Embed Size (px)
Citation preview

w.sciencedirect.com
i n t e r n a t i o n a l j o u r n a l o f nu r s i n g s c i e n c e s 2 ( 2 0 1 5 ) 2 9 5e3 0 3
HOSTED BY Available online at ww
ScienceDirect
journal homepage: ht tp: / /www.elsevier .com/journals / internat ional -journal -of -nursing-sciences/2352-0132
Original Article
Efficacy of combining traditional Chinese medicinefumigation with Western medicine for diabeticperipheral neuropathy: A systematic review andmeta-analysis
Lei Zhang a, Xu Tian a, Yue Ma b, Ying-Hui Jin c, Fan-Jie Meng d,*
a Graduate College, Tianjin University of Traditional Chinese Medicine, Tianjin 300193, Chinab Department of Nursing, Shijiazhuang College of Medicine, Shijiazhuang 050061, Chinac School of Nursing, Tianjin University of Traditional Chinese Medicine, Tianjin 300193, Chinad Department of Teachers' Development and Evaluation, Tianjin University of Traditional Chinese Medicine, Tianjin
300193, China
a r t i c l e i n f o
Article history:
Received 25 May 2015
Received in revised form
12 July 2015
Accepted 27 July 2015
Available online 18 September 2015
Keywords:
Fumigation
Diabetic
Peripheral neuropathy
Traditional Chinese medicine
* Corresponding author.E-mail address: [email protected] (F
Peer review under responsibility of Chinesehttp://dx.doi.org/10.1016/j.ijnss.2015.08.0042352-0132/Copyright © 2015, Chinese Nursinarticle under the CC BY-NC-ND license (http
a b s t r a c t
Objective: A systematic review and meta-analysis was conducted to evaluate the effec-
tiveness of supplementing Western medicine with Traditional Chinese medicine (TCM)
fumigation in patients with diabetic peripheral neuropathy.
Methods: The China Biomedical Literature, Chinese full-text periodical, China National
Knowledge Infrastructure, WanFang, PubMed, EMbase, and Cochrane Library databases
were searched for relevant randomized controlled trials published from inception through
May 2015. The methodological quality of eligible studies was evaluated using the Cochrane
Risk Bias Assessment tool, and summarized effects were calculated using Reviewer Man-
ager 5.1 software. Subgroup analysis was conducted based on the duration of intervention.
Results: The initial search identified 312 relevant studies, of which 40 randomized
controlled trials involving 3497 patients were eligible for analysis. The results indicated
that TCM fumigation significantly improved the curative effects [risk ratio (RR) ¼ 1.34, 95%
CI (confidence interval): 1.29e1.39], common peroneal motor nerve conduction velocity
[standard mean difference (SMD) ¼ 2.93, 95% CI: 2.26e3.61], common peroneal sensory
nerve conduction velocity (SMD ¼ 2.23, 95% CI: 1.46e3.01), and plasma viscosity
(SMD ¼ �1.02, 95% CI: �1.35e0.69) compared to Western medicine alone (all p < 0.01). A
subgroup analysis indicated that the curative effects were significant after 15 days
(RR ¼ 1.31, 95% CI: 1.21e1.42), 30 days (RR ¼ 1.33, 95% CI: 1.26e1.40), and 60 days (RR ¼ 1.50,
95% CI: 1.32e1.71) of combined treatment (all p < 0.01).
.-J. Meng).
Nursing Association.
g Association. Production and hosting by Elsevier (Singapore) Pte Ltd. This is an open access://creativecommons.org/licenses/by-nc-nd/4.0/).

i n t e r n a t i o n a l j o u rn a l o f n u r s i n g s c i e n c e s 2 ( 2 0 1 5 ) 2 9 5e3 0 3296
Conclusion: TCM fumigation significantly improves the clinical outcomes of diabetic pe-
ripheral neuropathy, though further confirmatory studies are needed.
Copyright © 2015, Chinese Nursing Association. Production and hosting by Elsevier
(Singapore) Pte Ltd. This is an open access article under the CC BY-NC-ND license (http://
creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Diabetic peripheral neuropathy (DPN) is the most common
chronic complication of diabetes mellitus [1]. It is the main
contributor to diabetic foot ulcers, which are responsible for
the majority of non-traumatic amputations, and ultimately
increases the risk for mortality in diabetic patients [2,3]. The
pathogenesis of DPN is not well understood, and current
Western medicines fail to adequately treat this condition [4].
However, Traditional Chinese medicine (TCM) offers consid-
erable advantages overWesternmedicine for the treatment of
chronic diseases and their associated complications. For
example, previous work has shown that TCM fumigation
promotes local circulation of blood and lymphatic fluids via
stimulation of blood vessels and nerves [5]. Nonetheless, data
demonstrating the benefits obtained from TCM fumigation in
DPN patients are inconclusive. This systematic review and
meta-analysis of randomized controlled trials was conducted
in order to evaluate the efficacy of TCM fumigation compared
to Western medicine alone in the treatment of patients with
DPN.
