Embed Size (px)
Citation preview
Efficacy and Safety of Nivolumab Plus Ipilimumab in Patients with Melanoma Metastatic to the Brain:
Results of the Phase II Study CheckMate 204
Hussein Tawbi,1 Peter Forsyth,2 Alain Algazi,3 Omid Hamid,4 F. Stephen Hodi,5 Stergios Moschos,6
Nikhil Khushalani,2 Rene Gonzalez,7 Christopher Lao,8 Michael Postow,9 Michael B. Atkins,10 Marc Ernstoff,11 Igor Puzanov,11 Ragini Kudchadkar,12 Reena Thomas,13 Ahmad Tarhini,14 Joel Jiang,15
Alexandre Avila,15 Sheena Demelo,15 Kim Margolin16
1University of Texas, MD Anderson Cancer Center, Houston, TX, USA; 2Moffitt Cancer Center and Research Institute, Tampa, FL, USA; 3University of California-San Francisco, San Francisco, CA, USA; 4The Angeles Clinic and Research Institute, Los Angeles, CA, USA;
5Dana-Farber Cancer Institute, Boston, MA, USA; 6University of North Carolina Lineberger Comprehensive Cancer Center, Chapel Hill, NC, USA; 7University of Colorado Comprehensive Cancer Center, Aurora, CO, USA; 8University of Michigan, Ann Arbor, MI, USA;
9Memorial Sloan Kettering Cancer Center and Weill Cornell Medical College, New York, NY, USA; 10Georgetown-Lombardi Comprehensive Cancer Center, Washington DC, USA; 11Roswell Park Cancer Institute, Buffalo, NY, USA; 12Winship Cancer Institute of Emory University,
Atlanta, GA, USA; 13Stanford University Hospital, Palo Alto, CA, USA; 14University of Pittsburgh Medical Center, Pittsburgh, PA, USA; 15Bristol-Myers Squibb, Princeton, NJ, USA; 16Department of Medical Oncology, City of Hope, Duarte, CA, USA.
Abstract Number 9507
Disclosure InformationHussein Tawbi, MD, PhD
I have the following financial relationships to disclose:
Consultant for: Bristol-Myers Squibb, Novartis, Roche/Genentech, Merck
Speaker’s Bureau for: None
Grant/Research support from: Bristol-Myers Squibb, Novartis, Roche/Genentech,
Merck, Celgene, GlaxoSmithKline
Stockholder in: None
Honoraria from: Bristol-Myers Squibb, Novartis, Roche/Genentech
Travel, accommodations, expenses from: Bristol-Myers Squibb, Novartis,
Roche/Genentech
Employee of: None
I will discuss the following off label use and/or investigational use in my
presentation: None
2
Background
• Melanoma brain metastases (MBM) are a common clinical presentation associated with
poor prognosis (median OS ~4-5 months)1
• Surgery and/or stereotactic radiation therapy (SRT) are widely used for oligometastatic
disease and whole brain radiation therapy (WBRT) for miliary or leptomeningeal disease
– No impact on survival or extracranial disease, significant early and late neurotoxicity
• BRAF-targeted therapy has demonstrated intracranial activity (dabrafenib, vemurafenib
and dabrafenib+trametinib)1-6
• Experience with immunotherapy is limited
– Ipilimumab (IPI): 18% disease control in 51 asymptomatic patients7
– IPI+fotemustine: 50% disease control in 20 asymptomatic patients8,9
– Pembrolizumab: 22% intracranial response in 18 asymptomatic patients10
OS = overall survival
1. Davies MA et al. Cancer 2011;117:1687-1696. 2. Long GV, Margolin KA. Am Soc Clin Oncol Educ Book. 2013:393-398. 3. Margolin K et al. Lancet Oncol. 2012;13:459-465. 4. Knisely JP et al. J Neurosurg. 2012;117:227-233. 5. Haanen J et al. Presented at SMR 13th International Congress; 2016. 6. Goldberg SB et al. Lancet Oncol. 2016;17:976-983. 7. Margolin K et al. Lancet Oncol 2012;13:459-465. 8. DiGiacomo A et al. Lancet Oncol 2012;13:879-886. 9. DiGiacomo A, Margolin K. Ann Oncol 2015;26:798-803. 10. Goldberg SB et al. Lancet Oncol 2016;17:976-983.
