Embed Size (px)
Citation preview

REVIEW
Novel devices
Percutaneous edge-to-edge MitraClip therapyin the management of mitral regurgitationJason H. Rogers1* and Olaf Franzen2
1Division of Cardiovascular Medicine, Davis Medical Center, University of California, Sacramento CA, USA; and 2University Heart Center, Rigshospitalet, Copenhagen, Denmark
Received 28 February 2011; accepted 11 March 2011; online publish-ahead-of-print 23 May 2011
MitraClip therapy consists of percutaneous edge-to-edge coaptation of the mitral leaflets that is analogous to the surgical Alfieritechnique. The safety profile of the MitraClip device is favourable, and survival outcomes in high-surgical-risk patients are superiorto historical controls. However, questions remain regarding long-term efficacy and durability. In the USA, the MitraClip device hasbeen studied in a safety and feasibility trial, a randomized pivotal trial against surgical mitral valve repair, and a non-randomizedhigh-risk registry. In addition, the MitraClip now has over 2 years of CE-mark approval and a rapidly expanding clinical experiencein Europe, primarily in patients at high risk for surgery. A dedicated multidisciplinary team is necessary, as well as thoughtful patientselection, familiarity with the technical aspects of the procedure including transesophageal ultrasound imaging and post-procedure moni-toring. Currently available clinical data are herein reviewed, with emphasis on the current role of MitraClip therapy in relation to exist-ing surgical techniques. Since the MitraClip procedure is still relatively new, continued investigation is required to further define patientpopulations that will benefit most.- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Mitral regurgitation † Percutaneous valve therapies † MitraClip
IntroductionMitraClip therapy is a new percutaneous approach for treatingmitral regurgitation (MR) which involves mechanicaledge-to-edge coaptation of the mitral leaflets that is analogousto the surgical Alfieri technique.1 In the USA, the MitraClipdevice has been studied in a safety and feasibility trial, a random-ized pivotal trial against surgical mitral valve repair, and a non-randomized high-risk registry (HRR). In addition, the MitraClipnow has over 2 years of CE-mark approval and a rapidlyexpanding clinical experience in Europe. Our understanding ofpatient selection, technical approaches, and integration withexisting therapies for MR has advanced considerably since thefirst human use of this device.2
We herein review clinical results of MitraClip therapy, anddiscuss the evolving role of MitraClip in the management ofpatients with clinically significant MR. It has been shown thatMitraClip therapy can be delivered safely with low morbidity,and can reduce MR in a broad spectrum of pathologies.
Mitral regurgitation prevalence,aetiology, and clinical backgroundMitral regurgitation is one of the most commonly encounteredvalvular lesions, with at least moderate regurgitation present in6.4% of the general population ≥65 years.3 Moderate–severeMR is present in 15–30% of patients with congestive heartfailure and up to 12% of patients within 1 month after myocardialinfarction. Mitral regurgitation severity has been positively corre-lated with the subsequent development of heart failure anddeath.4 –6 It is estimated that as many as 500 000 people inNorth America alone have clinically significant congestive heartfailure-associated or functional mitral regurgitation (FMR), manyof whom are currently not offered mitral valve intervention. InEurope, it is estimated that in individuals aged 55, almost one inthree will develop heart failure during their remaining lifespan.7
Since even asymptomatic patients with severe MR have higher5-year rates of death, heart, failure and atrial fibrillation, consider-ation of valve repair is clinically warranted in these patients. Until
* Corresponding author. Tel: +1 916 734 3764, Fax: +1 916 734 8394, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2011. For permissions please email: [email protected]
European Heart Journal (2011) 32, 2350–2357doi:10.1093/eurheartj/ehr101
at Hospital Severo O
choa on June 2, 2012http://eurheartj.oxfordjournals.org/
Dow
nloaded from

the advent of the percutaneous MitraClip procedure, surgicalmitral valve repair or replacement had been the sole option fortreating MR, and while this is efficacious, many patients withco-morbidities and high-surgical risk do not undergo surgerybecause of a failure to refer and perceived excessive morbidityand mortality.8,9
The anatomic aetiologies of MR are multiple and have been pre-viously described by Carpentier, Barlow, and others.10–12 Theseinclude degenerative pathologies in which the leaflets or chordaeare structurally ‘degenerated’, such as in fibroelastic deficiencywith leaflet prolapse, myxomatous leaflet degeneration, orBarlow’s disease with diffuse excess tissue and chordal elongation.In degenerative MR, the 10-year natural history of severe MR dueto a flail posterior leaflet has been documented, with 90% ofpatients either expiring or requiring an MV operation.13 SurgicalMV repair has been the preferred treatment for clinically significantdegenerative MR, and generally affords improved post-operativeoutcomes and survival when compared with MV replacement.14
Surgical intervention for degenerative MR consists of multiple tech-niques including leaflet repair with resection, chordal transfer, useof polytetrafluoroethylene neochordae, and prosthetic ring orband annuloplasty.15 These approaches are efficacious and resultin excellent freedom from reoperation.16 Edge-to-edge surgicalrepair of the mitral valve with annuloplasty (or without annulo-plasty in selected patients) has also been shown to afford favour-able outcomes in patients with degenerative or FMR.17,18.
Functional mitral regurgitation is a direct consequence of under-lying left ventricular dysfunction and annular dilation which secon-darily impairs the coaptation of otherwise structurally normalleaflets. Surgical correction of FMR has been shown to improvefunctional class and left ventricular remodelling,19 but a survivalbenefit has yet to be shown.20 Additionally, even with current sur-gical annuloplasty techniques, up to 35% of treated patients havemoderate or greater MR recur within 1 year of surgery.21– 23 Pre-operative predictors of recurrent MR and poor outcomes afterrestrictive annuloplasty for FMR include LV end-diastolic diameter.65 mm,24 posterior leaflet angle ≥458,25 and MV coaptationdepth ≥11 mm.26 Since surgical FMR repair in patients with lowejection fraction is associated with significant recurrence rates,morbidity, and mortality outside of select centres of excellence,surgery for isolated FMR is not routinely offered despite thedemonstrated improvements in quality of life.