2. Materials and methods
The search and screening of all potential studies, extraction of
data, assessment of study quality, and analysis and reporting
of results in this study were all in accordance with the
Preferred Reporting Items for Systematic Review and Meta-
analysis [6] and Cochrane Handbook for Systematic Reviews
of Interventions Version 5.1.0 [7]. All analyses were conducted
on data extracted from previously published studies; there-
fore, ethical approval and informed consent were not
required.
2.1. Literature search
Two investigators (L. Zhang and X. Tian) independently
searched for potential studies that compared Western medi-
cine and TCM fumigation with Western medicine alone for
treatment of DPN listed in PubMed, EMBASE, the Cochrane
Central Register of Controlled Trials, Google Scholar,
Clinicaltrials.gov (http://clinicaltrials.gov), China Biomedical
Literature, Chinese full-text periodical, Wanfang, and China
National Knowledge Infrastructure databases up through May
2015. The following search terms were used: “diabet*” OR
“diabetes mellitus” (Mesh) AND “peripheral neuropathy” OR
“neuritis” (Mesh) OR “peripheral nerve” OR “peripheral neur*”
AND “Traditional Chinese medicine fumigation” OR “fumiga-
tion*” OR “fumigation” (Mesh) OR “embalm wash” OR “drug
fumigation” AND “randomized controlled trial” (publication
type) OR “randomized controlled trials as topic” (Mesh) OR
“random*” AND human NOT animal. The reference lists of
topic-related reviews and eligible studies were also searched
to include any latent articles and guarantee the recall ratio.
Only studies published in English or Chinese languages were
eligible. Any discrepancies that occurred during the search
and selection of literature were resolved by discussion with a
third investigator (Y. Ma).
2.2. Selection criteria
Selection criteria were specified a priori according to the PICOS
acronym: population, all diabetic patients with DPN were
eligible [8]; interventions and comparisons, studies comparing
the efficacy of Western medicine (methycobal, alprostadil,
alpha lipoic acid, ligustrazine, vitamin B1, vitamin B6, or
epalrestat) plus TCM fumigation or alone; outcomes, the
outcomes included in this study were total effect rate (defined
as self-conscious symptom and tendon reflection improve-
ment, electromyography nerve conduction velocity increase
<5 m/s, or the traditional Chinesemedicine syndrome integral
reduce 30% or higher), nerve conduction velocity, vibration
perception threshold, and plasma viscosity; study design, only
randomized controlled trials were included. Any discrep-
ancies that occurred between authors concerning the eligi-
bility of a studywere resolved by consulting a third author (Y.-
H. Jing) or by consensus.
2.3. Data extraction
The total effective rate and nerve conduction velocity were
extracted as primary outcomes, and vibration perception
threshold and plasma viscosity were specified as secondary
outcome measures of interest in this study. Relevant data
were independently extracted from eligible full-text articles
by two investigators (L. Zhang and F.-J. Meng) using a pre-
designed standardized data extraction form. If essential in-
formation from an included study was incomplete, the cor-
responding author of the original study was contacted. Any
discrepancies that occurred between authors concerning the
extracted data were resolved by consulting a third author (L.
Zhang).
2.4. Quality assessment
The Cochrane Risk of Bias tool released by the Cochrane
Collaboration was used to assess the methodological quality
of each of eligible study [7]. Six domains, including selection,
performance, detection, attrition, reporting, and other biases,

i n t e r n a t i o n a l j o u r n a l o f nu r s i n g s c i e n c e s 2 ( 2 0 1 5 ) 2 9 5e3 0 3 297
were critically assessed to judge the level of risk of bias of each
included study. Each domainwas rated as “high,” “unclear,” or
“low” bias risk depending on the degree of matching between
information extracted from the study and the assessment
criteria [7].
2.5. Statistical analysis
All analyses and estimations of summary effects were per-
formed using Review Manager 5.3 software (Copenhagen: The
Nordic Cochrane Centre, The Cochrane Collaboration, 2013).
The pooled effect estimates of dichotomous outcomes were
expressed as relative risk (RR) with corresponding 95% confi-
dence intervals (CIs), and the standard mean difference (SMD)
with 95% CI was used to express continuous outcomes such as
nerve conduction velocity. The heterogeneity across studies
was assessed using the Cochrane's Q statistic with corre-
sponding p value and quantified as an I2 statistic; I2 �50% in-
dicates substantial heterogeneity. Meta-analyses was
performed using a random effects model based on the Man-
teleHaenszel method, or a fixed effects model based on an
inverse variance statistical approach according to the clinical
characteristics and methodologies of the pooled studies. A
subgroup analysis was conducted according to duration of
intervention. Stata 12.0 software (StataCorp, LP, College Sta-
tion, TX, USA)was used to perform an Egger's linear regressionanalysis and construct a funnel plot to assess publication bias.
For all results, a p < 0.05 was considered statistically
significant.
3. Results
3.1. Study identification and selection
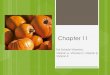
The initial search identified 312 articles, which were system-
atically sorted using EndNote (version 7.1) software (Thomson
Reuters, New York, NY, USA). Of these, 112 articles were
eliminated due to duplication and 103 were excluded after
screening the title and abstract. The full-text of the remaining
studies were examined, and 57 studies were excluded because
their topic of study did not meet our inclusion criteria. Thus,
40 studies [9e48] were eligible for inclusion in the meta-
analysis (Fig. 1).