3
Study Overview
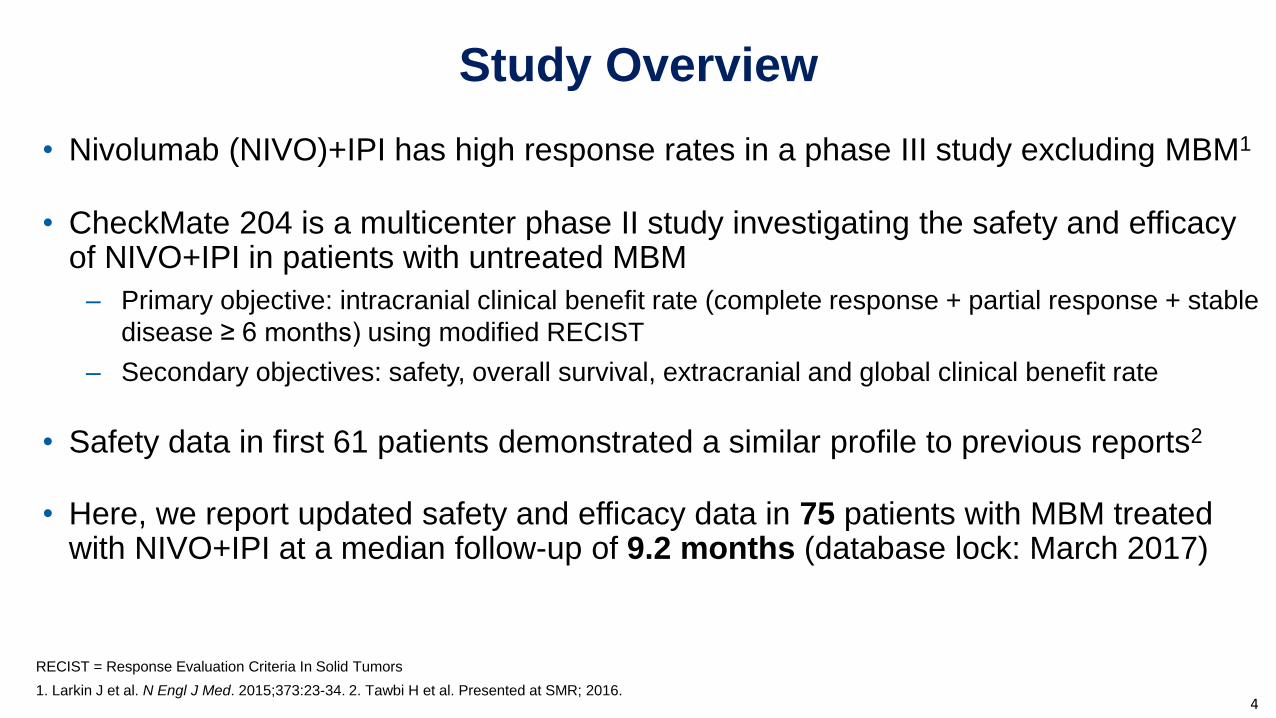
• Nivolumab (NIVO)+IPI has high response rates in a phase III study excluding MBM1
• CheckMate 204 is a multicenter phase II study investigating the safety and efficacy of NIVO+IPI in patients with untreated MBM
– Primary objective: intracranial clinical benefit rate (complete response + partial response + stable
disease ≥ 6 months) using modified RECIST
– Secondary objectives: safety, overall survival, extracranial and global clinical benefit rate
• Safety data in first 61 patients demonstrated a similar profile to previous reports2
• Here, we report updated safety and efficacy data in 75 patients with MBM treated with NIVO+IPI at a median follow-up of 9.2 months (database lock: March 2017)
4
RECIST = Response Evaluation Criteria In Solid Tumors
1. Larkin J et al. N Engl J Med. 2015;373:23-34. 2. Tawbi H et al. Presented at SMR; 2016.
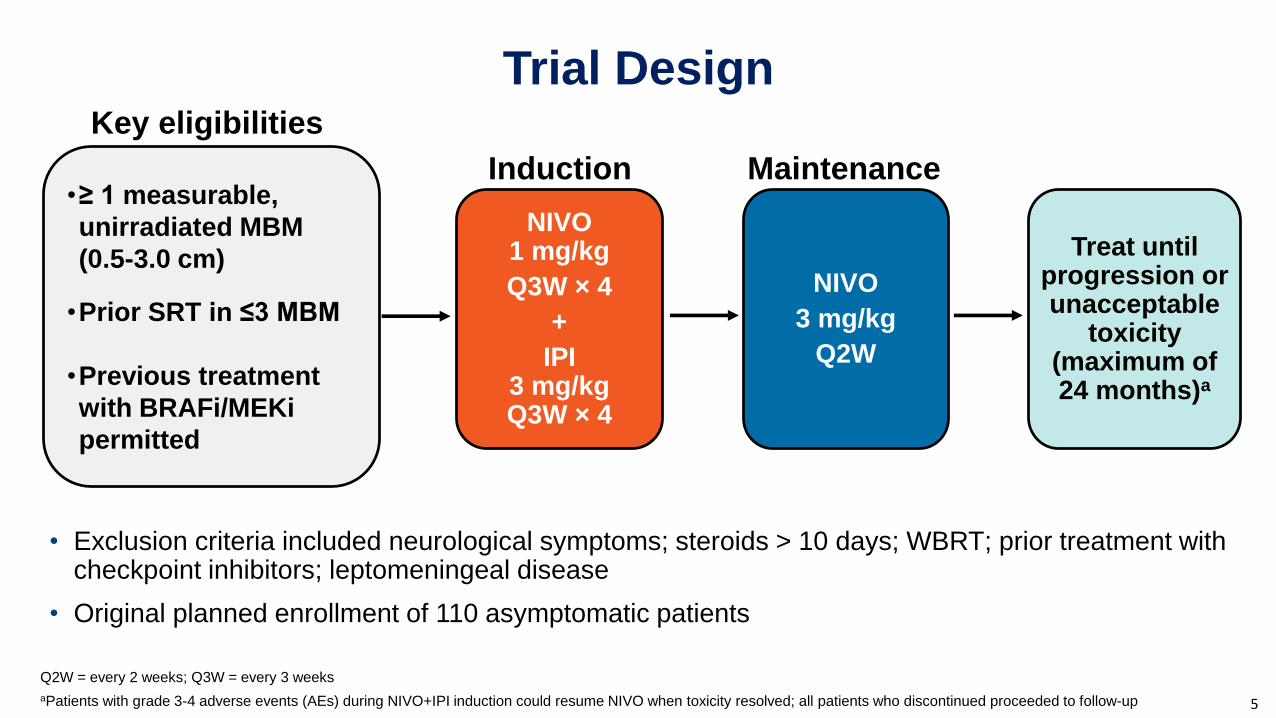
Trial Design
