexia affects about half of all cancer patients and is associated with negative effects on functionalAbstractstatus and quality of life. This condition is also a major contributor to the morbidity and mortality of patients withadvanced malignancy. Although current strategies to improve appetite and lean body mass by administeringappetite stimulants, increasing physical activity and using nutritional supplementation have a scientific rationale,randomised studies have continued to demonstrate that a reduction in the loss of lean body mass is difficult toachieve unless the underlying metabolic abnormalities in cancer cachexia are corrected. Initial studies usinganimal models have demonstrated that nuclear factor-κ B (NF-κB) is upregulated in cancer cachexia, increasingproteolysis and breakdown of myofibrillar proteins, which results in sarcopenia. Laboratory studies have shownthat eicosapentaenoic acid (EPA), an n-3 fatty acid, has anticachectic effects and may attenuate proteindegradation by preventing NF-κB accumulation in the nucleus. EPA is associated with weight stabilisation, gainin lean body mass, and improvement in quality-of-life markers in weight-losing patients with advancedpancreatic cancer. Although animal studies have demonstrated the molecular basis of the effects of EPA, this hasnever been validated in human clinical trials. On the basis of the promising results of the laboratory and clinicalstudies, we hypothesise that selective targeting of proteasome activity by EPA (a polyunsaturated fatty acid)administered to cancer patients, including elderly patients, with cancer cachexia will alter metabolic abnormali-ties by downregulating NF-κB, modulating immune and inflammatory response and thus preventing thebreakdown of myofibrillar proteins. This will result in promotion of anabolism, reduction of weight loss andincrease in lean body mass and physical function, thus establishing a case for future, prospective clinical trials.

190 Kumar & Dalton
1. Cancer Cachexia and Implications of ia.[5,13-15] The transcription factor nuclear factor-κ B (NF-κB) is aMalnutrition in the Elderly Cancer Patient known regulator of the genes that encode cytokines, cytokine
receptors and cell-adhesion molecules that modulate immune andThe complex syndrome of cancer cachexia involves altered inflammatory responses. The cytokines 40–44 tumour necrosis
metabolism of proteins, carbohydrates and lipids, leading to an- factor (TNF)-α and interleukin (IL)-6 have been shown to sup-orexia, weight loss and loss of adipose tissue and skeletal muscle press myogenesis by activating NF-κB in muscle cells through amass manifested in the cardinal feature of emaciation.[1-5] Cancer process that involves disassociation of NF-κB from its inhibitorycachexia affects about half of all cancer patients and occurs protein IκB.[16,17] A key proteolytic pathway is then activatedprimarily in patients with advanced disease. Cachexia is associated leading to degradation of IκB and breakdown of myofibrillarwith negative effects in the patient’s functional status and quality proteins. In cancer cachexia, this dysregulation may induce theof life and is a major contributor to the morbidity and mortality of cellular breakdown of muscle and bone, resulting in sarcopeniapatients with advanced malignancy.[1,2] Twenty percent of deaths and osteopenia. In simple starvation, the body readily adapts toin cancer patients are related to cancer-induced or treatment- calorie deficit by shifting of fatty acids as the major source ofrelated wasting and malnutrition; this number may be as high as energy, thereby preserving lean body mass. In cancer cachexia, the40% in certain populations. Anorexia or lack of appetite resulting body fails to make this adaptation.[18] The cytokines produced byin involuntary decline in food intake is the most common problem the host in response to tumour presence cause metabolic abnor-contributing to malnutrition for individuals with cancer. Malnutri- malities observed in cancer cachexia, including hyperglycaemia,tion can be defined as a nutritional deficit or altered nutritional insulin resistance, increased basal energy expenditure, decreasedstatus associated with increased risk of adverse clinical events, lipoprotein lipase, lipidaemia and proteolysis of muscle.[2,5,19-21]
