Embed Size (px)
Citation preview

ORIGINAL PAPER
Efficacy of Amlodipine and Olmesartan Medoxomil in HypertensivePatients With Diabetes and Obesity
Henry Punzi, MD;1 Ali Shojaee, PharmD;2 William F. Waverczak, MS;2 Jen-Fue Maa, PhD2
From the Trinity Hypertension Research Institute, Punzi Medical Center, Carrollton, TX;1 and Daiichi Sankyo, Inc, Parsippany, NJ2
A subgroup analysis of a prospective, open-label, single-arm titration study in patients with hypertension and type 2diabetes or obesity is reported. The primary end point wasthe change from baseline in mean 24-hour ambulatory sys-tolic blood pressure (BP) after 12 weeks. Patients receivedamlodipine 5 mg ⁄ d and were uptitrated (if seated [Se] BPwas �120 ⁄ 80 mm Hg) at 3-week intervals to amlodi-pine ⁄ olmesartan medoxomil 5 ⁄ 20 mg ⁄ d, 5 ⁄ 40 mg ⁄ d, and10 ⁄ 40 mg ⁄ d. In patients with diabetes and obesity, base-line 24-hour ambulatory BP (�standard deviation) was145.6�10.4 ⁄ 83.1�9.0 mm Hg and 143.7�9.8 ⁄ 84.9�8.2mm Hg, respectively, and baseline SeBP was 159.1�11.3 ⁄ 90.3�9.2 mm Hg and 158.2�12.5 ⁄ 94.2�8.5 mm Hg,
respectively. Changes from baseline in mean 24-hourambulatory BP (�standard error of the mean) were)21.5�1.8 ⁄ )12.6�1.1 mm Hg and 21.6�1.1 ⁄ 13.4�0.8 mmHg in patients with diabetes and obesity, respectively. Pre-specified 24-hour ambulatory BP targets of <130 ⁄ 80 mmHg, <125 ⁄ 75 mm Hg, and <120 ⁄ 80 mm Hg were achievedby 79.1%, 53.5%, and 39.5% of patients with diabetesand 75.3%, 58.4%, and 43.8% of obese patients, respec-tively. The SeBP goal of <130 ⁄ 80 mm Hg was achieved by26.1% of patients with diabetes and <140 ⁄ 90 mm Hg wasachieved by 78.1% of obese patients. J Clin Hypertens(Greenwich). 2011;13:422–430. �2011 Wiley Periodicals,Inc.
The growing epidemic of obesity and obesity-relatedhypertension parallels the increased prevalence of themetabolic syndrome (MS) and type 2 diabetes.1,2
Among US adults, the incidence of diagnosed diabetesincreased by 41% from 4.9 to 6.9 per 1000 from1997 to 2003 (P<.01).3 Data from the 2003–2004National Health and Nutrition Examination Surveyrevealed that up to 76.8% of patients with diabetesand 61.5% of patients with the MS (without diabetes)have hypertension.4 However, only one third ofpatients with diabetes and just less than one half ofpatients with the MS receiving antihypertensive treat-ment achieve a recommended seated cuff blood pres-sure (SeBP) goal.4 Every 10-mm Hg reduction in SeBPreduces the risk of any diabetes-related cardiovascularcomplication by 12%.5
Hypertension treatment guidelines in the UnitedStates and Europe now recommend initiating treat-ment with 2 drugs when BP levels are �20 ⁄ 10 mm Hgabove the desired goal.6–8 Regimens that includeangiotensin-converting enzyme (ACE) inhibitors orangiotensin II receptor blockers (ARBs), plus a thiazidediuretic if necessary, are recommended.6,7 Recent find-ings challenge the guideline recommendation thatfavors the use of diuretics. In the Avoiding Cardiovas-cular Events Through Combination Therapy inPatients Living With Systolic Hypertension (ACCOM-PLISH) trial, treatment with the ACE inhibitor bena-zepril combined with amlodipine was superior to
benazepril ⁄ hydrochlorothiazide (HCTZ) in reducingcardiovascular morbidity and mortality (relative risk,0.80; 95% confidence interval [CI], 0.71–0.90).9
Several large randomized controlled trials havereported a greater incidence of new-onset diabetes inpatients receiving HCTZ, other diuretics, or b-block-ers compared with patients receiving ACE inhibitors,calcium channel blockers (CCBs), or ARBs.9–14 Asthe number of insulin-resistant patients with hyper-tension continues to increase, it is increasinglyimportant to consider therapies that may preventnew-onset diabetes when choosing antihypertensiveagents.14
Another important criterion for the selection of ahypertensive regimen is whether BP control is main-tained throughout a 24-hour dosing period. This mini-mizes the impact of the morning BP surge, which canbe an important trigger of cardiovascular events.15
Ambulatory BP monitoring (ABPM) can be used tomonitor responses to therapy during a 24-hour periodand also during defined time periods.16,17
This report presents a subgroup analysis of theAZOR Trial Evaluating Blood Pressure Reduction andControl (AZTEC), which was a prospective, open-label clinical trial that used ABPM to assess the effi-cacy and safety of an amlodipine (AML) and olmesar-tan medoxomil (OM) step-wise titration regimen inpatients with hypertension.18 AZTEC showed that thiscombination regimen was well tolerated and producedrobust mean 24-hour ambulatory BP reductions of21.4 ⁄ 12.7 mm Hg from baseline, which were main-tained throughout the dosing interval. The presence orabsence of MS was not assessed during enrollmentinto AZTEC. However, the efficacy of the treatmentregimen was evaluated in the present prespecified sub-
Address for correspondence: Henry A. Punzi, MD, Punzi MedicalCenter, 1932 Walnut Plaza, Carrollton, TX 75006E-mail: [email protected]
Manuscript received: December 17, 2010; Accepted: December 17,2010DOI: 10.1111/j.1751-7176.2010.00422.x
422 The Journal of Clinical Hypertension Vol 13 | No 6 | June 2011 Official Journal of the American Society of Hypertension, Inc.

group analysis of patients with or without type 2diabetes and post hoc analysis of obese (body massindex [BMI] �30 kg ⁄ m2) and nonobese patients.
METHODS
Study Design and PatientsAZTEC was a 15- to 16-week prospective, open-label,single-arm titration study conducted at 18 clinical sitesin the United States. Extensive inclusion and exclusioncriteria have been published previously.18 Patients withseated cuff systolic BP (SeSBP) �140 mm Hg and�199 mm Hg or seated cuff diastolic BP (SeDBP) �90mm Hg or �109 mm Hg and a difference of �15 mmHg between SeSBP at the last two consecutive visitsduring the placebo run-in were eligible. Additionally,participants had a mean daytime 8-hour ambulatorysystolic BP (SBP) of �135 mm Hg and �199 mm Hgand ambulatory diastolic BP (DBP) of <110 mm Hgat the completion of the placebo run-in. Patients withtype 1 diabetes were excluded, as were patients withtype 2 diabetes unless they were stable on treatmentfor �4 weeks and had a fasting plasma glucose<160 mg ⁄ dL at screening. Patients were classified asobese if baseline BMI was �30 kg ⁄ m2.
