EHS Webinar and...Peggy Jenkins Jeffrey Johnson Fay Johnston Peter Mazey Mark Nicas Fabienne Reisen...
50
EHS Webinar: Wildfire Smoke & Public Health in British Columbia June 5 th , 2014 Vancouver, BC, Canada
EHS Webinar and...Peggy Jenkins Jeffrey Johnson Fay Johnston Peter Mazey Mark Nicas Fabienne Reisen Susan Roberecki Jat Sandhu Tom Kosatsky Health Canada Acknowledgements 1. Consensus
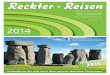
Key message – Smoke can disperse over thousands of kilometers affecting distant populations e.g. PHOTO LEFT: More than 30 taiga fires in Far East of Russia - 2012, image from July 10,2012 when over 4000 hectares had burned – smoke distributed 1000s of kilometres, with increased PM in parts of BC In 2010 smaller fires, closer to Moscow, fire smoke and heat associated with and estimated substantial increases in mortality in Moscow (estimated 10 to 50% increases) PHOTO RIGHT: In 2010, smoke from fires burning in BC affected air quality in Edmonton and beyond. August 1998 forest fires in Canada/NWT, >1 million ha produced large haze layers over Europe (http://onlinelibrary.wiley.com/doi/10.1029/2001JD900115/full) 2010 – fires lit to burn forest for agricultural use in Indonesia – peat fires – smoldering combustion, lots of smoke generated, dispersed internationally. ____________________ EDMONTON, ALTA: AUGUST 19, 2010 -- An exercise class near the Kinsmen Sports Centre in a smoke filled river valley with a barely visible High Level Bridge in Edmonton, August 19, 2010. The smoke is being blown in by the prevailing winds from the B.C. forest fires which is causing health alerts. Photograph by: Ed Kaiser , edmontonjournal.com
Agenda
1. Guidelines for Public Health Decision Making During Wildfire Smoke Events - Catherine Elliott
2. BC Asthma Monitoring System - Sarah Henderson
3. Questions and Discussion
Guidelines for Public Health Decision Making During Wildfire
Smoke Events
EHS Webinar
June 4th, 2014
Vancouver, BC, Canada
Project Team Catherine Elliott Karen Rideout Prabjit Barn Lawrence Pernica Scientific Advisory Committee Michael Brauer Mike Flannigan Sarah Henderson Fay Johnston Susan Roberecki Authors Prabjit Barn Linda Dix-Cooper Sandra Duran Anya Keefe Kathryn Morrison Colleen Reid Hind Sbihi Joanne Stares Angela Yao
Expert Reviewers Ryan Allen Nima Atabaki Michael Brauer Ed Chessor Rita Ciconte Shelley DuTeaux Paul English Rick Erland Mike Flannigan Paul Hasselback Sarah Henderson Peggy Jenkins Jeffrey Johnson Fay Johnston Peter Mazey Mark Nicas Fabienne Reisen Susan Roberecki Jat Sandhu Tom Kosatsky Health Canada
Acknowledgements
1. Consensus Guidelines
2. Preliminary BC Guidance: Practice Pearls
Scope & Considerations
• Wildfire, not planned, not structural
• Informative, not prescriptive
• Must be applied within local & situational context
Health effects Active and exciting area of research Strong consistent evidence for respiratory outcomes and asthma exacerbations (medication use, physician visits, hospitalization) across numerous studies and locations it has been challenging to find cardiovascular associations with wildfire PM, few studies are suggestive - Unlike urban PM, where chronic exposure has strongest association with cardiovascular outcomes, For other outcomes, research is currently limited – e.g. low birth weight
Respiratory: asthma, COPD bronchitis, pneumonia
All cause mortality
Cardiovascular
Birth outcomes
• Atherosclerosis
• Childhood respiratory disease
• Lung cancer
• Birth outcomes
Linked to short-term PM exposure but not yet studied for wildfire smoke:
Presenter
Presentation Notes
Health effects Active and exciting area of research Strong consistent evidence for respiratory outcomes and asthma exacerbations (medication use, physician visits, hospitalization) across numerous studies and locations it has been challenging to find cardiovascular associations with wildfire PM, few studies are suggestive - Unlike urban PM, where chronic exposure has strongest association with cardiovascular outcomes, For other outcomes, research is currently limited – e.g. low birth weight
•Older adults •Unborn children •Populations with pre-existing respiratory disease
•Populations with pre-existing cardiovascular disease •Populations with lower socio-economic status
Populations susceptible to wildfire smoke
• Children
• Populations with chronic inflammatory diseases (e.g., diabetes, obesity)
• Populations with specific genetic polymorphisms that mediate physiologic response to air pollution
Populations susceptible to particulate matter but evidence
for wildfire smoke is insufficient
Presenter
Presentation Notes
Populations that are known or suspected to be susceptible to wildfire smoke:
• Smoke measures: • Monitored PM (MoE)
• Modeled smoke (BCCDC)
• Predicted smoke (BlueSky)
• Health outcomes: • Medication refills
• Physician visits
• Emergency visits
• Hospital admissions
Situational Awareness during wildfire smoke events
Presenter
Presentation Notes
Smoke: each measure has different strengths and weaknesses & provides different types of information Health: those of lower acuity/severity – higher numbers and therefore may have higher signal and be more responsive to smoke Limitations: what is available
There are few studies that evaluate the effectiveness of staying indoors at reducing adverse health effects of wildfire smoke. The existing evidence suggests that staying indoors reduces asthma symptoms in children, but the effectiveness in other populations has barely been studied. If good quality indoor air is achieved, then staying indoors even part of the time is likely to provide some benefit for everyone. The benefits of staying indoors must be weighed against potential harms such as disruption of normal activities and associated health, social and economic costs.
