Embed Size (px)
Citation preview

Vol. 35, No. 11ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Nov. 1991, p. 2375-23810066-4804/91/112375-07$02.00/0Copyright © 1991, American Society for Microbiology
Efficacy of Chloramphenicol, Enrofloxacin, and Tetracycline forTreatment of Experimental Rocky Mountain Spotted Fever in DogsEDWARD B. BREITSCHWERDT,1* MICHAEL G. DAVIDSON,' DAVID P. AUCOIN,2 MICHAEL G. LEVY,3
NANCY S. SZABADOS,1 BARBARA C. HEGARTY,1 ANITA L. KUEHNE,l AND ROBERT L. JAMES4Departments of Companion Animal and Special Species Medicine,' Anatomy, Physiology, and Radiology,2 and
Microbiology, Pathology, and Parasitology,3 College of Veterinary Medicine, and the Department ofStatistics,4 North Carolina State University, Raleigh, North Carolina 27606
Received 17 June 1991/Accepted 11 September 1991
Dogs were experimentally inoculated with Rickettsia rickettsii to characterize the comparative efficacies ofchloramphenicol, enrofloxacin, and tetracycline for the treatment of Rocky Mountain spotted fever (RMSF).All three antibiotics were equally effective in abrogating the clinical, hematologic, and vascular indicators ofrickettsial infection. Antibiotic treatment for 24 h was sufficient to decrease the rickettsemia to levels belowdetection by Vero cell culture. Early treatment with all three antibiotics resulted in a similar decrease inantibody titer, but acute and convalescent serum samples taken at appropriate times would have still facilitatedan accurate diagnosis of RMSF in all but one dog, which did not seroconvert. We conclude that chloramphen-icol, enrofloxacin, and tetracycline are equally efficacious for treating experimental canine RMSF.
Rocky Mountain spotted fever (RMSF), caused by Rick-ettsia rickettsii, is the most common human rickettsiosis inthe United States (5, 15). The pathophysiologic conse-quences of cytopathic rickettsial injury contribute to similarhistorical findings and physical abnormalities and nearlyidentical hematologic, serum biochemical, and pathologicchanges in both dogs and people (2, 7, 18). Like the diseasein humans, canine RMSF is often associated with severemorbidity and occasional mortality (1, 11). Because of thesefactors, information generated through experimental studiesutilizing dogs may be applicable to both species.We are not aware of any controlled clinical or experimen-
tal studies that have compared the efficacies of chloramphen-icol, enrofloxacin, and tetracycline for the treatment ofRMSF. Clinical experience dictates various opinions amongveterinarians and physicians as to the comparative efficaciesof chloramphenicol and tetracycline for the treatment ofRMSF. Recent epidemiologic findings suggest that mortalityis higher when chloramphenicol, rather than tetracycline, isused for the treatment of human RMSF (10). However, thistrend may be related to physician preference for chloram-phenicol in patients with severe disease.Recent demonstration of in vitro rickettsicidal properties
of ciprofloxacin, a broad-spectrum quinolone antibiotic (3,24, 25), suggests that this class of drugs may be useful in thetreatment of RMSF. Quinolones may be of particular benefitin those instances when tetracycline or chloramphenicol useis undesirable. Enrofloxacin (Baytril; Mobay Corporation,Animal Health Division, Shawnee, Kans.), an analog ofciprofloxacin, was selected for study because it has receivedFood and Drug Administration approval for use in dogs andbecause it is being used with increasing frequency by veter-inarians for treating dogs with febrile illness. The purpose ofthis study was to compare the efficacies of chloramphenicol,enrofloxacin, and tetracycline in dogs experimentally in-fected with R. rickettsii.
* Corresponding author.
MATERIALS AND METHODS
Study design. Sixteen 13-month-old female beagles wererandomly divided into four groups, with four dogs in eachgroup (the nontreated control group and chloramphenicol-,enrofloxacin-, and tetracycline-treated groups). All dogswere seronegative to R. rickettsii by microimmunofluores-cence testing, as described previously (22), and were nega-tive for dirofilariae and intestinal parasites. Complete bloodcounts and serum biochemical analyses were normal prior toinfection.R. rickettsu. All four groups were inoculated intradermally
in two sites over the pelvis (0.5 ml per site) with a canineisolate of R. rickettsii (strain Domino; inoculum strength, 5x 104 PFU/ml). Rickettsiae were diluted in sterile brain heartinfusion broth for inoculation.Treatment protocol. Beginning on postinoculation (p.i.)
day 6, antibiotics were administered to the three treatmentgroups. The mean group dosages were as follows: chloram-phenicol, 29.9 mg/kg of body weight orally at 8-h intervals;enrofloxacin, 3.0 mg/kg orally at 12-h intervals; tetracyclineHCI, 31.3 mg/kg orally at 8-h intervals. In all three treatmentgroups, antibiotics were continued for 7 days.