The study consisted of a screening phase, followed bya 3- to 4-week placebo run-in, and a 12-week activetreatment period in which patients initially receivedAML 5 mg ⁄ d for 3 weeks and were uptitrated as neededat 3-week intervals to AML ⁄ OM 5 ⁄ 20 mg ⁄ d followedby AML ⁄ OM 10 ⁄ 40 mg ⁄ d. Patients were uptitrated ifSeBP was �120 ⁄ 80 mm Hg. Patients with SeBP<120 ⁄ 80 mm Hg remained on their current dosageunless they subsequently became uncontrolled (ie, SeS-BP �140 mm Hg and ⁄ or SeDBP �90 mm Hg), in whichcase they were uptitrated.
Efficacy and Tolerability AssessmentsThe primary efficacy end point was the change frombaseline in mean 24-hour SBP after 12 weeks of activetreatment as assessed by ABPM. Secondary end pointsincluded the change from baseline in mean 24-hourambulatory DBP; changes from baseline in meanambulatory SBP and DBP during the daytime (8 AM–4PM), nighttime (12 AM–6 AM), and the last 2, 4, and6 hours of the dosing interval; and the proportions ofpatients achieving various ambulatory BP targets of<130 ⁄ 80 mm Hg, <125 ⁄ 75 mm Hg, and <120 ⁄ 80mm Hg during 24 hours, daytime, and nighttime andthe last 2, 4, and 6 hours of the dosing period. Addi-tional secondary end points were changes from base-line in mean SeSBP and SeDBP at 12 weeks in thetotal cohort and by titration period and the propor-tions of patients achieving SeBP goals of <140 ⁄ 90 mmHg, <130 ⁄ 80 mm Hg, and <120 ⁄ 80 mm Hg by titra-tion period. Adverse events were assessed at eachstudy visit. Routine clinical laboratory tests and physi-cal examinations were performed at screening and atthe end of study or early termination. The safety pop-
ulation comprised all randomized patients whoreceived �1 dose of study medication.
Statistical AnalysisThe intent-to-treat analysis data set (efficacy cohort)was defined as all patients who received �1 dose ofactive study medication and had a baseline and �1post-baseline BP assessment. Patients with both a base-line and week 12 ABPM measurement were includedin all ambulatory BP analyses. Descriptive statisticswere used for categoric variables and summary statis-tics for continuous variables. The primary efficacy var-iable was assessed using a 1-sample t test performedfor the within-group change from baseline to end ofstudy, measured by ABPM. The last-observation-car-ried-forward (LOCF) method was used for SeBP endpoints. For BP targets and BP reduction categories,numbers and percentages of patients were provided.Cumulative percentages were calculated using the totalnumber of patients in the treatment cohort as thedenominator. Analyses were not performed to deter-mine statistical significance of differences betweensubgroups.
RESULTSOf the 325 patients screened, 290 entered the placeborun-in phase and 185 received active treatment. Atotal of 172 patients had both baseline and week 12ABPM measurements and were included in the ambu-latory BP analysis. Baseline demographics for theefficacy cohort are provided in Table I.
Efficacy in the Obese SubgroupA total of 96 patients (52%) were obese (BMI�30 kg ⁄ m2) and 89 (48%) were nonobese (BMI<30 kg ⁄ m2). Baseline mean ages (�standard deviation[SD]) for obese and nonobese patients were 54.9�8.9years and 58.9�9.4 years, respectively. Baseline meanambulatory BP (�SD) for the ABPM cohort was simi-lar for obese and nonobese patients (143.7�9.8 ⁄84.9�8.2 mm Hg and 146.1�12.2 ⁄ 86.6�7.6 mm Hg,respectively). Baseline mean SeBP (�SD) was 158.2�12.5 ⁄ 94.2�8.5 mm Hg and 158.3�12.8 ⁄ 91.4�8.6mm Hg for obese and nonobese patients, respectively.More obese patients had stage 2 hypertension (59.4%)compared with nonobese patients (51.7%). Mostpatients were uptitrated to the maximum dosage ofAML ⁄ OM 10 ⁄ 40 mg ⁄ d (obese, 72.9%; nonobese,71.9%).
Mean 24-hour ambulatory SBP (�standard error ofthe mean [SEM]) reductions from baseline at week 12were 21.6�1.1 ⁄ 13.4�0.8 mm Hg in obese patientsand 21.1�1.2 ⁄)12.0�0.7 mm Hg in nonobese patients(all P<.0001) (Figure 1). Significant reductions inambulatory BP from baseline were seen during thedaytime, nighttime, and during the last 2, 4, and6 hours of the dosing interval for all patients (allP<.0001) (Figure 1). As shown in the 24-hour BP pro-files (Figure 2), the AML ⁄ OM–based regimen reduced
Official Journal of the American Society of Hypertension, Inc. The Journal of Clinical Hypertension Vol 13 | No 6 | June 2011 423
Efficacy of AML and OM in Hypertensive Patients | Punzi et al.
