-
Efficacy and Safety of Epicutaneous Immunotherapy (EPIT) for
Peanut Allergy in Subjects With and Without Concomitant Food
Allergies
Philippe Bégin, MD, PhD, FRCPC Director, Oral Immunotherapy
ClinicCHU Sainte-Justine, Montreal, QC, Canada
Philippe Bégin, Gordon Sussman, Kirsten Beyer, Roxanne C. Oriel,
Lara Ford, Wayne Shreffler, Dianne E. Campbell, Todd D. Green,
Robin Mukherjee, David M. Fleischer
-
Disclosures
Type Company
Employment full time/part time None
Research grant (PI, collaborator, or consultant; pending and
received grants) DBV Technologies, Sanofi, Regeneron, Novartis
Other research support None
Speakers bureau/honoraria Novartis, ALK, Aralez, DBV
Technologies
Ownership interest (stock, stock-options, patent or intellectual
property) None
Consultant/advisory board Novartis, ALK, Aralez, Pfizer,
Sanofi-Genzyme
In relation to this presentation, I declare the following real
or perceived conflicts of interest:
-
Background1
Study Objective2
Methods3
Results4
Table of Contents
Conclusions5
-
Background – The Burden of Peanut Allergy1
240-550million
individuals worldwide suffer from food allergy1
Among common food allergies, peanut allergy
patients report the highest rate of severe reactions2,3
1. World Allergy Organization. WAO White Book on Allergy: Update
2013.
http://www.worldallergy.org/UserFiles/file/WhiteBook2-2013-v8.pdf.
Accessed May 18, 2020. 2. Gupta RS, et al. Pediatrics.
2018;142:e20181235. 3. Gupta RS, et al. JAMA Netw Open. 2019 Jan
4;2:e185630. 4. Al-Muhsen S, et al. CMAJ. 2003;168:1279-1285. 5.
Deschildre A, et al. Clin Exp Allergy. 2016;46:610-620. 6. Jones
SM, Burks AW. N Engl J Med. 2017;377:1168-1176. 7. Green TD, et al.
Pediatrics. 2007;120:1304-1310. 8. Cherkaoui S, et al. Clin Transl
Allergy. 2015;5:16. 9. Neuman-Sunshine DL, et al. Ann Allergy
Asthma Immunol. 2012;108:326-331.
In some patients, reactions can occur after exposure to low
doses of peanut4,5
Even trace amounts of peanut can trigger a reaction,
including
potentially severe reactions4,5
Standard of care for peanut allergy is strict avoidance plus
personalized medical intervention plans…6
…however, despite practicing strict avoidance, accidental
exposure often occurs and commonly leads to allergic
reactions7-9
-
Avoidance is often characterized by a number of unmet needs, as
patients and caregivers are often left to manage the condition by
themselves
Background – Unmet Need in the Management of Peanut
Allergy11
The goal of food allergy care should be the empowerment of
patients and caregiversFigure from Bégin P, et al. 20201 (CC
license http://creativecommons.org/licenses/by/4.0/).1. Bégin P, et
al. Allergy Asthma Clin Immunol. 2020;16(20).
https://doi.org/10.1186/s13223-020-0413-7.
Considerations for balanced decision-making in medicine
TECHNICAL CONSIDERATIONS
HUMAN CONSIDERATIONS
ETHICAL CONSIDERATIONS
DECISION
-
Background – Epicutaneous Immunotherapyfor the Management of
Peanut Allergy1
Viaskin Peanut 250 µg (VP250)1,2
• Single, daily-dose patch o Applied to the back
• Dose: 250 µg o ~1/1000 of a peanut3
• 2-week at-home treatment initiation leading to 24-hour wear
time
• No restrictions based on illness or daily activities
required
1. Sampson HA, et al. JAMA. 2017;318:1798-1809. 2. Tilles SA, et
al. Ann Allergy Asthma Immunol. 2018;121:145-149. 3. Parrish CP. Am
J Manag Care. 2018;24:S419-S427.
-
Background – VP250 Clinical Trial Program1-71
1. Sampson HA, et al. JAMA. 2017;318:1798-1809. 2. Fleischer DM,
et al. JAMA. 2019;321:946-955. 3. DBV Technologies.
https://www.dbv-technologies.com/wp-content/uploads/2017/09/4221-pr-people-eng-pdf-1.pdf.