such as morbidity or death.[1,2,6] Nearly in three senior Americans This results in malnutrition, disproportionate wasting of lean bodymay be at high risk for malnutrition, which amounts to almost 10 mass and loss of strength and functional status, leading to negativemillion Americans today.[7] The prevalence of malnutrition in the outcomes in the cancer patient in addition to profound effects onfree-living elderly is relatively low (5–10%) compared with hos- quality of life.[22,23] These symptoms are accelerated in the elderly,pitalised or institutionalised elderly,[8] where it is estimated that who have relatively lower steroid hormone levels as a result of30–65% are malnourished. Malnutrition is an important predictor ‘hormonal ageing’ and lowered physical activity as a result ofof morbidity and mortality, even more so in the elderly than in treatment-related fatigue, which has been demonstrated to contrib-younger adults.[8-10] Unplanned weight loss, especially in the eld- ute to lowered bone mineral density and muscle mass. These age-erly cancer patient,[8-10] is also identified as a clinically significant related conditions may thus be exacerbated, resulting in falls,independent predictor of morbidity and mortality. Even a weight fractures and general muscle weakness. Although it was initiallyloss of 5% in older persons reflects poor health, hospitalisation and believed that the best way to treat cancer cachexia is to cure thea higher rate of mortality. Research also indicates that the elderly cancer, with our better understanding of the molecular mechanismare particularly at risk for deficiency of vitamins and trace miner- of cancer cachexia based on animal studies, in most cases, theals. Other pre-existing chronic diseases and drug therapies in this consequence of cancer cachexia is what often leads to death andspecial population may increase requirements of certain nutrients not the cancer.[5]
because of changes in absorptive and metabolic capacity. Recentstudies have also shown that advanced malnutrition is much more 3. Efficacy of Current Therapies for Cancerdifficult to treat in the elderly than in younger adults, and failure to Cachexia in the Elderlycorrect malnutrition delays recovery and has a significant impact
Traditional therapies have focused on treating the patient withon functional dependence and quality of life.[11,12]
appetite stimulants and nutritional interventions using high calo-rie-protein supplemental feeding, with limited success in treating2. Cancer Cachexia: Potential Mechanismscancer cachexia. High calorie and high protein supplemental feed-
Based on animal models, several potential mechanisms have ings result in substitution of regular meals and thus a reduction ofbeen proposed to explain the protein catabolism resulting in mus- caloric and protein intake in this patient population.[24-28] Appetitecle wasting observed in cancer cachexia. One of the most plausible stimulants have been shown to ameliorate or slow age-relatedmechanisms of cancer cachexia comes from a group of studies anorexia and unintentional weight loss in other populations butusing rodent models of muscle wasting, which have indicated that have not been shown to increase lean body mass or markers ofaccelerated protein degradation by the proteasome is the principal protein metabolism in cachectic elderly cancer patients. The mostcause of muscle atrophy and wasting induced by cancer cachex- common agents used to enhance patient appetite are orexigenic
© 2004 Adis Data Information BV. All rights reserved. Evid Based Integrative Med 2004; 1 (3)

Eicosapentaenoic Acid in Treatment of Cancer Cachexia 191
agents such as megestrol acetate, which acts by reducing cytokine 4. Eicosapentaenoic Acid as anproduction.[27] However, this is also associated with a reduction in Anticachectic Agentsteroid hormones, which results in decline in muscle mass (which
Evidence from laboratory and clinical studies has demonstratedis already decreased in the elderly) and an increase in fat mass.that eicosapentaenoic acid (EPA), an n-3 fatty acid, has antitumourAnother common agent is dronabinol, a cannabis derivativeand anticachectic effects.[1,23-31] EPA is an essential fatty acid thatdemonstrated to enhance appetite and mood in cancer patients.cannot be synthesised completely by mammalian tissue and has toHowever, the pharmacokinetic profile of this agent in elderlybe consumed in the diet. These polyunsaturated fats are present incancer patients has not been examined. In addition, mood altera-fish oils such as cod liver, sardine and salmon oil. There is notions secondary to drug treatment can be confused with dementia,established dietary reference intake for n-3 fatty acids, yet theespecially in individuals who have never used cannabinoids in theadequate intake (AI) is set at 1.6 g/day and 1.1 g/day for men andpast.[11,12,28] More recently, antidepressants such as Remeron® 1