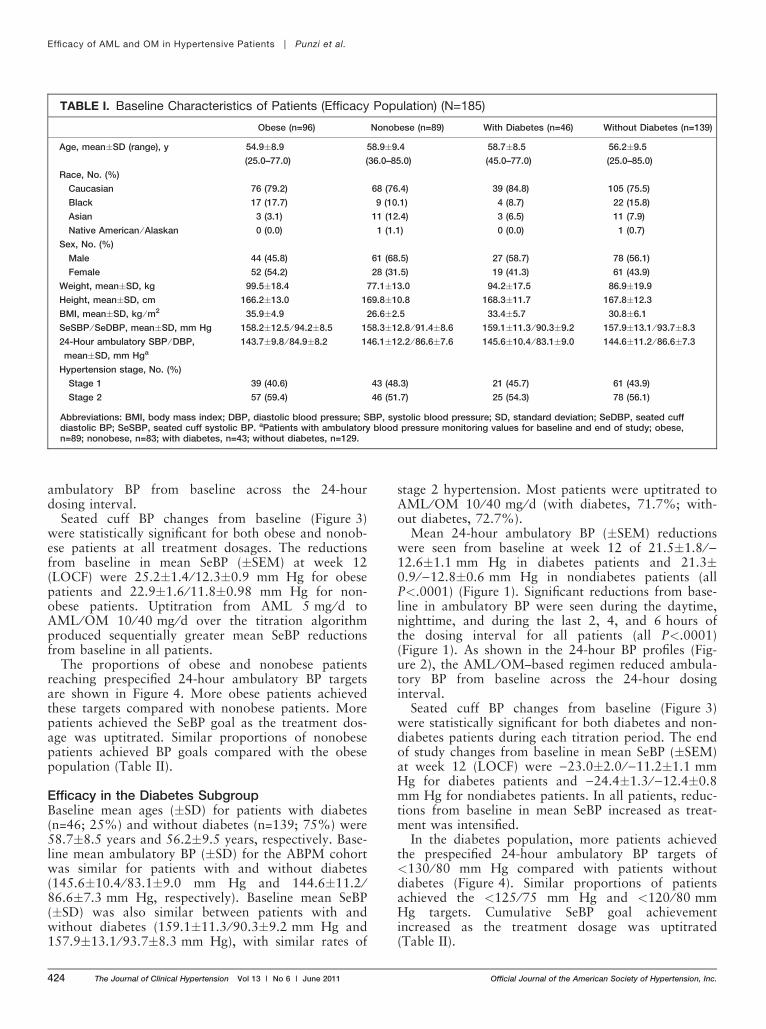
ambulatory BP from baseline across the 24-hourdosing interval.
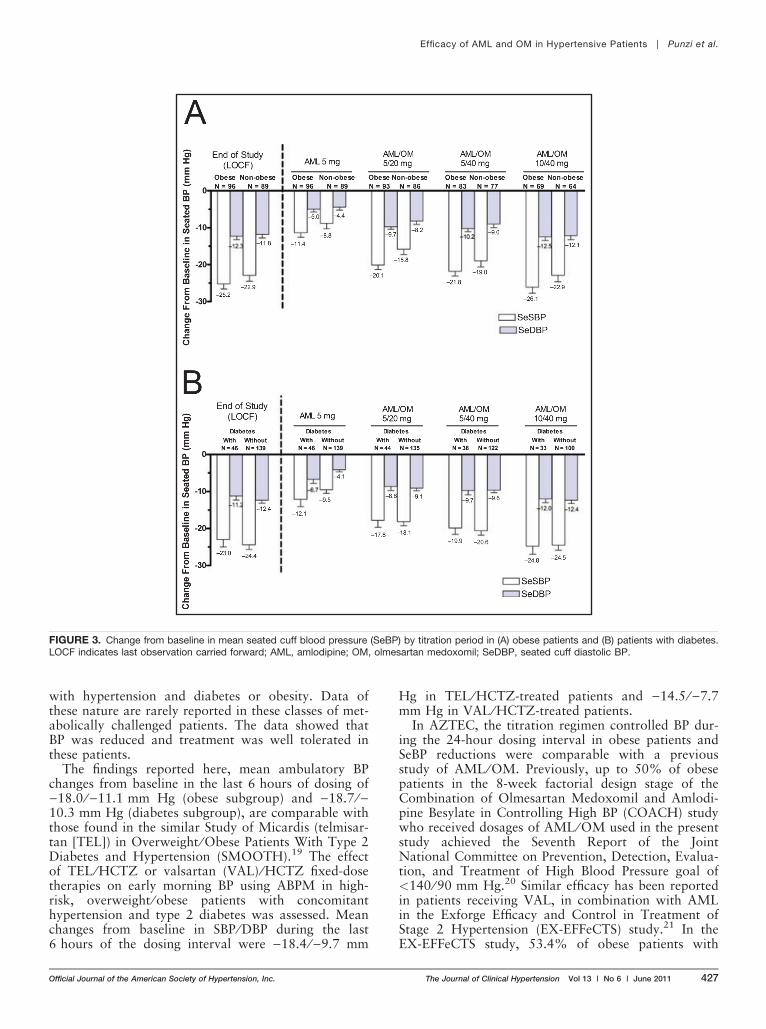
Seated cuff BP changes from baseline (Figure 3)were statistically significant for both obese and nonob-ese patients at all treatment dosages. The reductionsfrom baseline in mean SeBP (�SEM) at week 12(LOCF) were 25.2�1.4 ⁄ 12.3�0.9 mm Hg for obesepatients and 22.9�1.6 ⁄ 11.8�0.98 mm Hg for non-obese patients. Uptitration from AML 5 mg ⁄ d toAML ⁄ OM 10 ⁄ 40 mg ⁄ d over the titration algorithmproduced sequentially greater mean SeBP reductionsfrom baseline in all patients.
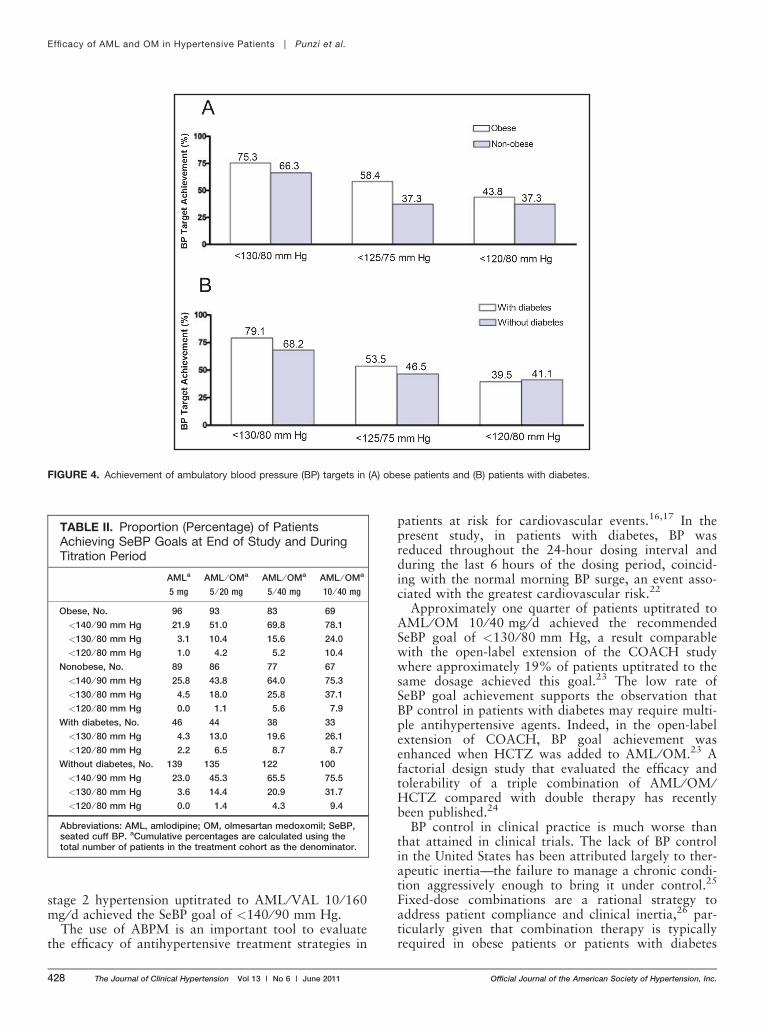
The proportions of obese and nonobese patientsreaching prespecified 24-hour ambulatory BP targetsare shown in Figure 4. More obese patients achievedthese targets compared with nonobese patients. Morepatients achieved the SeBP goal as the treatment dos-age was uptitrated. Similar proportions of nonobesepatients achieved BP goals compared with the obesepopulation (Table II).
