Embed Size (px)
Citation preview

Crit Care Med 2012 Vol. 40, No. 7 2141
Anemia is frequent among criti-cally ill patients. Around 60% of the critically ill suffer from ane-mia upon intensive care unit
admission. Anemia is associated with in-creased length of stay, higher morbidity, and mortality (1, 2). The prevalence and severity of anemia upon discharge from the intensive care unit are also high, con-cerning up to 80% of the patients (3). Correcting anemia may thus be highly beneficial. Nowadays, blood transfusion is less frequent, as recommended trans-fusion thresholds have been decreased (3–5). There is a need to better under-stand the causes of anemia in this setting
and to consider additional therapeutic options.
The pathophysiology of anemia of the critically ill is complex. The two main fac-tors leading to iron deficiency are inflam-mation and blood loss (4, 6). Inflammation occurs in virtually all critically ill patients. Anemia of the critically ill is therefore con-sidered as an anemia of inflammation (7), characterized by iron-restricted erythro-poiesis with iron being diverted from the circulation and stored inside macrophages (8). Blood withdrawal is also a major cause of anemia during the intensive care unit stay, with a median blood loss of 128 mL per day, representing a daily iron loss of about
64 mg (1, 9, 10). Finally, iron deficiency is also common in critically ill patients, affecting around one third of all patients (11–13). Thus, iron may be considered as an option for treating anemia in critically ill patients (6, 14, 15). This option is sup-ported by the recent increase in knowledge on the regulation of iron metabolism.
Indeed, the discovery of hepcidin, the main regulator of iron metabolism, has opened up new therapeutic possibilities for critically ill anemic patients (6). Hepcidin expression is known to be highly inducible by inflammation and fully suppressed by in-creased bone marrow erythropoiesis. Using a mouse model mimicking critical care anemia, we have shown that stimulation of erythropoiesis by phlebotomy-induced iron deficiency may dominate over inflamma-tion for hepcidin regulation (16). In other words, in this model, despite inflammation, iron could be mobilized from the storage compartment and used for erythropoi-esis. These findings were confirmed in two other animal models where erythropoiesis stimulation through blood withdrawal or
Objective: Anemia is common in critically ill patients, due to inflammation and blood loss. Anemia can be associated with iron deficiency and low serum hepcidin levels. However, iron admin-istration in this setting remains controversial because of its po-tential toxicity, including oxidative stress induction and sepsis fa-cilitation. The objective of this work was to determine the efficacy and toxicity of iron administration using a mouse model mimicking critical care anemia as well as a model of acute septicemia.
Design: Prospective, randomized, open label controlled animal study.
Setting: University-based research laboratory.Subjects: C57BL/6 and OF1 mice.Interventions: Intraperitoneal injection of zymosan inducing
generalized inflammation in C57BL/6 mice, followed in our full model by repeated phlebotomies. A dose equivalent to 15 mg/kg of ferric carboxymaltose was injected intravenously on day 5. To assess the toxicity of iron in a septicemia model, OF1 mice were simultaneously injected with iron and different Escherichia coli strains.
Measurements and Main Results: To investigate the effect of iron on oxidative stress, we measured reactive oxygen species production in the blood using luminol-amplified chemiluminescence and super-oxide dismutase 2 messenger RNA levels in the liver. These markers of oxidative stress were increased after iron administration in control mice but not in zymosan-treated mice. Liver catalase messenger RNA levels decreased in iron-treated control mice. Iron administration was not associated with increased mortality in the septicemia model or in the generalized inflammation model. Iron increased hemoglobin levels in mice fed with a low iron diet and subjected to phlebotomies and zymosan 2 wks after treatment administration.
Conclusions: Adverse effects of intravenous iron supplementa-tion by ferric carboxymaltose seem to be minimal in our animal models. Furthermore, iron appears to be effective in correcting anemia, despite inflammation. Studies of efficacy and safety of iron in critically ill patients are warranted. (Crit Care Med 2012; 40: 2141–2148)
KEY WORDS: anemia; critical care; iron; mice; oxidative stress; septicemia
Efficacy and toxicity of intravenous iron in a mouse model of critical care anemia*
Nicholas Heming, MD; Philippe Lettéron, PhD; Fathi Driss, MD, PhD; Sarah Millot, MD; Jamel El Benna, PhD; Jérome Tourret, MD, PhD; Erick Denamur, MD, PhD; Philippe Montravers, MD, PhD; Carole Beaumont, PhD; Sigismond Lasocki, MD, PhD
*See also p. 2252.From the INSERM U773 (NH, PL, FD, SM, JEB, CB,
SL), Univ Paris Diderot, Sorbonne Paris Cité, Site Bichat, Paris, France; Assistance Publique–Hôpitaux de Paris (NH, PM), Hôpital Bichat, Service d’Anesthésie-Réanimation Chirurgicale, Paris, France, Univ Paris Diderot, Sorbonne Paris Cité, Site Bichat, Paris, France; INSERM U722 (JT, ED), Univ Paris Diderot, Sorbonne Paris Cité, Site Bichat, Paris, France; and Université d’Angers (SL), Pole d’Anesthésie Réanimation CHU Angers, Angers, France.
Dr. Heming received grant support from the Fondation pour la Recherche Médicale. Supported, in part, by a grant from Vifor Pharma France to INSERM U773.
The authors have not disclosed any potential con-flicts of interest.
For information regarding this article, E-mail: [email protected]
Copyright © 2012 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins
DOI: 10.1097/CCM.0b013e31824e6713

2142 Crit Care Med 2012 Vol. 40, No. 7
erythropoietin treatment overrode inflam-mation for hepcidin regulation and allowed the mobilization of tissue iron (17, 18), and by the observation of low hepcidin levels in some critically ill patients (11).
