Embed Size (px)
Citation preview

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . - , N O . - , 2 0 1 7
ª 2 0 1 7 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 1 9 3 6 - 8 7 8 X / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c m g . 2 0 1 7 . 0 6 . 0 1 7
Effusive-Constrictive Pericarditis AfterPericardiocentesis
Incidence, Associated Findings, and Natural HistoryKye Hun Kim, MD,a,b William R. Miranda, MD,a Larry J. Sinak, MD,a Faisal F. Syed, MBCHB,a
Rowlens M. Melduni, MD,a Raul E. Espinosa, MD,a Garvan C. Kane, MD,a Jae K. Oh, MDa
ABSTRACT
Fro
Me
rel
Ma
OBJECTIVES This study sought to investigate the incidence, associated findings, and natural history of
effusive-constrictive pericarditis (ECP) after pericardiocentesis.
BACKGROUND ECP is characterized by the coexistence of tense pericardial effusion and constriction of the
heart by the visceral pericardium. Echocardiography is currently the main diagnostic tool in the assessment
of pericardial disease, but limited data have been published on the incidence and prognosis of ECP diagnosed
by echo-Doppler.
METHODS A total of 205 consecutive patients undergoing pericardiocentesis at Mayo Clinic, Rochester, Minnesota,
were divided into 2 groups (ECP and non-ECP) based on the presence or absence of post-centesis echocardiographic
findings of constrictive pericarditis. Clinical, laboratory, and imaging characteristics were compared.
RESULTS ECP was subsequently diagnosed in 33 patients (16%) after pericardiocentesis. Overt clinical cardiac
tamponade was present in 52% of ECP patients and 36% of non-ECP patients (p ¼ 0.08). Post-procedure
hemopericardium was more frequent in the ECP group (33% vs. 13%; p ¼ 0.003), and a higher percentage of neutrophils
and lower percentage of monocytes were noted on pericardial fluid analysis in those patients. Clinical and laboratory
findings were otherwise similar. Baseline early diastolic mitral septal annular velocity was significantly higher in the ECP
group. Before pericardiocentesis, respiratory variation of mitral inflow velocity, expiratory diastolic flow reversal of
hepatic vein, and respirophasic septal shift were significantly more frequent in the ECP group. Fibrinous or loculated
effusions were also more frequently observed in the ECP group. Four deaths occurred in the ECP group; all 4 patients had
known malignancies. During median follow-up of 3.8 years (interquartile range: 0.5 to 8.3), only 2 patients required
pericardiectomy for persistent constrictive features and symptoms.
CONCLUSIONS In a large cohort of unselected patients undergoing pericardiocentesis, 16% were found to have ECP.
Pre-centesis echocardiographic findings might identify such patients. Long-term prognosis in those patients remains
good, and pericardiectomy was rarely required. (J Am Coll Cardiol Img 2017;-:-–-) © 2017 by the American College of
Cardiology Foundation.
P ericardial effusion causes a variety of symp-toms depending on its acuity and volume,including dyspnea, chest or abdominal pain,
hypotension, and cardiac tamponade, which can befatal (1,2). Pericardiocentesis is the treatment ofchoice for patients with symptomatic pericardial
m the aDepartment of Cardiovascular Diseases, Mayo Clinic, Rochester,
dicine, Chonnam National University Hospital, Gwangju, Republic of K
ationships relevant to the contents of this paper to disclose.
nuscript received April 18, 2017; revised manuscript received June 19, 20
effusion. Although symptomatology and hemody-namic abnormalities typically improve dramaticallyafter pericardiocentesis, a subset of patients mightfail to show resolution of symptoms or may evenworsen after pericardiocentesis. This finding is usu-ally associated with the development of typical
Minnesota; and the bDepartment of Cardiovascular
orea. All authors have reported that they have no
17, accepted June 22, 2017.

ABBR EV I A T I ON S
AND ACRONYMS
CP = constrictive pericarditis
CT = computed tomography
E = mitral inflow early
diastolic velocity
e0 = early diastolic mitral septal
annular velocity
ECP = effusive-constrictive
pericarditis
HV = hepatic vein
Kim et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7
Effusive-Constrictive Pericarditis After Pericardiocentesis - 2 0 1 7 :- –-
2
features of constrictive pericarditis (CP). Thisentity has been previously described aseffusive-constrictive pericarditis (ECP) (3–5).