Current ACC/AHA and ESCguidelines for correctionof mitral regurgitationThe current 2008 American College of Cardiology/AmericanHeart Association (ACC/AHA) and 2007 European Society of Car-diology (ESC) Guidelines for the Management of Valvular HeartDisease make no specific statements related to appropriatepatient selection and timing for application of MitraCliptherapy.27,28 The 2008 ACC/AHA guidelines describe threetypes of MV operations: (i) MV repair; (ii) MV replacement withchordal preservation; and (iii) MV replacement with removal ofthe mitral apparatus. The ACC/AHA guidelines support MV
surgery for patients with severe (3–4+) MR who are symptomaticwith preserved LV size and function, asymptomatic with LV dys-function or increased LV size, who have recent onset atrial fibrilla-tion or evidence of pulmonary hypertension, or in symptomaticpatients with severe LV dysfunction (LVEF ,30%) despiteoptimal medical therapy. The guidelines address the fact thatoverall mortality from MV surgery for patients older than 75 canbe significant, especially when combined with CABG, with operat-ive mortality exceeding 14%.29 This constitutes an unmet clinicalneed and potential target for MitraClip therapy. The 2007 ESCguidelines mention percutaneous edge-to-edge repair but statethat ‘further evaluation is needed’ before the specific role of thistechnique can be established. This likely refers to the importanceof having robust safety, efficacy, and durability data for newpercutaneous approaches.
The MitraClip systemMitraClip therapy is based on the surgical edge-to-edge repair firstdescribed by Alfieri.1 The surgical technique involves the use ofsuture to convert a regurgitant mitral orifice into a competentdouble orifice valve with decreased or eliminated regurgitation.The MitraClip device, which was designed to mimic anedge-to-edge repair, consists of a percutaneously delivered MRI-compatible cobalt chromium implant with two arms and two grip-pers which are used to grasp the opposing free edges of theanterior and posterior leaflet in order to improve leaflet coapta-tion and generate a double-orifice valve. Each arm is 4 mm wideand 8 mm long, and the device is covered in a polyester fabricto promote tissue in-growth. Complete encapsulation of thedevice occurs by 12 weeks in a porcine model.30 The device isdelivered by a transseptal route using a steerable guide catheter(24 Fr proximally and 22 Fr at the interatrial septum), throughwhich the steerable clip delivery system with the MitraClipattached at the distal end is delivered. The MitraClip is steeredand advanced under echocardiographic and fluoroscopic guidanceinto the left ventricle at the point of regurgitation, and withdrawnwith the arms opened to allow capture of both leaflets with thegrippers and arms. Once adequate leaflet insertion is confirmed,the MitraClip can then be tightened to assess efficacy. If thedesired result is achieved, the MitraClip is deployed and releasedfrom the catheter. If the grasp is felt to be suboptimal, the leafletscan be released and the grasping procedure can be repeated(Figure 1). Although no more than two MitraClips could beimplanted per patient in the US feasibility and pivotal trials, up tofour MitraClips have been implanted in a single patient inEurope. The only limitation to the number of MitraClips implantedfrom a safety standpoint appears to be the development of mitralstenosis.
The procedure is performed in the catheterization laboratoryunder general anaesthesia for patient comfort (due to use ofTEE during the procedure), but more importantly to eliminatepatient movement and to perform controlled breath-holdingduring the MitraClip grasping step, thereby allowing accurate place-ment and controlled leaflet insertion. However, as the technique isrefined, it may be possible that in selected patients the procedurecould be performed using conscious sedation.31 The MitraClip
Percutaneous edge-to-edge MitraClip therapy 2351
at Hospital Severo O
choa on June 2, 2012http://eurheartj.oxfordjournals.org/
Dow
nloaded from

procedure requires a multidisciplinary team in the catheterizationlaboratory, including 1–2 interventional cardiologists, an echocar-diographer, and an anaesthesiologist. Although the morbidity ofthe procedure is less than MV surgery, MitraClip resource utiliz-ation remains significant and is similar to surgical mitral valverepair in terms of reported procedure length and number ofphysicians involved (Table 1).
The MitraClip has been applied to a wide spectrum of degen-erative (anterior, posterior, and bileaflet prolapse) and functionalregurgitant pathologies. The presence of active endocarditis,rheumatic valve disease, and mitral stenosis are contraindicationsto MitraClip therapy. Regardless of regurgitation aetiology, thefinal common pathway of MitraClip implantation is the gener-ation of a double-orifice valve. The MitraClip is analogous tosurgical suture, and can be used to approximate leaflets atdifferent locations along the leaflet coaptation surface(Figure 2). For wide regurgitant orifices, more than one clipmight be needed. Treating MR at the medial and lateral commis-sures requires care as the ability to manoeuvre the MitraClip inthe left ventricle is limited. Given the complex structure of thesubcommissural chordae a higher risk of clip entanglement canbe expected. Treatment of para-commissural jets is nonethelessfeasible.
MitraClip therapy is highly compatible with other minimally inva-sive procedures that are often applied to patients with MR. Forexample, access to the left atrium is not restricted for atrial fibrilla-tion ablation procedures, and access to the coronary sinus is pre-served for biventricular lead ICD placement or for future coronarysinus mitral annuloplasty devices. Biventricular pacing and cardiacresynchronization therapy is an important treatment for patientswith ischaemic cardiomyopathy and can reduce FMR acutely andchronically in selected patients. Greater than one-half of respon-ders to CRT have sustained reductions in MR by at least onegrade for 6 months or longer.32
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Resource utilization, MitraClip procedure vs.surgical mitral valve repair
MitraClipprocedure
Surgical mitralvalve repair
Condition treated Mitral regurgitation Mitral regurgitation
Implant Yes Yes
General anaesthesia Yes Yes
TEE guidance Yes Yes
Overall procedure time 2–4 h 2–4 h
ICU 24 h 24 h
Post-procedure LOS 3 4–7
MD’s required (includingAnaesthesiologists)
3 3
Operating room staff 3–4 3–4
Procedure location Cath lab/hybrid OR/hybrid
LOS, length of stay.
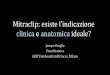
Figure 1 The MitraClip System and Procedure. (A) The MitraClip delivery system consists of a guiding catheter and nested delivery catheterwhich can be steered in multiple planes with control knobs. (B) The MitraClip attached to the clip delivery system. The leaflets are graspedbetween the two clip arms (covered with Dacron) and two gripper elements. (C) 3D TEE view showing the MitraClip delivery systemacross the interatrial septum with the clip in the left atrium. (D) The MitraClip is oriented perpendicular to the coaptation plane of themitral valve. (E) Final appearance of the MitraClip in place at the A2/P2 interface with generation of a double orifice valve.