Unfortunately, iron may also be toxic for critically ill patients. Iron has the abil-ity to donate electrons and may induce oxidative stress through the Fenton reac-tion. Iron may also facilitate infection and sepsis because it is an essential element for all living organisms, including patho-gens (19, 20). Indeed, high doses of iron have been shown to increase mortality in a mouse model of sepsis (21).
To address this controversy, we de-signed a study evaluating the efficacy and toxicity of intravenous iron supplemen-tation in mice in an inflammatory con-text, with or without iron deficiency. We assessed short-term toxicity of iron sup-plementation in both generalized inflam-mation and septicemia mouse models. Furthermore, we assessed long-term ef-ficacy of iron supplementation in a mouse model of critical care anemia (16).
MATERIALS AND METHODS
Animals. Mice were cared for in accor-dance with criteria outlined in the European Convention for the Protection of Laboratory Animals. The study received approval from the lo-cal authorities. Before use, animals were allowed to acclimatize for at least 3 days. Animals were maintained in a temperature and light-controlled environment and were given free access to tap water and normal iron diet (standard laboratory mouse chow, AO3; SAFE, Augy, France) unless otherwise specified. All reagents and compounds were obtained from Sigma, St. Quentin Fallavier, France, unless otherwise specified.
Zymosan-Induced Generalized Inflamma-tion Model, With or Without Phlebotomies. The zymosan-induced generalized inflamma-tion model (ZIGI) induces a septic shock-like syndrome in mice, leading to multiple organ dysfunctions (22). In this model, we used 8 to 10-wk-old C57BL/6 male mice, weighing 20–25 g (Centre d’Elevage Janvier, Le Genest St Isle, France). Because early mortality dramatically in-creased, most likely due to changing conditions in our central animal facility, we introduced mi-nor modifications to the initial model (i.e., a re-duction in zymosan A dose) (16). Inflammation was first induced by an intraperitoneal injection of 40 mg of Escherichia coli O128-B12 lipopoly-saccharide diluted in 200 mL saline solution, fol-lowed by an intraperitoneal injection of 10 mg of zymosan A diluted in 500 mL saline 3 days later. The lipopolysaccharide injection prevents an excessive response to zymosan A, by activat-ing the immune system, so that the ZIGI model constitutes a model of chronic inflammation. The day of zymosan injection is referred to as
day 1. No injections were performed on the con-trol animals.
The critical care anemia model consists of the combination of a low iron diet and phlebot-omies in mice previously treated by lipopoly-saccharide and zymosan A. Mice were provided with an iron-depleted diet (C1038, Genestil, Royancourt, France) starting 4 wks prior to zy-mosan administration and maintained during the whole experiment.
Phlebotomies were performed by with-drawal of 250–300 mL of blood from the orbital sinus with a calibrated heparinized capillary tube on days 1, 2, and 4, as previously described (16). Blood obtained on day 4 was processed in the hematology laboratory for determination of hematological indices.
C57BL/6 mice received 0.3 mg of elemental iron in the form of Ferric carboxymaltose (fer-ric carboxymaltose; Ferinject, Vifor pharma, Fribourg, Switzerland) diluted in 100 mL of saline on day 5 by intravenous injection by the retro-orbital route under light-inhaled isoflu-rane (Belamont, Paris, France) anesthesia (23). Control mice received 100 mL of saline by the same route. The 0.3 mg dose of ferric carboxy-maltose was chosen because it is equivalent to 15 mg iron/kg body weight, which is the maximum dose of ferric carboxymaltose that may be given in one shot to human beings.Furthermore, this dose covered the estimated iron loss resulting from repeated blood with-drawals (around 0.23–0.28 mg). Mice were killed either 4 hrs later for short-term experi-ments or on day 19 (i.e., 2 wks after iron in-jection) for long-term experiments. A total of 55 mice divided into four groups were used for the short-term experiments. Eighteen of these mice died within 4 days of zymosan administra-tion, leaving 37 mice alive, which were divided into four groups of 8–11 animals. A total of 51 mice divided into five groups of 5–15 animals were used for the long-term experiments.
Septicemia Mouse Model. The septicemia mouse model was performed using 14–16 g OF1 female mice (Charles River, L’Arbresle, France), as previously described (24). Briefly, E. coli strains were grown on Luria–Bertani agar for 24 hrs. One colony was then picked up and grown overnight in a Luria–Bertani broth at 37°C. After two washes in saline, bacteria were diluted to the chosen inoculum. E. coli inoculum was controlled for each experiment by serial plat-ing. OF1 mice were simultaneously given an intravenous injection of 0.2 mg (equivalent to 15 mg iron/kg body weight) ferric carboxymalt-ose diluted in 100 mL of saline or saline alone, and a subcutaneous injection of 106, 107, or 108 colony forming units (CFU) of the bacteria di-luted in 200 mL of saline. Mortality was assessed during the following week. In this model, E. coli natural isolates inoculated at 108 CFU are either “killer” (>90% of inoculated mice killed) or “nonkiller” (<10% of inoculated mice killed), and very few strains have intermediary lethal-ity (25). In order to observe increased mortality rates after iron administration in this model, we chose two bacterial strains with intermediate
levels of virulence in mice (IAI76 and IAI78) (24) and modulated the inoculum to obtain between 0% and 50% of inoculated mice killed. These two strains were isolated from urinary tract infections, belong to the B2 phylogenetic group associated with extraintestinal virulence, and bear various virulence determinants includ-ing the iron capture systems yersiniabactin and iron (IAI76) and yersiniabactin and aerobactin (IAI78) (25). Each experiment was conducted on two groups of 25 mice. Both groups received the same bacterial strain at the same concen-tration; the first group additionally received saline whilst the second group received ferric carboxymaltose.