ECP is an uncommon clinical syndromecharacterized by the coexistence of tensepericardial effusion and constriction of theheart by the visceral pericardium (3–5). Thediagnostic hallmark of ECP is the persistenceof elevated right atrial pressure measuredby invasive hemodynamic assessment afterintrapericardial pressure is reduced to anormal level by pericardiocentesis (5). Peri-
cardiectomy was required in more than one-half ofthe patients with ECP in previous studies. ECP ismost likely part of a natural history of pericardialinflammation that occurs with pericardial effusion.Identification of constrictive features in the post-pericardiocentesis setting is important because suchpatients require closer follow-up.
Although invasive hemodynamic assessment bycardiac catheterization is the gold standard for thediagnosis of ECP, echo-Doppler evaluation is animportant diagnostic strategy for various pericardialdiseases, including cardiac tamponade and CP (6,7).It is proposed that ECP can be diagnosed post-pericardiocentesis by 2-dimensional and echo-Dopplerdemonstration of abnormal ventricular septal motion(due to exaggerated ventricular interdependence)and dissociation of intrathoracic and intracardiacpressures, which are the key features of CP (3).However, limited data have been published on theincidence and natural history of ECP diagnosed byecho-Doppler in a large group of patients. Therefore,we sought to investigate the incidence, echo-Dopplerfindings, and natural history of ECP detected byechocardiography after pericardiocentesis.
METHODS
From January 2006 to December 2007, peri-cardiocentesis was performed in a total of 217 patientsat Mayo Clinic, Rochester, Minnesota. Among thesepatients, 12 did not have echocardiographic imagesavailable for review. Hence, a total of 205 consecutivepatients who underwent echocardiography beforeand after pericardiocentesis were included in thepresent study. These patients were divided into 2groups based on echocardiographic evidence of CPfeatures after pericardiocentesis (ECP and non-ECPgroups). The study protocol was approved by theInstitutional Review Board of Mayo Clinic.
Baseline and follow-up information was abstractedfrom clinical notes. Before pericardiocentesis,comprehensive 2-dimensional and echo-Doppler
assessments were performed to evaluate the size,location, and hemodynamic effects of the pericardialeffusion, if the hemodynamic status of the patientallowed. In hemodynamically unstable patients,echo-Doppler assessments were limited to obtainingessential information, including the location of peri-cardial effusion and the ideal entry site for peri-cardiocentesis. Overt clinical cardiac tamponade wasdefined by a combination of: 1) pulsus paradoxus >10mm Hg, systemic hypotension (blood pressure <100mm Hg), or elevated neck veins; 2) presence of hemo-dynamic instability believed to be secondary to thepericardial effusion; or 3) the need for emergent peri-cardiocentesis during invasive procedures (8,9).
Echocardiography-guided pericardiocentesis wasperformed as previously described by our group (10).To ensure complete drainage of the pericardial fluid, apigtail catheter was introduced into the pericardialspace and kept in place until output was <50 cc over a24-h period. Follow-up comprehensive echo-Dopplerstudies were performed to assess for the develop-ment of ECP within 1 week of pericardiocentesis.The presence of constrictive features was definedby post-pericardiocentesis echo-Doppler findings ofinspiratory decrease and expiratory increase of earlydiastolic mitral inflow velocity (E) >25% accompaniedby at least 1 of the following: expiratory diastolic flowreversal of hepatic vein (HV); respirophasic inter-ventricular septal shift; or augmented early diastolicmitral septal annular velocity (e0) and to a level higherthan that of the lateral mitral e0.
Fibrinous pericardial effusion was defined as thepresence of pericardial effusion with multiple fibri-nous strands. Circumferential pericardial effusionwas defined as an effusion that encircled the entireheart. Loculated pericardial effusion was defined asan effusion that was located adjacent to 1 or otherheart wall or an effusion that was compartmentalizedby pericardial adhesion to the heart wall. Pericardialrind was defined as the presence of diffuse pericardialthickening associated with echolucent soft tissues.