Monitoring. Physical examinations, including rectal tem-perature measurements, observations related to attitudinalchange, and oral and ocular examinations, were conductedin an examiner-blinded fashion twice daily. An attitudinalscore was recorded for each dog twice daily, with scoringand criteria as follows: 5, alert, active, and eating; 4, alert,inactive, and eating; 3, depressed, inactive, and anorexic; 2,severely depressed and anorexic; 1, recumbent; and 0, dead.Blood was collected by jugular venipuncture on p.i. days 3,5, 7, 10, 12, 14, 18, and 21 for complete blood counts, serumbiochemical analysis, and serologic testing for R. rickettsiiby microimmunofluorescence.
Vascular permeability studies. Fluorescein angiography ofthe ocular fundus was performed prior to inoculation and onp.i. days 3, 5, 8, 10, 12, and 17, using previously describedmethods (7). The area of sodium fluorescein dye leakagefrom injured retinal vessels was quantitated by computer-
2375
on July 18, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

2376 BREITSCHWERDT ET AL.
assisted morphometric analysis, using photographic prints (4by 5 in. [ca. 10 by 13 cm]) of angiograms taken between 30and 45 s after sodium fluorescein administration. The totalsurface area of retinal dye leakage per dog was assigned anumerical value corresponding to a fractional area of anoptic nerve (which was assigned a numerical value of 1).Drug analysis and pharmacokinetic studies. On p.i. days 6,
11, and 25, blood samples were obtained by jugular veni-puncture at 0, 30, 60, 180, 300, and 480 min for pharmaco-kinetic characterization of each dog within an antibioticgroup. For the enrofloxacin group, the last sample wasobtained at 720 rather than 480 min. Chloramphenicol,tetracycline HCl, and enrofloxacin concentrations in serumwere determined by high performance liquid chromatogra-phy, using previously published methods (27, 31, 32).
Rickettsial isolation. Sterile, heparinized venous blood wascollected from each dog on p.i. day 3 and from two dogsfrom each group on p. i. days 5, 7, 10, 12, 14, 18, 21, 25, and28. A modification of the tissue culture isolation methoddescribed by Kaplowitz et al. (17) was used. Whole blood(0.10 ml) was evenly distributed onto a confluent monolayerof Vero cells in each of four glass cell culture tubes (16 by125 mm) from which the medium had been removed. Theinoculated Vero cells were incubated at 34°C for 1 h, afterwhich 2 ml of cell culture medium was added and the tubeswere reincubated at 34°C at a 5° angle. On the 9th, 14th, 21st,and 28th days, the tubes were vortexed and centrifuged topellet the cells and debris. The medium was removed, andthe pellet was resuspended in phosphate-buffered saline (pH7.3) containing 0.5% bovine serum albumin. Slides wereprepared, air dried, and acetone fixed before being stainedfor the presence of rickettsiae by indirect fluorescent anti-body and direct fluorescent antibody. If there were nodetectable rickettsiae during this time, the cultures wereconsidered negative.
Microimmunofluorescence testing. A microimmunofluores-cence test was used to evaluate for the presence of antibod-ies to R. rickettsii (strain Sheila Smith) in dogs. Canine serawere evaluated with fluorescein isothiocyanate goat anti-
41.2
40.8 _
0
Q)
ad
E-
40.4
40.0
39.6
39.2
38.8
38.4
canine immunoglobulin G (IgG) (heavy- and light-chain-specific) conjugate. All sera were screened at 1:16 dilutions,and the titers of those reacting were determined to the endpoint. Positive and negative controls were evaluated witheach group.
Statistics. Antibiotic treatment effects were analyzed byusing multivariate repeated-measures analysis of variance. Aseparate analysis was performed for each physiologicalparameter. Linear contrasts within the repeated-measuresanalysis tested for differences between the control andantibiotic treatments. Profile contrasts were used to detectsignificant differences in the shape of the parameter responsecurves among the treatments (16). The nonparametricWilcoxon's rank sum test was performed on attitudinalscores and on the retinal vascular lesion data because of thenonnormality of the data.
RESULTS
Clinicopathologic studies. Prior to the initiation of antibi-otic treatment, there was no significant difference in meanvalues for rectal temperature, attitudinal score, plateletnumber, and the ratio of albumin concentration to totalprotein concentration in serum among the four groups ofdogs. Compared with the nontreated control group, antibi-otic treatment initiated on p.i. day 6 caused a rapid decreasein rectal temperature (P = 0.001), an improvement in attitu-dinal score (P = 0.01), and a cessation of albumin loss (P =0.02). Although the overall drug effect on platelet numbersdid not differ significantly between the control and antibiotictreatments, the shape of the platelet response curve overtime differed between the control and antibiotic treatments(P = 0.0004). The platelet number returned to preinoculationlevels sooner with the antibiotic treatments than with thecontrol. There was no difference in any of the above param-eters among the three treatment groups.Fever (rectal temperature 2 39.6°C) was the first indica-
tion of infection. All dogs became febrile between p.i. days2 and 5. Rectal temperature was 40°C in 12 of 16 dogs on p.i.