• Exclusion criteria included neurological symptoms; steroids > 10 days; WBRT; prior treatment with checkpoint inhibitors; leptomeningeal disease
• Original planned enrollment of 110 asymptomatic patients
NIVO1 mg/kg
Q3W × 4
+
IPI3 mg/kgQ3W × 4
NIVO
3 mg/kg
Q2W
Treat until progression or unacceptable
toxicity (maximum of 24 months)a
Induction Maintenance
5
•≥ 1 measurable,
unirradiated MBM
(0.5-3.0 cm)
•Prior SRT in ≤3 MBM
•Previous treatment
with BRAFi/MEKi
permitted
Key eligibilities
Q2W = every 2 weeks; Q3W = every 3 weeks
aPatients with grade 3-4 adverse events (AEs) during NIVO+IPI induction could resume NIVO when toxicity resolved; all patients who discontinued proceeded to follow-up
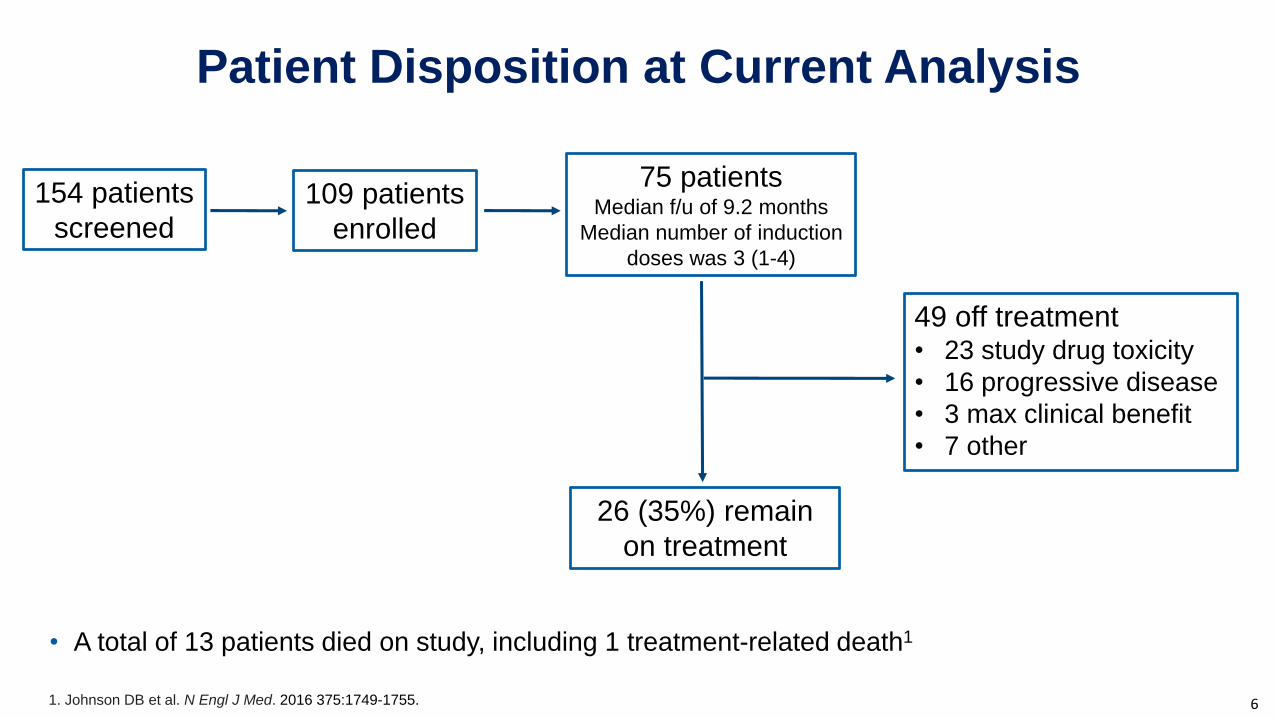
Patient Disposition at Current Analysis
• A total of 13 patients died on study, including 1 treatment-related death1
6
26 (35%) remain
on treatment
75 patients Median f/u of 9.2 months
Median number of induction
doses was 3 (1-4)