Specimen Collection. On the day the mice were killed, they were weighed. Blood was col-lected by puncture of the orbital sinus as for phle-botomy (see above), and the heparinized sample was sent to the hematology laboratory for deter-mination of hematologic indices using a Sysmex XE 2100 automate (Roche Diagnostics, Meylan, France). Mice were then killed by cervical dislo-cation. The abdomen was opened; the liver and spleen were removed. Samples of liver and spleen were aseptically collected and immediately fro-zen in liquid nitrogen and stored at 280°C.
Whole Blood Chemiluminescence. Phagocyte stimulation activates the nicotinamide adenine dinucleotide phosphate oxidase-2, which produc-es superoxide anions and generates other reactive oxygen species, such as hydrogen peroxide. This phagocyte function can be evaluated by the lumi-nol-amplified chemiluminescence technique, as previously described (26). Briefly, 2.5 mL of freshly isolated whole blood was resuspended in 0.5 mL Hank’s buffered salt solution containing 10 mM luminol and 5 units of horseradish peroxidase, and was left at room temperature in the chamber of the luminometer (Berthold–Biolumat LB937) and allowed to stabilize. After a baseline reading, cells were stimulated with 1026 M of formyl-Met-Leu-Phe. Changes in chemiluminescence were measured over a 15-min period. The peak of chemiluminescence after formyl-Met-Leu-Phe stimulation is reported. Peaks were normalized by the neutrophil blood count, and determined by blood smear examination and by the peak value of chemiluminescence after formyl-Met-Leu-Phe stimulation of control animals measured on the same day.
Determination of Advanced Oxidation Protein Products. Protein oxidation was mea-sured in plasma separated from blood by de-termining the advanced oxidation protein products (AOPP) level spectrophotometrically (27). Briefly, 0.1 mL of plasma diluted 1/10 in phosphate buffered saline was mixed with 5 mL of acetic acid and 2.5 mL of 1.16 M potassium iodide in test tubes. The absorbance of the reaction mixture was read at 340 nm. 0.1 mL of 0–100 mmol/L chloramine T was added in standard tubes. The absorbance of chloramine T was linear between 0 and 100 mmol/L.
RNA Extraction and Quantitative Real Time–Polymerase Chain Reaction. Total RNA was extracted from livers using the RNA plus Extraction Solution Kit (MP Biomedicals SA,

Crit Care Med 2012 Vol. 40, No. 7 2143
Ilkrich, France), according to the manufac-turer’s instruction. The purity and yield of total RNA were determined spectrophotometrically. The integrity of ribosomal RNA bands (18S and 28S) was checked on agarose gel electro-phoresis. Single-strand complementary DNA was synthesized using SuperScript II Reverse Transcriptase (Invitrogen Life Technologies, Cergy-Pontoise, France). Real-time polymerase chain reaction quantification of transcripts was performed in 20 mL reactions using the SYBER green I master mix (Roche Diagnostics, Mannheim, Germany), 10 pmol of forward (Fwd) and reverse (Rev) primers, 5 mL of re-verse transcriptase reaction mixture, and the LightCycler 480 (Roche Diagnostics, Rotkreuz, Switzerland), as previously described (16). The following conditions were used: 3 mins dena-turation at 95°C followed by 40 cycles at 95°C during 30 secs, and 60°C during 60 secs. All samples were analyzed in duplicate. Analyses were performed with the LightCycler 480 Software v1.5 (Roche Diagnostics, Rotkreuz, Switzerland). The expression of tested genes was normalized by that of housekeeping genes, Glyceraldehyde-3- phosphate dehydrogenase, Hypoxanthine phosphoribosyl-transferase I, and -2-microglobulin, and the geNorm pro-gram (28). Primers were designed using the primer-BLAST software (http://www.ncbi.nlm.nih.gov/; National Center for Biotechnology Information, National Library of Medicine, Bethesda, MD). Forward and reverse primers were designed to span at least one large intron. Primers were obtained from Eurogentec France SA (Angers, France). Primer sequences are given in Table 1. The amplification efficiency of each target was determined using two-fold se-rial dilutions of pooled complementary DNA for each experiment. The polymerase chain reac-tion efficiency in each case was close to 100%.
Organ Culture. For short-term toxicity evalu-ation, spleens were aseptically removed, homog-enized in saline solution, and plated. Bacterial counts were obtained by plating serial dilutions on blood agar, after 48 hrs of culture at 37°C.
Tissue Iron Determination. Tissue iron concentration was determined after tissue digestion by three different acids followed by quantification of iron using an IL test (Instrumentation Laboratory, Lexington, MA) and an Olympus AU400 automate (Chema Diagnostica, Monsano, Italy) (29). In order to determine the effect of the iron-restricted diet on tissue iron stocks, we compared control ani-mals receiving a normal diet (n 5) to control animals submitted to an iron poor diet.
Statistics and Data Analysis. All statistics were calculated using the Graphpad Prism v4,00 software (GraphPad Software, Inc., La Jolla, CA). Data are reported as median (interquartile range) or as percentage as appropriate. The number of observations is reported for each data and each group. Mann–Whitney tests were performed for between-group comparisons. Survival dif-ferences were determined by the Logrank test. Categorical data were compared using the Fisher’s exact test. The Bonferroni correction
for multiple comparisons was used for analysis of hematological parameters. All tests were two-tailed. p.05 was considered significant.