STATISTICAL ANALYSIS. The Statistical Package forSocial Sciences for Windows, version 13.0 (SPSS, Inc.,Chicago, Illinois) was used for statistical analyses.Data are expressed as mean � SD or median (inter-quartile range [IQR]; 25th to 75th percentiles) forparametric and nonparametric continuous variables,respectively, and as percentage for categorical data.Chi-square test was used to compare differences incategorical values between the 2 groups. IndependentStudent t test was used to compare differencesin parametric continuous variables, whereas Wilcoxonrank sum test was used for nonparametric continuous

TABLE 1 Baseline Clinical Characteristics
No ECP(n ¼ 172)
ECP(n ¼ 33) p Value
Age, yrs 62 (50–72) 57 (46.5–67.5) 0.09
Male 75 (43.6) 19 (57.5) 0.14
Body mass index, kg/m2 26.6 (22.7–31.8) 29.8 (25.8–32.9) 0.56
SBP, mm Hg 109.5 (96–123) 105 (94.5–121.5) 0.52
DBP, mm Hg 66 � 13 65 � 13 0.76
Heart rate, beats/min 91 � 18 92 � 17 0.67
NYHA functional class 3 (2–3) 3 (2–3) 0.80
Overt clinical tamponade 61 (35.5) 17 (51.5) 0.08
Etiology
Post-cardiac surgery 53 (30.8) 6 (18.2) 0.14
Idiopathic 43 (25.0) 9 (27.3) 0.78
Procedure-related hemopericardium 22 (12.8) 11 (33.3) 0.003
Malignancy 22 (12.8) 2 (6.1) 0.27
Post-viral pericarditis 11 (6.4) 3 (9.1) 0.57
Other 21 (12.2) 2 (6.1) 0.31
Previous anti-inflammatory therapy 10 (5.8) 3 (9.1) 0.48
Previous colchicine therapy 0 0 0.99
Previous chest radiation therapy 7 (4.1) 1 (3.0) 0.78
Values are median (interquartile range), n (%), or mean � SD.
DBP ¼ diastolic blood pressure; ECP ¼ effusive-constrictive pericarditis; NYHA ¼ New York Heart Association;SBP ¼ systolic blood pressure.
TABLE 2 Pericardial Fluid Analysis
No ECP(n ¼ 172)
ECP(n ¼ 33) p Value
Drainage amount, ml 500 (365.0–700.0) 387.5 (308.8–547.5) 0.046
Bloody effusion 109 (63.4) 24 (72.7) 0.44
WBC count, per mm3 1,175 (200.0–3,487.5) 1,950 (787.5–3,662.5) 0.18
Neutrophils, % 19.5 (5.0–42.3) 50 (25.0–65.5) 0.004
Lymphocytes, % 26.5 (11.0–56.3) 32.5 (4.8–50.5) 0.61
Monocytes, % 25 (9.5–48.0) 11 (4.0–19.5) 0.007
Hematocrit, % 13.8 (3.5–26.5) 27.8 (8.3–35.1) 0.19
pH 7.5 (7.5–7.8) 7.8 (7.39–8.00) 0.69
Specific gravity 1.028 (1.025–1.032) 1.029 (1.027–1.034) 0.29
Protein, g/dl 4.2 (3.3–5.1) 4.4 (3.7–5.1) 0.62
Glucose, mg/dl 91 (69.0–111.0) 82 (59.0–102.0) 0.29
LDH, mg/dl 445 (182.0–1,033.8) 597 (402.8–956.8) 0.46
Values are median (interquartile range) or n (%).
LDH ¼ lactate dehydrogenase; WBC ¼ white blood cell; other abbreviation as in Table 1.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7 Kim et al.- 2 0 1 7 :- –- Effusive-Constrictive Pericarditis After Pericardiocentesis
3
variables. Correlations between the variables wereestablished by Pearson correlation. In order to assessthe prevalence of ECP in cardiac tamponade related tocardiac surgery/percutaneous interventions versustamponade unrelated to procedures, we used Poissonregression models with sandwich estimators beforeand after adjustment for baseline covariates. Values ofp < 0.05 was considered statistically significant.
RESULTS
Post-pericardiocentesis echo-Doppler examinationwas performed after a mean 2.0 � 1.5 days. Of a totalof 205 patients, 33 (16.1%) were found to have ECP(ECP group), whereas 172 (83.9%) did not meet echo-Doppler criteria for constriction (non-ECP group).Overt clinical cardiac tamponade was present in 78patients (38% of the entire cohort). The presence ofclinical cardiac tamponade was similar betweengroups (p ¼ 0.08).
Baseline clinical characteristics of both groups aresummarized in Table 1. Cardiac surgery (28.8%),idiopathic pericarditis (25.4%), procedure-relatedpericardial effusion (16.1%), and malignancy (11.7%)were the most common causes of pericardial effusionrequiring pericardiocentesis. Baseline characteristicswere not different between the groups, except forprocedure-related pericardial effusion (which ismostly bloody effusion or coagulum tamponade),being significantly more frequent in the ECP group(33.0% vs. 12.8%; p ¼ 0.003). However, using Poissonregression models and adjusting for baseline cova-riates, cardiac surgery/procedure-related tamponadewas not associated with subsequent diagnosis of ECP(risk ratio: 0.90; 95% confidence interval: 0.66 to 1.26).