women, respectively. While intake in the US occurs at much lower(mirtazapine) have been used to treat depression, which may be athan the proposed AI and no signs of deficiency are observed, themajor reversible contributor to weight loss in elderly cancer pa-AI is proposed to provide optimal health benefits associated withtients. Increasing physical activity, aerobic and anaerobic, as aconsuming n-3 fatty acids.non-pharmacological means to improve muscle and bone mass is
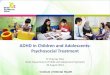
As indicated earlier, initial studies using animal models havecurrently being examined.demonstrated that NF-κB is upregulated in cancer cachexia, in-In a recently completed pilot study to determine the prevalencecreasing proteolysis and inducing apoptosis in myotubes. Severaland efficacy of the use of traditional anti-anorectic therapies forrecent laboratory studies have shown that EPA may attenuatethe treatment of cancer cachexia at Moffitt Cancer Center, weprotein degradation, by preventing NF-κB accumulation in thecollected data on elderly cancer patients, all of whom were onnucleus.[14,15] Administration of n-3 fatty acids and EPA capsuleschemotherapy or radiation therapy and were placed on the aboveor supplements with EPA has been shown to be associated totraditional anticachectic therapies at the cancer centre. Using aweight stabilisation, gain in lean body mass, and improvement indata collection instrument, we collected basic, easily available andquality-of-life markers in weight-losing patients with advancedpertinent serial data on markers of nutritional status (anthropome-pancreatic cancer.[29-31] Although the patient population had termi-try and weight) and biochemical data (albumin, protein status,nal illness and a life expectancy of 2 months, promising changes inhaemoglobin/haematocrit [anaemia] and lymphocytes [immuni-net gain in weight, lean body mass and improved quality ofty]) from the start to the end of treatment. Prospective data werelife[1,23,29-31] were noted. Nutritional supplementation alone hasobtained in this pilot study from 17 subjects. Although the mecha-been unable to reverse the process of muscle wasting, since itnism is poorly understood, our pilot study indicated that thearises from the activation of the ubiquitin proteasome pathway,current anticachectic therapies may be effective only in increasingwhich is independent of nutritional intake. It is logical, then, toweight or maintaining the bodyweight of the cancer patient andhypothesise that agents such as EPA that can inhibit NF-κB mightmay produce moderate increases or stable markers of immunitystimulate recovery of muscle mass in this patient population andand protein status. Cannabinoids produced the most significantoffer the most promise for the development of an effective molec-weight gain and corticosteroids and Megace® produced no changeular-based approach for the treatment of cancer cachexia[5] (figurein weight over the 6- to 8-week period of observation. However,1).lymphocyte counts and serum albumin decreased in all three
groups. It is important to note that this was only a pilot study with a 5. Valid Intermediate Endpoint Biomarkerssmall sample size, using easy-to-obtain intermediate endpointbiomarkers (IEBs) to monitor efficacy of treatment and performed The utility of IEBs in the development of agents for treatingin a group of acutely ill cancer patients during treatment. However, cancer cachexia is solidly established. With rigorous attention toit is evident that although these strategies to improve appetite and methodology, identification of high-risk cohorts and validatedlean body mass may have a scientific rationale and merit, IEBs, the evaluation of efficacy, safety and the mechanism ofrandomised studies, including our pilot study, have continued to action of potential agents for the treatment of cancer cachexia indemonstrate that reduction in the loss of lean body mass is difficult clinical trials has become an increasingly critical area of research.to achieve unless the underlying metabolic abnormalities are cor- In addition, EPA may have multiple molecular activities, some ofrected.[12,24-28] which may be interrelated. Also, a single activity, even if it is the