RESULTS
Short-Term Pro-Oxidant Effect of Intravenous Iron. In order to determine whether administration of intravenous iron was associated with the occurrence
of oxidative stress, we assessed the activ-ity of the phagocytes’ (mainly neutrophil) nicotinamide adenine dinucleotide phos-phate oxidase-2, by whole-blood chemilu-minescence and the level of mRNA coding for antioxidant enzymes in the liver of control and ZIGI mice (Fig. 1). In control mice, whole-blood chemiluminescence was higher in iron-treated than in saline-treated mice. Surprisingly, in ZIGI mice
Table 1. Primer sequences
Symbol Forward Primer Reverse Primer
B2m CATGGCTCGCTCGGTGACC AATGTGAGGCGGGTGGAACTGGapd TGAAGCAGGCATCTGAGGG CGAAGGTGGAAGAGTGGGAGHprtI AGCTACTGTAATGATCAGTCAACG AGAGGTCCTTTTCACCAGCASod2 CCAGCGGGCCTACGTGAACA TGCAGGCTGAAGAGCGACCTGCat GCAGTGGAAGGAGCAGCGGG ATTGGGTTCCCGCCTCCGGTHepc GCAGACATTGCGATACCA CAGATACCACACTGGGAATT
B2m, -2-microglobulin; Gapd, glyceraldehyde-3-phosphate dehydrogenase; HprtI, hypoxanthine phosphoribosyl-transferase I; Sod2, superoxide dismutase 2; Cat, catalase; Hepc, hepcidin.
A B
C D
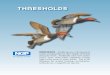
Figure 1. Short-term oxidative stress induced by iron in zymosan-treated mice. Whole blood chemi-luminescence after addition of formyl-Met-Leu-Phe (FMLP) (A) and serum advanced oxidation protein products (AOPP) concentrations (B) in control and zymosan-treated mice 4 hrs after administration of intravenous iron (1) or saline (2). Quantitative reverse transcriptase–polymerase chain reaction of sod2 (C) and catalase (D) messenger RNA (mRNA) in the liver of control and zymosan-treated mice 4 hrs after administration of intravenous iron (1) or saline (2). Z, zymosan; Iron, intravenous iron administration. The lines represent the median value.

2144 Crit Care Med 2012 Vol. 40, No. 7
on day 5, chemiluminescence levels were similar in iron-treated and saline-treated mice (Fig. 1A).
We subsequently determined the levels of AOPP in the plasma, an indirect marker of tissue oxidative stress. AOPP levels were higher, albeit without reaching statistical significance, in control mice treated with iron than in control animals treated with saline. ZIGI mice exhibited similar levels of plasma AOPP, whether they had been treated with iron or saline (Fig. 1B).
We subsequently determined the he-patic expression of two genes coding for enzymes implicated in detoxifying reac-tive oxygen species, namely superoxide dismutase 2 (sod2) and catalase. Sod2 mRNA levels were higher in iron-treated control mice than in saline-treated con-trol animals. Conversely, iron-treated and saline-treated ZIGI mice had similar levels of expression of sod2 in the liver. Catalase expression was lower in iron-treated con-trol mice than in saline-treated control animals. The level of expression of cata-lase was comparable in both groups of ZIGI mice, albeit below the level of expres-sion of control animals (Fig. 1, C and D). The association of higher levels of sod2 and lower levels of catalase in control mice treated by iron could lead to the ex-cessive production of hydrogen peroxide,
and thus induce oxidative stress. This unbalance was not found in ZIGI mice. Overall, intravenous iron seems to induce oxidative stress in control mice, whereas ZIGI mice seem to be protected from iron-induced oxidative stress.
Short-term Pro-Infectious Effect of Intravenous Iron. The pro-infectious ef-fect of iron was assessed in both the ZIGI and the septicemia mouse models (Fig. 2). The ZIGI mouse model is considered to be due to a generalized inflammatory re-sponse, although bacterial translocation can also occur, as previously described (22). In order to demonstrate that bacterial translocation is present but not increased after iron administration, we determined the bacterial load in the spleen of control and ZIGI mice, treated by iron or saline. None of the control mice showed evidence of bacterial translocation. ZIGI mice were associated with significant bacterial translocation. Bacterial translocation was not modified by iron administration. As a matter of fact, ZIGI mice treated by iron or saline showed a comparable percentage of spleens containing bacteria (65% and 70% respectively, p 1) and a compara-ble median number of bacteria per mg of spleen (p .8, Fig. 2A).
We then determined whether the ad-ministration of iron was associated with
increased mortality rates using a mouse model of septicemia. E. coli IAI76 or IAI78 are extra-intestinal pathogenic strains with an intermediate level of virulence in the mouse model of septicemia (24). We first tested the model in conditions of very low mortality (“nonkiller”). When iron or saline was simultaneously administered with 106 CFU of E. coli of the IAI78 strain, no increased mortality was induced by iron after 7 days (0% mortality in both iron- and saline-treated mice, data not shown). The same was observed when the inoculum was increased to 107 CFU (4% mortality for iron and saline, p .9, Fig. 2B). We then tested the model in conditions of intermediate mortality by simultaneously administering iron or sa-line and 108 CFU of E. coli of the IAI76 strain. No increased mortality was ob-served with iron in these conditions, after 7 days (32% mortality for iron vs. 44% for saline, p .4) (Fig. 2C).
Intravenous iron was not associated with an increased mortality in these E. coli–induced septicemia models, nor with increased bacterial translocation in the ZIGI model.
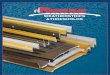
Long-Term Efficacy and Toxicity of Intravenous Iron in a Mouse Model of Critical Care Anemia. The critical care anemia model was obtained by combining the ZIGI model with phlebotomies and by feeding the animals with a low iron diet. Control mice were also fed the iron defi-cient diet. Figure 3A is a schematic repre-sentation of the experimental protocol.
We confirmed that our model was a “true” model of iron deficiency by mea-suring hepcidin mRNA levels and iron stores in the liver and spleen.