0 5 10 15 20Postinoculation Days
FIG. 1. Mean daily rectal temperature curves foliowing inoculation with R. rickettsii (day 0) and after the initiation of antibiotics (day 6)in the three treatment groups. Each datum point represents the mean value of an AM and PM temperature for four dogs.
ANTIMICROB. AGENTS CHEMOTHER.
on July 18, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

ANTIBIOTIC EFFICACY FOR EXPERIMENTAL RMSF IN DOGS
6.0
5.5 -
AS/ V 00-0'/
0
0 Control
v '% O o.o U ChloramphenicV Enrofloxacin
11 55 t *tibotics 1 0started
col
A Tetracycline
20
Postinoculation Days
FIG. 2. Mean daily attitudinal scores after inoculation with R. rickettsii (day 0) and after the initiation of antibiotics (day 6) in the threetreatment groups. Each datum point represents the mean value of an AM and PM score for each of the four dogs in the group.
day 2. Attitudinal scores began to decrease on p.i. day 3, 4,or 5. Antibiotic treatment was initiated within 24 to 72 h afterthe attitudinal score decreased from 5. Defervescence oc-curred in the three treatment groups within 24 h after theinitiation of antibiotics (Fig. 1), whereas fever (rectal tem-perature 2 39.6°C) persisted in all four control dogs throughp.i. day 10. One control dog remained febrile until p.i. day17. Daily attitudinal scores ranged from 5 to 3 in all groups(Fig. 2). The attitudinal score in the three treatment groupsreturned to a 5 by p.i. day 8, whereas control dogs returnedtoa5byp.i. day 14.
550
500
450
0Y-4
400 _
350
.0 300a'
250
200
150
1000
Vascular permeability. In the three treatment groups,platelet numbers (Fig. 3) increased, and the decline in theratio of albumin concentration to total protein concentratiqn(Fig. 4) stabilized more rapidly than in the nontreated controlgroup. Prior to the initiation of antibiotic therapy, there wereno differences in the total number of retinal vascular lesionsor in the area of nontapetal retinal sodium fluorescein dyeleakage among the four groups of dogs. Nontreated contrpldogs developed a pattern of retinal vascular lesions typical ofexperimental R. rickettsii infection (7), with development oflesions on p.i. days 5 to 8 and progression of lesions over the
5 t Antibiotics 1 0started
Postinoculation Days
1 5 20
FIG. 3. Mean platelet values of the control and treatment groups after inoculation with R. rickettsii (day 0) and after the initiation ofantibiotics (day 6).
5.0 t
4.5 t
InU)0C)U)
P4.
.P4.
4.0
3.5f
3.0
2.50
O ControlV Earoflozacin* ChloramphenicolA Tetracycline
~7 0
L
VOL. 35, 1991 2377
I I
on July 18, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
2378 BREITSCHWERDT ET AL.
A
A.~
0
o ControlV Enrofloxacin
* ChloramphenicolA Tetracycline J v
V A
//~~~0
O 0
5 tAntibiotics 1 0started
15 20
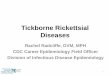
Postinoculation DaysFIG. 4. Mean ratios of albumin to total protein for the control and treatment groups after inoculation with R. rickettsii (day 0) and after
the initiation of antibiotics (day 6).
next 5 to 7 days p.i. Treated dogs either had rapid resolutionof existing retinal vascular lesions or failed to develop retinalfoci visible with fluorescein angiography, resulting in adecrease in the total number (P = 0.06) (Fig. 5) and mor-phometric severity (Fig. 6) (P = 0.03) of retinal vascularlesions when compared with control groups. There was nodifference in retinal vascular permeability among the threetreatment groups as determined by these indicators.