1 The use of trade names is for product identification purposes only and does not imply endorsement.
© 2004 Adis Data Information BV. All rights reserved. Evid Based Integrative Med 2004; 1 (3)

192 Kumar & Dalton
critical to incorporate these markers in studies, to be measuredserially along with bodyweight.[36-40]
5.2 Biochemical Markers of Protein Status (Serum Albuminand Transferrin)
Assessment of protein status is critical in the identification andtreatment of protein metabolism. Measurements of body composi-tion should be combined with more objective and sensitive mea-sures of protein status such as biochemical assessment of intravas-cular and visceral protein stores. Serum protein level is influencedby hydration status, and rate of synthesis can be altered by liver orrenal dysfunction, sepsis and surgery. It may thus be important tocombine two valid IEBs that represent intravascular and visceral
Prevent loss of lean body mass and weight
Prevention of breakdown of myofibrillar protein
Modulation of immune and Inflammatory responsesDecreases PIF and cytokine production (IL-6, TNFα)
Downregulates NF-κB and PIFUpregulates IκB
Eicosapentaenoic acid
Fig. 1. Molecular-based therapeutic approach in the treatment of cancercachexia in the elderly cancer patient. IκB = inhibitory factor-κ B; lL =interleukin; NF-κB = nuclear factor-κ B; PIF = proteolysis-inducing factor;TNF = tumour necrosis factor.
protein pools – transferrin and albumin, respectively – as thebiochemical indicators of protein status.
agent’s predominant pharmacological activity, may not be theSerum albumin is the most validated as a prognostic index and
most important or the only one effecting the metabolic modula-the most readily available biochemical parameter used to assess
tions. Thus, although observing effects at the morphological andprotein status. However, its relatively long half-life (14–20 days)
biochemical levels is a key approach to identifying potentialmakes it slow to respond to dietary interventions and thus more
agents, it should be complemented by molecular targeting.[32]
suitable for prospective long-term interventions exceeding 25days.
5.1 Morphological Markers Transferrin is a serum β-globulin protein synthesised primarilyin the liver, but in contrast to albumin it is located intravascularly
Morphological markers such as anthropometric measurements (as a transporter of iron), has a shorter half-life (8–10 days) andresponds more rapidly to changes in protein status. Serum transfer-of body mass index (height, weight) and skinfold measurements ofrin, either singly or as part of a multiparameter index, is theupper and lower body compartments to determine body composi-strongest predictor of patient mortality and morbidity.[6,41]tion (lean body mass, percentage of fat)[33] are valid IEBs that can
be used to reliably measure efficacy of treatment. Current weight5.3 Molecular Targetsis useful as an indicator of nutritional risk or depletion only if it is
evaluated in comparison to the patient’s usual weight. Weight lossInitial studies have demonstrated that NF-κB is upregulated inmust also be assessed in relation to its duration and whether it is
cancer cachexia, increasing proteolysis and inducing apoptosis inunintentional or intended weight loss.[34] In addition, weight andmyotubes. Several recent laboratory studies have shown that EPAweight change must be assessed in combination with other anthro-may attenuate protein degradation, by preventing NF-κB accumu-pometric parameters such as body composition, as a marker oflation in the nucleus and upregulating IκB.[14,15] Proteasomes thusagent efficacy.may indeed be the target for EPA, in its role in prevention of