Liver hepcidin mRNA levels on day 19 (corresponding to 7 wks of iron-restricted diet) in C, C1P1S, and C1P1I animals were undetectable confirming iron de-ficiency and the repression of hepcidin. Z1P1S and Z1P1I animals had low levels of hepcidin expression, but higher in Z1P1I with respectively 4.731023
[2.931023210.831023] and 68.131023
[34.4310232100.331023] fold control (p .02).
Lastly, we measured liver and spleen iron contents in our animals. Control an-imals receiving a normal diet had higher liver and spleen iron content than con-trol animals fed with an iron poor diet. Z1P1I animals also had higher liver and spleen iron content than Z1P1S animals (Fig. 3B). These results confirm that 1) our model is a true iron deficiency model; and 2) the iron treatment (only)
A
B C
Figure 2. Evaluation of the pro-infectious effect of intravenous iron. A, Spleen bacterial counts 4 hrs after administration of iron or saline to control or zymosan-induced generalized inflammation animals. Control mice treated by saline and zymosan-induced generalized inflammation mice treated by saline (Z1S) spleen bacterial counts were significantly different (p = .04 Wilcoxon test). Control mice treated by iron (C1I) and zymosan-induced generalized inflammation mice treated by iron (Z1I) spleen bacte-rial counts were significantly different (p = .02 Wilcoxon test). There was no statistical difference between Z1S and Z1I spleen bacterial counts. B, Survival curve of animals simultaneously treated by intrave-nous iron (dotted line) or saline (bold line) and 107 colony forming units (CFU) Escherichia coli of the IAI78 strain by the subcutaneous route. Logrank test n.s. C, Survival curve of animals simultaneously treated by intravenous iron (dotted line) or saline (bold line) and 108 CFU Escherichia coli of the IAI76 strain by the subcutaneous route. Logrank test nonsignificant. The lines represent the median value.

Crit Care Med 2012 Vol. 40, No. 7 2145
partially restore iron stores in control and ZIGI mice.
No death was recorded in the nonphle-botomized control group (C) nor in the control and phlebotomy group, whether
mice had been treated by iron (C1P1I) or by saline (C1P1S). After zymosan ad-ministration and during 1–2 days, mice became lethargic, had ruffled fur, and di-arrhea. In the phlebotomized ZIGI mice,
3-wk mortality rates were indistinguish-able between the iron-treated (Z1P1I) and saline-treated (Z1P1S) groups (47% mortality in both groups, p 1) (Fig. 3C).
Hematological parameters before ei-ther iron or saline administration (day 4) showed that both control and ZIGI mice were anemic and that phlebo-tomized ZIGI mice (Z1P) had signifi-cantly lower hemoglobin levels than phlebotomized control animals (C1P) (Table 2). Anemia was normocytic and poorly regenerative.
On day 19, there was a significant increase in hemoglobin levels in phle-botomized control mice treated by iron (C1P1I) compared to phlebotomized con-trol animals treated by saline (C1P1S), although hemoglobin levels remained below that of nonphlebotomized control mice (C; Table 3). Iron administration to the phlebotomized ZIGI mice (Z1P1I) also raised hemoglobin levels significant-ly (compared to Z1P1S), although to a lesser extent than in the phlebotomized control animals (C1P1I), and was asso-ciated with a two- to three-fold increase in red blood cell number.
Overall, iron did not induce an increase in mortality rates in our mouse model of critical care anemia. In phlebotomized ZIGI mice, iron was partially effective in increasing the number of red blood cells and hemoglobin levels, even in the pres-ence of inflammation.
DISCUSSION
In this study, we investigated efficacy as well as short- and long-term toxicity of intravenous iron in a mouse model of crit-ical care anemia. We observed that iron induces little toxicity while being partially effective in correcting mixed, inflamma-tory, and iron deficiency–linked anemia in this animal model. These observations are at odds with the common thought that iron could be toxic and/or inefficient in the critical care context (30).
Indeed, administration of iron to criti-cally ill patients may theoretically induce two types of toxicities: 1) Labile iron may promote the formation of reactive oxygen species through the Fenton reaction; 2) Increased iron availability may promote pathogen growth and proliferation and have pro-infectious effects. The most sur-prising finding of this study is that iron administration in inflammatory mice induces little to no oxidative stress, com-pared to control mice. Furthermore, iron
Table 2. Hematological parameters prior to iron injections (day 4)
Control 1 Phlebotomy (C1P; n 16)
Zymosan 1 Phlebotomy (Z1P; n 18) p
White blood cell count (109/L) 6.99 [6.48–7.65] 4.28 [2.78–4.94] .0001Red blood cell count (1012/L) 5.55 [5.29–5.89] 4.56 [4.22–4.95] .0001Hemoglobin (g/L) 77 [67–80] 61 [56−66] .0001Mean corpuscular volume (fL) 44.6 [43.9–45.3] 44.3 [43.8–45] n.s.Mean corpuscular hemoglobin
concentration (g/dL)30.1 [29.4–30.4] 29.9 [29.4–30.2] n.s.
Reticulocytes (109/L) 292 [265–323] 353 [158–425] n.s.
C1P, control mice bled by three phlebotomies; Z1P, zymosan mice bled by three phlebotomies; n.s., nonsignificant.
Values are given as median [quartile 1–quartile 3].All mice were fed an iron poor diet starting 4 wks prior and were maintained throughout the
experiment.