J.H. Rogers and O. Franzen2352
at Hospital Severo O
choa on June 2, 2012http://eurheartj.oxfordjournals.org/
Dow
nloaded from

Current registry and randomizedtrial data
EVEREST trialsThe key results of currently published North American and Euro-pean clinical experience with the MitraClip are shown in Table 2.Feldman et al.33 published results from 55 patients treated in theEVEREST (Endovascular Valve Edge-to-Edge Repair STudy) PhaseI feasibility trial, and 52 patients treated in the pre-randomizationstart-up experience (roll-in phase) of the EVEREST II pivotal trial.These data represent the early North American experience withthe MitraClip device, with 70% of these procedures being thefirst, second, or third procedures at each respective site. Patientswere selected if they were candidates for MV surgery, metmajor ACC/AHA indications for MV surgery, and had specific ana-tomic criteria including a primary central regurgitant jet associatedwith the A2/P2 segments, a coaptation length ≥2 mm, a coaptationdepth ≤11 mm, a flail gap ,10 mm, and a flail width ,15 mm. Keyexclusion criteria included LVEF ≤25%, LV end-systolic dimension.55 mm, mitral valve orifice area ,4 cm2, or recent myocardialinfarction. These EVEREST-specific clinical and anatomic criteriawere used for all North American trial and registry data, buthave not been consistently applied in the European experience.Of the 107 patients who underwent the MitraClip procedure inthis early US experience, 70 (74%) achieved acute proceduralsuccess (APS), defined as a post-procedure reduction in MR to
≤2+. Of subjects who did not achieve APS, 17 (16%) had Mitra-Clip implantation with acute MR grade .2+, and 11 (10%) had noMitraClip implanted with post-procedure MR .2+. At 12 months,not including crossover to surgery, 50 of 76 APS patients (66%)had echocardiographic follow-up and continued with MR ≤2+.A total of 32 patients underwent MV surgery after a clip pro-cedure, and when repair was planned, 84% were successfullyrepaired, demonstrating that MV repair is feasible after prior Mitra-Clip attempt or implantation. Freedom from death at up to 3-yearfollow-up was 90.1%, and freedom from surgery was 76.3%. Themajority of patients included had degenerative MR (79%), butpatients with FMR (21%) had similar acute results and durability.
An important feature of the EVEREST data is that an indepen-dent echocardiographic core laboratory assessed all echocardio-grams. Mitral regurgitation was graded strictly according toAmerican Society of Echocardiography guidelines using a compo-site of colour flow Doppler of the regurgitant jet area, pulmonaryvein flow, regurgitant volume, and regurgitant fraction. Interobser-ver variability was low using this methodology, with 84% concor-dance in regard to MR severity. This analysis of echocardiogramspre- and post-percutaneous or surgical MV therapy differs fromthe majority of prior surgical repair studies which have not usedquantitative echocardiographic methods or core laboratories. Ana-lyses of echocardiograms from enrolling EVEREST sites demon-strated that without the use of quantitative methodologybaseline MR grade is often overestimated by using qualitativemethods.34
Figure 2 Spectrum of pathologies treatable with the MitraClip. The top panel illustrates the various aetiologies of MR that can be managedwith MitraClip therapy. Note how the MitraClip can be positioned at different approach angles to match leaflet anatomy. Carpentier Type I,normal leaflet motion with annular dilation; Type II, increased leaflet motion (leaflet prolapse or flail); Type IIIb, restricted leaflet motion insystole, seen in ischaemic cardiomyopathy. Lower panel illustrates the final common pathway for MitraClip therapy, which consists of generatinga double-orifice valve. One or more MitraClips can be placed (A and B). For lateral or commissural jets, a MitraClip can be placed in the para-commissural region with a resultant single orifice (C).
Percutaneous edge-to-edge MitraClip therapy 2353
at Hospital Severo O
choa on June 2, 2012http://eurheartj.oxfordjournals.org/
Dow
nloaded from

The landmark prospective, randomized EVEREST II trial is thefirst randomized trial of a percutaneous mitral repair devicemeasured against conventional surgical therapy; it also representsthe first echocardiographic core-laboratory adjudicated follow-upafter surgical mitral valve repair.35 This trial randomized 279patients with 3–4+ MR prospectively to receive either devicetherapy with the MitraClip device (n ¼ 184) or conventional surgi-cal repair or replacement (n ¼ 95) in a 2:1 ratio. The primarysafety endpoint was the major adverse event rate (MAE) at 30days, and the primary efficacy endpoint was defined as 12 monthfreedom from the combined outcome of death, new surgery formitral valve dysfunction, or the occurrence of .2 + MR. Pre-specified MAEs were death, major stroke, reoperation of mitralvalve, urgent/emergent CV surgery, myocardial infarction, renalfailure, deep wound infection, ventilation .48 h, new onset per-manent atrial fibrillation, septicaemia, GI complication requiringsurgery, or transfusion ≥2 units. The intention-to-treat 30-dayMAE rate was lower in the MitraClip group when comparedwith the surgery group (15 vs. 48%, superiority P , 0.001). TheMAE difference was driven largely by transfusion requirements inthe surgical arm; however, in response to this critique, a modifiedMAE analysis which defined major bleeding as transfusion ≥4 unitsor requiring surgical intervention still demonstrated a lower MAErate in the MitraClip group (5.0 vs. 30.9%, P , 0.0001).36 Primaryclinical efficacy at 12 months by intention-to-treat was achievedin 55% of the MitraClip device patients and 73% of the surgerygroup (non-inferiority P ¼ 0.007). At 2 years of follow-up,primary clinical efficacy was preserved in 52% of the percutaneous-repair group and 66% in the surgery group (P ¼ 0.04). It is impor-tant to emphasize that the EVEREST II trial examined the safetyand efficacy of MitraClip therapy as an initial approach to the treat-ment of patients with MR. Not every procedure was successful inreducing MR, but of these failures at APS, the majority went on tohave successful subsequent mitral valve surgery. A non-prespecified analysis reported in the EVEREST II publicationshowed that in subgroups with age ≥70 years, FMR, and LVEF,60%, surgery was not superior to percutaneous treatmentwith regard to efficacy. Concomitant with the EVEREST II trial, asingle-arm ’HRR’ enrolled 78 patients with MR and an STS orsurgeon-estimated surgical procedural mortality risk of ≥12%.The HRR enrolled a higher percentage of patients with FMR, anddemonstrated superior safety compared with the estimated surgi-cal risk, as well as improved symptoms in most patients. Formalresults of the HRR have not yet been published. UntilFDA-approval is granted, in the USA the MitraClip is availableonly through the REALISM continued-access registry.
European registry dataIn March 2008, the MitraClip received CE-mark approval. Sincethen, the majority of MitraClip implants has been performed inEurope. In addition, the clinical characteristics of European patientsare different than those enrolled in the EVEREST trials, as the rela-tively limiting mitral leaflet anatomic inclusion and exclusion cri-teria were not required. The two largest reports to date on theEuropean MitraClip experience emanate from a single centre inGermany37 and two centres in Italy38 for a total of 82 patients.
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
.