The results of pericardial fluid analysis are summa-rized in Table 2. Pericardiocentesis volumewas smallerin the ECP group (387.5 ml [IQR: 308.8 to 547.5 ml] vs.500ml [IQR: 365 to 700ml]; p¼0.046). Although therewas no significant difference in total leukocyte countbetween the 2 groups (1,950.0 per mm3 [IQR: 787.5 to3,662.5 per mm3] vs. 1,175.0 per mm3 [IQR: 200.0to 3,487.5 per mm3]; p ¼ 0.18), the percentage ofneutrophils was significantly higher (50.0% [IQR:25.0% to 65.5%] vs. 19.5% [IQR: 5.0% to 42.3%];p ¼ 0.004), and the percentage of monocytes wassignificantly lower (11.0% [IQR: 4.0% to 19.5%]vs. 25.0% [IQR: 9.5% to 48.0%]; p ¼ 0.007) in ECPcompared to non-ECP patients. No differences in otherpericardial fluid parameters were identified.
ECHOCARDIOGRAPHIC FEATURES PRE- AND POST-
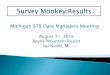
PERICARDIOCENTESIS. Pre-pericardiocentesis echo-Doppler findings are summarized in Table 3.Figure 1 illustrates echo-Doppler findings pre- and
post-pericardiocentesis in a patient with ECP. Figure 2shows post-pericardiocentesis respirophasic shift,mitral inflow, and tissue Doppler findings in adifferent patient with ECP (Online Videos 1 and 2).Mean medial mitral e0 velocity was higher in the ECPgroup (8.9 � 2.5 vs. 6.9 � 2.4; p < 0.001), andrespirophasic interventricular septal shift was morefrequently observed in ECP patients (21.2% vs. 1.2%;p < 0.001). Mitral inflow variation was seen in 89.3%of ECP patients and 62.3% of non-ECP patients(p ¼ 0.006). Expiratory HV flow reversals were alsocommonly encountered in the ECP group (48.0% vs.

TABLE 3 Echocardiographic Findings Before Pericardiocentesis
No ECP(n ¼ 172)
ECP(n ¼ 33) p Value
LVEF, % 63 (57.5–67.0) 63.5 (58.8–65.0) 0.74
E (expiratory) m/s 0.90 (0.70–1.1) 0.90 (0.80–1.1) 0.48
E (inspiratory), m/s 0.70 (0.50–0.85) 0.60 (0.50–0.75) 0.51
A, m/s 0.73 (0.60–1.0) 0.60 (0.45–0.90) 0.12
DT, ms 172 (156.5–208.0) 162 (151.3–181.3) 0.07
e0 (medial), cm/s 6.9 � 2.4 8.9 � 2.5 <0.001
e0 (lateral), cm/s 8 (6.0–9.8) 9 (7.5–9.5) 0.08
Respirophasic septal shift 2 (1.2) 7 (21.2) <0.001
Mitral inflow variation 91/146 (62.3) 25/28 (89.3) 0.006
Hepatic vein flow reversal 27/120 (22.5) 12/25 (48.0) 0.009
Dilation of the IVC 118/149 (79.2) 24/31 (77.4) 0.83
Fibrinous PE 26 (15.1) 12 (36.4) 0.004
Loculated PE 28 (16.3) 11 (33.3) 0.02
Values are median (interquartile range), mean � SD, or n (%). Denominators for mitral inflow, inferior vena cavadilation, and hepatic vein flow reversal represent the total number of patients with available echo-Doppler data.
A ¼ mitral inflow late diastolic velocity; DT ¼ mitral inflow deceleration time; E ¼ mitral inflow early diastolicvelocity; e0 ¼ early diastolic mitral septal annular velocity; LVEF ¼ left ventricular ejection fraction; IVC ¼ inferiorvena cava; PE ¼ pericardial effusion; other abbreviation as in Table 1.
Kim et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7
Effusive-Constrictive Pericarditis After Pericardiocentesis - 2 0 1 7 :- –-
4
22.5%; p ¼ 0.009). There were no differences in mitralinflow deceleration time or in expiratory E or inspi-ratory E- or A-wave velocities on transmitral Doppler.Fibrinous and loculated pericardial effusions werealso more common in the ECP group.