Limited evidence of reduction in childrens’ asthma symptoms
Presenter
Presentation Notes
There are few studies that evaluate the effectiveness of staying indoors at reducing adverse health effects of wildfire smoke. The existing evidence suggests that staying indoors reduces asthma symptoms in children, but the effectiveness in other populations has barely been studied. If good quality indoor air is achieved, then staying indoors even part of the time is likely to provide some benefit for everyone. The benefits of staying indoors must be weighed against potential harms such as disruption of normal activities and associated health, social and economic costs.
Clean indoor air (existing central air, HEPA, electrostatic precipitator)
Home Clean Air Shelter
Air cleaner
Presenter
Presentation Notes
The evidence supports the use of home-CASs in reducing indoor particulate matter concentrations during wildfire smoke events. In the absence of HEPA filtration or EP, increased filtration may be achieved by using a higher efficiency filter within existing air systems or even by running air systems with standard filtration, provided that they are on recirculation mode. There is limited published research demonstrating that HEPA filters and EPs improve health outcomes during wildfire events. The evidence is suggestive of improved markers of cardiac effects in adults and reduced asthma symptoms in children. Given that improved filtration provided by home-CAS reduces exposures, an associated health benefit is expected, however there is limited research in this area.
Limit infiltration from outdoors
Limit indoor air pollution
Clean indoor air (existing central air, HEPA, electrostatic precipitator)
Home Clean Air Shelter: Effective?
Reduces indoor particulate matter
Limited evidence of reduction in respiratory symptoms & cardiovascular health
Air cleaner
Presenter
Presentation Notes
The evidence supports the use of home-CASs in reducing indoor particulate matter concentrations during wildfire smoke events. In the absence of HEPA filtration or EP, increased filtration may be achieved by using a higher efficiency filter within existing air systems or even by running air systems with standard filtration, provided that they are on recirculation mode. There is limited published research demonstrating that HEPA filters and EPs improve health outcomes during wildfire events. The evidence is suggestive of improved markers of cardiac effects in adults and reduced asthma symptoms in children. Given that improved filtration provided by home-CAS reduces exposures, an associated health benefit is expected, however there is limited research in this area.
Limit infiltration from outdoors
Limit indoor air pollution
Clean indoor air: existing or augmented
Community Clean Air Shelter
No Specific Evidence for CCAS:
Similar effects as home clean air shelter depending on level of air cleaning
Air cleaner
Presenter
Presentation Notes
The evidence supports the use of home-CASs in reducing indoor particulate matter concentrations during wildfire smoke events. In the absence of HEPA filtration or EP, increased filtration may be achieved by using a higher efficiency filter within existing air systems or even by running air systems with standard filtration, provided that they are on recirculation mode. There is limited published research demonstrating that HEPA filters and EPs improve health outcomes during wildfire events. The evidence is suggestive of improved markers of cardiac effects in adults and reduced asthma symptoms in children. Given that improved filtration provided by home-CAS reduces exposures, an associated health benefit is expected, however there is limited research in this area.
Effective only if people seek cleaner air
Canceling outdoor events
No evaluation studies
Consider other options:
- Modified event
- Informed participation
Presenter
Presentation Notes
The evidence supports the use of home-CASs in reducing indoor particulate matter concentrations during wildfire smoke events. In the absence of HEPA filtration or EP, increased filtration may be achieved by using a higher efficiency filter within existing air systems or even by running air systems with standard filtration, provided that they are on recirculation mode. There is limited published research demonstrating that HEPA filters and EPs improve health outcomes during wildfire events. The evidence is suggestive of improved markers of cardiac effects in adults and reduced asthma symptoms in children. Given that improved filtration provided by home-CAS reduces exposures, an associated health benefit is expected, however there is limited research in this area.
Widely available and inexpensive
Must be fit tested & trained
N95 Respirator (Mask)
Presenter
Presentation Notes
There are few studies that evaluate the effectiveness of staying indoors at reducing adverse health effects of wildfire smoke. The existing evidence suggests that staying indoors reduces asthma symptoms in children, but the effectiveness in other populations has barely been studied. If good quality indoor air is achieved, then staying indoors even part of the time is likely to provide some benefit for everyone. The benefits of staying indoors must be weighed against potential harms such as disruption of normal activities and associated health, social and economic costs.
There are few studies that evaluate the effectiveness of staying indoors at reducing adverse health effects of wildfire smoke. The existing evidence suggests that staying indoors reduces asthma symptoms in children, but the effectiveness in other populations has barely been studied. If good quality indoor air is achieved, then staying indoors even part of the time is likely to provide some benefit for everyone. The benefits of staying indoors must be weighed against potential harms such as disruption of normal activities and associated health, social and economic costs.
Each box is a piece of information used by decision makers The evidence reviews will inform what goes each the box (only partially included here for demonstration purposes) Surveillance informs population health response and smoke characteristics Knowledge of preparedness delineates available and best potential options
Summary
• Number of interventions
• Challenge is deciding appropriate interventions for the situation