Tab
le2
Co
mpa
rati
vesu
mm
ary
of
publ
ishe
dM
itra
Clip
clin
ical
tria
ls
n (pat
ient
s)E
VE
RE
ST
/no
n-E
VE
RE
ST
elig
ibili
ty
Deg
ener
ativ
e/fu
ncti
ona
lae
tio
logy
Age
,m
ean
Bas
elin
eL
VE
F,%
ST
Ssc
ore
/lo
gist
icE
uro
SC
OR
E,
mea
n
Bas
elin
eN
YH
AII
I/IV
,%
Fo
llow
-up
NY
HA
III/
IV,%
Mea
nM
Rgr
ade
atba
selin
e
MR
≤2
1at
follo
w-u
pE
cho
card
iogr
aphi
cco
rela
bora
tory
Pro
cedu
ral
mo
rtal
ity/
in-h
osp
ital
deat
h
EVER
EST
and
EVER
EST
IIR
oll-I
nR
egis
try
(USA
),Fe
ldm
anet
al.
107
100%
/0%
79%
/21%
7162
NR
/N
R46
%8%
(at
12m
onth
s)3.
374
%(d
isch
arge
)/66
%(1
2m
onth
s)Y
es0
(0%
)/1
(0.9
%)
EVER
EST
IIR
ando
miz
edT
rial
(USA
),Fe
ldm
anet
al.
184
100%
/0%
73%
/27%
6760
NR
/NR
52%
2%3.
279
%(1
2m
onth
s)Y
es0
(0%
)/2
(1%
)at
30da
ys
Ger
man
expe
rien
ceFr
anze
net
al.
5131
%/6
9%31
%/6
9%73
3616
/28
98%
33%
(at
disc
harg
e)3.
694
%(a
tdi
scha
rge)
No
0(0
%)/
0(0
%)
Italia
nex
peri
ence
Tam
buri
noet
al.
3110
0%/0
%42
%/5
8%71
4210
.3/1
4.3
87%
0%(a
t30
days
)3.
997
%(3
0da
ys)
No
0(0
%)/
NR
NR
,not
repo
rted
.
J.H. Rogers and O. Franzen2354
at Hospital Severo O
choa on June 2, 2012http://eurheartj.oxfordjournals.org/
Dow
nloaded from

German experienceFranzen et al. have reported their initial experience with theMitraClip system in patients who met current guideline criteriafor treatment of MR. Their interdisciplinary team of interventionalcardiologists and cardiac surgeons treated 51 patients with ≥3 +MR who were at high risk for mitral valve surgery based on a logis-tic EuroSCORE .20, an STS score .12, or by other clinicalfactors which the team felt conferred a high-surgical risk (i.e.prior chest radiation therapy, frailty, prior stroke, and prior ster-notomy). The exclusion criteria were relatively few and consistedof a mitral valve area (MVA) ≤2.0 cm2, active endocarditis, orextensively prolapsed or flail leaflets (prolapse width .25 mm,flail gap .20 mm).
Patients in this series had significantly worse left ventricular dys-function and more adverse valve morphology than those patientsenrolled in the EVEREST trials. Specifically, there was no lowerlimit on LVEF or upper limit on LV size, and there was a broaderspectrum of allowable leaflet anatomy and regurgitant jet location(non-central jet allowed). Of the patients undergoing MitraCliptherapy, there were 35 patients (69%) with LV or leaflet character-istics that would have excluded them from enrolment in theEVEREST trials. These were termed the ’EVEREST –’ cohort,and had a significantly higher logistic EuroSCOREs (33 vs. 18)and larger LV end-systolic volumes (124 vs. 101 mm3). The remain-ing patients were defined as ’EVEREST +’, and would have metenrolment criteria for the EVEREST trials.
MitraClip therapy was performed in 51 consecutive patientswith a mean logistic EuroSCORE of 29+22 and a Society of Thor-acic Surgeons score of 15+ 11. MitraClip implantation was suc-cessful in 49 patients (96%), with the majority of patients (34/49,69%) treated with a single clip, 14 patients (29%) receiving twoclips, and one patient receiving three clips. All 16 EVEREST +patients had successful MitraClip implantation, where as 2 of the35 EVEREST—patients did not have clips implanted. This wasdue to a 17-cm left atrium in one case, and substantial subvalvularcalcification in the other case. Procedure-related reduction in MRseverity was one grade in 16 patients (31%), two grades in 24patients (47%), and three grades in 9 patients (18%). There wasno clinically significant mitral stenosis observed after therapy,and there were no procedure-related major adverse events andno in-hospital mortality. In summary, the authors demonstratedthe feasibility and short-term efficacy of the MitraClip inhigh-surgical-risk patients, with a substantial proportion of patientstreated that would have been excluded from the EVEREST trials.Longer term outcomes from this cohort have not been reported,and therefore effects on prognosis, left ventricular remodelling,and durability of MR reduction cannot yet be assessed.
Italian experienceTamburino et al. have reported results from the initial Italian clini-cal experience with the MitraClip at two centres. Their multidisci-plinary teams selected patients who met criteria for mitralintervention based on established guidelines, and who were high-risk for surgery based on the consensus between cardiologistand cardiac surgeon, logistic EuroSCORE .20, hepatic cirrhosis,autoimmune disease, severe renal failure requiring haemodialysis,
or any contraindication to extracorporeal circulation. Anatomicleaflet criteria were similar to EVEREST criteria, with a require-ment for primarily central regurgitation (at the A2/P2 interface)and sufficient leaflet tissue for mechanical coaptation. Key exclu-sion criteria were very similar to the EVEREST trials, includingmitral valve orifice area ,4 cm2, flail width ≥15 mm, flail gap≥10 mm, coaptation depth ≥11 mm, and coaptation length,2 mm. Importantly, unlike EVEREST, there was no exclusionfor very low LV ejection fraction, nor was there an upper limiton LV size. The primary efficacy endpoint was acute devicesuccess defined as clip placement with reduction in MR to ≤2+.The primary acute safety endpoint was 30-day freedom frommajor adverse events, defined as the composite of death, myocar-dial infarction, non-elective cardiac surgery for adverse events,renal failure, transfusion of .2 units of blood, ventilation for.48 h, deep wound infection, septicaemia, and new onset atrialfibrillation.
Thirty-one patients were successfully treated using standardtechniques, with 19 patients undergoing single MitraClip implan-tation, and 12 patients having 2 clips placed. There were no unsuc-cessful attempts at MitraClip placement, and no proceduralmortality. At 30 days, there was an intra-procedural cardiac tampo-nade (treated successfully with pericardiocentesis and subsequentMitraClip implantation), and one non-cardiac death, resulting in aprimary safety endpoint of 93.6%. Acute device success wasobserved in 96.8% of patients. At 30 days, there was favourableLV remodelling seen, with reduction in the diastolic mitralannular septal-lateral dimension. Mitral valve area significantlydiminished at 30 days, but this did not result in any clinically signifi-cant mitral stenosis. In summary, the Italian registry demonstratedthe excellent acute safety and efficacy of MitraClip therapy in apopulation of patients similar to EVEREST patients but at highersurgical risk. Longer term efficacy and durability in this initialcohort has not yet been reported.