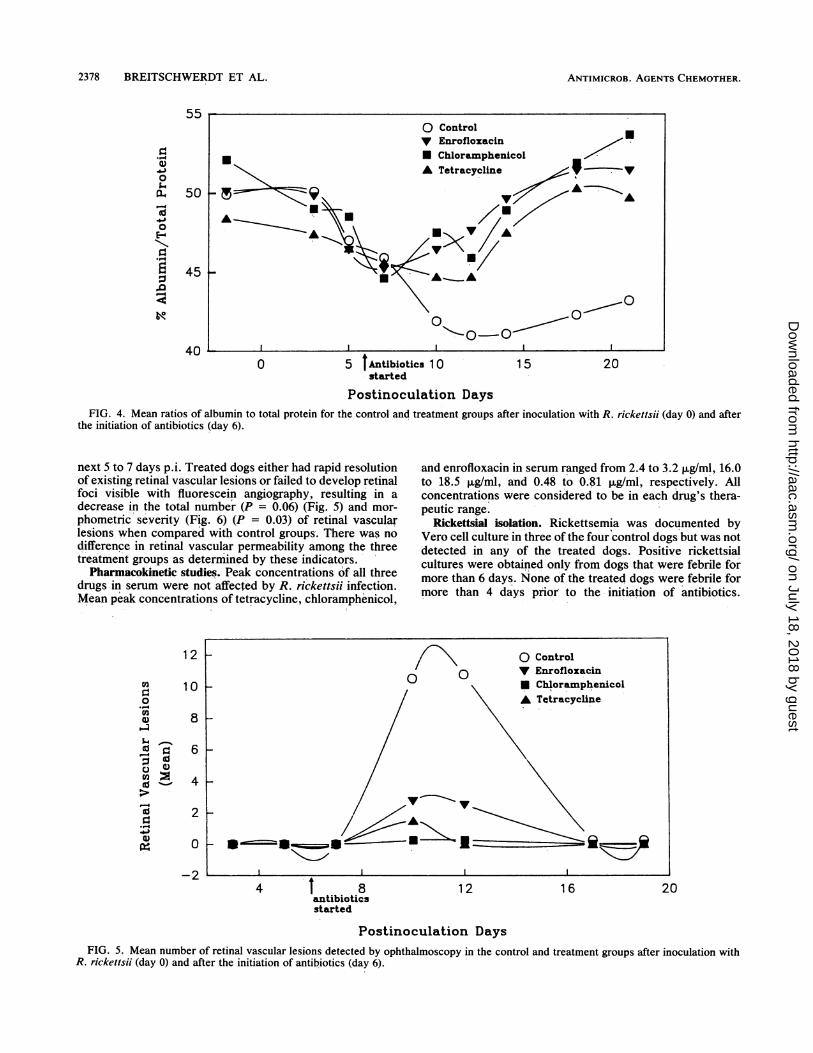
Pharmacokinetic studies. Peak concentrations of all threedrugs in serum were not affected by R. rickettsii infection.Mean peak concentrations of tetracycline, chloramphenicol,
and enrofloxacin in serum ranged from 2.4 to 3.2 pug/ml, 16.0to 18.5 ,ug/ml, and 0.48 to 0.81 ,ug/ml, respectively. Allconcentrations were considered to be in each drug's thera-peutic range.
Rickettsial isolation. Rickettsemia was documented byVero cell culture in three of the four control dogs but was notdetected in any of the treated dogs. Positive rickettsialcultures were obtained only from dogs that were febrile formore than 6 days. None of the treated dogs were febrile formore than 4 days prior to the initiation of antibiotics.
12
VI0.-
VI
U)
~1)5.4
-I0)
*_-l
to
10
8
0co
6
4
2
0
-2 1 l
4 t 8 12 16 20antibioticsstarted
Postinoculation DaysFIG. 5. Mean number of retinal vascular lesions detected by ophthalmoscopy in the control and treatment groups after inoculation with
R. rickettsii (day 0) and after the initiation of antibiotics (day 6).
0)
Q.4
-
toE-
d
:3
55
50
45
40
ANTIMICROB. AGENTS CHEMOTHER.
on July 18, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
ANTIBIOTIC EFFICACY FOR EXPERIMENTAL RMSF IN DOGS 2379
0.4
03
4)Li0
64
0.3
0.2
0.1
0.0
-0.120lantibiotflcs
startedPostinoculation Days
Fractional area of optic nerve
FIG. 6. Mean surface area of retinal fluorescein leakage in the control and treatment groups after inoculation with R. rickettsii (day 0) andafter the initiation of antibiotics (day 6). A numerical value for the lesion surface area was determined by measuring the morphometric areaof the lesions compared with the fractional area of the optic nerve.
Positive cultures were obtained from the three control dogsuntil 24 h prior to defervescence.