Figure 3. A, Mouse model of critical care anemia. All animals were fed with an iron poor diet starting 4 wks before and during the whole experimentation. Inflammation was obtained by an intraperitoneal (IP) injection of 40 µg lipopolysaccharide (LPS) followed by a single IP injection of 0.4 mg/g zymosan 3 days later. The day of zymosan injection is considered as day 1 (D1). Phlebotomies were performed on D1, day 2 (D2), and day 4 (D4). Ferric carboxymaltose (0.15 mg elemental iron/kg) was administered intravenously (IV) on day 5 (D5). Mice were killed on day 19 (D19). B, Tissue iron content. All tissues where harvested on D19. The lines represent the median value. C, Long-term toxicity of iron in a mouse model of critical care anemia. Survival curves of phlebotomized zymosan-induced generalized inflam-mation mice maintained on an iron poor diet and treated by intravenous iron (dotted line; zymosan-induced generalized inflammation-phlebotomized mice treated by iron [Z1P1I]) or saline (bold line; zymosan-induced generalized inflammation-phlebotomized mice treated by saline [Z1P1S]). Logrank test nonsignificant. C, control; The lines represent the median value.
A
B
C

2146 Crit Care Med 2012 Vol. 40, No. 7
administration does not increase mortal-ity in any of our models, including the septicemia model.
First, we showed that, in vivo, iron activates blood neutrophils in control mice, as evidenced by increased chemi-luminescence production, and moder-ately increases the production of protein oxidation markers. This is in accordance with several studies showing an increase in plasma oxidative stress markers follow-ing iron injections in chronic hemodialy-sis patients (31, 32). Others, however, did not observe increased oxidative stress formation following iron injections in chronic hemodialysis patients (33). We did not find any increase in chemilumi-nescence production in ZIGI mice. This may be due to the lower generation of labile plasma iron following iron injec-tion in inflammatory mice. Indeed, these mice have a lower transferrin saturation (16), thereby offering a higher buffer-ing capacity towards exogenous iron. Furthermore, macrophage activation could also increase the clearance rate of colloidal iron. Finally, the form of iron we used (ferric carboxymaltose) may be associated with a lower induction of oxi-dative stress (34). We also found that iron administration induces adaptive changes in enzymes implicated in oxidative stress metabolism in the liver. In control mice, iron induced an increased expression of sod2 and a decreased expression of cata-lase. Sod2 catalyzes the transformation of the superoxide radical to hydrogen peroxide, whereas catalase catalyzes the transformation of hydrogen peroxide into water. Of note, messenger RNA levels of
catalase and sod2 have been shown to be closely correlated with the final enzy-matic activities of the respective enzymes (35). Thus, the association of higher lev-els of sod2 and lower levels of catalase observed in control mice treated by iron could lead to the excessive production of hydrogen peroxide and thus induce oxidative stress. These findings have previously been reported in inflamma-tory situations (35–37). The mechanism leading to a decreased expression of cata-lase is not clear. Catalase expression has been shown to be negatively regulated in response to cytokine stimulation such as interleukin-1, tumor necrosis factor–, and interferon-g (37). ZIGI animals did not show evidence of a change in the level of expression of catalase or sod2 after iron administration, possibly be-cause of an earlier insult resulting in their downregulation or because of a decrease in the level of iron induced-oxidative stress. Overall, there was no evidence in favor of iron toxicity in our experiments, or in favor of its pro-infectious activity. Using two E. coli strains in a septicemia model, we have shown that intravenous iron does not increase mouse mortality. Each strain had different iron uptake and acquisition systems; the three main siderophore systems were represented in the different strains we used. The three experimental conditions that we have used mimic different pathological situations ranging from septicemia with no or very low mortality rates to septic shock associated with 30%–40% mor-tality rates. In addition, the ZIGI model is also partly an infectious model (22),
with bacterial translocation (i.e., posi-tive spleen cultures, at day 5) concerning more than two thirds of the animals. We observed no increase in short- (day 5) or long-term (day 19) mortality in either the ZIGI model or our mouse model of criti-cal care anemia. Our findings are in con-tradiction with those of Javadi et al (21), where iron was administered in a model of peritonitis secondary to caecal ligation and puncture, and was associated with increased mortality rates. These differ-ences might be explained by the fact that Javadi et al administered very high doses of iron (5 mg of iron dextrose daily during 5 days). We used an iron dosage closer to everyday clinical practice (equivalent to 15 mg/kg of ferric carboxymaltose given in a single injection). In clinical prac-tice, several large observational studies of chronic kidney failure patients showed no link between the administration of intravenous iron and the prevalence of infection or bacteremia (38, 39). Lastly, a recent meta-analysis including 13 ran-domized clinical trials did not identify any relationship between iron adminis-tration and infection (40). Even if these studies probably do not have the power to detect differences in infection rate, they are in accordance with our results show-ing no increase in mortality rates when clinically relevant doses of intravenous iron are used.
Finally, we showed that intravenous iron corrected critical care anemia, at least partially. This was achieved without coadministration of erythropoiesis stimu-lating agents. This is in accordance with our previous work using the same animal
Table 3. Hematological parameters 15 days after iron administration (day 19)
C (n 5 5) C1P1S (n 5 8) C1P1I (n 5 8) Z1P1S (n 5 8) Z1P1I (n 5 8)
White blood cell count (109/L)
6.08 [6.04–6.28] 4.45 [4.3–4.7] 2.97 [2.61–4.17]a 6.99 [5.25–8.9]c 5.19 [4.99–5.48]
Red blood cell count (1012/L)
8.77 [8.53–9.3] 5.2 [4.54–5.29] 7.94 [7.65–8.41]a,b 2.81 [2.57–3.28]a,b 6.46 [6.21–6.88]a,b,c,d
Hemoglobin (g/L) 117 [115−129] 62 [55−64]a 106 [101−111]b 38 [33−43]a,b,c 85 [77−89]a,b,c,d
Mean corpuscular volume (fL)
41 [40.9–41.4] 40.6 [40–40.9] 42.2 [41.4–42.9] 43 [42.1–43.9] 39.4 [39–39.8]c
Mean corpuscular hemoglobin concentration (g/dL)
33.4 [32.8–33.9] 30 [29.1–31.1]a 31.9 [31.1–32.2] 30.7 [29.7–31.1]a 30.9 [30.3–32.1]
Reticulocytes (109/L) 360 [358–400] 255 [101–316] 315 [286–319] 249 [207–625]a 355 [329–387]d
C, control mice; C1P1S, control phlebotomized mice treated by saline; C1P1I, control phlebotomized mice treated by iron; Z1P1S, zymosan-induced generalized inflammation–phlebotomized mice treated by saline; Z1P1I, zymosan-induced generalized inflammation–phlebotomized mice treated by iron.
ap.05 compared to C; bp.05 compared to C1P1S; cp.05 compared to C1P1I; dp.05 compared to Z1P1S.Values are given as median [quartile 1–quartile 3].All mice were fed an iron poor diet starting 4 wks prior and were maintained throughout the experiment.

