Embed Size (px)
Citation preview

EHR Stakeholder Workshop:
Toward New Interaction Models
Two Illustrative Instances and a Suggested Framework
“What’s right is what’s left when you’ve done everything else wrong.” – Robin Williams
“For every 25% increase in complexity, there is a 100% increase in effort” – Scott Woodfield
Charles N Mead, MD, MScChief Technology OfficerNational Cancer InstituteWashington, DC (USA)
Senior AssociateGlobal Health GroupBooz Allen Hamilton

2
Example 1: The caBIG™ Program: “Connecting the cancer community…from bedside to bench and back.”
Now in 4th year: will release ‘first version of a product’ Feb 1, 2008
Connecting cancer researchers (basic science) and clinical trialists (clinicians) across
– 60+ cancer centers
– Multiple ‘cooperative groups’ (e.g. Centers of Excellence)
– Multiple vendors
Initially focused on static data exchange at a computational semantic interoperable level
– Top-down governance
– Bottom-up input
– Standards-based application development

3
Example 1: The caBIG™ Program: Some Lessons Learned
Computable Semantic Interoperability is hard but achievable
In addition to the software engineering concerns, CSI must be based on
– Human Semantic Interoperability
• the BRIDG Model (and its siblings)
• Centralized vocabulary management
– Organizational Semantic Interoperability
• Data sharing and Intellectual Property in the clinical research setting
• Learning to collaborate in a competitive environment
• The “Common Cause” philosophy
– Motivators of change: conflicts-of-interest vs conflicts-of-conscience

4
Example 1: The caBIG™ Program: Some Lessons Learned
Stepwise (iterative/incremental) approaches are essential
Connecting the ‘bench’ to the ‘clinical research’ domain was the first step
Connecting to the clinical care community is the next step
Pilot program in breast cancer enabling ‘single source’ EHR/CRF data entry now under consideration
– Robust IT infrastructure (e.g. HL7 RIM, V3 data types, standardized terminologies, run-time wizards to prompt clinicians for appropriate data to satisfy CRF in the context of clinical care

5
Example 2: The Health Service Specification Project (HSSP)
Joint effort by HL7 EHR Technical Committee (EHR TC) and the Object Management Group (OMG)
– HL7 responsibility: produce semantically robust service specifications
• Driven by business cases
• Manifest as Interface specifications (implementation-independent) bound to “semantic signafiers” (e.g. BRIDG Model, terminologies, etc.)
– OMG responsibility: manage an RFP process that results in the implementation of the specified service
Overall goal is to produce a set of standardized services that can be deployed by multiple vendors across the life sciences/clinical research/clinical care continuum
E.G. Clinical Research Filtered Query (CRFQ) service

6
CRFQ and its clients…
P4
I/E criteria
P2
I/E criteria
P1
I/E criteria
I/E criteria
P3
List Qualified Protocol Interface
CRFQ
CRFQ client(clinician,caregiver,
patient Clinical data set
Qualified protocols
P1
Pt data
P2
Pt dataP4
Pt data
P3
Pt data
List Qualified Patients Interface
CRFQ
CRFQ client(trial sponsor,
CRO,Pharma) Protocol
I/E criteria/
Safety criteria
Qualified patients

7
An Exemplar Scenario…
A Trial Sponsor has developed a new intervention for Type I diabetes and has developed a clinical trial protocol to test this new intervention. A repository containing the Electronic Health Records (EHRs) for a number of patients is available to the Sponsor as a possible source of subjects for the protocol. The Trial Sponsor would like to compare the protocol’s inclusion/exclusion (I/E) criteria against patient-specific data in the EHR repository to see how many patients could be potentially eligible to participate in the intervention study.

8
This should be easy except for issues of…
Security and Access to EHR repository
Consent of individual patient (not necessarily the same as the previous point)
Non-standard expression of I/E criteria
Non-standard expression of patient-specific data

9
And those were just the ‘easy’ limitations. Also there are… Many additional steps involved in ‘recruiting a subject for a trial’ including
More finely granulated analysis of data (beyond I/E criteria)
– Lack of standards for automating this analysis, i.e. every recruitment is a one-off process
Multitude of regulatory hurdles to cross
– Local/State/regional
– National/International
Multiple stakeholders (with multiple value propositions) working from within multiple systems. For each system involved:
– Who mandates a system?
– Who pays for a system?
– Who uses (primary and secondary) the system?
– Who builds the system?
– Who regulates the system?
Differing levels of organization maturity

10
Complexity “Complicated”, “Multi-faceted”, “Multi-factorial”, “Multi-layered”
Ivar Jacobson (paraphrase): “A multi-leveled, vertically hierarchical organization whose products of value are produced through one or more horizontal processes that cross vertical organizational lines.”
With cross-organization processes – whether they involve people or systems –syntactic and semantic problems occur at the vertical boundaries.
Cumulative experience in industry, art, and (cognitive) science has repeatedly shown that the best way to deal with complexity is through abstraction, layering, and the use of standards.