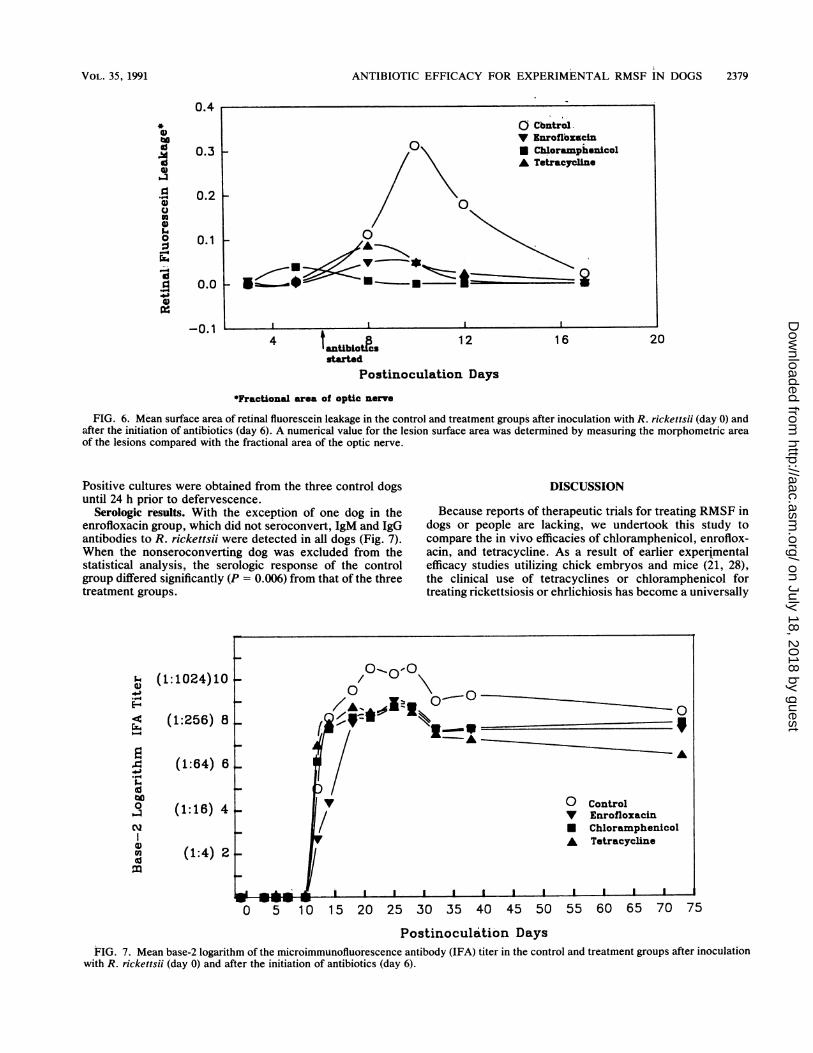
Serologic results. With the exception of one dog in theenrofloxacin group, which did not seroconvert, IgM and IgGantibodies to R. rickettsii were detected in all dogs (Fig. 7).When the nonseroconverting dog was excluded from thestatistical analysis, the serologic response of the controlgroup differed significantly (P = 0.006) from that of the threetreatment groups.
L (1:1024)10E- ~ ~ ~ A4
4 (1:256) 8 (
4 (1:64) 6Li
9 (1:16) 4 v
(1:4) 2
WL iis Ii I I0 5 10 15 20 21
DISCUSSION
Because reports of therapeutic trials for treating RMSF indogs or people are lacking, we undertook this study tocompare the in vivo efficacies of chloramphenicol, enroflox-acin, and tetracycline. As a result of earlier experimentalefficacy studies utilizing chick embryos and mice (21, 28),the clinical use of tetracyclines or chloramphenicol fortreating rickettsiosis or ehrlichiosis has become a universally
-9A
0VUA
I I I
ControlEnrofloxacinChloramphenicolTetracycline
5 30 35 40 45 50 55 60 65 70 75
Postinoculation DaysFIG. 7. Mean base-2 logarithm of the microimmunofluorescence antibody (IFA) titer in the control and treatment groups after inoculation
with R. rickettsii (day 0) and after the initiation of antibiotics (day 6).
VOL. 35, 1991
on July 18, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

2380 BREITSCHWERDT ET AL.
accepted practice (13, 26, 30). Since there are contraindica-tions for both antibiotics that make them less than ideal insome situations, alternative antibiotics for treating rickettsialinfections are needed. Recent in vitro (3, 24, 25) and in vivomouse studies (20), as well as clinical studies (9, 12, 23, 29),indicate that rickettsiae, including R. conorii, R. rickettsii,R. tsutsugamushi, R. typhi, and Ehrlichia sennetsu, aresusceptible to quinolone antibiotics such as enrofloxacin orciprofloxacin.Because enrofloxacin possesses broad-spectrum bacteri-
cidal activity against canine pathogens (34), it may proveuseful for the treatment of undiagnosed, acute-febrile illnessin adult dogs in endemic areas of tick-transmitted rickettsialdisease. Our results, in conjunction with recent findings (12,23-26), also suggest that investigation of the use of aquinolone antibiotic for treating RMSF in people is war-ranted, particularly in those instances when tetracycline orchloramphenicol use is undesirable.