3.2. Study characteristics
The characteristics of the included studies are shown in Table
1. The studies were published between 2007 and 2015, and all
were planned and performed by researchers in China. The
sample size of each study ranged from 50 to 320 for a total of
3497 patients.
3.3. Risk of bias
Of all included studies, 14 [9,12,17,24,27,35e39,43e45,48] con-
ducted appropriate randomization methods, such as the use
of random number table; one study [38] utilized a sealed
opaque envelope and a specific coordinator to carry out the
randomization of group assignment. Only one study [45]
utilized blinding of the investigators. Although the number
and reason for study dropout were reported in three studies
[17,38,39], intention-to-treat was not adopted to analyze the
results. Nine [9,12,13,16,22e25,30] studies did not report the
results of the outcomemeasures of interest. An assessment of
risk of bias indicated that the overall quality of the included
studies was low (Table 1).
3.4. Total effective rate
A total of 37 studies [9e11,13e33,35e47] comprising 3289 pa-
tients reported the total effective rate. A fixed effects model
was used to calculate the summary effect estimate, as no
clinical characteristics or methodological differences were
detected among these studies and there was no significant
heterogeneity (I2 ¼ 0%, p ¼ 0.53). The results indicated a sig-
nificant difference between groups treated with Western
medicine plus TCM fumigation and Western medicine alone
(RR ¼ 1.34; 95% CI: 1.29e1.39; p < 0.01).
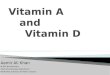
Subgroup analyses of this outcome were conduced based
on the duration of intervention (Fig. 2). Nine studies
[11,13e17,42,46,47] comprising 627 patients reported the 15-
day total effective rate. There was no significant heterogene-
ity among these studies (I2 ¼ 0%, p ¼ 0.52), therefore, a fixed
effects model was used. The pooled result indicated that the
addition of TCM fumigation significantly improved the treat-
ment of DPN patients (RR ¼ 1.31, 95% CI: 1.21e1.42; p < 0.01).
Similar results were found with additional subgroup analyses
for treatments after 20 days, 30 days, 40 days, and 60 days (all
p < 0.01). Only one study [10] determined the total effective
rate 10 days after implementing interventions and found no
significant difference between TCM fumigation and Western
medicine alone.
3.5. Nerve conduction velocity
Common peroneal motor nerve conduction velocity was re-
ported in twelve of the included studies [19,28,29,31e38,40],
which were divided into three subgroups according to when
the evaluations were conducted after implementing in-
terventions: 30 days [19,28,29], 40 days [31e33], and 60 days
[34e38]. Significant heterogeneity was only detected in the 30-
day subgroup (I2 ¼ 94%, p < 0.01), thus the random effects
model was used for this evaluation. The results of thesemeta-
analyses showed that supplementation of Western medicine
with TCM fumigation significantly improved common pero-
neal motor nerve conduction velocity in patients with DPN (all
p < 0.05) (Table 2). Similar effects were found with studies
evaluating the conduction velocities in the median and tibial
nerves (both p < 0.01).
Sensory nerve conduction velocity was evaluated in the
common peroneal nerve after 40 days in two studies [31,32]
and after 60 days of treatment in six studies [34e38,40]. No
statistical heterogeneity was detected, therefore, a fixed ef-
fects model was used. The results indicated that TCM fumi-
gation significantly improved common peroneal sensory
nerve conduction velocity in patients with DPN (both p < 0.01)
(Table 2). Similar effects were found with studies evaluating
the conduction velocities in the median sensory nerve (both
p < 0.01).

Records iden fied through database searching
(n = 306)
Screen
ing
Includ
edEligibility
Iden
fica
on
Addi onal records iden fied through other sources
(n = 6)
Records a er duplicates removed
(n = 200)
Records screened(n = 97)
Records excluded(n = 103)
Full-text ar cles assessed for eligibility
(n = 40)
Full-text ar cles excluded:
non-RCTs (n = 19)Duplica ons (n = 21)Interven on did not conform with inclusion criteria (n = 17 )
Studies included in qualita ve synthesis
(n = 40)
Studies included in quan ta ve synthesis
(meta-analysis)(n = 39)
Fig. 1 e Flowchart of the study selection. RCT ¼ randomized controlled trial.
i n t e r n a t i o n a l j o u rn a l o f n u r s i n g s c i e n c e s 2 ( 2 0 1 5 ) 2 9 5e3 0 3298
3.6. Vibration perception threshold
Two studies [14,48] including 128 patients reported vibration
perception thresholds assessed 15 days after initiating ther-
apy. There was no significant heterogeneity between the
studies (I2 ¼ 0%, p ¼ 0.58), therefore, a fixed effects model was
used. The results showed that there was no significant dif-
ference between TCM fumigation and Western medicine
compared to Western medicine alone in reducing the vibra-
tion perception threshold (mean difference ¼ �1.53, 95% CI:
�3.65e0.59; p ¼ 0.16).
3.7. Plasma viscosity
Two studies [35,39] including 175 patients reported on plasma
viscosity. There was no significant heterogeneity between the
studies (I2 ¼ 0%, p ¼ 0.44), therefore, a fixed effects model was
used. The results indicated that, compared with Western
medicine alone, the addition of TCM fumigation significantly
decreased plasma viscosity in patients with DPN
(SMD ¼ �1.02, 95% CI: �1.35e0.69; p < 0.01).
