Embed Size (px)
Citation preview

ARTICLE
Effects of acute NEFA manipulation on incretin-induced insulin secretionin participants with and without type 2 diabetes
Brenno Astiarraga1 & Valéria B. Chueire2& Aglécio L. Souza2 & Ricardo Pereira-Moreira2 & Sarah Monte Alegre2 &
Andrea Natali1 & Andrea Tura3 & Andrea Mari3 & Ele Ferrannini4 & Elza Muscelli2
Received: 26 February 2018 /Accepted: 4 April 2018 /Published online: 7 May 2018# Springer-Verlag GmbH Germany, part of Springer Nature 2018
AbstractAims/hypothesis Incretin effect—the potentiation of glucose-stimulated insulin release induced by the oral vs the i.v. route—isimpaired in dysglycaemic states. Despite evidence from human islet studies that NEFA interfere with incretin function, littleinformation is available about the effect in humans. We tested the impact of acute bidirectional NEFA manipulation on theincretin effect in humans.Methods Thirteen individuals with type 2 diabetes and ten non-diabetic volunteers had a 3 h OGTT, and, a week later, an i.v.isoglycaemic glucose infusion (ISO; OGTT matched). Both pairs of studies were repeated during an exogenous lipid infusion in thenon-diabetic volunteers, and following acipimox administration (to inhibit lipolysis) in people with diabetes. Mathematical modellingof insulin secretion dynamics assessed total insulin secretion (TIS), beta cell glucose sensitivity (β-GS), glucose-induced potentiation(PGLU) and incretin-induced potentiation (PINCR); the oral glucose sensitivity index was used to estimate insulin sensitivity.Results Lipid infusion increased TIS (from 61 [interquartile range 26] to 78 [31] nmol/m2 on OGTTand from 29 nmol/m2 [26] to57 nmol/m2 [30] on ISO) and induced insulin resistance. PINCR decreased from 1.6 [1.1] to 1.3 [0.1] (p < 0.05). β-GS, PGLU andglucagon, glucagon-like peptide 1 (GLP-1) and gastric inhibitory polypeptide (GIP) responses were unaffected. Acipimox(lowering NEFA by ~55%) reduced plasma glucose and TIS and enhanced insulin sensitivity, but did not change β-GS,PINCR, PGLU or glucagon, GLP-1 or GIP responses. As the per cent difference, incretin effect was decreased in non-diabeticparticipants and unchanged in those with diabetes.Conclusions/interpretation Raising NEFA selectively impairs incretin effect and insulin sensitivity in non-diabetic individuals,while acute NEFA reduction lowers plasma glucose and enhances insulin sensitivity in people with diabetes but does not correctthe impaired incretin-induced potentiation.
Keywords Acipimox . Beta cell function . Incretin effect . Incretin hormones . Isoglycaemic protocol . NEFA . Potentiation
AbbreviationsAcp-OGTT OGTT following acipimoxAcp-ISO ISO following acipimoxβ-GS Beta cell glucose sensitivityGIP Gastric inhibitory polypeptideGLP-1 Glucagon-like peptide 1GSIS Glucose-stimulated insulin secretionISO Isoglycaemic glucose infusionISR Insulin secretion rateL-ISO Lipid infusion/ISOL-OGTT Lipid infusion/OGTTOGIS OGTT-derived index of insulin sensitivityPGLU Glucose-induced potentiationPINCR Incretin-induced potentiationTIS Total insulin secretion
Brenno Astiarraga and Valéria B. Chueire contributed equally to thisstudy.
Electronic supplementary material The online version of this article(https://doi.org/10.1007/s00125-018-4633-z) contains peer-reviewed butunedited supplementary material, which is available to authorised users.
* Ele [email protected]
1 Department of Clinical and Experimental Medicine, University ofPisa, Pisa, Italy
2 Department of Internal Medicine, University of Campinas,Campinas, Brazil
3 CNR Institute of Neuroscience, Padua, Italy4 CNR Institute of Clinical Physiology, Via Savi, 10, 56100 Pisa, Italy
Diabetologia (2018) 61:1829–1837https://doi.org/10.1007/s00125-018-4633-z