In this study, all three antibiotics were equally effective inabrogating clinical, hematologic, and vascular indicators ofrickettsial infection in dogs. Sequential changes in plateletnumbers, the ratio of albumin concentration to total proteinconcentration in serum, and the severity of retinal vascularlesions as determined by fluorescein dye leakage providedthe best indicators of rickettsia-induced vascular injury (Fig.3 to 6). Compared with the more protracted clinical andhematologic course in the control group, treatment withchloramphenicol, enrofloxacin, and tetracycline facilitated,to a similar degree, the cessation of rickettsia-induced vas-cular injury. This is evidenced by a rapid increase in plateletnumbers and a stabilization of the decline in the ratio ofalbumin concentration to total protein concentration. Theseindicators coincided with rapid amelioration of focal alter-ations in retinal vascular permeability after antibiotic ther-apy or with abrogation of vascular endothelial injury intreated dogs that had not developed lesions. The rapidrestoration of functional retinal vascular integrity in thesedogs following antibiotic therapy supports previous histo-pathologic findings in tetracycline-treated guinea pigs withRMSF, which demonstrated rapid changes in endothelialfine structure indicative of cellular repair within 48 to 72 h ofthe initiation of antibiotic therapy (33). Presumably, thecontinued decline in the ratio of albumin concentration tototal protein concentration in the control dogs reflects theleakage of albumin through damaged blood vessels, withconcurrent retention of high-molecular-weight proteinswithin the vessels.We were not able to detect quantitative differences in
attitudinal improvement among the three treatment groups.A study that compared a 2-day course of oral ciprofloxacinand a 2-day course of oral doxycycline for treating Mediter-ranean spotted fever in people found that patients treatedwith doxycycline had a shorter defervescence period and aslightly more rapid disappearance of some clinical symptoms(12). Compared with doxycycline, chloramphenicol inducesa slower rate of killing of intracellular R. rickettsii in vitro(35), and terramycin induced more consistent death-delayingactivity in R. rickettsii-infected embryos than did chloram-phenicol (21). Collectively, these studies suggest only minortherapeutic differences between tetracyclines, quinolones,and chloramphenicol.
Previous reports on children (14) and dogs (2) suggest thatearly treatment with antibiotics will decrease the antibodytiter to R. rickettsii. In this study, all three antibiotics causeda similar decrease in antibody titer compared with titers fornontreated control dogs. Although antibody titers for the
treated dogs were significantly lower than for the controls,serologic testing of acute and convalescent serum samplestaken at appropriate times would have resulted in a four-fold increase in the microimmunofluorescence antibody ti-ters of all but one treated dog, thereby facilitating anaccurate diagnosis of RMSF. These results are comparableto a human study in which serodiagnosis (fourfold increasein antibody titer) was possible for six unvaccinated volun-teers who developed RMSF and were treated with tetracy-cline within 6 h after the onset of fever (6).For the first time in the course of our experimental studies
related to canine RMSF, a dog that developed mild clini-cal and hematologic indications of rickettsial infectionfailed to seroconvert to R. rickettsii by microimmunofluo-rescence testing. Although the importance of this occurrenceto the natural disease state is unclear, it does suggest thatearly antibiotic administration, or perhaps other factors,might eliminate a measurable serologic response to theorganism. In this study, treatment was started on p.i. day 6,compared with an initiation of treatment on day 12 in aprevious study (2) that failed to identify a difference inserologic response among tetracycline-treated and non-treated dogs during the same observation period. On thebasis of existing information, we conclude that antibiotictreatment for RMSF in people or dogs rarely interferes withserodiagnosis.
Rickettsemia was documented only in blood samplesobtained between p.i. days 7 and 10 and only from threeof the four control dogs. In previous experimental studieswith dogs, rickettsemia was detected by tissue culture iso-lation as early as the first 24 to 48 h of fever, and detectablelevels of rickettsemia decrease with defervescence (2, 4, 8).Rickettsiae can be successfully isolated from the blood offebrile human patients if cultures are initiated within thefirst 36 h of treatment with tetracycline or 48 h with chlor-amphenicol (8, 17, 19). In the guinea pig model, deferves-cence occurred after 4 days of tetracycline treatment, butrickettsial organisms could not be found in tissues by im-munofluorescent staining after 72 h (33). In our study,treatment with antibiotics resulted in defervescence within24 h. Our results seem to indicate that the level of rickett-semia was too low to afford positive cultures on p.i. day 3,but other factors, such as the fact that the blood sample wasfrozen prior to tissue culture inoculation, may have contrib-uted to negative cultures in eight dogs (two dogs from eachgroup) on p.i. day 5. We have been able to demonstraterickettsemia in dogs on p.i. day 5 by inoculating a Derma-centor variabilis cell culture with fresh plasma (2). It alsoappears that antibiotic treatment for 24 h was sufficient tolower the number of organisms in the blood to levels belowdetection.The results of this study must be interpreted with the
qualification that infective dose, the strain of R. rickettsii, orpotentially other factors might alter the severity of diseaseand thereby potentially modify the outcome associated withantibiotic treatment. This particular caution in interpretationis emphasized because the case-fatality rate with humanRMSF patients treated with chloramphenicol is not signifi-cantly lower than with untreated patients (10). Our studymay not address the comparative efficacy of these antibioticsin severe, potentially fatal RMSF.