MitraClip safety and patient selectionBased on the available data from expert high-volume centres, it hasbeen demonstrated that the MitraClip can be safely and success-fully applied to a diverse patient population in terms of age, surgicalrisk, and mitral valve pathologies. These findings will need to beconfirmed in centres with more limited experience. The rate ofmajor adverse events after MitraClip placement is very low. Theanatomic leaflet criteria for MitraClip patient selection were rigor-ously defined in the EVEREST trials, but the European experiencehas shown us proof of principle that the MitraClip can be deliveredto more complex (non-EVEREST) leaflet anatomy. Althoughfurther investigation will undoubtedly refine our understanding of‘acceptable’ leaflet anatomy, the main limitations appear to bethe ability to grasp both leaflets, and the undesired developmentof mitral stenosis.
Herrmann et al.39 examined the effect of implanting one or twoMitraClips on MVA and mean transmitral gradient (MVG) in 96patients enrolled in the EVEREST studies followed for up to 24months. By planimetry the authors found that the mean MVAdecreased from 6.0+1.3 to 3.6+1.2 cm2 after clip placement,and remained unchanged after 24 months of follow-up. Therewas also a small increase in the mean MVG after clip placement
Percutaneous edge-to-edge MitraClip therapy 2355
at Hospital Severo O
choa on June 2, 2012http://eurheartj.oxfordjournals.org/
Dow
nloaded from

from 1.7+ 0.9 to 4.1+ 2.2 mmHg, which did not increase furtherafter 24 months. Although patients with FMR had a slightly smallerbaseline and follow-up MVA, there were no differences in MVA orMVG between patients who received one clip (69%) and thosereceiving two clips (31%). These data confirm that MitraCliprepair with the EVEREST inclusion criteria of a baseline MVA≥4.0 cm2 does not result in significant mitral stenosis.
MitraClip efficacy and surgery afterMitraClip therapyA concern with any new therapy is how it will compare in efficacywith existing therapies. A key issue at this point is that the longerterm durability (5–10 year) of the MitraClip procedure is not yetknown. In high-surgical-risk populations, the safety advantage of theMitraClip may partially outweigh durability concerns, although thepoint at which this balance becomes equivalent or favours surgeryis yet to be defined. For instance, a younger patient at low surgicalrisk with degenerative MR and a high likelihood of successful sur-gical repair may be more appropriately treated with surgical mitralvalve repair.
In the surgical literature (mostly dealing with degenerative repairwith leaflet resection techniques), post-operative MR.mild hasbeen shown to be a risk factor for reoperation. Suri et al.40 exam-ined the durability of mitral repair for leaflet prolapse in 1411patients. At up to 15 years of follow-up, greater than mild residualpost-operative MR prior to discharge was shown to be a multi-variate predictor for reoperation, but not for mortality. Fixet al.41 reported that those patients with 1–2+ MR by post-pumpintraoperative echocardiography had a trend towards more reo-perations than ‘echo-perfect’ patients with zero or trivial post-operative MR, but there was no difference in morbidity ormortality at up to 5-year follow-up. While less post-procedureMR is certainly desirable, these data cannot be directly extrapo-lated to the MitraClip experience, as the predictors of recurrentMR in degenerative and functional subgroups are not known.The primary endpoint of MitraClip therapy in the EVEREST trialswas post-procedure MR ≤2+. Previously published surgical litera-ture cannot answer the question of whether a patient undergoingMitraClip therapy with post-procedure 1 + MR has a inferior long-term outcome than a patient with 2+ post-procedure MR.Abstract data have shown that patients with residual MR of 1+or 2+ at 12 months following MitraClip therapy both experiencemeaningful clinical benefits in terms of LV size reduction, LVvolume reduction, and functional class improvement.42
Although the initial clinical results with the MitraClip areencouraging, there has been discussion as to the potential impor-tance of concomitant annuloplasty in edge-to-edge leaflet repair.Annuloplasty has become routine during surgical degenerativemitral valve repair, and it is also an essential component ofsurgery for FMR. Failure to perform annuloplasty at the time ofdegenerative leaflet repair (mostly with partial leaflet resectiontechniques) has been shown to adversely affect the repair dura-bility.16,43,44 The MitraClip procedure specifically mimics theAlfieri procedure in which the free edges of the A2 and P2segments are sutured together, generating a double orifice mitralvalve. In ischaemic MR, the application of edge-to-edge repair
without annuloplasty has resulted in significant rates of recurrentMR.45,46 In a series with mostly degenerative MR, Alfieri et al.1
demonstrated that freedom from reoperation was less in patientsthat did not have concomitant annuloplasty. In defence of theedge-to-edge approach without annuloplasty, Maisano et al.18
have published outcomes on a retrospective series of 29 patientswith degenerative or FMR, reporting the 5-year freedom fromrecurrent MR .2+ or reoperation as 90+ 5%. Whether or notemerging percutaneous annuloplasty procedures will be comp-lementary to the MitraClip procedure, and whether either willhave robust stand-alone or long-term efficacy remains to beshown.
A desirable feature of any percutaneous therapy for MR is thatsubsequent surgical options for MV repair are preserved if needed.Argenziano et al.47 have previously reported on the 32 patientswho underwent MV surgery after a MitraClip procedure fromthe EVEREST and EVEREST II roll-in cohort. Twenty-seven patientsunderwent the surgical procedure planned before surgery(21 repairs, 6 replacements), one patient without a known pre-procedure strategy had MV replacement, and four plannedrepairs subsequently underwent MV replacement. The overallrepair rate after the MitraClip procedure was 66%. Glower et al.have presented data from EVEREST II regarding repairability ofthe mitral valve after MitraClip placement and found that the sur-gical repair rate ≤90 days after MitraClip attempt or placementwas 52% (14 of 27 patients), and the repair rate .90 days afterMitraClip was 60% (6 of 10). The presence of anterior/bileafletflail or prolapse was a significant predictor of the need for MVreplacement. However, surgeon experience, defined as thenumber of surgeries performed annually, duration of implant, oran operative note of valve injury or difficulty removing thedevice did not have an impact on whether a repair or replacementwas performed.48 Geidel et al.49 have reported that mitral valvepathology can be aggravated by MitraClip implantation, butcomplex successful mitral valve repair was still achieved. Rogerset al.50 reported a series of four patients who underwent success-ful surgical MV repair up to 5 years and 2 months after MitraClipdevice implantation, demonstrating that very late MV repairremains possible, including after implantation of two clips. Otherthan for degenerative MR, it is debatable whether mitral valverepair after a failed MitraClip procedure in ischaemic MR shouldbe attempted. Magne et al.51 did not find a mortality differencebetween repair vs. replacement in patients with ischaemic MR6 years after surgery.