The most widely accepted method of estimating body composi- proteolysis and subsequent sarcopenia in cancer cachexia. It istion changes is the use of standardised equipment and procedures thus relevant to measure serum proteasomes using methods de-for measuring triceps skinfold and mid-arm muscle circumference. scribed and previously validated by our group.[42,43]
These values are then compared with a table of standard measure-ments based on a reference group of healthy individuals. There is 5.4 Immune and Inflammatory Markers (Interleukin-6 andstill controversy regarding the validity of these measurements as Tumour Necrosis Factor-α)part of the initial baseline assessment owing to influences ofinactivity and the disease process on muscle mass and difficulty Unlike anorexia of aging, cancer cachexia features a range ofwith obtaining accurate results in the presence of oedema or metabolic responses triggered by inflammatory and immunologi-obesity.[35] However, there is general agreement that these mea- cal responses. It is believed that the putative mediators of cancersurements can be useful for serial evaluation, as proposed in this cachexia are cytokines, and increased expression of TNFα andstudy, to identify changes in body fat and lean body mass. It is thus IL-6 has been observed in patients with cancer cachexia. It is thus
© 2004 Adis Data Information BV. All rights reserved. Evid Based Integrative Med 2004; 1 (3)

Eicosapentaenoic Acid in Treatment of Cancer Cachexia 193
3. Barton BE. IL-6-like cytokines and cancer cachexia: consequences of chronicideal to select these cytokines as valid biochemical IEBs that caninflammation. Immunol Res 2001; 23 (1): 41-58
be measured.[4,19,41,44-46]4. Mantovani G, Madeddu C, Gramignano G, et al. Association of serum IL-6 levels
with comprehensive geriatric assessment variables in a population of elderlycancer patients. Oncol Rep 2004 Jan; 11 (1): 197-206
5.5 Functional Markers (Karnofsky Performance Score)5. Hamerman D. Molecular-based therapeutic approaches in treatment of anorexia of
aging and cancer cachexia. J Gerontol A Biol Sci Med Sci 2002 Aug; 57 (8):Limitations in the activities of daily living have been identified M511-8
6. Dempsey DT, Mullen JL. Macronutrient requirements in the malnourished cancersecondary to and as a cause of weight loss in older adults. Cancerpatient. Cancer 1985; 55: 290-4
and other chronic diseases pose difficulties for the elderly in 7. Kinsella K, Velkoff VA. An aging world: 2001. Washington, DC: US CensusBureau, 2001 Nov. Series P95/01-1carrying out activities of daily living. A loss of postural and
8. Vellas B, Lauque S, Andrieu S, et al. Nutrition assessment in the elderly. Curr Opinlocomotive muscle mass has been observed within 7 days ofClin Nutr Metab Care 2001 Jan; 4 (1): 5-8
inactivity.[47] The Karnofsky performance scale index allows pa- 9. Pirlich M, Lochs H. Nutrition in the elderly. Best Pract Res Clin Gastroenterol2001 Dec; 15 (6): 869-84tients to be classified as to their functional impairment. This has
10. Huffman GB. Evaluating and treating unintentional weight loss in the elderly. Ambeen used to compare effectiveness of different therapies and to Fam Physician 2002 Feb; 65 (4): 640-50assess the prognosis in individual patients; it has been validated in 11. Morley JE. Pathophysiology of anorexia. Clin Geriatr Med 2002 Nov; 18 (4):
661-73the elderly cancer patient population.[48] This serves as an ideal,12. Morley JE. Anorexia and weight loss in older persons. J Gerontol A Biol Sci Med
easy-to-use scale in a clinical setting to reliably measure changes Sci 2003 Feb; 58 (2): 131-713. Whitehouse AS, Tisdale MJ. Increased expression of the ubiquitin-proteasomein functional status.