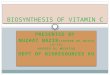
3.8. Publication bias
A funnel plot was constructed to evaluate the potential for
publication bias with regard to the total effective rate. The
results of an Egger's linear regression indicated that there was
no significant publication bias (t ¼ 1.29; p ¼ 0.21) (Fig. 3).
4. Discussion
The increase in the prevalence of diabetes mellitus has led to
an increase in the incidence of DPN [5]. This loss of sensation
from the neuropathy can seriously reduce the patient's qualityof life, as well as lead to diabetic foot ulcers and gangrene, or
even amputation [49]. Although the pathogenesis of DPN is
complex, it is influenced by factors such as metabolism, blood
vessels, neurotrophins, and oxidative stress [50]. As a conse-
quence, effective treatments are urgently needed.
A multitude of Western medicines have been developed to
control DPN. These include such compounds as a methycobal
[51], which can reduce limb numbness and pain, alpha lipoic

Table 1 e Characteristics and quality of included studies.
Study Number ofpatients (T/C)
Interventions Outcomes Risk of bias
T C Adequatesequencegeneration
Allocationconcealment
Blinding Incompleteoutcome
data
Selectivereporting
Otherbias
Kong C X et al., 2011 [10] 25/25 A þ B B( ) I U U U Yes Yes U
Xiao J H et al., 2013 [11] 30/30 A þ B B( ) I þ II U U U Yes Yes U
Song H L et al., 2011 [12] 40/40 A þ B B( ) II Yes U U Yes No U
Wan L et al., 2008 [13] 30/30 A þ B B( ) I þ II U U U Yes No U
Liu T et al., 2012 [48] 34/34 A þ B B( ) IV Yes U U Yes Yes U
Xiong XD et al., 2013 [14] 30/30 A þ B B( ) I þ IV U U U Yes Yes U
Hu G et al., 2012 [15] 25/25 A þ B B( ) I U U U Yes Yes U
Che S S et al., 2010 [16] 60/58 A þ B B( ) I U U U Yes No U
Shen et al.,L X 2012 [17] 34/30 A þ B B( ) I þ II Yes U U No Yes U
Huang et al., P 2008 [27] 64/64 A þ B B( ) I þ II Yes U U Yes Yes U
Chen J et al., 2009 [18] 30/30 A þ B B( ) I U U U Yes Yes U
Gao M S et al., 2011 [19] 42/42 A þ B B( ) I þ II U U U Yes Yes U
Zhang XN et al., 2013 [20] 20/20 A þ B B( ) I þ III þ IV U U U Yes Yes U
Hu X J et al., 2013 [21] 160/160 A þ B B( ) I þ IV U U U Yes Yes U
Hao D et al., 2011 [22] 51/47 A þ B B( ) I U U U Yes No U
Huang Z et al., 2007 [23] 40/38 A þ B B( ) I U U U Yes No U
Zhang S F et al., 2013 [24] 60/60 A þ B B( ) I Yes U U Yes No U
Hu X L et al., 2007 [25] 40/38 A þ B B( ) I U U U Yes No U
Wang Y F et al., 2011 [26] 30/30 A þ B B( ) I U U U Yes Yes U
Zhu N et al., 2012 [9] 56/56 A þ B B( ) I Yes U U Yes No U
Chen J Y et al., 2009 [28] 40/40 A þ B B( ) I þ II U U U Yes Yes U
Li Q et al., 2009 [29] 150/150 A þ B B( ) I þ II U U U Yes Yes U
Li Q et al., 2010 [30] 30/30 A þ B B( ) I U U U Yes No U
Ding Y et al., 2011 [31] 50/50 A þ B B( ) I þ II U U U Yes Yes U
Fan G J et al., 2010 [32] 34/28 A þ B B( ) I þ II U U U Yes Yes U
Meng QH et al., 2010 [33] 40/40 A þ B B( ) I þ II U U U Yes Yes U
Wang ZX et al., 2012 [34] 30/30 A þ B B( ) II U U U Yes Yes U
Qiu X T et al., 2013 [35] 80/40 A þ B B( ) I þ II þ III Yes U U Yes Yes U
Hou S F et al., 2010 [36] 30/30 A þ B B( ) I þ II Yes U U Yes Yes U
Xu Q S et al., 2009 [37] 30/30 A þ B B( ) I þ II Yes U U Yes Yes U
Li M D et al., 2009 [38] 31/30 A þ B B( ) I þ II Yes Yes U No Yes U
Guan Y H et al., 2009 [39] 28/27 A þ B B( ) I þ III þ IV Yes U U No Yes U
Wu X et al., 2014 [40] 40/40 A þ B B( ) I þ II U U U Yes Yes U
Shao G J et al., 2015 [41] 35/33 A þ B B( ) I U U U Yes Yes U
Su W B et al., 2014 [42] 42/42 A þ B B( ) I þ II U U U Yes Yes U
Qin Y et al., 2015 [43] 34/34 A þ B B( ) I þ IV Yes U U Yes Yes U
Pan Z W et al., 2014 [44] 60/60 A þ B B( ) I Yes U U Yes Yes U
Li Y X et al., 2015 [45] 30/30 A þ B B( ) I Yes No Yes Yes Yes U
Liu M et al., 2015 [46] 36/35 A þ B B( ) I U U U Yes Yes U
Chen Y F et al., 2015 [47] 30/30 A þ B B( ) I U U U Yes Yes U
A ¼ traditional chinese medicine fumigation; B¼ common therapy including foundational treatments (insulin, diet, sports, health education) andWestern medicine; C¼ control group; I¼ total effect
rate; II ¼ nerve conduction velocity; III ¼ blood viscosity; IV ¼ vibration perception thresholds; T ¼ experimental group; U ¼ unclear.