Conclusion and future directionsThe MitraClip procedure is rapidly evolving as an important optionamong the current therapies for MR. The safety profile of thisdevice appears to be excellent. Acute outcomes are favourable,and for those patients with APS, mid-term durability (up to2years) is reasonable. Although surgical risk calculators may over-estimate morbidity and mortality in high-risk patients with MRundergoing surgery, early survival outcomes with MitraCliptherapy in these high-surgical-risk patients have been superior tohistorical controls. There is no question that surgical mitral valverepair for degenerative MR has been shown to be highly effective
J.H. Rogers and O. Franzen2356
at Hospital Severo O
choa on June 2, 2012http://eurheartj.oxfordjournals.org/
Dow
nloaded from

in multiple large series, resulting in a 10-year freedom from reo-peration of up to 97%.52 Minimally invasive degenerative surgicalmitral valve repair has also been shown in expert hands to haveexcellent efficacy and durability, with a 5-year freedom from thecardiac reoperation rate of 95.6%.53 Surgical repair options havematured over time and are numerous, including leaflet repairwith resection, chordal transfer, use of polytetrafluoroethyleneneochordae, and prosthetic ring or band annuloplasty. However,we are still early in the MitraClip experience, and unansweredquestions remain regarding long-term efficacy, adoption, andapproval indications. Based on adoption patterns in Europe, andsubgroup analyses from the EVEREST II trial, it would appearthat patients who are older, at higher risk for surgical therapy,or with FMR and depressed ejection fractions will constitute theinitial target population for MitraClip therapy. Since FMR is primar-ily a ventricular problem, it remains to be seen whether a leafletintervention will have durable efficacy. Numerous predictors ofrecurrent MR after restrictive annuloplasty for FMR have beenidentified and their relevance to determining patient selectionfor MitraClip therapy is yet to be determined.24 –26 Whether ornot the MitraClip should be translated for use in lower risk patientswith degenerative valve disease is a matter of debate, but clearlythe surgical bar has been set quite high in these patients.
While some MitraClip cases are straightforward, many cases canbe technically challenging, comparable with complex percutaneousaortic valve replacement, multivessel stenting or chronic totalocclusion interventions. Future MitraClip and delivery systemdesigns may allow a wider range of valve anatomies to betreated, and may simplify leaflet insertion and grasping. In addition,innovations in echocardiographic and intracardiac imaging willincreasingly revolutionize this and other structural heart pro-cedures. For instance, 3D TEE was not widely available at theoutset of the MitraClip experience but has now become standardduring the procedure, markedly improving the ease and visualiza-tion of the procedure.
The MitraClip procedure is a promising new therapy, but newways must continue to be found to refine its application and estab-lish ever more meaningful clinical indications for its use. Like all firstgeneration techniques, the MitraClip will evolve and change in thefuture.
Conflict of interest: none declared.
References1. Alfieri O, Maisano F, De Bonis M, Stefano PL, Torracca L, Oppizzi M, La Canna G.
The double-orifice technique in mitral valve repair: a simple solution for complexproblems. J Thorac Cardiovasc Surg 2001;122:674–681.
2. Condado JA, Acquatella H, Rodriguez L, Whitlow P, Velez-Gimo M, St Goar FG.Percutaneous edge-to-edge mitral valve repair: 2-year follow-up in the firsthuman case. Catheter Cardiovasc Interv 2006;67:323–325.
3. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M.Burden of valvular heart diseases: a population-based study. Lancet 2006;368:1005–1011.
4. Bursi F, Enriquez-Sarano M, Nkomo VT, Jacobsen SJ, Weston SA, Meverden RA,Roger VL. Heart failure and death after myocardial infarction in the community:the emerging role of mitral regurgitation. Circulation 2005;111:295–301.
5. Robbins JD, Maniar PB, Cotts W, Parker MA, Bonow RO, Gheorghiade M. Preva-lence and severity of mitral regurgitation in chronic systolic heart failure. Am JCardiol 2003;91:360–362.
6. Trichon BH, Felker GM, Shaw LK, Cabell CH, O’Connor CM. Relation of fre-quency and severity of mitral regurgitation to survival among patients with leftventricular systolic dysfunction and heart failure. Am J Cardiol 2003;91:538–543.
7. Bleumink GS, Knetsch AM, Sturkenboom MC, Straus SM, Hofman A, Deckers JW,Witteman JC, Stricker BH. Quantifying the heart failure epidemic: prevalence,incidence rate, lifetime risk and prognosis of heart failure The RotterdamStudy. Eur Heart J 2004;25:1614–1619.
8. Mirabel M, Iung B, Baron G, Messika-Zeitoun D, Detaint D, Vanoverschelde JL,Butchart EG, Ravaud P, Vahanian A. What are the characteristics of patientswith severe, symptomatic, mitral regurgitation who are denied surgery? EurHeart J 2007;28:1358–1365.
9. O’Brien SM, Shahian DM, Filardo G, Ferraris VA, Haan CK, Rich JB, Normand SL,DeLong ER, Shewan CM, Dokholyan RS, Peterson ED, Edwards FH, Anderson RP.The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 2—iso-lated valve surgery. Ann Thorac Surg 2009;88(Suppl. 1):S23–S42.
10. Carpentier A. Cardiac valve surgery—the “French correction”. J Thorac CardiovascSurg 1983;86:323–337.
11. Adams DH, Rosenhek R, Falk V. Degenerative mitral valve regurgitation: bestpractice revolution. Eur Heart J 2010;31:1958–1966.
12. Barlow JB, Pocock WA. The significance of late systolic murmurs and mid-late sys-tolic clicks. Md State Med J 1963;12:76–77.
13. Ling LH, Enriquez-Sarano M, Seward JB, Tajik AJ, Schaff HV, Bailey KR, Frye RL.Clinical outcome of mitral regurgitation due to flail leaflet. N Engl J Med 1996;335:1417–1423.
14. Enriquez-Sarano M, Schaff HV, Orszulak TA, Tajik AJ, Bailey KR, Frye RL. Valverepair improves the outcome of surgery for mitral regurgitation. A multivariateanalysis. Circulation 1995;91:1022–1028.