Efficacy in the Diabetes SubgroupBaseline mean ages (�SD) for patients with diabetes(n=46; 25%) and without diabetes (n=139; 75%) were58.7�8.5 years and 56.2�9.5 years, respectively. Base-line mean ambulatory BP (�SD) for the ABPM cohortwas similar for patients with and without diabetes(145.6�10.4 ⁄ 83.1�9.0 mm Hg and 144.6�11.2 ⁄86.6�7.3 mm Hg, respectively). Baseline mean SeBP(�SD) was also similar between patients with andwithout diabetes (159.1�11.3 ⁄ 90.3�9.2 mm Hg and157.9�13.1 ⁄ 93.7�8.3 mm Hg), with similar rates of
stage 2 hypertension. Most patients were uptitrated toAML ⁄ OM 10 ⁄ 40 mg ⁄ d (with diabetes, 71.7%; with-out diabetes, 72.7%).
Mean 24-hour ambulatory BP (�SEM) reductionswere seen from baseline at week 12 of 21.5�1.8 ⁄)12.6�1.1 mm Hg in diabetes patients and 21.3�0.9 ⁄)12.8�0.6 mm Hg in nondiabetes patients (allP<.0001) (Figure 1). Significant reductions from base-line in ambulatory BP were seen during the daytime,nighttime, and during the last 2, 4, and 6 hours ofthe dosing interval for all patients (all P<.0001)(Figure 1). As shown in the 24-hour BP profiles (Fig-ure 2), the AML ⁄ OM–based regimen reduced ambula-tory BP from baseline across the 24-hour dosinginterval.
Seated cuff BP changes from baseline (Figure 3)were statistically significant for both diabetes and non-diabetes patients during each titration period. The endof study changes from baseline in mean SeBP (�SEM)at week 12 (LOCF) were )23.0�2.0 ⁄ )11.2�1.1 mmHg for diabetes patients and )24.4�1.3 ⁄)12.4�0.8mm Hg for nondiabetes patients. In all patients, reduc-tions from baseline in mean SeBP increased as treat-ment was intensified.
In the diabetes population, more patients achievedthe prespecified 24-hour ambulatory BP targets of<130 ⁄ 80 mm Hg compared with patients withoutdiabetes (Figure 4). Similar proportions of patientsachieved the <125 ⁄ 75 mm Hg and <120 ⁄ 80 mmHg targets. Cumulative SeBP goal achievementincreased as the treatment dosage was uptitrated(Table II).
TABLE I. Baseline Characteristics of Patients (Efficacy Population) (N=185)
Obese (n=96) Nonobese (n=89) With Diabetes (n=46) Without Diabetes (n=139)
Age, mean�SD (range), y 54.9�8.9
(25.0–77.0)
58.9�9.4
(36.0–85.0)
58.7�8.5
(45.0–77.0)
56.2�9.5
(25.0–85.0)
Race, No. (%)
Caucasian 76 (79.2) 68 (76.4) 39 (84.8) 105 (75.5)
Black 17 (17.7) 9 (10.1) 4 (8.7) 22 (15.8)
Asian 3 (3.1) 11 (12.4) 3 (6.5) 11 (7.9)
Native American ⁄ Alaskan 0 (0.0) 1 (1.1) 0 (0.0) 1 (0.7)
Sex, No. (%)
Male 44 (45.8) 61 (68.5) 27 (58.7) 78 (56.1)
Female 52 (54.2) 28 (31.5) 19 (41.3) 61 (43.9)
Weight, mean�SD, kg 99.5�18.4 77.1�13.0 94.2�17.5 86.9�19.9
Height, mean�SD, cm 166.2�13.0 169.8�10.8 168.3�11.7 167.8�12.3
BMI, mean�SD, kg ⁄ m2 35.9�4.9 26.6�2.5 33.4�5.7 30.8�6.1
SeSBP ⁄ SeDBP, mean�SD, mm Hg 158.2�12.5 ⁄ 94.2�8.5 158.3�12.8 ⁄ 91.4�8.6 159.1�11.3 ⁄ 90.3�9.2 157.9�13.1 ⁄ 93.7�8.3
24-Hour ambulatory SBP ⁄ DBP,
mean�SD, mm Hga
143.7�9.8 ⁄ 84.9�8.2 146.1�12.2 ⁄ 86.6�7.6 145.6�10.4 ⁄ 83.1�9.0 144.6�11.2 ⁄ 86.6�7.3
Hypertension stage, No. (%)
Stage 1 39 (40.6) 43 (48.3) 21 (45.7) 61 (43.9)
Stage 2 57 (59.4) 46 (51.7) 25 (54.3) 78 (56.1)
Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; SBP, systolic blood pressure; SD, standard deviation; SeDBP, seated cuffdiastolic BP; SeSBP, seated cuff systolic BP. aPatients with ambulatory blood pressure monitoring values for baseline and end of study; obese,n=89; nonobese, n=83; with diabetes, n=43; without diabetes, n=129.
424 The Journal of Clinical Hypertension Vol 13 | No 6 | June 2011 Official Journal of the American Society of Hypertension, Inc.
Efficacy of AML and OM in Hypertensive Patients | Punzi et al.