pathway in murine myotubes by proteolysis-inducing factor (PIF) is associatedwith activation of the transcription factor NF-κB. Br J Cancer 2003 Sep; 89 (6):
6. Future Directions 1116-2214. Smith HJ, Tisdale MJ. Signal transduction pathways involved in proteolysis-
inducing factor induced proteasome expression in murine myotubes. Br JCurrent clinical trials using EPA have tested the anticachecticCancer 2003 Nov; 89 (9): 1783-8
efficacy in terminal pancreatic cancer patients with a 2-month life 15. Whitehouse AS, Khal J, Tisdale MJ. Induction of protein catabolism in myotubesby 15 (S)-hydroxyeicosatetraenoic acid through increased expression of theexpectancy. This agent has never been evaluated in populationsubiquitin-proteasome pathway. Br J Cancer 2003 Aug; 89 (4): 737-45with a relatively better prognosis, nor in special populations such
16. Wigmore SJ, Ross JA, Falconer JS, et al. The effect of polyunsaturated fatty acidsas elderly cancer patients, in whom effective, proactive and timely on the progress of cachexia inpatients with pancreatic cancer. Nutrition 1996
Jan; 12 (1 Suppl.): S27-30interventions can improve mortality and quality of life. It is also17. Mitch WE, Price SR. Transcription factors and muscle cachexia: is there a
clear that there is a need to use a molecular-based approach to therapeutic target? Lancet 2001 Mar; 357 (9258): 734-5identify potential nutritional agents for the treatment of cancer 18. Schneider SM, Al-Jaouni R, Pivot X, et al. Lack of adaptation to severe malnutri-
tion in elderly patients. Clin Nutr 2002 Dec; 21 (6): 499-504cachexia. It may also be critical to examine the potential to19. Laviano A, Meguid MM, Rossi-Fanelli F. Cancer anorexia: clinical implications,
intervene in pathways understood at the molecular level to im- pathogenesis, and therapeutic strategies. Lancet Oncol 2003 Nov; 4 (11):686-94prove appetite, modify metabolic alterations that contribute to
20. Tisdale MJ. Cachexia in cancer patients. Nat Rev Cancer 2002 Nov; 2 (11): 862-71wasting, and downregulate transcription factors or cytokine-in-21. Tisdale MJ. The ‘cancer cachectic factor’. Support Care Cancer 2003 Feb; 11 (2):
duced events to treat cancer cachexia. Based on the evidence from 73-822. Ravasco P, Monteiro-Grillo I, Vidal PM, et al. Cancer: disease and nutrition arelaboratory and clinical trials, EPA is a promising agent that may
key determinants of patients’ quality of life. Support Care Cancer 2004; 12 (4):attenuate protein degradation by targeting the proteasomes, and 246-52
23. Wallace JI, Schwartz RS. Epidemiology of weight loss in humans with specialthere is enough evidence to warrant its use in clinical trials toreference to wasting in the elderly. Int J Cardiol 2002 Sep; 85 (1): 15-21examine its efficacy for the treatment of cancer cachexia.
24. Desport JC, Gory-Delabaere G, Blanc-Vincent MP, et al. FNCLCC. Standards,options and recommendations for the use of appetite stimulants in oncology(2000). Br J Cancer 2003 Aug; 89 Suppl. 1: S98-100Acknowledgements
25. Golden AG, Daiello LA, Silverman MA, et al. University of Miami division ofclinical pharmacology therapeutic rounds: medications used to treat anorexia inWe thank Jayne Wellner for her assistance with the data management andthe frail elderly. Am J Ther 2003 Jul-Aug; 10 (4): 292-8
in the preparation of this manuscript. No funding was used to assist in the26. Walsh D, Nelson KA, Mahmoud FA. Established and potential therapeutic applica-
preparation of this review. The authors have no conflicts of interest directly tions of cannabinoids in oncology. Support Care Cancer 2003 Mar; 11 (3):relevant to the contents of this review. 137-43
27. Karcic E, Philpot C, Morley JE. Treating malnutrition with megestrol acetate:literature review and review of our experience. J Nutr Health Aging 2002 May;
References 6 (3): 191-2001. Fearon KC, Von Meyenfeldt MF, Moses AG, et al. Effect of a protein and energy 28. Morley JE. Orexigenic and anabolic agents. Clin Geriatr Med 2002 Nov; 18 (4):
dense N-3 fatty acid enriched oral supplement on loss of weight and lean tissue 853-66in cancer cachexia: a randomised double blind trial. Gut 2003 Oct; 52 (10): 29. Barber MD, Fearon KC, Tisdale MJ, et al. Effect of a fish oil-enriched nutritional1479-86 supplement on metabolic mediators in patients with pancreatic cancer cachexia.