Accessed May 18, 2020. 4. ClinicalTrials.Gov. NCT02916446.
https://clinicaltrials.gov/ct2/show/NCT02916446. Accessed May 18,
2020. 5. ClinicalTrials.Gov. NCT03859700.
https://clinicaltrials.gov/ct2/show/NCT03859700. Accessed May 18,
2020. 6. ClinicalTrials.Gov. NCT03211247.
https://clinicaltrials.gov/ct2/show/NCT03211247. Accessed May 18,
2020.7. DBV. Press Release.
https://www.dbv-technologies.com/wp-content/uploads/2018/10/pr-epitope-part-b-fpi-final_102618.pdf.
Accessed May 18, 2020.
Phase 3 N=3934–11 years of age36 months (ongoing)
Phase 3 Part A: N=51; Part B: N=3501–3 years of age12 months
(ongoing)
Phase 3 N=All eligible patients who complete EPITOPE1–3 years of
age36 months (enrolling)
Open-label follow up to EPITOPE
Real Life Useand Safety
Phase 2bVIPES
OLFUS-VIPES
N=171 (OLFUS-VIPES)6–55 years of ageVIPES: 12 monthsOLFUS-VIPES:
24 months
Phase 3 N=3564–11 years of age12 months
Phase 3N=2984–11 years of age60 months (ongoing)Open-label
follow-up
to PEPITES
-
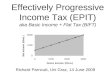
Background – VP250 Clinical Trial Data: Phase 3 PEPITES1
*Participants with missing food challenge values at 12 months
were counted as nonresponders in this analysis.AE=adverse event;
CI=confidence interval; ITT=intent-to-treat; TEAE=treatment
emergent adverse event.1. Fleischer DM, et al. JAMA.
2019;321(10):946-955. 2. Davis CM, et al. Poster presented at:
AAAAI Annual Meeting 2019. February 22-25, 2019; San Francisco, CA.
3. Lange L, et al. Poster presented at: EAACI Congress 2019. June
1-5, 2019; Lisbon, Portugal.
0
5
10
15
20
25
30
35
40 P
-
About a third of patients have more than one food allergy. This
increases to 78% when considering food allergy referral
practices1
Background – Patients With Multiple Food Allergies1
1. Park JH, et al. J Allergy Clin Immunol. 2010;125(2,
Suppl1):AB216. 2. Christie L, et al. J Am Diet Assoc.
2002;102:1648-1651. 3. Sicherer SH, et al. Ann Allergy Asthma
Immunol. 2001;87:461-464. 4. Wang J. Curr Allergy Asthma Rep.
2010;10:271-277. 5. Gupta RS, et al. Pediatrics. 2011;128:e9-17. 6.
Bégin P, et al. Allergy Asthma Clin Immunol. 2020;16(20).
https://doi.org/10.1186/s13223-020-0413-7.
Multi-food allergies are generally more severe, have greater
impact on quality of life, and are less likely to spontaneously
resolve2-5
There is a need for personalized care, considering the
heterogeneity and specificity of the condition and individual
patient contexts6
-
Study Objective2
• To examine efficacy and safety of VP250 in peanut-allergic
children to understand whether concomitant food allergies (CFA)
affect the treatment response or safety outcomes
-
Methods – Study Design3
• Primary outcome: response rate difference between VP250 and
placebo treatment groups after 12 months* • Post-hoc analysis of
the differences in efficacy and safety among peanut-allergic
children with and without CFA at
study entry • Response rate for each group calculated using
Wilson 95% CI and difference between VP250 and placebo response
calculated with Newcombe two-sided 95% CI. Participants with
missing food challenge values at 12 months were counted as
nonresponders in this analysis
*Treatment response was defined as a post-treatment ED of ≥300
mg or ≥1000 mg of peanut protein for subjects with an initial ED of
≤10 mg or >10 mg, respectively.CFA=concomitant food allergies;
CI=confidence interval; DBPCFC=double-blind, placebo-controlled
food challenge; M=month.1. Fleischer DM, et al. JAMA.
2019;321:946-955.
Phase 3, randomized, double-blind, placebo-controlled trial of
VP250 in children 4–11 years of age (N=356)1
Placebo
VP250
n=118
n=238
PEPITES
M0 M12Denotes a DBPCFC.
-
Results – Patient Distribution4
*Twenty-eight of the 150 children had a history of a food
allergy other than peanut which had resolved by baseline, and they
were no longer allergic to foods other than peanut at time of study
entry.