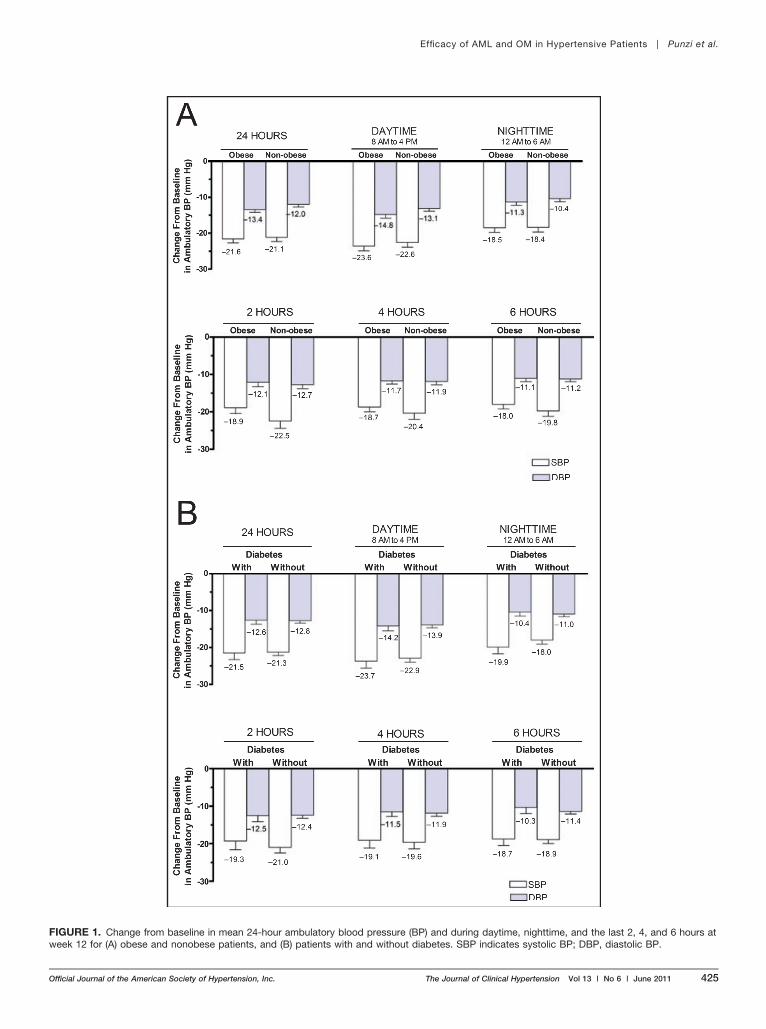
FIGURE 1. Change from baseline in mean 24-hour ambulatory blood pressure (BP) and during daytime, nighttime, and the last 2, 4, and 6 hours atweek 12 for (A) obese and nonobese patients, and (B) patients with and without diabetes. SBP indicates systolic BP; DBP, diastolic BP.
Official Journal of the American Society of Hypertension, Inc. The Journal of Clinical Hypertension Vol 13 | No 6 | June 2011 425
Efficacy of AML and OM in Hypertensive Patients | Punzi et al.
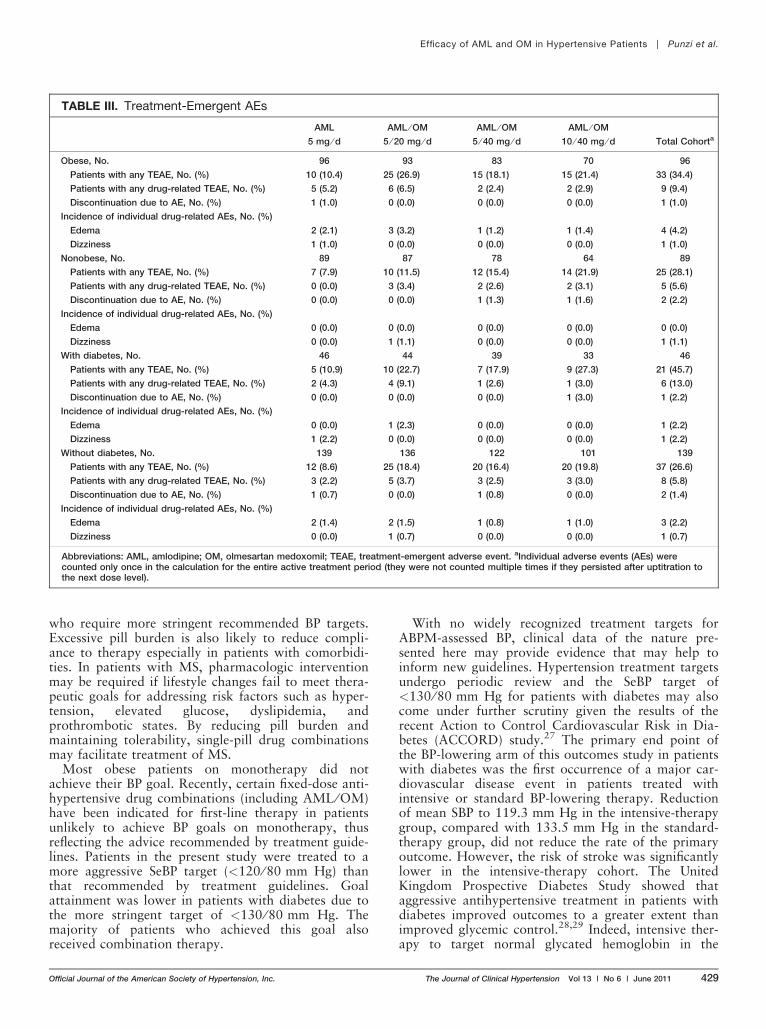
Safety and TolerabilityThe AML ⁄ OM–based treatment regimen was well tol-erated in each subgroup (Table III). In the safetycohort, 31.4% of patients reported treatment-emergentadverse events (TEAEs) and only 7.6% were con-sidered to be drug-related (DR). In the obese andnonobese subgroups, 9.4% and 5.6% experienced �1DR-TEAE, respectively. The diabetes group and non-diabetes group experienced �1 DR-TEAE at a rateof 13.0% and 5.8%, respectively. No cases of hypo-tension were reported in the study. The most
common DR-TEAE, peripheral edema, occurred in4 of 185 patients in the total study cohort. All4 of these patients were in the obese subgroup(Table III).
DISCUSSIONThe results of this subgroup analysis parallel thosefound in the primary study.18 The trial design assessedBP throughout the 24-hour dosing interval and thisnovel subgroup study allowed an analysis of the effectof the AML ⁄ OM–based titration regimen in patients
FIGURE 2. Twenty-four–hour blood pressure (BP) profiles in (A) obese patients and (B) patients with diabetes. SBP indicates systolic BP; DBP,diastolic BP.
426 The Journal of Clinical Hypertension Vol 13 | No 6 | June 2011 Official Journal of the American Society of Hypertension, Inc.
Efficacy of AML and OM in Hypertensive Patients | Punzi et al.
with hypertension and diabetes or obesity. Data ofthese nature are rarely reported in these classes of met-abolically challenged patients. The data showed thatBP was reduced and treatment was well tolerated inthese patients.