2. Tisdale MJ. Wasting in cancer. J Nutr 1999 Jan; 129 Suppl.: 243S-6S Nutr Cancer 2001; 40 (2): 118-24
© 2004 Adis Data Information BV. All rights reserved. Evid Based Integrative Med 2004; 1 (3)

194 Kumar & Dalton
30. Barber MD, Fearon KC. Tolerance and incorporation of a high-dose eicosapentae- 42. Kazi A, Urbizu DA, Kuhn DJ, et al. A natural musaceas plant extract inhibitsnoic acid diester emulsion by patients with pancreatic cancer cachexia. Lipids proteasome activity and induces apoptosis selectively in human tumor and2001 Apr; 36 (4): 347-51 transformed, but not normal and non-transformed, cells. Int J Mol Med 2003
Dec; 12 (6): 879-8731. Barber MD, McMillan DC, Preston T, et al. Metabolic response to feeding inweight-losing pancreatic cancer patients and its modulation by a fish-oil- 43. Kazi A, Daniel KG, Smith DM, et al. Inhibition of the proteasome activity, a novelenriched nutritional supplement. Clin Sci (Lond) 2000 Apr; 98 (4): 389-99 mechanism associated with the tumor cell apoptosis-inducing ability of genis-
32. Kumar NB, Cantor A, Allen K, et al. The specific role of isoflavones in reducing tein. Biochem Pharmacol 2003 Sep; 66 (6): 965-76prostate cancer risk. Prostate 2004 May; 59 (2): 141-7
44. Barber MD, McMillan DC, Wallace AM, et al. The response of leptin, in-33. Al-Jaouni R, Schneider SM, Filippi J, et al. Evolution of body composition during
terleukin-6 and fat oxidation to feeding in weight-losing patients with pancreat-weight loss in elderly malnourished patients: a longitudinal study. Clin Nutr
ic cancer. Br J Cancer 2004 Mar; 90 (6): 1129-322003 Aug; 22 Suppl. 1: S4
45. Barber MD, Wigmore SJ, Ross JA, et al. Proinflammatory cytokines, nutritional34. Nutrition Assessment of Adults. Manual of clinical dietetics. Chicago (IL): Thesupport, and the cachexia syndrome: interactions and therapeutic options [ab-American Dietetic Association, 1992stract]. Cancer 1998 Mar; 82 (5): 100035. Frisancho AR. Anthropometric standards for the assessment of growth and nutri-
tional status. Ann Arbor (MI): University of Michigan Press, 1990 46. Mantovani G, Maccio A, Mura L, et al. Serum levels of leptin and proinflammatorycytokines in patients with advanced-stage cancer at different sites. J Mol Med36. Kumar NB, Cantor A, Allen K, et al. Android obesity at diagnosis and breast2000; 78 (10): 554-61carcinoma survival. Cancer 2000 Jun; 88 (12): 2751-7
37. Kumar NB, Allen K, Cantor A, et al. Weight gain associated with adjuvant 47. Baracos VE. Management of muscle wasting in cancer-associated cachexia. Can-tamoxifen therapy in stage I and II breast cancer: fact or artifact. Breast Cancer cer 2001; 92 (6 Suppl.): 1669-77Res Treat 1997; 44: 135-43
48. Schag CC, Heinrich RL, Ganz PA. Karnofsky performance status revisited: relia-38. Kumar NB, Lyman GH, Allen K, et al. Timing of weight gain and breast cancer
bility, validity, and guidelines. J Clin Oncol 1984; 2: 187-93risk. Cancer 1995; 76 (2): 243-9
39. Schapira DV, Kumar NB, Lyman GH, et al. Upper body fat distribution andendometrial cancer risk. JAMA 1991; 266: 1808-11
Correspondence and offprints: Dr Nagi B. Kumar, H. Lee Moffitt Cancer40. Schapira DV, Kumar NB, Lyman GH, et al. Abdominal obesity and breast cancer
Center & Research Institute, University of South Florida, 12902 Magnoliarisk. Ann Intern Med 1990; 112: 182-6Drive, Tampa, FL 33612-9497, USA.41. Laye S, Gautron L. Cytokines and nutritional disorders [in French]. J Soc Biol
2003; 197 (2): 123-31 E-mail: [email protected]
© 2004 Adis Data Information BV. All rights reserved. Evid Based Integrative Med 2004; 1 (3)