Crit Care Med 2012 Vol. 40, No. 7 2147
model, showing that hepcidin synthesis is repressed and iron mobilized from tissue stores when blood withdrawal is associ-ated to inflammation (16). We confirmed here the repression of hepcidin synthesis by iron deficiency (or blood withdraw-als), despite inflammation, as observed in other animal models (17, 18). In a rat model, Theurl et al (17) showed that the repression of hepcidin synthesis observed in the combined situation of inflamma-tion and blood withdrawals was associated with iron being released from macrophag-es. Indeed, the repression of hepcidin is necessary to iron utilization. However, the correction of anemia remains par-tial, probably because proinflammatory cytokines, especially interferon-g, limit the bone marrow erythroid response (41). More importantly, in a clinical study car-ried out in critically ill patients, we also observed that serum hepcidin levels may be very low despite persistent inflamma-tion (11). It is also possible that the dose of iron we used was insufficient. The admin-istered dosage only covered the loss of iron secondary to blood withdrawals, but did not compensate the iron deficiency due to the low iron diet. Indeed, iron stores of the animals remained low despite iron admin-istration. Iron treatment could be of inter-est when true iron deficiency is associated with the anemia of inflammation (15).
Our model has several limitations. We may not have been able to detect oxidative stress in inflammatory mice because of an incorrect timeframe, i.e., transient oxi-dative stress could have appeared within the 4-hr period following iron injections. Although we chose to assess neutrophil activation and AOPP levels (two makers of oxidative stress) and activation of anti-oxidant defense enzymes in the liver, it is possible that other biological markers of oxidative stress would have given differ-ent results. We were nonetheless able to detect an increase in oxidative stress in con-trol animals treated by iron. Concerning the risk of iron supplementation in the context of sepsis, the ZIGI model used is not a direct infectious model and may not fully mimic the situation found in septic critically ill patients. We did, however, observe a high rate of bacterial transloca-tion associated with the ZIGI model, and we confirmed the absence of increased mortality in the septicemia model. Finally, we used a new intravenous iron formula-tion, ferric carboxymaltose, which has not yet been studied to the same extent as iron sucrose. The use of this product
seems to be safer and may explain some of the differences observed compared to the published literature (34).
CONCLUSIONS
In summary, we showed that intrave-nous iron in a mouse model of critical care anemia is associated with little toxic-ity and allowed partial correction of ane-mia. These findings warrant clinical trials aimed at correcting anemia in the critical care setting by iron supplementation.
ACKNOWLEDGMENTS
We thank Claudette Müller-Serieys for her help with the bacterial counts, Sarah Dion for her help in caring for the animals, Valérie Andrieu for her help with the blood smear analysis, and Stéphane Bouee for his kind advice regarding sta-tistical analysis.
REFERENCES
1. Vincent JL, Baron JF, Reinhart K, et al; ABC (Anemia and Blood Transfusion in Critical Care) Investigators: Anemia and blood transfusion in critically ill patients. JAMA 2002; 288:1499–1507
2. Corwin HL, Gettinger A, Pearl RG, et al: The CRIT Study: Anemia and blood transfusion in the critically ill–current clinical practice in the United States. Crit Care Med 2004; 32:39–52
3. Walsh TS, Lee RJ, Maciver CR, et al: Anemia during and at discharge from intensive care: The impact of restrictive blood transfusion practice. Intensive Care Med 2006; 32:100–109
4. Shander A: Anemia in the critically ill. Crit Care Clin 2004; 20:159–178
5. Hébert PC, Wells G, Blajchman MA, et al: A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999; 340:409–417
6. Lasocki S, Longrois D, Montravers P, et al: Hepcidin and anemia of the critically ill patient: Bench to bedside. Anesthesiology 2011; 114:688–694
7. Corwin HL, Krantz SB: Anemia of the critically ill: “Acute” anemia of chronic disease. Crit Care Med 2000; 28:3098–3099
8. Weiss G, Goodnough LT: Anemia of chronic disease. N Engl J Med 2005; 352:1011–1023
9. van Iperen CE, Gaillard CA, Kraaijenhagen RJ, et al: Response of erythropoiesis and iron metabolism to recombinant human erythropoietin in intensive care unit patients. Crit Care Med 2000; 28:2773–2778
10. von Ahsen N, Müller C, Serke S, et al: Important role of nondiagnostic blood loss and blunted erythropoietic response in the
anemia of medical intensive care patients. Crit Care Med 1999; 27:2630–2639
11. Lasocki S, Baron G, Driss F, et al: Diagnostic accuracy of serum hepcidin for iron deficiency in critically ill patients with anemia. Intensive Care Med 2010; 36:1044–1048
12. Bellamy MC, Gedney JA: Unrecognised iron deficiency in critical illness. Lancet 1998; 352:1903