49 off treatment• 23 study drug toxicity
• 16 progressive disease
• 3 max clinical benefit
• 7 other
1. Johnson DB et al. N Engl J Med. 2016 375:1749-1755.
154 patients
screened109 patients
enrolled
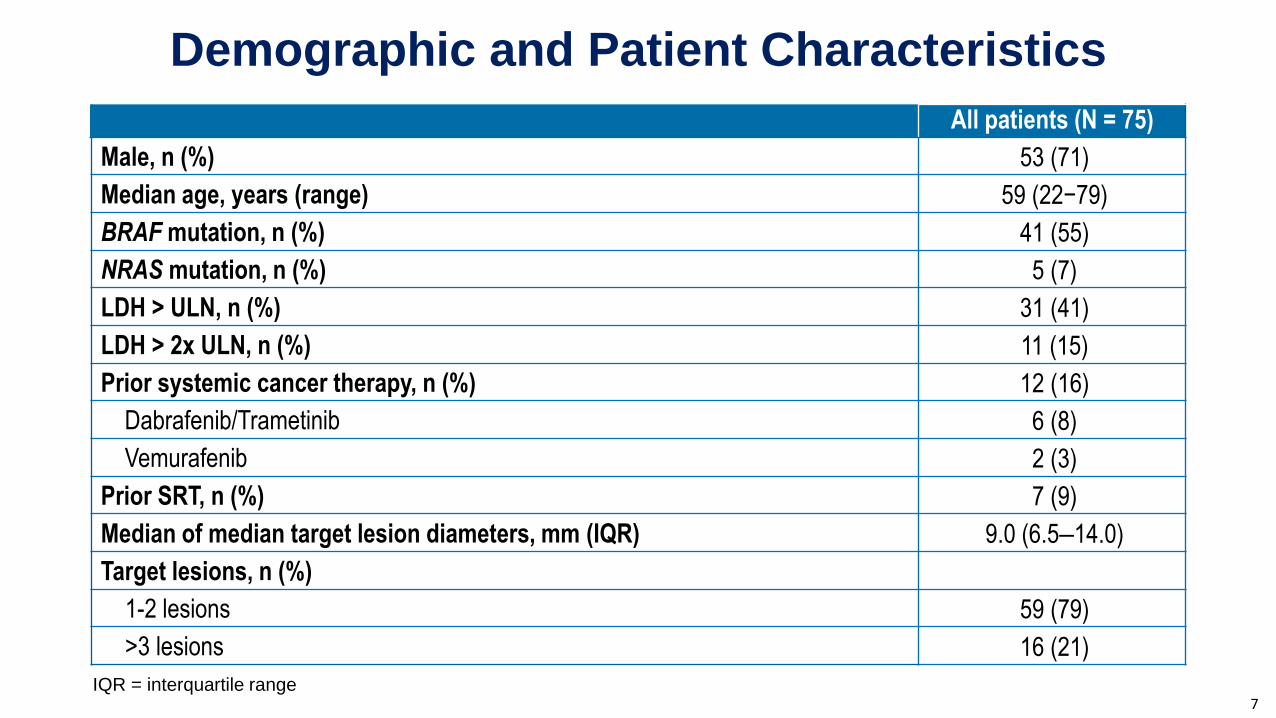
Demographic and Patient Characteristics
All patients (N = 75)
Male, n (%) 53 (71)
Median age, years (range) 59 (22−79)
BRAF mutation, n (%) 41 (55)
NRAS mutation, n (%) 5 (7)
LDH > ULN, n (%) 31 (41)
LDH > 2x ULN, n (%) 11 (15)
Prior systemic cancer therapy, n (%) 12 (16)
Dabrafenib/Trametinib 6 (8)
Vemurafenib 2 (3)
Prior SRT, n (%) 7 (9)
Median of median target lesion diameters, mm (IQR) 9.0 (6.5‒14.0)
Target lesions, n (%)
1-2 lesions 59 (79)
>3 lesions 16 (21)
7IQR = interquartile range
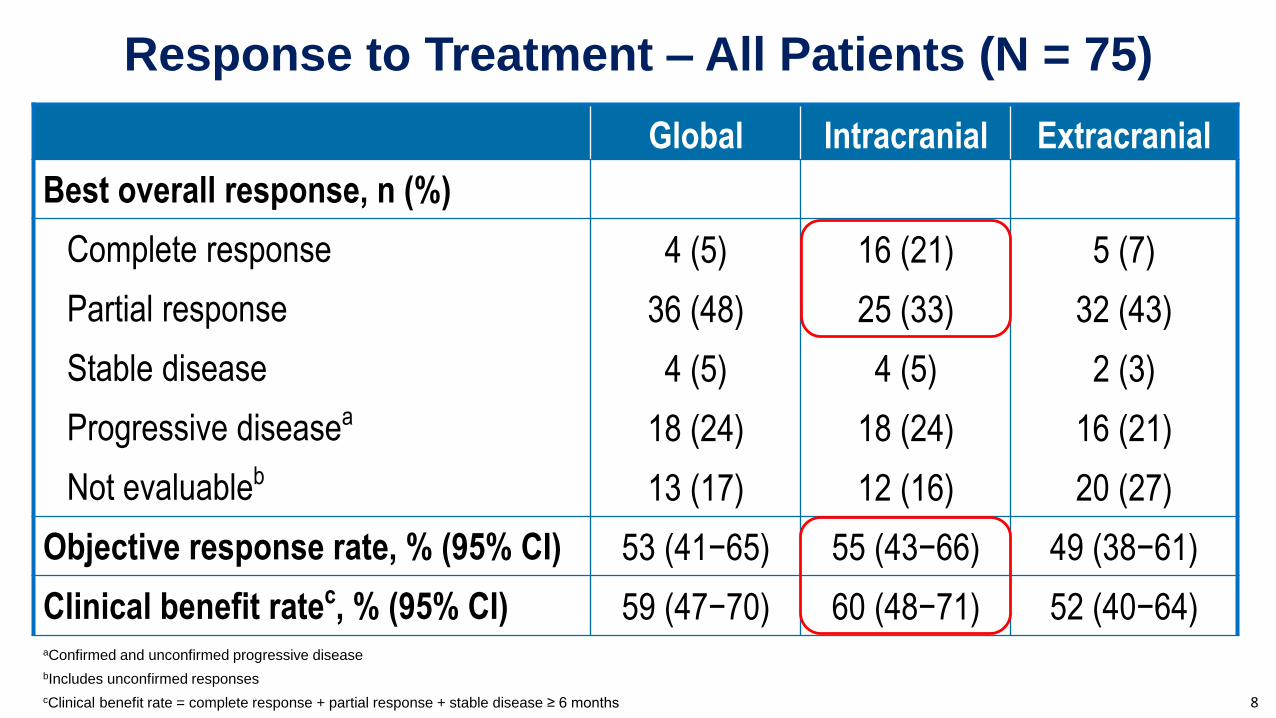
Response to Treatment – All Patients (N = 75)
8
Global Intracranial Extracranial
Best overall response, n (%)
Complete response 4 (5) 16 (21) 5 (7)
Partial response 36 (48) 25 (33) 32 (43)
Stable disease 4 (5) 4 (5) 2 (3)
Progressive diseasea 18 (24) 18 (24) 16 (21)
Not evaluableb 13 (17) 12 (16) 20 (27)
Objective response rate, % (95% CI) 53 (41−65) 55 (43−66) 49 (38−61)