15. Seeburger J, Falk V, Borger MA, Passage J, Walther T, Doll N, Mohr FW. Chordaereplacement versus resection for repair of isolated posterior mitral leaflet pro-lapse: a egalite. Ann Thorac Surg 2009;87:1715–1720.
16. Gillinov AM, Cosgrove DM, Blackstone EH, Diaz R, Arnold JH, Lytle BW,Smedira NG, Sabik JF, McCarthy PM, Loop FD. Durability of mitral valve repairfor degenerative disease. J Thorac Cardiovasc Surg 1998;116:734–743.
17. Maisano F, Torracca L, Oppizzi M, Stefano PL, D’Addario G, La Canna G,Zogno M, Alfieri O. The edge-to-edge technique: a simplified method tocorrect mitral insufficiency. Eur J Cardiothorac Surg 1998;13:240–245; discussion245–6.
18. Maisano F, Vigano G, Blasio A, Colombo A, Calabrese C, Alfieri O. Surgical iso-lated edge-to-edge mitral valve repair without annuloplasty clinical proof of theprinciple for an endovascular approach. EuroIntervention 2006;2:181–186.
19. Bax JJ, Braun J, Somer ST, Klautz R, Holman ER, Versteegh MI, Boersma E,Schalij MJ, van der Wall EE, Dion RA. Restrictive annuloplasty and coronary revas-cularization in ischemic mitral regurgitation results in reverse left ventricularremodeling. Circulation 2004;110(Suppl. 1):II103–II108.
20. Wu AH, Aaronson KD, Bolling SF, Pagani FD, Welch K, Koelling TM. Impact ofmitral valve annuloplasty on mortality risk in patients with mitral regurgitationand left ventricular systolic dysfunction. J Am Coll Cardiol 2005;45:381–387.
21. Hung J, Papakostas L, Tahta SA, Hardy BG, Bollen BA, Duran CM, Levine RA.Mechanism of recurrent ischemic mitral regurgitation after annuloplasty: contin-ued LV remodeling as a moving target. Circulation 2004;110(Suppl. 1):II85–II90.
22. Marwick TH. Restrictive annuloplasty for ischemic mitral regurgitation: too littleor too much?. J Am Coll Cardiol 2008;51:1702–1703.
23. McGee EC, Gillinov AM, Blackstone EH, Rajeswaran J, Cohen G, Najam F,Shiota T, Sabik JF, Lytle BW, McCarthy PM, Cosgrove DM. Recurrent mitralregurgitation after annuloplasty for functional ischemic mitral regurgitation.J Thorac Cardiovasc Surg 2004;128:916–924.
24. Braun J, van de Veire NR, Klautz RJ, Versteegh MI, Holman ER, Westenberg JJ,Boersma E, van der Wall EE, Bax JJ, Dion RA. Restrictive mitral annuloplastycures ischemic mitral regurgitation and heart failure. Ann Thorac Surg 2008;85:430–436; discussion 436–7.
25. Magne J, Pibarot P, Dagenais F, Hachicha Z, Dumesnil JG, Senechal M. Preopera-tive posterior leaflet angle accurately predicts outcome after restrictive mitralvalve annuloplasty for ischemic mitral regurgitation. Circulation 2007;115:782–791.
26. Calafiore AM, Gallina S, Di Mauro M, Gaeta F, Iaco AL, D’Alessandro S, Mazzei V,Di Giammarco G. Mitral valve procedure in dilated cardiomyopathy: repair orreplacement?. Ann Thorac Surg 2001;71:1146–1152; discussion 1152–3.
27. Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD,Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT, O’Rourke RA, Otto CM,Shah PM, Shanewise JS. 2008 Focused update incorporated into the ACC/AHA2006 guidelines for the management of patients with valvular heart disease: areport of the American College of Cardiology/American Heart AssociationTask Force on Practice Guidelines (Writing Committee to Revise the 1998Guidelines for the Management of Patients With Valvular Heart Disease):endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardio-vascular Angiography and Interventions, and Society of Thoracic Surgeons. Circula-tion 2008;118:e523–661.
Percutaneous edge-to-edge MitraClip therapy 2357
at Hospital Severo O
choa on June 2, 2012http://eurheartj.oxfordjournals.org/
Dow
nloaded from

28. Vahanian A, Baumgartner H, Bax J, Butchart E, Dion R, Filippatos G,Flachskampf F, Hall R, Iung B, Kasprzak J, Nataf P, Tornos P, Torracca L,Wenink A. Guidelines on the management of valvular heart disease: the TaskForce on the Management of Valvular Heart Disease of the European Societyof Cardiology. Eur Heart J 2007;28:230–268.
29. Nowicki ER, Birkmeyer NJ, Weintraub RW, Leavitt BJ, Sanders JH, Dacey LJ,Clough RA, Quinn RD, Charlesworth DC, Sisto DA, Uhlig PN, Olmstead EM,O’Connor GT. Multivariable prediction of in-hospital mortality associated withaortic and mitral valve surgery in Northern New England. Ann Thorac Surg2004;77:1966–1977.
30. Luk A, Butany J, Ahn E, Fann JI, St Goar F, Thornton T, McDermott L, Madayag C,Komtebedde J. Mitral repair with the Evalve MitraClip device: histopathologicfindings in the porcine model. Cardiovasc Pathol 2009;18:279–285.
31. Ussia GP, Barbanti M, Tamburino C. Feasibility of percutaneous transcathetermitral valve repair with the MitraClip system using conscious sedation. CatheterCardiovasc Interv 2010;75:1137–1140.
32. Ypenburg C, van Bommel RJ, Borleffs CJ, Bleeker GB, Boersma E, Schalij MJ, Bax JJ.Long-term prognosis after cardiac resynchronization therapy is related to theextent of left ventricular reverse remodeling at midterm follow-up. J Am CollCardiol 2009;53:483–490.
33. Feldman T, Kar S, Rinaldi M, Fail P, Hermiller J, Smalling R, Whitlow PL, Gray W,Low R, Herrmann HC, Lim S, Foster E, Glower D. Percutaneous mitral repairwith the MitraClip system: safety and midterm durability in the initial EVEREST(Endovascular Valve Edge-to-Edge REpair Study) Cohort. J Am Coll Cardiol 2009;54:686–694.
34. Foster E, Wasserman HS, Gray W, Homma S, Di Tullio MR, Rodriguez L,Stewart WJ, Whitlow P, Block P, Martin R, Merlino J, Herrmann HC,Wiegers SE, Silvestry FE, Hamilton A, Zunamon A, Kraybill K, Gerber IL,Weeks SG, Zhang Y, Feldman T. Quantitative assessment of severity of mitralregurgitation by serial echocardiography in a multicenter clinical trial of percuta-neous mitral valve repair. Am J Cardiol 2007;100:1577–1583.