13. Fernandez R, Tubau I, Masip J, et al: Low reticulocyte hemoglobin content is associated with a higher blood transfusion rate in critically ill patients: A cohort study. Anesthesiology 2010; 112:1211–1215
14. Pieracci FM, Barie PS: Diagnosis and management of iron-related anemias in critical illness. Crit Care Med 2006; 34:1898–1905
15. Heming N, Montravers P, Lasocki S: Iron deficiency in critically ill patients: Highlighting the role of hepcidin. Crit Care 2011; 15:210
16. Lasocki S, Millot S, Andrieu V, et al: Phlebotomies or erythropoietin injections allow mobilization of iron stores in a mouse model mimicking intensive care anemia. Crit Care Med 2008; 36:2388–2394
17. Theurl I, Aigner E, Theurl M, et al: Regulation of iron homeostasis in anemia of chronic disease and iron deficiency anemia: Diagnostic and therapeutic implications. Blood 2009; 113:5277–5286
18. Huang H, Constante M, Layoun A, et al: Contribution of STAT3 and SMAD4 pathways to the regulation of hepcidin by opposing stimuli. Blood 2009; 113:3593–3599
19. Pieracci FM, Barie PS: Iron and the risk of infection. Surg Infect (Larchmt) 2005; 6(Suppl 1):S41–S46
20. Marx JJ: Iron and infection: Competition between host and microbes for a precious element. Best Pract Res Clin Haematol 2002; 15:411–426
21. Javadi P, Buchman TG, Stromberg PE, et al: High-dose exogenous iron following cecal ligation and puncture increases mortality rate in mice and is associated with an increase in gut epithelial and splenic apoptosis. Crit Care Med 2004; 32:1178–1185
22. Volman TJ, Hendriks T, Goris RJ: Zymosan-induced generalized inflammation: Experi-mental studies into mechanisms leading to multiple organ dysfunction syndrome. Shock 2005; 23:291–297
23. Yardeni T, Eckhaus M, Morris HD, et al: Retro-orbital injections in mice. Lab Anim (NY) 2011; 40:155–160
24. Picard B, Garcia JS, Gouriou S, et al: The link between phylogeny and virulence in Escherichia coli extraintestinal infection. Infect Immun 1999; 67:546–553
25. Johnson JR, Clermont O, Menard M, et al: Experimental mouse lethality of Escherichia coli isolates, in relation to accessory traits, phylogenetic group, and ecological source. J Infect Dis 2006; 194:1141–1150
26. O’Dowd Y, Driss F, Dang PM, et al: Antioxidant effect of hydroxytyrosol, a polyphenol from olive oil: Scavenging of hydrogen peroxide

2148 Crit Care Med 2012 Vol. 40, No. 7
but not superoxide anion produced by human neutrophils. Biochem Pharmacol 2004; 68:2003–2008
27. Witko-Sarsat V, Friedlander M, Capeillère-Blandin C, et al: Advanced oxidation protein products as a novel marker of oxidative stress in uremia. Kidney Int 1996; 49:1304–1313
28. Vandesompele J, De Preter K, Pattyn F, et al: Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol 2002; 3:RESEARCH0034
29. Galy B, Ferring D, Minana B, et al: Altered body iron distribution and microcytosis in mice deficient in iron regulatory protein 2 (IRP2). Blood 2005; 106:2580–2589
30. Patruta SI, Hörl WH: Iron and infection. Kidney Int Suppl 1999; 69:S125–S130
31. Tovbin D, Mazor D, Vorobiov M, et al: Induction of protein oxidation by intravenous iron in hemodialysis patients: Role of inflammation. Am J Kidney Dis 2002; 40:1005–1012
32. Pai AB, Boyd AV, McQuade CR, et al: Comparison of oxidative stress markers
after intravenous administration of iron dextran, sodium ferric gluconate, and iron sucrose in patients undergoing hemodialysis. Pharmacotherapy 2007; 27:343–350
33. Malindretos P, Sarafidis PA, Rudenco I, et al: Slow intravenous iron administration does not aggravate oxidative stress and inflammatory biomarkers during hemodialysis: A comparative study between iron sucrose and iron dextran. Am J Nephrol 2007; 27:572–579
34. Toblli JE, Cao G, Olivieri L, et al: Comparison of the renal, cardiovascular and hepatic toxicity data of original intravenous iron compounds. Nephrol Dial Transplant 2010; 25:3631–3640
35. Hosakote YM, Liu T, Castro SM, et al: Respiratory syncytial virus induces oxidative stress by modulating antioxidant enzymes. Am J Respir Cell Mol Biol 2009; 41:348–357
36. Berkovich A, Massaro D, Clerch LB: Pertussis toxin alters the concentration and turnover of manganese superoxide dismutase in rat lung. Am J Physiol 1996; 271(6 Pt 1):L875–L879
37. Chung-man Ho J, Zheng S, Comhair SA, et al: Differential expression of manganese superoxide dismutase and catalase in lung cancer. Cancer Res 2001; 61:8578–8585
38. Aronoff GR, Bennett WM, Blumenthal S, et al; United States Iron Sucrose (Venofer) Clinical Trials Group: Iron sucrose in hemodialysis patients: Safety of replacement and maintenance regimens. Kidney Int 2004; 66:1193–1198
39. Hoen B, Paul-Dauphin A, Kessler M: Intravenous iron administration does not significantly increase the risk of bacteremia in chronic hemodialysis patients. Clin Nephrol 2002; 57:457–461
40. Notebaert E, Chauny JM, Albert M, et al: Short-term benefits and risks of intravenous iron: A systematic review and meta-analysis. Transfusion 2007; 47:1905–1918
41. Millot S, Andrieu V, Letteron P, et al: Erythropoietin stimulates spleen BMP4-dependent stress erythropoiesis and partially corrects anemia in a mouse model of generalized inflammation. Blood 2010; 116:6072–6081