Clinical benefit ratec, % (95% CI) 59 (47−70) 60 (48−71) 52 (40−64)aConfirmed and unconfirmed progressive disease
bIncludes unconfirmed responses
cClinical benefit rate = complete response + partial response + stable disease ≥ 6 months
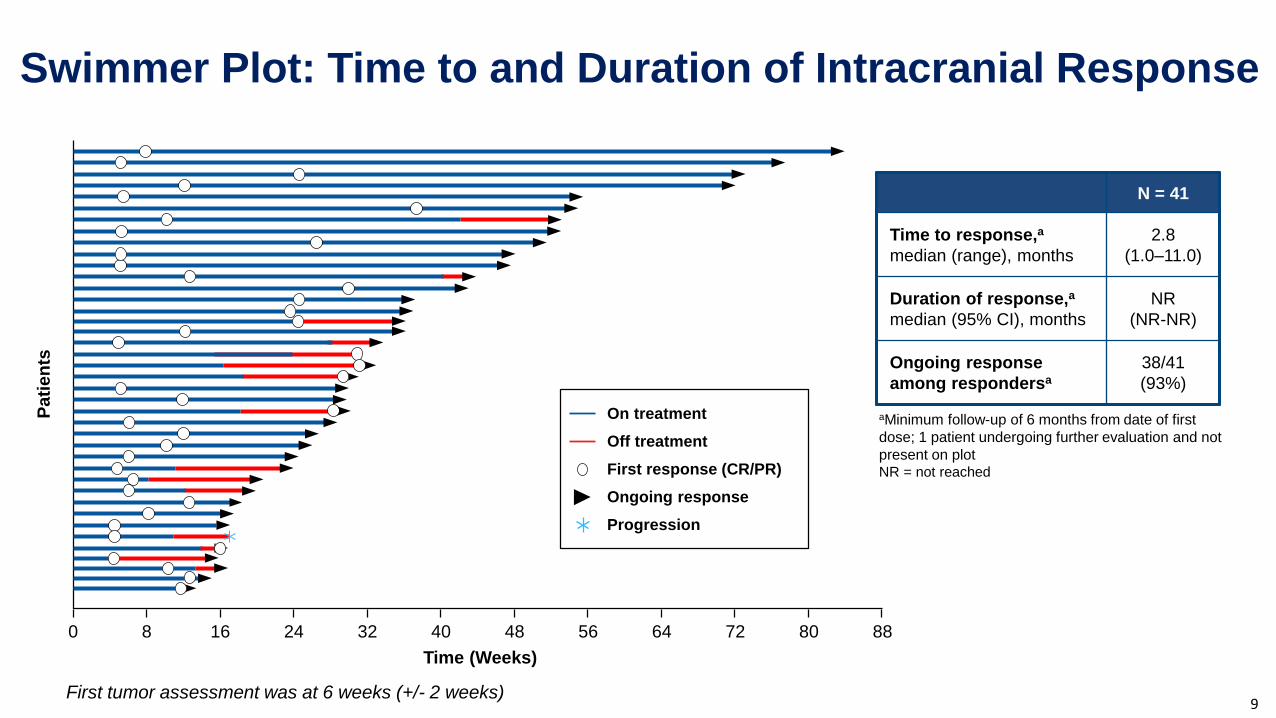
Swimmer Plot: Time to and Duration of Intracranial Response
N = 41
Time to response,a
median (range), months
2.8
(1.0–11.0)
Duration of response,a
median (95% CI), months
NR
(NR-NR)
Ongoing response
among respondersa
38/41
(93%)
aMinimum follow-up of 6 months from date of first
dose; 1 patient undergoing further evaluation and not
present on plotNR = not reached
Pati
en
ts
0 8 16 24 32 40 48 56 64 72 80 88
Time (Weeks)
On treatment
Off treatment
First response (CR/PR)
Ongoing response
Progression
First tumor assessment was at 6 weeks (+/- 2 weeks)9
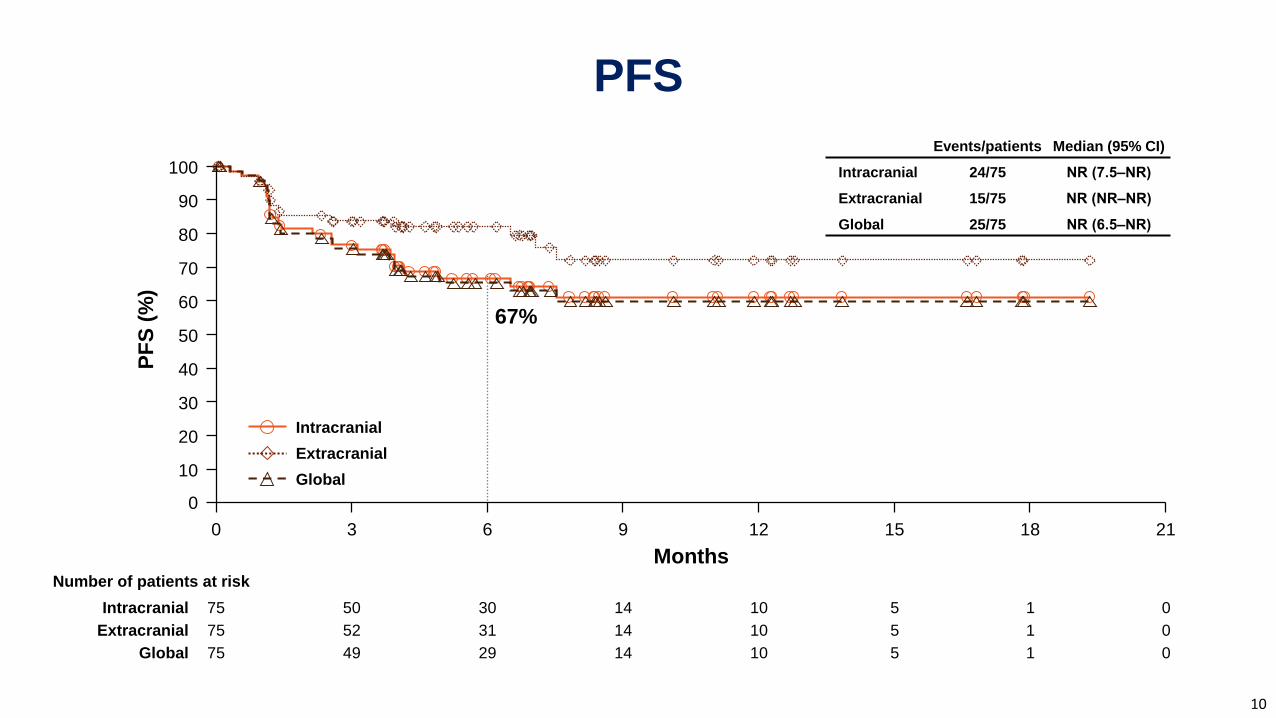
PFS
Events/patients Median (95% CI)
Intracranial 24/75 NR (7.5‒NR)
Extracranial 15/75 NR (NR‒NR)
Global 25/75 NR (6.5‒NR)
Months
PF
S (
%)
100
90
80
70
60
50
40
30
10
0
20
Number of patients at risk
0 181512963 21
67%
Intracranial 151014305075 0