The findings reported here, mean ambulatory BPchanges from baseline in the last 6 hours of dosing of)18.0 ⁄)11.1 mm Hg (obese subgroup) and )18.7 ⁄)10.3 mm Hg (diabetes subgroup), are comparable withthose found in the similar Study of Micardis (telmisar-tan [TEL]) in Overweight ⁄ Obese Patients With Type 2Diabetes and Hypertension (SMOOTH).19 The effectof TEL ⁄ HCTZ or valsartan (VAL) ⁄ HCTZ fixed-dosetherapies on early morning BP using ABPM in high-risk, overweight ⁄ obese patients with concomitanthypertension and type 2 diabetes was assessed. Meanchanges from baseline in SBP ⁄ DBP during the last6 hours of the dosing interval were )18.4 ⁄)9.7 mm
Hg in TEL ⁄ HCTZ-treated patients and )14.5 ⁄)7.7mm Hg in VAL ⁄ HCTZ-treated patients.
In AZTEC, the titration regimen controlled BP dur-ing the 24-hour dosing interval in obese patients andSeBP reductions were comparable with a previousstudy of AML ⁄ OM. Previously, up to 50% of obesepatients in the 8-week factorial design stage of theCombination of Olmesartan Medoxomil and Amlodi-pine Besylate in Controlling High BP (COACH) studywho received dosages of AML ⁄ OM used in the presentstudy achieved the Seventh Report of the JointNational Committee on Prevention, Detection, Evalua-tion, and Treatment of High Blood Pressure goal of<140 ⁄ 90 mm Hg.20 Similar efficacy has been reportedin patients receiving VAL, in combination with AMLin the Exforge Efficacy and Control in Treatment ofStage 2 Hypertension (EX-EFFeCTS) study.21 In theEX-EFFeCTS study, 53.4% of obese patients with
FIGURE 3. Change from baseline in mean seated cuff blood pressure (SeBP) by titration period in (A) obese patients and (B) patients with diabetes.LOCF indicates last observation carried forward; AML, amlodipine; OM, olmesartan medoxomil; SeDBP, seated cuff diastolic BP.
Official Journal of the American Society of Hypertension, Inc. The Journal of Clinical Hypertension Vol 13 | No 6 | June 2011 427
Efficacy of AML and OM in Hypertensive Patients | Punzi et al.
stage 2 hypertension uptitrated to AML ⁄ VAL 10 ⁄ 160mg ⁄ d achieved the SeBP goal of <140 ⁄ 90 mm Hg.
The use of ABPM is an important tool to evaluatethe efficacy of antihypertensive treatment strategies in
patients at risk for cardiovascular events.16,17 In thepresent study, in patients with diabetes, BP wasreduced throughout the 24-hour dosing interval andduring the last 6 hours of the dosing period, coincid-ing with the normal morning BP surge, an event asso-ciated with the greatest cardiovascular risk.22
Approximately one quarter of patients uptitrated toAML ⁄ OM 10 ⁄ 40 mg ⁄ d achieved the recommendedSeBP goal of <130 ⁄ 80 mm Hg, a result comparablewith the open-label extension of the COACH studywhere approximately 19% of patients uptitrated to thesame dosage achieved this goal.23 The low rate ofSeBP goal achievement supports the observation thatBP control in patients with diabetes may require multi-ple antihypertensive agents. Indeed, in the open-labelextension of COACH, BP goal achievement wasenhanced when HCTZ was added to AML ⁄ OM.23 Afactorial design study that evaluated the efficacy andtolerability of a triple combination of AML ⁄ OM ⁄HCTZ compared with double therapy has recentlybeen published.24
BP control in clinical practice is much worse thanthat attained in clinical trials. The lack of BP controlin the United States has been attributed largely to ther-apeutic inertia—the failure to manage a chronic condi-tion aggressively enough to bring it under control.25
Fixed-dose combinations are a rational strategy toaddress patient compliance and clinical inertia,26 par-ticularly given that combination therapy is typicallyrequired in obese patients or patients with diabetes
FIGURE 4. Achievement of ambulatory blood pressure (BP) targets in (A) obese patients and (B) patients with diabetes.
TABLE II. Proportion (Percentage) of PatientsAchieving SeBP Goals at End of Study and DuringTitration Period
AMLa
5 mg
AML ⁄ OMa
5 ⁄ 20 mg
AML ⁄ OMa
5 ⁄ 40 mg
AML ⁄ OMa
10 ⁄ 40 mg
Obese, No. 96 93 83 69
<140 ⁄ 90 mm Hg 21.9 51.0 69.8 78.1
<130 ⁄ 80 mm Hg 3.1 10.4 15.6 24.0
<120 ⁄ 80 mm Hg 1.0 4.2 5.2 10.4
Nonobese, No. 89 86 77 67
<140 ⁄ 90 mm Hg 25.8 43.8 64.0 75.3
<130 ⁄ 80 mm Hg 4.5 18.0 25.8 37.1
<120 ⁄ 80 mm Hg 0.0 1.1 5.6 7.9
With diabetes, No. 46 44 38 33
<130 ⁄ 80 mm Hg 4.3 13.0 19.6 26.1
<120 ⁄ 80 mm Hg 2.2 6.5 8.7 8.7
Without diabetes, No. 139 135 122 100
<140 ⁄ 90 mm Hg 23.0 45.3 65.5 75.5
<130 ⁄ 80 mm Hg 3.6 14.4 20.9 31.7
<120 ⁄ 80 mm Hg 0.0 1.4 4.3 9.4
Abbreviations: AML, amlodipine; OM, olmesartan medoxomil; SeBP,seated cuff BP. aCumulative percentages are calculated using thetotal number of patients in the treatment cohort as the denominator.
428 The Journal of Clinical Hypertension Vol 13 | No 6 | June 2011 Official Journal of the American Society of Hypertension, Inc.
Efficacy of AML and OM in Hypertensive Patients | Punzi et al.
who require more stringent recommended BP targets.Excessive pill burden is also likely to reduce compli-ance to therapy especially in patients with comorbidi-ties. In patients with MS, pharmacologic interventionmay be required if lifestyle changes fail to meet thera-peutic goals for addressing risk factors such as hyper-tension, elevated glucose, dyslipidemia, andprothrombotic states. By reducing pill burden andmaintaining tolerability, single-pill drug combinationsmay facilitate treatment of MS.
Most obese patients on monotherapy did notachieve their BP goal. Recently, certain fixed-dose anti-hypertensive drug combinations (including AML ⁄ OM)have been indicated for first-line therapy in patientsunlikely to achieve BP goals on monotherapy, thusreflecting the advice recommended by treatment guide-lines. Patients in the present study were treated to amore aggressive SeBP target (<120 ⁄ 80 mm Hg) thanthat recommended by treatment guidelines. Goalattainment was lower in patients with diabetes due tothe more stringent target of <130 ⁄ 80 mm Hg. Themajority of patients who achieved this goal alsoreceived combination therapy.