Table 4 lists post-pericardiocentesis echocardio-graphic findings. By definition, mitral inflow variationwas present in all of the ECP patients, as opposed toonly 1.2% of non-ECP patients. Respirophasic septalshift was present in 97% of ECP patients, and dilationof the inferior vena cava was present in all; thosefeatures were present in 21.5% and 41.3% of non-ECPpatients, respectively (p < 0.001 for both). Althoughno significant differences in E- and A-wave velocitieswere seen, mitral inflow deceleration time wasshorter in the ECP group. Diffuse pericardial thick-ening was present in 72.7% of ECP patients but in only19.2% of non-ECP patients (p < 0.001).
ADDITIONAL IMAGING AND CARDIAC CATHETERIZATION
DATA IN PATIENTS WITH ECP. Four ECP patients un-derwent computed tomography (CT) scanning within7 days after pericardiocentesis. Only 1 study wasperformed to assess the pericardium, and mild peri-cardial thickening was present in this patient. Tenpatients underwent CT within a week before peri-cardiocentesis. Four of those were dedicated cardiacCTs (performed before cardiac ablation); all patientshad normal pericardial thickness without any evi-dence of CP. None of the patients underwent cardiacmagnetic resonance within 7 days pre- or post-pericardiocentesis.
One ECP patient underwent cardiac catheterizationthe day after pericardiocentesis. Right atrial pressure
was 19 mm Hg, and hemodynamic findings wereconsistent with constrictive physiology.
CLINICAL OUTCOMES OF POST-PERICARDIOCENTESIS
CONSTRICTIVE FEATURES. Of the 33 patients withconstrictive features, 16 were treated with steroids(n ¼ 3) or nonsteroidal anti-inflammatory therapy(n ¼ 13). Colchicine was prescribed to 6 patients (asmonotherapy in 3). During follow-up (median 3.8years [IQR: 0.5 to 8.3 years]), 4 patients died early intheir clinical course; all of them had known malig-nancies. Six patients (18%) were rehospitalized withprogressive shortness of breath or symptoms of heartfailure (median 33 days [IQR: 29 to 78 days] afterinitial pericardiocentesis). Follow-up echocardiogra-phy (median 134 days [IQR: 36.5 to 395.5 days]) wasavailable for 26 of 33 patients (79%) and showed res-olution of constrictive features in 24 of them. Twopatients showed persistent constrictive physiologyand symptoms despite anti-inflammatory therapyand underwent successful pericardiectomy. In bothcases, pathology revealed pericardial thickening, andmicroscopic findings were consistent with CP.
DISCUSSION
We present herein the incidence of ECP after peri-cardiocentesis and its long-term prognosis in a largegroup of patients seen at a tertiary care center.Among several important observations, our datasuggest that: 1) echocardiographic features of CPare common post-pericardiocentesis; and 2) ECPresolves in most patients but may require peri-cardiectomy in a small number of cases.
Features of CP after pericardiocentesis wereobserved in 16% of our cohort. This number issignificantly higher than the 1% to 2% reported inunselected series of patients with pericarditis (4,11),and it is still higher when compared to the subsetof patients presenting with cardiac tamponade(8%) (4). However, it is lower than the rates of ECPobserved in patients requiring pericardiectomy for CP(24% prevalence) (12). According to a recent system-atic review including a total of 642 patients withpericarditis/pericardial effusions, the prevalence ofECP varied between 2.4% and 14.8% (3).
There are several different explanations for thewide variation in the incidence of ECP reported in theliterature. First, the methodology used to diagnoseECP varied substantially between groups(4,9,11,13,14). Some studies included simultaneouscardiac catheterization in all patients undergoingpericardiocentesis; in other studies, the diagnosiswas based on echocardiography or a combination ofboth modalities. Moreover, the echocardiographic

FIGURE 1 Transthoracic Echo-Doppler Findings Before and After Pericardiocentesis in a Patient With Effusive-Constrictive Pericarditis
*5
10
[cm]
2
4
6
8
10
12 -9
-4 -2 0
0
-6 -3
12 -9 -6 -3
12
14
1.5
1.0
0.5
0.6
0.4
0.2
-0.5
[m/s]
[m/s]
-0.2
-0.4
-0.6
-0.893
HR
DR
15
20
A
B
C
D
E
(A) Pre-centesis echocardiography shows moderate-to-large pericardial effusion (asterisk). (B) Post-centesis echocardiography shows diffuse pericardial
thickening by echolucent soft tissue (pericardial rind) (arrow). (C) Respirophasic septal shift (thin arrows) is illustrated by M-mode at the level of the
midventricle. (D and E) Doppler reveals typical respiratory variation of mitral inflow (D) and expiratory diastolic flow reversal (DR) in the hepatic veins (E).