Western Medicines: Oral methycobal; Intramuscular methycobal; Intravenous drip alprostadil; Intravenous drip alpha lipoic acid; Intravenous drip methycobal; Intravenous drip lig-
ustrazine; Intravenous push note methycobal; Intramuscular vitamin B1; Intramuscular vitamin B6; Oral vitamin B1; Oral vitamin B6; Oral epalrestat.
internatio
naljo
urnalofnursin
gscie
nces
2(2
015)295e303
299

Fig. 2 e Forest plots showing results of meta-analyses comparing patients treated with Traditional Chinese and Western
medicines (experimental) and Western medicine alone (control).
i n t e r n a t i o n a l j o u rn a l o f n u r s i n g s c i e n c e s 2 ( 2 0 1 5 ) 2 9 5e3 0 3300

Table 2 e Meta-analyses on nerve conduction velocity.
Outcomes Included studies No.of patients
Effect size Heterogeneity Test for overall effect
n Ref. MD/SMD (95%CI) c2 value p value I2 Z value p value
Motor nerve conduction velocity
Common peroneal nerve
After 30 days of treatmenta 3 [19,28,29] 464 4.72 (0.41e9.03) 32.40 <0.01 94% 2.15 0.03
After 40 days of treatment 3 [31e33] 242 3.45 (2.85e4.05) 0.80 0.67 0% 11.30 <0.01After 60 days of treatment 6 [34e38,40] 441 2.93 (2.26e3.61) 8.75 0.12 43% 8.52 <0.01Median nerve
After 15 days of treatment 2 [11,13] 120 10.23 (8.74e11.72) 0.50 0.48 0% 13.45 <0.01Tibial nerve
After 30 days of treatmenta 3 [19,28,29] 464 4.73 (2.18e7.28) 10.27 <0.01 81% 3.64 <0.01Sensory nerve conduction velocity
Common peroneal nerve
After 40 days of treatment 2 [31,32] 168 2.30 (1.30e3.30) 0.08 0.78 0% 4.50 <0.01After 60 days of treatment 6 [34e38,40] 441 2.23 (1.46e3.01) 2.61 0.76 0% 5.64 <0.01Median nerve
After 40 days of treatment 2 [31,32] 168 2.50 (1.29e3.71) 1.10 0.29 9% 4.05 <0.01After 60 days of treatment 4 [35e37,40] 320 2.63 (1.68e3.58) 2.56 0.46 0% 5.41 <0.01
CI ¼ confidence interval; MD ¼ mean difference; SMD ¼ standard mean difference.a Random-effects model.
i n t e r n a t i o n a l j o u r n a l o f nu r s i n g s c i e n c e s 2 ( 2 0 1 5 ) 2 9 5e3 0 3 301
acid [52], an antioxidant that helps restore nerve function, and
alprostadil [53], which improves circulation and thus pro-
motes recovery of nerve function. Interestingly, a recent
meta-analysis concluded that supplementation of Western
medicines with TCM decoction significantly improved treat-
ments for DPN [54]. The results of the current meta-analysis
support these findings, showing that TCM fumigation can
also significantly improve patient outcomes, specifically, the
total effective rate and limb sensory and motor nerve con-
duction velocities.
Diabetes mellitus belongs to the “Xiaoke” category within
TCM, with corresponding neurologic complications classified
as “Bizheng,” “Xuebi,” and “Weizheng.” In the TCM system,
DPN is characterized by pain, numb, stasis, and stubborn, and
is termed “Xiaoke-Bizheng.” [5] It is further divided into five
subtypes based on various pathogeneses, such as “deficiency
of both qi and yin,” “phlegm stasis Bizu,” “blood stasis
obstructing the collaterals,” “yang deficiency and cold,” and
“liver-wind stirring” [55]. According to the principle of dia-
lectic therapy, TCMs, such as safflower, cassia twig, ferlate,
angelica, and tougucao, were the ones commonly used in the
studies included in this meta-analysis. The reported effects of
Fig. 3 e Funnel plot for publication bias.
these are as follows: safflower activates the blood and
removes stasis, cassia twig warms channels and dredges
collaterals, thus activating yang-fluidizing chi, dispelling the
cold, and relieving pain; angelica alsowarms and activates the
blood to regulate the channels, relieve pain, and can be used
for blood deficiency and stasis; tougucao promotes dehu-
midification, relaxation of the muscles, stimulates blood cir-
culation, and acts as an analgesic [56]. Combinations of these
TCMs have a synergistic effect [57]. Moreover, pharmacologic
research has confirmed that safflower [58,59], cassia twig
[60e62], ferlate [63,64], angelica [65], and tougucao [66] have
analgesic, anti-inflammatory, antianaphylactic, antibacterial,
and antioxidant effects, and reduce blood lipids levels and
viscosity and reduce peripheral vascular resistance.