With no widely recognized treatment targets forABPM-assessed BP, clinical data of the nature pre-sented here may provide evidence that may help toinform new guidelines. Hypertension treatment targetsundergo periodic review and the SeBP target of<130 ⁄ 80 mm Hg for patients with diabetes may alsocome under further scrutiny given the results of therecent Action to Control Cardiovascular Risk in Dia-betes (ACCORD) study.27 The primary end point ofthe BP-lowering arm of this outcomes study in patientswith diabetes was the first occurrence of a major car-diovascular disease event in patients treated withintensive or standard BP-lowering therapy. Reductionof mean SBP to 119.3 mm Hg in the intensive-therapygroup, compared with 133.5 mm Hg in the standard-therapy group, did not reduce the rate of the primaryoutcome. However, the risk of stroke was significantlylower in the intensive-therapy cohort. The UnitedKingdom Prospective Diabetes Study showed thataggressive antihypertensive treatment in patients withdiabetes improved outcomes to a greater extent thanimproved glycemic control.28,29 Indeed, intensive ther-apy to target normal glycated hemoglobin in the
TABLE III. Treatment-Emergent AEs
AML
5 mg ⁄ dAML ⁄ OM
5 ⁄ 20 mg ⁄ dAML ⁄ OM
5 ⁄ 40 mg ⁄ dAML ⁄ OM
10 ⁄ 40 mg ⁄ d Total Cohorta
Obese, No. 96 93 83 70 96
Patients with any TEAE, No. (%) 10 (10.4) 25 (26.9) 15 (18.1) 15 (21.4) 33 (34.4)
Patients with any drug-related TEAE, No. (%) 5 (5.2) 6 (6.5) 2 (2.4) 2 (2.9) 9 (9.4)
Discontinuation due to AE, No. (%) 1 (1.0) 0 (0.0) 0 (0.0) 0 (0.0) 1 (1.0)
Incidence of individual drug-related AEs, No. (%)
Edema 2 (2.1) 3 (3.2) 1 (1.2) 1 (1.4) 4 (4.2)
Dizziness 1 (1.0) 0 (0.0) 0 (0.0) 0 (0.0) 1 (1.0)
Nonobese, No. 89 87 78 64 89
Patients with any TEAE, No. (%) 7 (7.9) 10 (11.5) 12 (15.4) 14 (21.9) 25 (28.1)
Patients with any drug-related TEAE, No. (%) 0 (0.0) 3 (3.4) 2 (2.6) 2 (3.1) 5 (5.6)
Discontinuation due to AE, No. (%) 0 (0.0) 0 (0.0) 1 (1.3) 1 (1.6) 2 (2.2)
Incidence of individual drug-related AEs, No. (%)
Edema 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
Dizziness 0 (0.0) 1 (1.1) 0 (0.0) 0 (0.0) 1 (1.1)
With diabetes, No. 46 44 39 33 46
Patients with any TEAE, No. (%) 5 (10.9) 10 (22.7) 7 (17.9) 9 (27.3) 21 (45.7)
Patients with any drug-related TEAE, No. (%) 2 (4.3) 4 (9.1) 1 (2.6) 1 (3.0) 6 (13.0)
Discontinuation due to AE, No. (%) 0 (0.0) 0 (0.0) 0 (0.0) 1 (3.0) 1 (2.2)
Incidence of individual drug-related AEs, No. (%)
Edema 0 (0.0) 1 (2.3) 0 (0.0) 0 (0.0) 1 (2.2)
Dizziness 1 (2.2) 0 (0.0) 0 (0.0) 0 (0.0) 1 (2.2)
Without diabetes, No. 139 136 122 101 139
Patients with any TEAE, No. (%) 12 (8.6) 25 (18.4) 20 (16.4) 20 (19.8) 37 (26.6)
Patients with any drug-related TEAE, No. (%) 3 (2.2) 5 (3.7) 3 (2.5) 3 (3.0) 8 (5.8)
Discontinuation due to AE, No. (%) 1 (0.7) 0 (0.0) 1 (0.8) 0 (0.0) 2 (1.4)
Incidence of individual drug-related AEs, No. (%)
Edema 2 (1.4) 2 (1.5) 1 (0.8) 1 (1.0) 3 (2.2)
Dizziness 0 (0.0) 1 (0.7) 0 (0.0) 0 (0.0) 1 (0.7)
Abbreviations: AML, amlodipine; OM, olmesartan medoxomil; TEAE, treatment-emergent adverse event. aIndividual adverse events (AEs) werecounted only once in the calculation for the entire active treatment period (they were not counted multiple times if they persisted after uptitration tothe next dose level).
Official Journal of the American Society of Hypertension, Inc. The Journal of Clinical Hypertension Vol 13 | No 6 | June 2011 429
Efficacy of AML and OM in Hypertensive Patients | Punzi et al.
ACCORD study did not significantly reduce majorcardiovascular events but actually increased mortality,leading to early termination of this arm of the clinicaltrial.30
LIMITATIONSThe present study demonstrated the efficacy of anAML ⁄ OM titration regimen in patients with hyperten-sion and who were obese or had diabetes. A majorityof the patients with diabetes were treated to the SeBPtarget <130 ⁄ 80 mm Hg. However, limitations of thisstudy were that long-term efficacy of the treatmentcould not be determined and the trial was of an open-label and single-arm design. Another limitation wasthat obese patients were not further stratified by diabe-tes status. In addition, it was not possible to analyzepatient outcomes or to determine the statistical signifi-cance of differences between subgroups.
CONCLUSIONSA fixed-dose combination of AML ⁄ OM is an effectiveapproach to managing hypertension in all patients,including traditionally difficult-to-treat patients suchas those with diabetes and ⁄ or obesity.
Acknowledgments: We thank Kathryn Leonard, BSc, and Christopher J.Jones, PhD, of inScience Communications, a Wolters Kluwer business, forproviding medical writing support funded by Daiichi Sankyo, Inc.
Disclosure: This study was supported by Daiichi Sankyo, Inc. Henry Punzi,MD, received a research grant from Daiichi Sankyo, Inc. Ali Shojaee,PharmD, William F. Waverczak, MS, and Jen-Fue Maa, PhD are employedby Daiichi Sankyo, Inc.
References1. Lorenzo C, Williams K, Hunt KJ, et al. Trend in the prevalence of
the metabolic syndrome and its impact on cardiovascular diseaseincidence: the San Antonio Heart Study. Diabetes Care. 2006;29(3):625–630.