Simultaneous respirometry during Doppler recording is shown. Upward inflection represents inspiration; downward inflection represents expiration.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7 Kim et al.- 2 0 1 7 :- –- Effusive-Constrictive Pericarditis After Pericardiocentesis
5
assessment of CP has evolved tremendously over theyears. Currently, echo-Doppler allows for the diag-nosis of constrictive physiology with greater sensi-tivity and specificity than ever before (15). Thus,cardiac catheterization is now reserved for patientswhose noninvasive evaluation is inconclusive.Defining the “expected” incidence of constrictivefeatures post-pericardiocentesis by echocardiographyand its associated findings is of clinical importancebecause it might guide follow-up and prevent theneed for further testing or procedures.
The incidence of ECP has also varied according tothe studied populations and associated etiologies. Forexample, rates of ECP in tuberculous pericarditis havebeen reported to be as high as 38% (16). The risk ofrequiring pericardiectomy in ECP also appears to bedirectly related to the underlying cause, varying from50% to 73% according to the series (3). In contrast,
Sagrista-Sauleda et al. (17) reported resolution ofconstrictive features in all 16 patients diagnosed withtransient constriction; those patients found to haveconstrictive features in the convalescent phase ofacute pericarditis. Because of differences in method-ology and underlying etiologies, comparison betweenstudies is difficult, and the prognosis of ECP/transientconstriction is still poorly understood. Moreover,studies published more than a decade ago involvedimaging during an era when the awareness of“uncommon” patterns of CP was not fully appreci-ated, and therapeutic options were more limited andless standardized (18). Thus, it is possible peri-cardiectomy was performed in patients with transientor reversible constriction. It is noteworthy that idio-pathic and post-operative cases accounted for >40%of our ECP patients. In addition, one-third of ECPcases were seen in procedure-related effusions

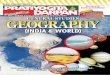
FIGURE 2 2-Dimensional and Doppler Findings Post-Pericardiocentesis in a Different Patient With Effusive-Constrictive Pericarditis
A10
5
[cm/s]
1.0
0.5
15
15
10
5
10
5
V
V
[m/s]
-0.5
-5
0-1-2
+1
-10
-15
-20
Expiration
Inspiration
-4 -2 0
C
DB
(A and B) Tissue Doppler shows elevated mitral e0 velocity (14 cm/s) (A), and mitral inflow reveals short deceleration time, increased E/A ratio, and
inspiratory decrease in E velocity (B). L-wave is also present (arrow), consistent with elevated filling pressures. (C and D) Respirophasic septal shift is
seen in the apical 4-chamber view (left ventricle becomes smaller with inspiration and larger with expiration, with opposite changes occurring in the right
ventricle). Note the echolucent soft tissue (pericardial rind) surrounding the left ventricle. Simultaneous respirometry during Doppler recording is shown.
Upward inflection represents inspiration; downward inflection represents expiration. See Online Videos 1 and 2.
TABLE 4 Echocardiographic Findings After Pericardiocentesis
No ECP(n ¼ 172)
ECP(n ¼ 33) p Value
LVEF, % 62 (58–66) 62 (56–66) 0.69
E, m/s 0.95 � 0.26 1.02 � 0.23 0.19
A, m/s 0.70 (0.51–1.00) 0.50 (0.40–0.80) 0.07
DT, ms 180 (166–206) 163 (151–174) <0.001
e0 (medial), cm/s 7 (6–9) 10 (8.5–11.5) <0.001
e0 (lateral), cm/s 8 (7–10) 9 (7–10) 0.44
Respirophasic septal shift 37 (21.5) 32 (97.0) <0.001
Mitral inflow variation 2 (1.2) 33 (100.0) N/A
Hepatic vein flow reversal 3 (1.7) 27 (81.8) <0.001
Dilation of the IVC 71 (41.3) 33 (100.0) <0.001
Pericardial rind 33 (19.2) 24 (72.7) <0.001
Residual pericardial effusion 0.87
None/trivial 115 (66.9) 23 (69.7)
Small 56 (32.6) 10 (30.3)
Moderate 1 (0.6) 0 (0.0)
Values are median (interquartile range), mean � SD, or n (%).
Abbreviations as in Tables 1 and 3.
Kim et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7
Effusive-Constrictive Pericarditis After Pericardiocentesis - 2 0 1 7 :- –-
6
(vs. 13% of non-ECP cases). Although cardiac surgery-or procedure-related effusions were not associatedwith higher risk of ECP, our results should beextrapolated with caution to populations that differfrom ours.