Intracranial
151014315275Extracranial 0
Extracranial
151014294975Global 0
Global
10
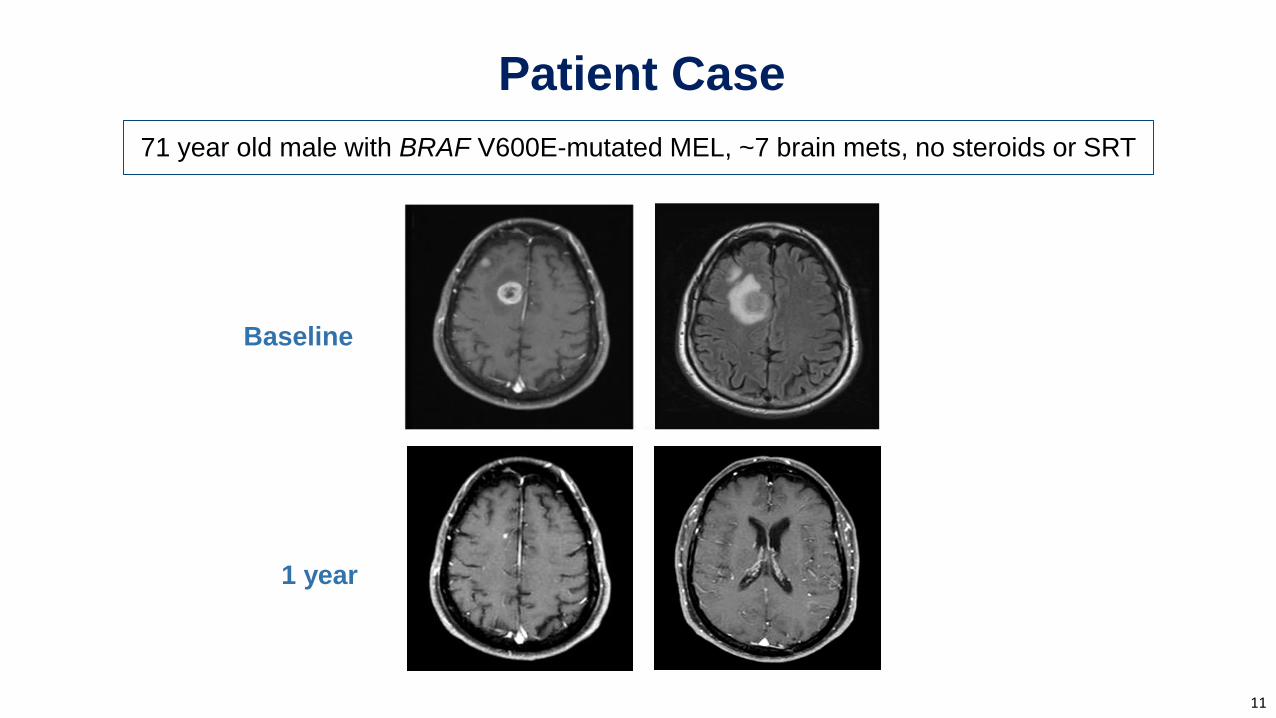
Patient Case
71 year old male with BRAF V600E-mutated MEL, ~7 brain mets, no steroids or SRT
Baseline
11
1 year
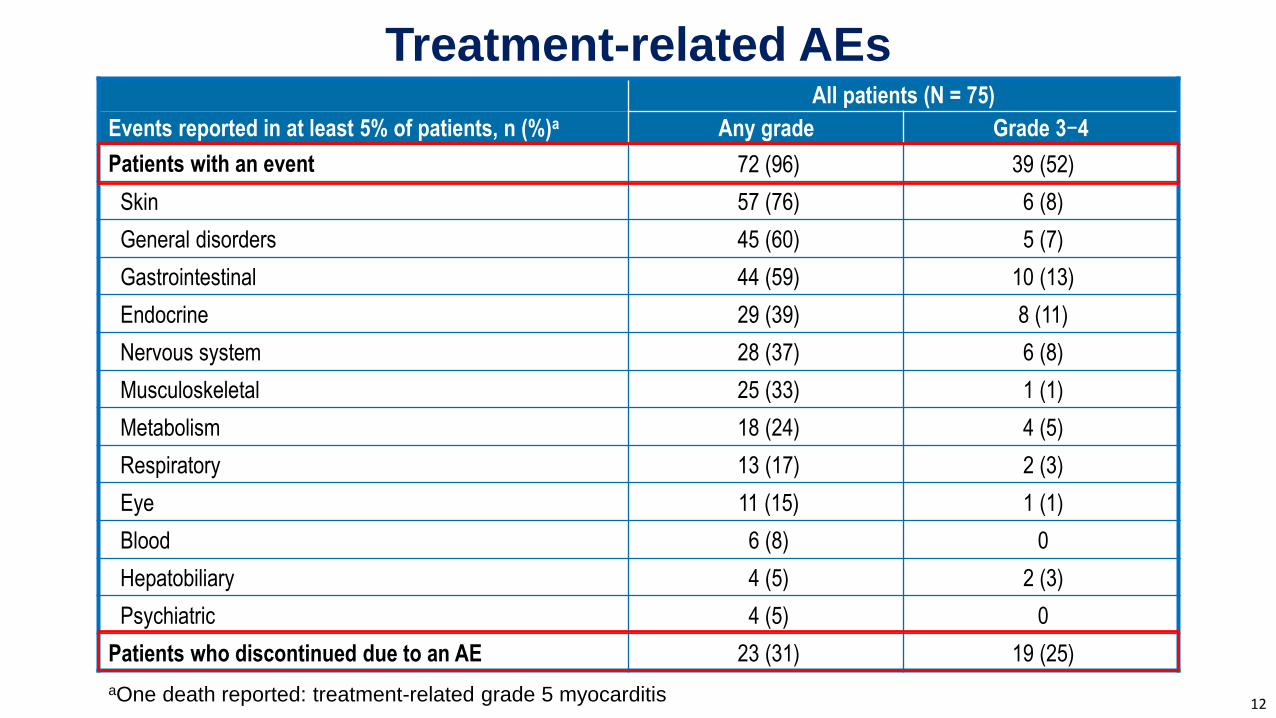
Treatment-related AEs
aOne death reported: treatment-related grade 5 myocarditis 12
All patients (N = 75)
Events reported in at least 5% of patients, n (%)a Any grade Grade 3−4
Patients with an event 72 (96) 39 (52)
Skin 57 (76) 6 (8)
General disorders 45 (60) 5 (7)
Gastrointestinal 44 (59) 10 (13)
Endocrine 29 (39) 8 (11)
Nervous system 28 (37) 6 (8)
Musculoskeletal 25 (33) 1 (1)
Metabolism 18 (24) 4 (5)
Respiratory 13 (17) 2 (3)
Eye 11 (15) 1 (1)
Blood 6 (8) 0
Hepatobiliary 4 (5) 2 (3)
Psychiatric 4 (5) 0
Patients who discontinued due to an AE 23 (31) 19 (25)
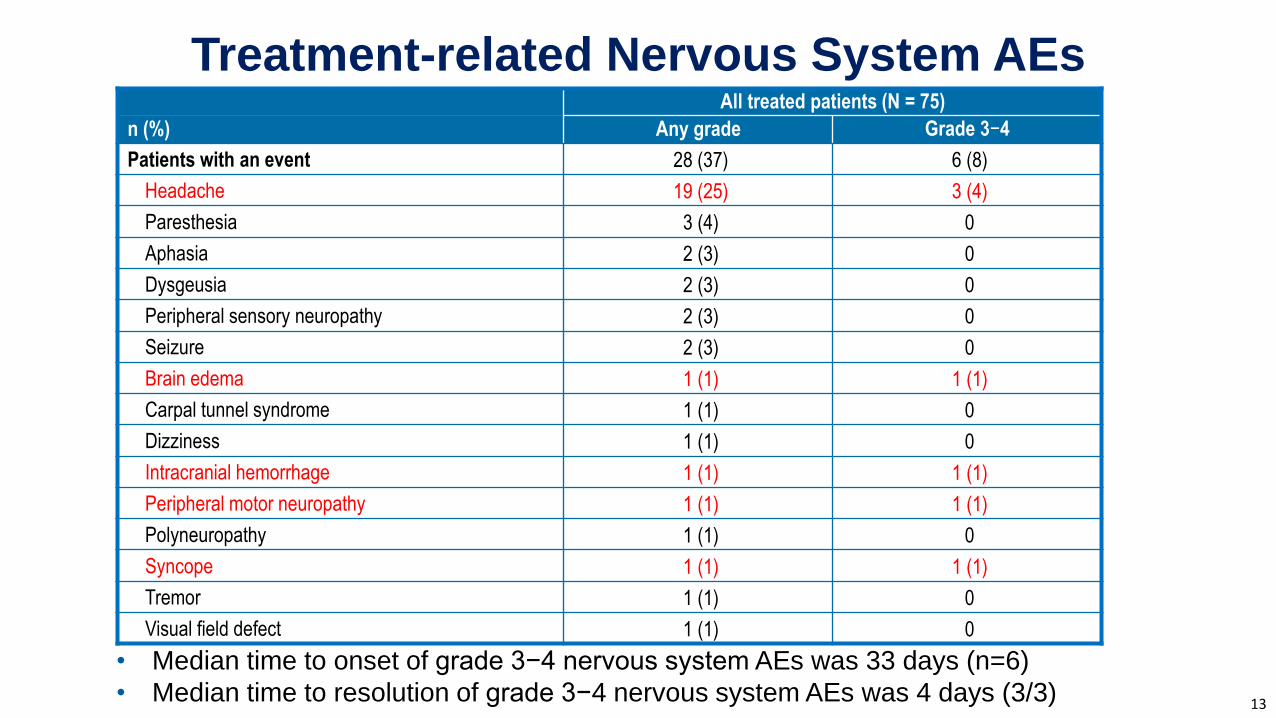
Treatment-related Nervous System AEs
13
All treated patients (N = 75)
n (%) Any grade Grade 3−4
Patients with an event 28 (37) 6 (8)
Headache 19 (25) 3 (4)
Paresthesia 3 (4) 0
Aphasia 2 (3) 0
Dysgeusia 2 (3) 0
Peripheral sensory neuropathy 2 (3) 0