REFERENCES
1. Breitschwerdt, E. B., D. J. Meuten, D. H. Walker, M. G. Levy,K. Kennedy, M. King, and B. C. Curtis. 1985. Canine Rocky
ANTIMICROB. AGENTS CHEMOTHER.
on July 18, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

ANTIBIOTIC EFFICACY FOR EXPERIMENTAL RMSF IN DOGS 2381
Mountain spotted fever: a kennel epizootic. Am. J. Vet. Res.46:2124-2128.
2. Breitschwerdt, E. B., D. H. Walker, M. G. Levy, W. Burgdorfer,W. T. Corbett, S. A. Huribert, M. E. Stebbins, B. C. Curtis, andD. A. Alien. 1988. Clinical, hematologic, and humoral immuneresponse in female dogs inoculated with Rickettsia rickettsii andRickettsia montana. Am. J. Vet. Res. 49:70-76.
3. Broqui, P., and D. Raoult. 1990. In vitro susceptibility ofEhrlichia sennetsu to antibiotics. Antimicrob. Agents Chemo-ther. 34:1593-1596.
4. Buhles, W. C., D. L. Huxsoll, G. Ruch, R. H. Kenyon, and B. L.Elisberg. 1975. Evaluation of primary blood monocyte and bonemarrow culture for the isolation of Rickettsia rickettsii. Infect.Immun. 12:1457-1463.
5. Centers for Disease Control. 1983. Annual summary 1982: re-ported morbidity and mortality in the United States. Morbid.Mortal. Weekly Rep. 31:142.
6. Clements, M. L., J. S. Dumler, P. Fiset, C. L. Wisseman, Jr.,M. J. Snyder, and-M. M. Levine. 1983. Serodiagnosis of RockyMountain spotted fever: comparison of IgM and IgG enzyme-linked immunoabsorbent assays and indirect fluorescent anti-body test. J. Infect. Dis. 148:876-880.
7. Davidson, M. G., E. B. Breitschwerdt, D. H. Walker, M. G.Levy, C. S. Carlson, E. M. Hardie, C. A. Grindem, and M. P.Nasisse. 1990. Vascular permeability and coagulation duringRickettsia rickettsii infection in dogs. Am. J. Vet. Res. 51:165-170.
8. Davis, J. P., C. M. Wilfert, D. J. Sexton, W. Burgdorfer, E. A.Casper, and R. N. Philip. 1981. Serologic comparison of R.rickettsii isolated from patients in North Carolina to R. rickettsiiisolated from patients in Montana, p. 139-147. In W. Burgdorferand R. L. Anacker (ed.), Rickettsiae and rickettsial diseases.Academic Press, Inc., New York.
9. Eaton, M., M. T. Cohen, D. R. Shlim, and B. Innes. 1989.Ciprofloxin treatment of typhus. JAMA 262:772-773. (Letter.)
10. Fishbein, D. B., M. G. Frontini, R. Giles, and L. L. Vernon.1990. Fatal cases of Rocky Mountain spotted fever in the UnitedStates, 1981-1988. Ann. N.Y. Acad. Sci. 590:246-247.
11. Greene, C. E., W. Burgdorfer, R. Cavagnolo, R. N. Philip, andM. G. Peacock. 1985. Rocky Mountain spotted fever in dogs andits differentiation from canine ehrlichiosis. J. Am. Vet. Med.Assoc. 186:465-472.
12. Gudiol, F., R. Paliares, J. Carratala, F. Bolao, J. Ariza, G. Rufi,and P. F. Viladrich. 1989. Randomized double-blind evaluationof ciprofloxacin and doxycycline for Mediterranean spottedfever. Antimicrob. Agents Chemother. 33:987-988.
13. Hattwick, M. A. W., R. J. L. O'Brien, and B. F. Hanson. 1976.Rocky Mountain spotted fever: epidemiology of an increasingproblem. Ann. Intern. Med. 84:732-739.
14. Hays, P. L. 1985. Rocky Mountain spotted fever in children inKansas: the diagnostic value of an IgM-specific immunofluores-cence assay. J. Infect. Dis. 151:369-370.
15. Helmick, C. G., K. W. Bernard, and L. J. D'Angelo. 1984.Rocky Mountain spotted fever: clinical, laboratory, and epide-miological features of 262 cases. J. Infect. Dis. 150:480-488.
16. Johnson, T. A., and D. W. Wichern. 1988. Applied multivariatestatistical analysis, 2nd ed., p. 607. Prentice-Hall, Inc., Engle-wood Cliffs, N.J.
17. Kaplowitz, L. G., J. V. Lange, J. J. Fischer, and D. H. Walker.1983. Correlation of rickettsial titers, circulating endotoxin andclinical features in Rocky Mountain spotted fever. Arch. Intern.Med. 143:1149-1151.