Interestingly, overt clinical cardiac tamponade waspresent is only one-half of our patients with ECP.Although the prevalence of tamponade physiology bycardiac catheterization could have been higher, ourresults would be in agreement with the observationsof Ntsekhe et al. (16). In their study, cardiac tampo-nade diagnosed by right heart catheterization waspresent in 53% of ECP cases, a rate similar to that ofpatients without ECP (56%). Although originallydescribed in the setting of cardiac tamponade, thoseresults support that the distinction between ECP andtransient CP is essentially academic. Both entities arepart of a clinical spectrum of patients presenting withpericardial inflammation, less compliant pericardium,and pericardial effusion. The hypothesis of inflam-mation playing a significant role in the pathophysi-ology of ECP (5) is also supported by our data, as a

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: Echocardio-
graphic features of CP are common after pericardiocentesis,
but the long-term prognosis is good. Pericardiectomy
was necessary in only a small number of patients. Pre-
pericardiocentesis, high mitral medial e0 velocities and
respirophasic septal shift were seen more frequently in the
ECP group, suggesting that these patients have distinct
echo-Doppler features even before pericardiocentesis is
performed.
TRANSLATIONAL OUTLOOK: Data regarding the natural
history of ECP are limited, and our results need to be
reproduced in other populations. In addition, studies correlating
echocardiographic findings and invasive hemodynamics
post-pericardiocentesis are needed to allow better
understanding of the pathophysiology and prognosis of ECP.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7 Kim et al.- 2 0 1 7 :- –- Effusive-Constrictive Pericarditis After Pericardiocentesis
7
higher proportion of acute inflammatory cells is seenin the pericardial fluid of ECP patients. Pericardialthickening by 2-dimensional echocardiography wasalso more frequent in that group, and the reversibilityof constriction could be predicted by intense peri-cardial inflammation noted on cardiac magneticresonance and by increased inflammatory biomarkers(19). Therefore, our finding suggests that patientswho undergo pericardiocentesis are best served by aperiod of anti-inflammatory treatment to shorten theperiod of ECP or perhaps even lessen the possibility ofchronic CP. It should be noted that one-fifth of ECPpatients were rehospitalized because of dyspnea orheart failure within 3 months. Although the long-termprognosis is good, those patients might require closerfollow-up shortly after their index event.
Our results also suggest that patients with ECPmight have distinct echo-Doppler features evenbefore pericardiocentesis compared to patients witheffusive pericarditis. Higher mitral medial e0 velocityand respirophasic septal shift, features typicallyencountered in patients with CP (15), were morefrequent in the ECP group. This is also the most likelyexplanation for the higher prevalence of mitral inflowvariation and HV flow reversal in the ECP group.Although those findings are seen in tamponadephysiology (8), the prevalence of clinical cardiactamponade was similar between groups. To ourknowledge, pre-pericardiocentesis echo-Dopplerfindings in patients with ECP have never been re-ported. Whether those features can predict post-pericardiocentesis findings and long-term prognosisrequires further investigation.
Our study represents the largest to assess theincidence of constrictive features/ECP in patientsundergoing pericardiocentesis in the United States.Although multiple studies have described the inci-dence of ECP in developing countries, the epidemi-ology of patients presenting with acute pericarditis/pericardial effusions is very different in NorthAmerica and Europe than in other parts of the world(2). In addition, our study is the first to include acomprehensive echo-Doppler assessment ofconstrictive features post-pericardiocentesis. This isclinically important because echocardiographycurrently is the main diagnostic tool for pericardialdiseases (1), and the incidence of echo-Doppler fea-tures of CP post-centesis in unselected patients hasnot been described. Our data suggest that the long-term prognosis in such patients is good, and thatobservation and medical management rather thanearly pericardiectomy are the preferred therapy.However, our favorable results need to be reproducedin other large-scale studies.
STUDY LIMITATIONS. This is a single-center, retro-spective study. Although our institution is a tertiarycenter, we included consecutive patients in order tominimize selection bias. However, referral bias mighthave contributed to the higher prevalence of ECPobserved in our study compared to others. Simulta-neous cardiac catheterization during pericardiocent-esis is not routinely performed in our practice, andthe incidence of ECP based on invasive versusnoninvasive assessment might have differed. Furtherstudies comparing invasive hemodynamic criteria toimaging criteria for ECP are required to address thisquestion. In addition, a small proportion of patientsin the non-ECP group had some but not all features ofconstriction, and whether these patients would havebeen diagnosed with ECP using invasive hemody-namic assessment is unknown.
CONCLUSIONS
The results of our study showed that evidence of ECPpost-pericardiocentesis is common and that CP fea-tures usually resolve either spontaneously or withmedical management. These observations suggest areversible, inflammatory cause for the hemodynamicabnormality and support a conservative approach tomanagement, reserving pericardiectomy for patientsrefractory to adequate anti-inflammatory therapy.