Children aged 4–11 years with peanut allergy
(N=356)
Children with concomitant food allergies (CFA)
(n=206)
Children with peanut allergy only (PAO)
(n=150)*
VP250(n=141)
Placebo(n=65)
VP250(n=97)
Placebo(n=53)
-
Results – Baseline Characteristics4
CFA (n=206) PAO (n=150)
Age (years), mean (SD) 7.4 (2.2) 7.3 (2.2) Sex, n (%)
Male 137 (67) 81 (54)Race, n (%)
CaucasianAsianOther
159 (77)19 (9)
28 (14)
131 (87)8 (5)
11 (7)ED ≤10 mg at baseline, n (%) 39 (19) 22 (15)Median PN-IgE,
kU/L (IQR) 101 (23–249) 68 (22–150)Median PN-IgG4 (IQR) 0.8
(0.39–1.69) 0.5 (0.23–1.13)Median PN-SPT, mm (IQR) 11 (9–14) 11
(9–14)
CFA=concomitant food allergies; ED=eliciting dose;
IQR=interquartile range; PAO=peanut allergy only; PN=peanut;
SD=standard deviation; SPT=skin prick test.
-
Results – Efficacy 4
AD=atopic dermatitis; CFA=concomitant food allergies;
CI=confidence interval; PAO=peanut allergy only.
Improvement in the predefined primary outcome was consistently
in favor of VP250irrespective of whether children had CFA or PAO at
study entry
Subgroup (ongoing history)
VP250 response rate
% (n/N)
Placebo response rate
% (n/N)
Difference (95% CI)
P value for interaction
Asthma (N=159)
No asthma (N=197)
36.9 (41/111)
33.9 (43/127)
12.5 (6/48)
14.3 (10/70)
24.4% (9.6–35.8)
19.6% (6.9–30.3)0.640
Eczema/AD (N=163)
No eczema/AD (N=193)
43.6 (44/101)
29.2 (40/137)
17.7 (11/62)
8.9 (5/56)
25.8% (11.2–38.1)
20.3% (7.8–29.8)0.800
CFA (N=206)
PAO (N=150)
33.3 (47/141)
38.1 (37/97)
16.9 (11/65)
9.4 (5/53)
16.4% (3.3–27.3)
28.7% (14.6–40.0)0.167
-10 0 10 20 30 40 50
Favors Placebo Favors Treatment
Difference (95% CI)
-
Results – Safety 4
AESI=adverse events of special interest; CFA=concomitant food
allergies; PAO=peanut allergy only; TEAE=treatment-emergent adverse
event.
Very similar rates of TEAEs, as well as similar and low rates of
TEAEs leading to permanent discontinuation, were observed between
CFA and PAO groups
CFA PAOVP250 (n=141) Placebo (n=65) VP250 (n=97) Placebo
(n=53)
TEAEs (n, %) 135 (95.7) 60 (92.3) 92 (94.8) 45 (84.9) Mild TEAEs
130 (92.2) 57 (87.7) 90 (92.8) 40 (75.5) Moderate TEAEs 80 (56.7)
27 (41.5) 46 (47.4) 25 (47.2) Severe TEAEs 10 (7.1) 0 4 (4.1) 2
(3.8) Serious TEAEs 3 (2.1) 3 (4.6) 4 (4.1) 2 (3.8)
TEAEs considered related to treatment 85 (60.3) 24 (36.9) 57
(58.8) 17 (32.1) Serious TEAEs considered related to treatment 1
(0.7) 0 2 (2.1) 0
TEAEs leading to permanent treatment discontinuation 2 (1.4) 0 2
(2.1) 0
TEAEs leading to temporary treatment discontinuation 22 (15.6) 6
(9.2) 10 (10.3) 5 (9.4)
Treatment-induced local TEAEs 82 (58.2) 17 (26.2) 55 (56.7) 16
(30.2) Systemic AESI 8 (5.7) 4 (6.2) 5 (5.2) 2 (3.8) Anaphylactic
reaction related to treatment (investigator-assessed) 4 (2.8) 1
(1.5) 4 (4.1) 0
-
Conclusions5
• Over half of participants recruited in the PEPITES trial had
CFA, suggesting that peanut EPIT addresses an unmet need in the
multi-food allergic population
• In peanut-allergic children aged 4–11 years who were treated
with EPIT for peanut allergy, improvement in the predefined primary
outcome measured over the 12-month treatment period was in favor of
VP250 over placebo, irrespective of whether they were allergic only
to peanut or had CFA at study entry
• The safety and tolerability profiles were similar in
peanut-allergic children randomized to VP250 with peanut allergy
alone and peanut allergy with CFA
• These results are in line with those previously reported that
found neither baseline asthma nor AD influenced the efficacy or
safety of VP250
AD=atopic dermatitis; CFA=concomitant food allergies;
EPIT=epicutaneous immunotherapy.
-
Slide Number 1Slide Number 2Slide Number 3Slide Number 4Slide
Number 5Slide Number 6Slide Number 7Slide Number 8Slide Number
9Slide Number 10Slide Number 11Slide Number 12Slide Number 13Slide
Number 14Slide Number 15Slide Number 16Slide Number 17