18. Keenan, K. P., W. C. Buhles, D. L. Huxsol, R. G. Wlliams,P. K. Hildebrandt, J. M. Campbell, and E. H. Stephenson. 1977.Pathogenesis of infection of Rickettsia rickettsii in the dog: a
disease model for Rocky Mountain spotted fever. J. Infect. Dis.135:911-917.
19. Marrero, M., and D. Raoult. 1989. Centrifugation-shell vialtechnique for rapid detection of Mediterranean spotted feverrickettsiae in blood culture. Am. J. Trop. Med. Hyg. 40:197-199.
20. McClain, J. B., B. Joshi, and R. Rice. 1988. Chloramphenicol,gentamicin, and ciprofloxacin against murine scrub typhus.Antimicrob. Agents Chemother. 32:285-286.
21. Ormsbee, R. A., H. Parker, and E. G. Pickens. 1955. Thecomparative effectiveness of aureomycin, terramycin, chloram-phenicol, erythromycin, and thiomycetin in suppressing exper-imental rickettsial infections in chick embryos. J. Infect. Dis.96:162-167.
22. Philip, R. N., E. A. Casper, R. A. Ormsbee, M. G. Peacock, andW. Burgdorfer. 1976. Microimmunofluorescence test for theserologic study of Rocky Mountain spotted fever and typhus. J.Clin. Microbiol. 3:51-61.
23. Raoult, D., H. Gallais, P. De Micco, and P. Casanova. 1986.Ciprofloxacin therapy for Mediterranean spotted fever. Antimi-crob. Agents Chemother. 30:606-607.
24. Raoult, D., P. Roussellier, V. Galicher, R. Perez, and J. Tamalet.1986. In vitro susceptibility of Rickettsia conorii to ciprofloxacinas determined by suppressing lethality in chicken embryos andby plaque assay. Antimicrob. Agents Chemother. 29:424-425.
25. Raoult, D., P. Roussellier, V. Galicher, and J. Tamalet. 1987. Invitro antibiotic susceptibility of Rickettsia rickettsii and Rick-ettsia conorii: plaque assay and microplaque colorimetric assay.J. Infect. Dis. 155:1059-1061.
26. Raoult, D., and D. H. Walker. 1990. Rickettsia rickettsii andother spotted fever group rickettsiae (Rocky Mountain spottedfever and other spotted fevers), p. 1465-1471. In G. Mandell, R.G. Douglas, and J. E. Bennett (ed.), Principles and practice ofinfectious diseases, 3rd ed. Churchill Livingstone, New York.
27. Riond, J. L., and J. E. Riviere. 1989. Doxycycline binding toplasma albumin of several species. J. Vet. Pharmacol. Ther.12:253-260.
28. Smadel, J. E., E. B. Jackson, and A. B. Cruise. 1948. Chloro-mycetin in experimental infections. J. Immunol. 62:49-55.
29. Strand, O., and A. Stromberg. 1990. Ciprofloxacin treatment ofmurine typhus. Scand. J. Infect. Dis. 22:503-504.
30. Troy, G. C., and S. D. Forrester. 1990. Canine ehrlichiosis, p.404-418. In C. E. Greene (ed.), Infectious diseases of the dogand cat. W. B. Saunders, Philadelphia.
31. Tyczkowska, K. L., K. M. Hedeen, D. P. Aucoin, and A. L.Aronson. 1989. High performance liquid chromatographymethod for the simultaneous determination of enrofloxacin andits primary metabolite, ciprofloxacin, in canine serum andprostatic tissue. J. Chromatogr. 493:337-346.
32. Tyczkowska, K. L., K. M. Hedeen, D. P. Aucoin, and A. L.Aronson. 1988. Simple LC method for determination of chlor-amphenicol in equine, canine, and feline serum. J. Chromatogr.Sci. 26:533-536.
33. Walker, D. H., B. G. Cain, J. V. Lange, and A. Harrison. 1981.Pathologic and rickettsial events in tetracycline-treated experi-mental Rocky Mountain spotted fever, p. 347-362. In W.Burgdorfer, and R. L. Anacker (ed.), Rickettsiae and rickettsialdiseases. Academic Press, Inc., New York.
34. Walker, R. D., G. E. Stein, J. G. Hauptman, K. H. MacDonald,S. C. Budsberg, and E. J. Rosser, Jr. 1990. Serum and tissuecage fluid concentrations of ciprofloxacin after oral administra-tion of the drug to healthy dogs. Am. J. Vet. Res. 51:896-900.
35. Wisseman, C. L., and S. V. Ordonez. 1981. Actions of antibiot-ics on Rickettsia rickettsii. J. Infect. Dis. 153:626-627.
VOL. 35, 1991
on July 18, 2018 by guesthttp://aac.asm
.org/D
ownloaded from