11
The Communication Pyramid
Communication
`Free-text Documents
Structured Documents
ad hoc Drawings
Non-standard Graphics
Discussions
Standardized Models (UML)
Probl
em S
pace
Solution Space
Impl
emen
tatio
n-In
depe
nden
t
Implem
entation-Specific
Ab
stra
ctio
n

12
“Protocol” – a ‘commonly used’ term…
Source: John Speakman
Symbol“Protocol”
“We need to sign off on the protocol by Friday”
Concept 1
Thing 1(Document)
“Protocol XYZ has enrolled 73 patients”
Concept 2
Thing 2(Study)
“Per the protocol, you must be at least
18 to be enrolled”
Concept 3Thing 3(Plan) Ogden/Richards
(Mead/Speakman)

13
A New Interaction Model
What is “An Interaction Model”?
Candidate definition (CNM): A formal representation of a a set of activities and deliverables that occur as the result of one or more participating entities requesting or responding to well-defined events in a control flow. A given interaction has well-defined
– pre- and post-conditions
– Inputs and outputs
If this sounds like empiric process and/or software engineering, it is…
– …but only because software engineering addresses complexity management in situations of equivalent complexity to the proposed goals of this conference
Best represented in visual diagrams augmented by text (rather than the inverse)

14
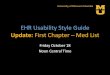
ad Activ ity Diagram - Load Labs In CDMS
CRA PSC caXchange Router/Transformer caXchange Persistence (CTOM db) C3PR Hospital Infor. Sys/Lab Infor Sys C3D
Relevant Labs Available in CDMS
STORYBOARD: CRA looks at the schedule of a given patient on a study for a specific visit. She identifies all the lab tests that should have been scheduled/ completed for that visit. CRA would need all the lab values in a given timeframe that would fall within the timeframe of the visit. CRA then reviews the lab tests/values and identifies which ones are relevant to be loaded into the CTMS (for example, a diabetic pt may have also had a A1C – inthis case, this values would not be stored in the CTMS)
CRA request s Patient
schedule for a specific viisit on
a study
«datastore»
PSC db
Retrieves patientschedule and list of activ ities that were
scheduled for that lastv isit date
CRA recieves
list of activities
Rev iews list and identifieslab tests
Requests all lab results recorded for
this patient between last visit
and today
Routes requests to datastore «datastore»
CTOM db
Retrieves all lab resultsbased on parameters
Routes lab results to CRA
CRA recieves all lab results for that
patient
Rev iews lab results andidentifies ones relevant to
load in CDMS
Routes selected lab results to C3D
«datastore»
C3D db
provides subject id, study id, lab test date, lab test id, lab result, uom high range, low range
«datastore»
Lab System db
Routes requests to CTOM db
Pass data elements - pt. id, study id, last visit date
Pass list of all activities (will these be activity names?)
«datastore»
C3PR db
send lab test id, lab results, UOM, LLN, HLN, (from C3PR - study id, study name, inv id, inv name and GRID id)
Pass pt. id, study id, last visit date, today's date
CRA intiates request
Is this Lab resultrelevant to theStudy?
Discard labs
Extract patient lab data onperiodic basis
Query db based on patientidentifier
Transform data into v3
Retrieve Study relatedinformation for the subjectPersists Lab domain data
into the db
pass patient id (MRN)
send lab test id, lab results, UOM, LLN, HLN,etc.
This is all the lab data for a patient,regardless of whether the patient is enrolledto a study or not)
C3PR provides study id, study name, investigator id and investigator name to which the subject is enrolled
No
Yes
Use Case 2 – Load Lab Data
A Formal Representation of an Interaction

15
A New Interaction Model: Critical Components
Identify stakeholders by role
– Capability, Capacity, Competency
– Stakeholders can be systems, organizations, or persons
– Many-to-many relationships are common
– Five ‘types’ of stakeholders, multiple instances of each type
Apply ongoing risk management strategies
– Static identification on a regular (e.g. weekly) basis
– Integration of risk mitigation strategies into project planning
Proceed iteratively and incrementally
– Apply project management Best Practices and avoid the Waterfall
• RUP
• Agile
• Scrum
• Etc.

16
Summary The problem we are trying is the embodiment of a (hyper) complex system apply the
appropriate tools, techniques, expertise, etc.
– “You can’t build a skyscraper by nailing together doghouses.”
The problem will not be solved ‘bottom up’ – a meaningful solution will require top-down mandates to focus bottom-up and middle-out efforts – they will not succeed on their own
Success will only occur iterative and incrementally – any attempt to solve this problem with Waterfall approaches is doomed to failure
Think architecture: business first, technology second
Success in a layered, I/I approach involves
– Continuous risk identification and management
– Multi-disciplinary teams
• Identification of discipline-specific value propositions for all stakeholders
– Prioritization of project goals and realistic expectation settting
The is a hard problem, but it is a solvable one if approached correctly

QUESTIONS & ANSWERS

18
Cumulative experience in industry, art, and (cognitive) science has repeatedly shown that the best way to deal with complexity is iteratively, using abstraction and layering
Complex problems require the application of complex cognitive processes in order to achieve meaningful solutions
Cognitive processes must apply layering and chunking (“the law of 7 +- 2”)
All disciplines that routinely deal with complex problems develop either formal or de facto approaches to Layering and Chunking
– Cyclical application of core process of definition, discovery, intervention, (re)evaluation (re-definition) “iterative/incremental process”
The Nursing Process as a model of complex problem solving
http://www.chambers.com.au/glossary/chunk.htm
Nursing Process
Assessment
Nursing DiagnosisEvaluation
Implementation Planning
ADPIE
Nursing Process
Assessment
Nursing DiagnosisEvaluation
Implementation Planning
ADPIE

19
Organizational Maturity
Level 1: Heroism and Passion (no defined process)
Level 2: A Set of Directions (minimal ability to deal with unexpected)
Level 3: A Map (unexpected events can be managed)
Level 4: Gathering Process Variance (parallel process improvement)
Level 5: Using Process Variance data to drive Process Improvement
Everyone wants to be Level 5
Progression to the ‘next level’ is stepwise
Level 1 does not mean incompetence! It just doesn’t scale well over time

20
Complexity
“Complicated”, “Multi-faceted”, “Multi-factorial”, “Multi-layered”
Ivar Jacobson (paraphrase): “A multi-leveled, vertically hierarchical organization whose products of value are produced through one or more horizontal processes that cross vertical organizational lines.”