ADDRESS FOR CORRESPONDENCE: Dr. Jae K. Oh,Department of Cardiovascular Diseases, Mayo Clinic,200 First Street SW, Rochester, Minnesota 55905.E-mail: [email protected].

Kim et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7
Effusive-Constrictive Pericarditis After Pericardiocentesis - 2 0 1 7 :- –-
8
RE F E RENCE S
1. Adler Y, Charron P, Imazio M, et al. 2015 ESCguidelines for the diagnosis and management ofpericardial diseases: the Task Force for theDiagnosis and Management of Pericardial Diseasesof the European Society of Cardiology (ESC).Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921–64.
2. Imazio M, Adler Y. Management of pericardialeffusion. Eur Heart J 2013;34:1186–97.
3. Ntsekhe M, Shey Wiysonge C, Commerford PJ,Mayosi BM. The prevalence and outcome ofeffusive constrictive pericarditis: a systematicreview of the literature. Cardiovasc J Afr 2012;23:281–5.
4. Sagrista-Sauleda J, Angel J, Sanchez A,Permanyer-Miralda G, Soler-Soler J. Effusive-constrictive pericarditis. N Engl J Med 2004;350:469–75.
5. Syed FF, Ntsekhe M, Mayosi BM, Oh JK. Effu-sive-constrictive pericarditis. Heart Fail Rev 2013;18:277–87.
6. Khandaker MH, Espinosa RE, Nishimura RA,et al. Pericardial disease: diagnosis and manage-ment. Mayo Clin Proc 2010;85:572–93.
7. Zagol B, Minderman D, Munir A, D’Cruz I.Effusive constrictive pericarditis: 2D, 3D echocar-diography and MRI imaging. Echocardiography2007;24:1110–4.
8. Burstow DJ, Oh JK, Bailey KR, Seward JB,Tajik AJ. Cardiac tamponade: characteristic Dopplerobservations. Mayo Clin Proc 1989;64:312–24.
9. Tsang TS, Barnes ME, Gersh BJ, Bailey KR,Seward JB. Outcomes of clinically significantidiopathic pericardial effusion requiring interven-tion. Am J Cardiol 2003;91:704–7.
10. Tsang TS, Freeman WK, Sinak LJ, Seward JB.Echocardiographically guided pericardiocentesis:evolution and state-of-the-art technique. MayoClin Proc 1998;73:647–52.
11. Nugue O, Millaire A, Porte H, et al. Peri-cardioscopy in the etiologic diagnosis of pericar-dial effusion in 141 consecutive patients.Circulation 1996;94:1635–41.
12. Cameron J, Oesterle SN, Baldwin JC,Hancock EW. The etiologic spectrum of constric-tive pericarditis. Am Heart J 1987;113:354–60.
13. George S, Salama AL, Uthaman B, Cherian G.Echocardiography in differentiating tuberculousfrom chronic idiopathic pericardial effusion. Heart2004;90:1338–9.
14. Reuter H, Burgess LJ, Louw VJ, Doubell AF.The management of tuberculous pericardialeffusion: experience in 233 consecutive patients.Cardiovasc J S Afr 2007;18:20–5.
15. Syed FF, Schaff HV, Oh JK. Constrictivepericarditis—a curable diastolic heart failure. NatRev Cardiol 2014;11:530–44.
16. Ntsekhe M, Matthews K, Syed FF, et al.Prevalence, hemodynamics, and cytokine profileof effusive-constrictive pericarditis in patientswith tuberculous pericardial effusion. PLoS One2013;8:e77532.
17. Sagrista-Sauleda J, Permanyer-Miralda G,Candell-Riera J, Angel J, Soler-Soler J. Tran-sient cardiac constriction: an unrecognizedpattern of evolution in effusive acute idio-pathic pericarditis. Am J Cardiol 1987;59:961–6.
18. Sagrista-Sauleda J. Pericardial constriction:uncommon patterns. Heart 2004;90:257–8.
19. Feng D, Glockner J, Kim K, et al. Cardiacmagnetic resonance imaging pericardial lategadolinium enhancement and elevated inflam-matory markers can predict the reversibility ofconstrictive pericarditis after antiinflammatorymedical therapy: a pilot study. Circulation 2011;124:1830–7.
KEY WORDS effusive-constrictivepericarditis, echocardiography,pericardiocentesis
APPENDIX For supplemental videos andtheir legends, please see the online version ofthis article.