Seizure 2 (3) 0
Brain edema 1 (1) 1 (1)
Carpal tunnel syndrome 1 (1) 0
Dizziness 1 (1) 0
Intracranial hemorrhage 1 (1) 1 (1)
Peripheral motor neuropathy 1 (1) 1 (1)
Polyneuropathy 1 (1) 0
Syncope 1 (1) 1 (1)
Tremor 1 (1) 0
Visual field defect 1 (1) 0
• Median time to onset of grade 3−4 nervous system AEs was 33 days (n=6)
• Median time to resolution of grade 3−4 nervous system AEs was 4 days (3/3)
Summary/Conclusions
• In patients with advanced MEL and untreated brain metastases, NIVO+IPI
demonstrates clinically meaningful efficacy, and can become a new treatment option
• With over 9 months of follow-up, NIVO+IPI resulted in an intracranial ORR of 55%,
with 21% of patients achieving a complete response
–Median PFS is not reached; 6-month PFS rate > 60%
• The safety profile was consistent with earlier experience in patients without MBM1,2
• Further investigations of systemic therapy should consider
– Patients who are symptomatic/requiring steroids: cohort of 20 is actively enrolling
– Approaches to incorporate and sequence radiation therapy
– Earlier inclusion of this MBM population into randomized studies of novel combinations
to accelerate drug development for MBM
141. Larkin J et al. N Engl J Med. 2015;373:23-34. 2. Hodi FS et al. Lancet Oncol. 2016;17:1558-1568.
Acknowledgments
• Patients and their families
• Physicians and research staff from study sites
• Funding from Bristol-Myers Squibb
• All authors contributed to and approved the presentation
Professional medical writing and editorial assistance were provided by Melissa Kirk, PhD and
Cara Hunsberger at StemScientific, an Ashfield Company, funded by Bristol-Myers Squibb
15
Text “204” to +1-609-917-7119
to receive a copy of the CheckMate 204 slidesBy requesting this content, you agree to receive a one-time communication using automated technology.
Msg. & data rates may apply. Links are valid for 30 days after the congress presentation date.


















![Fatal myositis and spontaneous haematoma induced by ......myositis in patients receiving ipilimumab plus nivolumab was 0.24% [5]. ICI-related myositis mimics primary dermatomyositis](https://img.pdfslide.us/doc/110x75/60a56f20301b9a411c564b9f/fatal-myositis-and-spontaneous-haematoma-induced-by-myositis-in-patients.jpg)