The results presented here show significant improvement
in almost all outcomes measured. In particular, nerve con-
duction velocities and plasma viscosity were significantly
improved in groups who also received TCM fumigation.
However, two studies [14,48] evaluated vibration perception
thresholds, and found that there was no significant effect of
TCM fumigation. It is possible that the lack of significance was
due to the early assessment (after 15 days), which may not
have been sufficient time to effectively influence vibration
perception thresholds.
There are some limitations of the currentmeta-analysis that
should be noted. First, the TCM fumigation regimes varied
among the included studies, which could potentially influence
the results. Second, assessment of bias was difficult inmany of
the studies because of unclear and inadequate descriptions of
methodologies. Overall, thequality of the studieswasquite low.
Thus, additional, high-quality studies are needed to more
accurately assess the benefits of TCM fumigation.
5. Conclusion
The results of this systematic review andmeta-analysis show
that supplementation of Western medicine with TCM

i n t e r n a t i o n a l j o u rn a l o f n u r s i n g s c i e n c e s 2 ( 2 0 1 5 ) 2 9 5e3 0 3302
fumigation significantly improves DPN patient outcomes.
TCM fumigation improved the total effective rate, nerve con-
duction velocity, and plasma viscosity within 15 days of
treatment. However, these results should be interpreted with
caution due to the low quality of included studies. Additional,
high-quality, large-scale randomized controlled trials are
warranted to confirm these beneficial effects.
Contributors
Lei Zhang, Xu Tian, Yue Ma, Ying-Hui Jin, and Fan-Jie Meng
conceived of and designed the protocol. Lei Zhang, Xu Tian,
and Yue Ma searched and selected the studies. Lei Zhang and
Xu Tian collected and analyzed the data. Lei Zhang, Xu Tian,
and Ying-Hui Jin wrote the manuscript. All authors carefully
reviewed the manuscript and approved this submission.
Competing interests
These authors have declared that there are no competing
interests.
r e f e r e n c e s
[1] Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM,et al. The prevalence by staged severity of various types ofdiabetic neuropathy, retinopathy, and nephropathy in apopulation-based cohort: the Rochester Diabetic NeuropathyStudy. Neurology 1993;43:817e24.
[2] Prompers L, Schaper N, Apelqvist J, Edmonds M, Jude E,Mauricio D, et al. Prediction of outcome in individuals withdiabetic foot ulcers: focus on the differences betweenindividuals with and without peripheral arterial disease. TheEURODIALE Study. Diabetologia 2008;51:747e55. http://dx.doi.org/10.1007/s00125-008-0940-0.
[3] Boulton AJ, Vinik AI, Arezzo JC, Bril V, Feldman EL,Freeman R, et al. Diabetic neuropathies: a statement by theAmerican Diabetes Association. Diabetes Care2005;28:956e62.
[4] Liu GW. Effect of cobamamide on diabetic neuropathies.Chin Med J Engl 1998;38:14e7.
[5] Li JH. Study on the curative effects and mechanisms ofwenjingtongluo xunxifang to diabetes mellitus peripheralneuropathy disease patients. Guangzhou University ofTraditional Chinese Medicine; 2008.
[6] Moher D, Liberati A, Tetzlaff J, Altman DG. Preferredreporting items for systematic reviews and meta-analyses:the PRISMA statement. Int J Surg 2010;8:336e41. http://dx.doi.org/10.1016/j.ijsu.2010.02.007.
[7] Higgins JPT, Green S. Cochrane handbook for systematicreviews of interventions version 5.1.0 (updated March 2011).2008.
[8] Lv RH. The diagnosis and treatment of Chinese and westernmedicine of II-diabetic and complications. 1997. p. 390e4.
[9] Zhu N, Cao XM, Fang CH. The observation of Chinesemedicine embalm wash party coalition cobamamide treatingdiabetic peripheral neuropathy 56 cases. Yunnan J TraditChin Med 2012;33:32e3.
[10] Kong CX, Chen W. The clinical effect of the treatmenttraditional Chinese medicine medicated bath of diabeticperipheral neuropathy. Seek Med Ask Med 2011;9:347.
[11] Xiao JH, Wang X, Qiao P. The clinical experience oftraditional Chinese medicine fumigation treatment ofdiabetic peripheral neuropathy of 60 cases. Cap Med2013;7:82e3.
[12] Song HL. Clinical observation on treating lower extremitydiabetic peripheral neuropathy by TCM fumigation. Clin JChin Med 2011;3:1e2.
[13] Wan L, Pan SB. The Chinese medicine fumigation auxiliarytreatment of diabetic peripheral neuropathy. Hubei J TraditChin Med 2008;30:30e1.
[14] Xiong XD. Efficacy of Chinese medicine fumigationcombination of alpha lipoic acid of vibration sensorythresholds in patients with diabetic peripheral neuropathy.World Heal Dig Med Period 2013;10:402e3.