2. Mokdad AH, Ford ES, Bowman BA, et al. Prevalence of obesity,diabetes, and obesity-related health risk factors, 2001. JAMA. 2003;289(1):76–79.
3. Geiss LS, Pan L, Cadwell B, et al. Changes in incidence of diabe-tes in U.S. adults, 1997–2003. Am J Prev Med. 2006;30(5):371–377.
4. Wong ND, Lopez VA, L’Italien G, et al. Inadequate control ofhypertension in US adults with cardiovascular disease comorbiditiesin 2003–2004. Arch Intern Med. 2007;167(22):2431–2436.
5. Centers for Disease Control and Prevention. National Diabetes FactSheet: General Information and National Estimates on Diabetes inthe United States. Atlanta, GA: Department for Health and HumanServices; 2005.
6. American Diabetes Association. Standards of medical care in diabe-tes–2008. Diabetes Care. 2008;31(suppl 1):S12–S54.
7. Mancia G, De Backer G, Dominiczak A, et al. Guidelines for themanagement of arterial hypertension: the Task Force for the Man-agement of Arterial Hypertension of the European Society of Hyper-tension (ESH) and of the European Society of Cardiology (ESC).J Hypertens. 2007; 25(6):1105–1187.
8. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report ofthe Joint National Committee on Prevention, Detection, Evaluation,and Treatment of High Blood Pressure: the JNC 7 report. JAMA2003;289(19):2560–2572.
9. Jamerson K, Weber MA, Bakris GL, et al. Benazepril plus amlodi-pine or hydrochlorothiazide for hypertension in high-risk patients. NEngl J Med. 2008;359(23):2417–2428.
10. Lindholm LH, Ibsen H, Dahlof B, et al. Cardiovascular morbidityand mortality in patients with diabetes in the Losartan InterventionFor Endpoint reduction in hypertension study (LIFE): a randomisedtrial against atenolol. Lancet. 2002;359(9311):1004–1010.
11. Hansson L, Lindholm LH, Ekbom T, et al. Randomised trial ofold and new antihypertensive drugs in elderly patients: cardio-vascular mortality and morbidity the Swedish Trial in OldPatients with Hypertension-2 study. Lancet. 1999;354(9192):1751–1756.
12. Lithell H, Hansson L, Skoog I, et al. The Study on Cognition andPrognosis in the Elderly (SCOPE): principal results of a rando-mized double-blind intervention trial. J Hypertens. 2003;21(5):875–886.
13. Hansson L, Lindholm LH, Niskanen L, et al. Effect of angiotensin-converting-enzyme inhibition compared with conventional therapyon cardiovascular morbidity and mortality in hypertension: the Cap-topril Prevention Project (CAPPP) randomised trial. Lancet.1999;353(9153): 611–616.
14. Punzi HA, Punzi CF. Metabolic issues in the Antihypertensive andLipid-Lowering Heart Attack Trial Study. Curr Hypertens Rep.2004;6(2):106–110.
15. Gosse P, Lasserre R, Minifie C, et al. Blood pressure surge on rising.J Hypertens. 2004;22(6):1113–1118.
16. Chavanu K, Merkel J, Quan AM. Role of ambulatory blood pres-sure monitoring in the management of hypertension. Am J HealthSyst Pharm. 2008;65(3):209–218.
17. Punzi HA. Why ambulatory blood pressure monitoring? Am JHealth Syst Pharm. 1998;55(suppl 3):S12–S16.
18. Punzi H, Neutel JM, Kereiakes DJ, et al. Efficacy of amlodipine andolmesartan medoxomil in patients with hypertension: the AZORTrial Evaluating Blood Pressure Reductions and Control (AZTEC)study. Ther Adv Cardiovasc Dis. 2010;4:209–221.
19. Sharma AM, Davidson J, Koval S, et al. Telmisartan ⁄ hydrochloro-thiazide versus valsartan ⁄ hydrochlorothiazide in obese hypertensivepatients with type 2 diabetes: the SMOOTH study. Cardiovasc Dia-betol. 2007;6:28.
20. Chrysant SG, Lee J, Melino M, et al. Efficacy and tolerability of am-lodipine plus olmesartan medoxomil in patients with difficult-to-treat hypertension. J Hum Hypertens. 2010;24:730–738.
21. Destro M, Luckow A, Samson M, et al. Efficacy and safety ofamlodipine ⁄ valsartan compared with amlodipine monotherapy inpatients with stage 2 hypertension: a randomized, double-blind,multicenter study: the EX-EFFeCTS Study. J Am Soc Hypertens.2008;2(4):294–302.
22. Neutel JM. The importance of 24-h blood pressure control. BloodPress Monit. 2001;6(1):9–16.
23. Oparil S, Chrysant SG, Melino M, et al. Long-term efficacy of acombination of amlodipine and olmesartan medoxomil+ ⁄ )hydro-chlorothiazide in patients with hypertension stratified by age, raceand diabetes status: a substudy of the COACH trial. J Hum Hyper-tens. 2010;24:831–838.
24. Oparil S, Melino M, Lee J, et al. Triple therapy with olmesartanmedoxomil, amlodipine besylate, and hydrochlorothiazide in adultpatients with hypertension: the TRINITY multicenter, randomized,double-blind, 12-week, parallel-group study. Clin Ther. 2010;32(7):1252–1269.
25. Okonofua EC, Simpson KN, Jesri A, et al. Therapeutic inertia is animpediment to achieving the Healthy People 2010 blood pressurecontrol goals. Hypertension. 2006; 47(3):345–351.
26. Sica DA. Rationale for fixed-dose combinations in the treatment ofhypertension: the cycle repeats. Drugs. 2002; 62(3):443–462.
27. Cushman WC, Evans GW, Byington RP, et al. Effects of intensiveblood-pressure control in type 2 diabetes mellitus. N Engl J Med.2010;362(17):1575–1585.
28. UK Prospective Diabetes Study Group. Tight blood pressure controland risk of macrovascular and microvascular complications in type2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ.1998;317(7160):703–713.
29. UK Prospective Diabetes Study Group. Effect of intensive blood-glu-cose control with metformin on complications in overweightpatients with type 2 diabetes (UKPDS 34). UK Prospective DiabetesStudy (UKPDS) Group. Lancet. 1998;352(9131):854–865.
30. Gerstein HC, Miller ME, Byington RP, et al. Effects of intensiveglucose lowering in type 2 diabetes. N Engl J Med.2008;358(24):2545–2559.
430 The Journal of Clinical Hypertension Vol 13 | No 6 | June 2011 Official Journal of the American Society of Hypertension, Inc.
Efficacy of AML and OM in Hypertensive Patients | Punzi et al.