35. Feldman T, Foster E, Glower DG, Kar S, Rinaldi MJ, Fail PS, Smalling RW, Siegel R,Rose GA, Engeron E, Loghin C, Trento A, Skipper ER, Fudge T, Letsou GV,Massaro JM, Mauri L. Percutaneous repair or surgery for mitral regurgitation. NEngl J Med 2011;364:1395–1406.
36. Feldman T, Mauri L, Kar S, Rinaldi M, Fail P, Hermiller J, Smalling R, Gray W,Wang A, Herrmann H, Rogers J, Lasala J, Bajwa T, Grayburn P, Pedersen W,Foster E, Trento A, Glower D. EVEREST II Randomized Clinical Trial: a CriticalAssessment of the Safety Data In Patients Treated with the MitraClip. J Am CollCardiol 2010;56 (Suppl. 1):B23.
37. Franzen O, Baldus S, Rudolph V, Meyer S, Knap M, Koschyk D, Treede H,Barmeyer A, Schofer J, Costard-Jackle A, Schluter M, Reichenspurner H,Meinertz T. Acute outcomes of MitraClip therapy for mitral regurgitation inhigh-surgical-risk patients: emphasis on adverse valve morphology and severeleft ventricular dysfunction. Eur Heart J 2010;31:1373–1381.
38. Tamburino C, Ussia GP, Maisano F, Capodanno D, La Canna G, Scandura S,Colombo A, Giacomini A, Michev I, Mangiafico S, Cammalleri V, Barbanti M,Alfieri O. Percutaneous mitral valve repair with the MitraClip system: acuteresults from a real world setting. Eur Heart J 2010;31:1382–1389.
39. Herrmann HC, Kar S, Siegel R, Fail P, Loghin C, Lim S, Hahn R, Rogers JH,Bommer WJ, Wang A, Berke A, Lerakis S, Kramer P, Wong SC, Foster E,Glower D, Feldman T. Effect of percutaneous mitral repair with the MitraClipdevice on mitral valve area and gradient. EuroIntervention 2009;4:437–442.
40. Suri RM, Schaff HV, Dearani JA, Sundt TM III, Daly RC, Mullany CJ,Enriquez-Sarano M, Orszulak TA. Survival advantage and improved durability ofmitral repair for leaflet prolapse subsets in the current era. Ann Thorac Surg2006;82:819–826.
41. Fix J, Isada L, Cosgrove D, Miller DP, Savage R, Blum J, Stewart W. Do patientswith less than ‘echo-perfect’ results from mitral valve repair by intraoperativeechocardiography have a different outcome? Circulation 1993;88(5 Pt 2):II39– II48.
42. Hermiller J, Kar S, Lim S, Rinaldi M, Fail P, Lim S, Smalling R, Gray W, Wang A,Herrmann H, Rogers J, Lasala J, Bajwa T, Grayburn P, Pedersen W,Whisenant B, Berke A, O’Donnell M, Whitlow P, Siegel R, Trento A,Glower D, Feldman T, Foster E. EVEREST II Randomized Clinical Trial: ClinicalBenefit by MR Grade in Patients One Year following Successful MitraClipTherapy. J Am Coll Cardiol 2010;56 (Suppl. 1):B38.
43. Flameng W, Herijgers P, Bogaerts K. Recurrence of mitral valve regurgitation aftermitral valve repair in degenerative valve disease. Circulation 2003;107:1609–1613.
44. DiBardino DJ, ElBardissi AW, McClure RS, Razo-Vasquez OA, Kelly NE, Cohn LH.Four decades of experience with mitral valve repair: analysis of differential indi-cations, technical evolution, and long-term outcome. J Thorac Cardiovasc Surg2010;139:76–83; discussion 83–4.
45. Bhudia SK, McCarthy PM, Smedira NG, Lam BK, Rajeswaran J, Blackstone EH.Edge-to-edge (Alfieri) mitral repair: results in diverse clinical settings. AnnThorac Surg 2004;77:1598–1606.
46. De Bonis M, Lapenna E, La Canna G, Ficarra E, Pagliaro M, Torracca L, Maisano F,Alfieri O. Mitral valve repair for functional mitral regurgitation in end-stage dilatedcardiomyopathy: role of the “edge-to-edge” technique. Circulation 2005;112(Suppl):I402–1408.
47. Argenziano M, Skipper E, Heimansohn D, Letsou GV, Woo YJ, Kron I,Alexander J, Cleveland J, Kong B, Davidson M, Vassiliades T, Krieger K, Sako E,Tibi P, Galloway A, Foster E, Feldman T, Glower D. Surgical revision after percu-taneous mitral repair with the MitraClip device. Ann Thorac Surg 2010;89:72–80;discussion p 80.
48. Glower D, Young JN, Alexander J, Gangahar D, Skipper E, Cleveland J, Trento A,Feldman T. EVEREST II Randomized Clinical Trial: a Critical Assessment of Ana-tomical Predictors of de novo Mitral Valve Replacement or following the Mitra-Clip Procedure. J Am Coll Cardiol 2010;56 (Supp. 1):B25.
49. Geidel S, Ostermeyer J, Lass M, Schmoeckel M. Complex surgical valve repairafter failed percutaneous mitral intervention using the MitraClip device. AnnThorac Surg 2010;90:277–279.
50. Rogers JH, Yeo KK, Carroll JD, Cleveland J, Reece TB, Gillinov AM, Rodriguez L,Whitlow P, Woo YJ, Herrmann HC, Young JN. Late surgical mitral valve repairafter percutaneous repair with the MitraClip system. J Card Surg 2009;24:677–681.
51. Magne J, Girerd N, Senechal M, Mathieu P, Dagenais F, Dumesnil JG,Charbonneau E, Voisine P, Pibarot P. Mitral repair versus replacement forischemic mitral regurgitation: comparison of short-term and long-term survival.Circulation 2009;120 (Suppl):S104–S111.
52. Johnston DR, Gillinov AM, Blackstone EH, Griffin B, Stewart W, Sabik JF III,Mihaljevic T, Svensson LG, Houghtaling PL, Lytle BW. Surgical repair of posteriormitral valve prolapse: implications for guidelines and percutaneous repair. AnnThorac Surg 2010;89:1385–1394.
53. Seeburger J, Borger MA, Doll N, Walther T, Passage J, Falk V, Mohr FW. Compari-son of outcomes of minimally invasive mitral valve surgery for posterior, anteriorand bileaflet prolapse. Eur J Cardiothorac Surg 2009;36:532–538.
J.H. Rogers and O. Franzen2357a
at Hospital Severo O
choa on June 2, 2012http://eurheartj.oxfordjournals.org/
Dow
nloaded from