[15] Hu G. The treatment of Tougu scattered fumigationcombined a cobamamide of diabetic peripheral neuropathy.Shanxi J Tradit Chin Med 2012;28:42e3.
[16] Che SS. The nursing experience of Chinese medicinefumigation auxiliary in treating diabetic peripheralneuropathy. J Emerg Tradit Chin Med 2010;12:528e9.
[17] Shen LX. The clinical observation a cobamamide combinedtraditional Chinese medicine for the treatment of diabeticperipheral neuropathy. J Pract Diabetol 2012;8:42e4.
[18] Chen J, Sang W, Zheng CH. The clinical observation oftongluo fumigation on treatment of diabetic peripheralneuropathy. J Pract Tradit Chin Intern Med 2009;23:58e9.
[19] Gao MS, Peng C, Tan Y. A summary of Chinese medicinefumigation combined with cobamamide of treating diabeticperipheral neuropathy in 42 cases. Guid J Tradit Chin MedPharm 2011;17:52e3.
[20] Zhang XN, Zhang XK, Li RY. Chinese medicine fumigation inthe treatment of type 2 diabetes peripheral neuropathy 40cases. J Shanxi Coll Tradit Chin Med 2011;4:61e2.
[21] Hu XJ, Yang HX, Li T, Li XH. Tongluo Zhitong No.1 fumigationtreatment of 320 cases of diabetic peripheral neuropathy. JShanxi Tradit Chin Med 2013;34:44e6.
[22] Hao D. Chinese fumigation treatment of 98 cases of diabeticperipheral neuropathy. J Pract Tradit Chin Intern Med2011;25:63e4.
[23] Huang Z. Chinese medicine fumigation auxiliary treatmentof 40 cases of diabetic peripheral neuropathy. J ZhejiangTradit Chin Med 2007;42:435.
[24] Zhang SF, Pan ZW, Qian CF, Tan XD, Liang HM. Xibifangfumigation combined with western medicine inrandomized parallel control study on treatment of diabeticperipheral neuropathy. J Pract Tradit Chin Intern Med2013;27:95e6.
[25] Hu XL. The observation and nursing of traditional Chinesemedicine fumigation for diabetes peripheral neuropathy oflower limbs. Tianjin J Nursin 2007;15:275e6.
[26] Wang YF. The curative effect of Yiqi huoxue tongluofumigation of diabetic peripheral neuropathy. Chin ForeignMed Res 2011;9:59e60.
[27] Huang P, Zheng JH. The western medicine combinedtraditional Chinese medicine fumigation for the treatment of64 cases of type 2 diabetes peripheral neuropathy. J PractMed 2008;24:853e4.
[28] Chen JY, Ying ZH. Chinese medicine fumigation incombination with cobamamide: a clinical observation ontreatment of diabetic peripheral neuropathy. J Emerg TraditChin Med 2009;19:901.
[29] Li Q, Wu Q, Wu WD, Cao YY, Xiong L. The treatment ofChinese medicine fumigation of 150 cases diabeticperipheral neuropathy. Yunnan J Tradit Chin Med2009;30:26e8.
[30] Li Q, Xu YP. Chinese medicine fumigation care for thetreatment of diabetic peripheral neuropathy. Yunnan J TraditChin Med 2010;31:73e4.

i n t e r n a t i o n a l j o u r n a l o f nu r s i n g s c i e n c e s 2 ( 2 0 1 5 ) 2 9 5e3 0 3 303
[31] Ding Y. Chinese medicine wash outside on treatment of 50cases of diabetic peripheral neuropathy: a clinicalobservation. J Trait Med 2011;23:140e1.
[32] Fan GJ, Tang XY, Liu ZH, Wei H, He L, Zou DY, et al. Theclinical observation of traditional Chinese medicinecombination of cobamamide on treatment of diabeticperipheral neuropathy. J New Chin Med 2010;42:27e8.
[33] Meng QH, Chen JL. The cobamamide combined withtraditional Chinese medicine bubble foot in treatment ofdiabetic peripheral neuropathy: a clinical observation. Clin JTradit Chin Med 2010;22:675e6.
[34] Wang ZX, Qian Q, Liang YW, Hu J, Xia WW, Jin J. Study theeffect of huangqi guizhi wuwu tang fumigation treatment ofdiabetic peripheral neuropathy. Mod Hosp 2012;12:21e4.
[35] Qiu XT, Zhang YJ. A clinical observation on traditionalChinese medicine fumigation treatment of diabeticperipheral neuropathy. Chin J Chin Med Inf TCM2013;20:74e5.
[36] Hou SF, Huang SL, Guan GD. Fracture lotion fumigation No.1combined with cobamamide: a clinical observation of 30cases of diabetic peripheral neuropathy. Guang Ming J ChinMed 2010;25:1063.
[37] Xu QS, Lu LY, Zhang HL. The medicated bath foot combinedwith cobamamide treatment of diabetic peripheralneuropathy 30 cases. J Jiangxi Tradit Chin Med 2007;40:33e4.
[38] Li MD, Lin L, Sun SC, Ni Q, Su H. Clinical study of Chineseherb formula tangtongfang by bathing the affected feet withdiabetic peripheral neuropathy. Chin J Rehabil Theory Pract2009;15:553e5.
[39] Guan YH. The observation of clinical effect tougusanfumigation therapy on patients with deficiency of both Qiand Yin with blood stasis and diabetic peripheralpolyneuropathy. Nanjing University of Chinese Medicine;2009.
[40] Wu X, Luo DZ, Wang QH. A research of Chinese medicinewith prostaglandin for diabetic peripheral neuropathy. JPract Tradit Chin Med 2014;30:535e6.
[41] Shao GJ, Wang XJ. TCM fumigation and epalrestat intreatment of diabetic peripheral neuropathy. Liaoning JTradit Chin Med 2015;42:291e2.
[42] Su WB, Li ZY, Liu XC. A clinical research of TCM fumigationfor diabetic peripheral neuropathy. Lishizhen Med MaterMedica Res 2014;25:2714e6.
[43] Qin Y, Hu XJ. Western medicine combined dredgingcollaterals analgesic powder no. 2 for diabetic peripheralneuropathy of 68 patients. J Pract Tradit Chin Med2015;30:410.
[44] Pan ZW, Zhang SF, Tan XD. The effect of Xiaobifang intreatment of 2-diabetes mellitus peripheral neuropathy. NewJ Tradit Chin Med 2014;46:128e9.
[45] Li YX. TCM fumigation for the treatment of Xiaokebizheng.Res Integr Tradit Chin West Med 2015;7:23e4.
[46] Liu M, Zhang XK. TCM fumigation witha-lipoic acid for thetreatment of diabetic peripheral neuropathy of 36 patients. JPract Tradit Chin Med 2015;31:232e3.
[47] Chen YF, Du YH, Huo Y. The effect of TCM fumigation fordiabetic peripheral neuropathy of 30 patients. Yunnan JTradit Chin Med Mater Medica 2015;36:39e40.
[48] Liu T, Huang Z, Wei AS, Mai WH, Liang XF. The randomparallel control study of total symptoms score (TSS) andvibration perception threshold in diabetic peripheralneuropathy patients treated with Chinese herb fumigationcombined with alpha lipoic acid. J Pract Med Tradit ChinIntern Med 2012;26:57e9.
[49] Lu ZQ. Progress in diagnosis and treatment of diabeticperipheral neuropathy. Drug Eval 2013;10:35e45.
[50] Liu YL. A review of pathogenesis and treatment of diabeticperipheral neuropath. Youjiang Med J 2011;33:356e8.
[51] Li G. Effect of mecobalamin on diabetic neuropathies. Beijingmethycobal clinical trial Collaborative group. Zhonghua NeiKe Za Zhi 1999;38:14e7.
[52] Scaramuzza A, Giani E, Redaelli F, Ungheri S, Macedoni M,Giudici V, et al. Alpha-lipoic acid and antioxidant diet help toimprove endothelial dysfunction in adolescents with type 1diabetes: a pilot trial. J Diabetes Res 2015;2015:474561. http://dx.doi.org/10.1155/2015/474561.
[53] Luo C, Li T, Zhang C, Chen Q, Li Z, Liu J, et al. Therapeuticeffect of alprostadil in diabetic nephropathy: possible roles ofangiopoietin-2 and IL-18. Cell Physiol Biochem2014;34:916e28. http://dx.doi.org/10.1159/000366309.pii:000366309.
[54] Xu ZY. Effect of Chinese decoction therapy for diabeticperipheral neuropathy: a meta-analysis. Liaoning Universityof Chinese Medicine; 2013.
[55] Wu Y. Clinical effects of quyutongluo washing decoction onpatients with diabetic peripheral neuropathy. HubeiUniversity of Chinese Medicine; 2011.
[56] Gao XM. Traditional Chinese pharmacology. 2002.[57] Liu Y, Ding HS. Class tougucao progress in the study of
traditional Chinese medicine. Inf Tradit Chin Med1999;16:10e2.
[58] Yang ZF, Mei QB, Jiang YP. Active constituents andpharmacological effects of safflower. Northwest Pharm J2001;16:131e3.
[59] Zhao G, Wan AH. Safflower resource and its medicinal value.Chin Wild Plant Resour 2004;23:24e5.
[60] Zhao JH, Liu SY. Pharmacological action and clinical of cassiatwig. Med Inf 2011;24:1575.
[61] Zhao JY. New pharmacological research and clinical use ofcassia twig. Guang Ming J Chin Med 2010;25:1546.
[62] Zhao Y. A discussion of cassia twig of modern pharmacologyand clinical application. Chin Med Mod Distance Educ China2009;7:77e8.
[63] Li QY, Gan GP, Liu YW. Chemical components andpharmacological research progress of rhizoma ligusticiwallichii. Lishizhen Med Mater Med Res 2006;17:1298.
[64] Qu P. Ligustici wallichii pharmacological effects: a review.Inn Mong J Tradit Chin Med 2010;29:78e9.
[65] Xia Q, Zhang P, Zhang SP, Wang YT. Pharmacological effectsof angelica sinennsis: a review. Lishizhen Med Mater MedRes 2004;15:164e6.
[66] Wang X, Xiao ZP. Comparative studies of Chinese drugtougucao on anti-inflammatory and analgesic effects. JBeijing Med Univ 1998;30:145e7.