Introduction
Previous studies in vitro [1, 2] and in intact animals [3]have consistently shown that acute exposure to NEFAresults in a substantial increase in both basal andglucose-stimulated insulin secretion (GSIS). Studies inhumans, however, have yielded contrasting results.Acute (3–12 h) lipid infusions in normal participants havebeen reported to have no effect [4], to increase [5–7] or toinhibit [8] GSIS. In participants with [9] or without [10]family history of type 2 diabetes, a physiological rise inNEFA induced a mild deterioration of beta cell function,which was more evident when insulin secretion was ex-amined in relation to the prevailing insulin resistance. Inthe same individuals, lowering plasma NEFA withacipimox was associated with an improvement in theacute insulin response to i.v. glucose [10, 11]. Differentapproaches to assessing GSIS, different types of test, ad-justment for the insulin sensitivity and genetic predispo-sition might influence the controversial results, asreviewed by Giacca et al [12]. Incretin-mediated insulinsecretion accounts for about 40–80% [13] of total insulinsecretion (TIS) in response to an oral stimulus and isimpaired in type 2 diabetic individuals and in those withsome degree of glucose intolerance [14–17]. However,surprisingly little information is available on the effectof NEFA on incretin-stimulated insulin secretion inhumans, despite recent evidence in human islets thatNEFA might interfere with incretin function [18, 19].
We designed this study to test: (1) whether incretin-inducedpotentiation of insulin secretion is reduced by acute elevationof plasma NEFA levels in healthy volunteers; and (2) whether,
in participants with type 2 diabetes, the impaired incretin ef-fect can be improved by an acute reduction in circulatingNEFA. The incretin effect was measured as the potentiationof glucose-induced insulin release selectively caused by theoral vs i.v. glucose route of entry. Plasma NEFA levels wereacutely raised in non-diabetic volunteers through an i.v. lipidinfusion and lowered in type 2 diabetic participants by theadministration of acipimox.
Methods
The study was carried out at two centres (University of Pisa,Italy, and State University of Campinas, Brazil). Fifteen indi-viduals with type 2 diabetes treated with diet or stable doses ofmetformin were recruited from the outpatient clinic of theCatholic University of Campinas and State University ofCampinas. Inclusion criteria were: age 18–60 years, HbA1c
47.5–85.8 mmol/mol (6.5–10.0%), BMI <40 kg/m2, no otherendocrine disease, no clinical evidence of neoplastic or chron-ic inflammatory disease, or major organ (liver, kidney, heart,pulmonary) failure. Two participants with diabetes were ex-cluded: one dropped out after the first test, the other was ex-cluded at the end of the study when it was realised that theparticipant had an HbA1c of 42.1 mmol/mol [6.0%], lowerthan the lower limit of the protocol; thus, 13 diabetic individ-uals were included in the final analysis. Ten healthy volunteerswere enrolled at the University of Pisa. Participants gave theirinformed consent, and the study was approved by the EthicsCommittees (Protocol number 23474 at the Pisa centre;Certificate of Presentation for Ethical Appreciation, CAAE,48181215.2.0000.5404 at the Campinas centre). The
•
•
•
•
•
•
1830 Diabetologia (2018) 61:1829–1837

anthropometric and metabolic characteristics of the study par-ticipants are summarised in Table 1.
Study protocol All participants had two control tests, a 3 hOGTT (75 g) and, on a separate occasion ~7 days later, a 3 hisoglycaemic glucose infusion (ISO) using an ad hoc
algorithm to exactly reproduce the glycaemic curve observedduring the OGTT (isoglycaemic protocol). In the healthy vol-unteers, both tests were repeated during an i.v. infusion of a20% (vol./vol.) lipid/water emulsion (60 ml/h) together with aprimed (200 U) continuous (0.4 U kg−1 min−1) heparin infu-sion, started 2 h before either test (lipid infusion/OGTT [L-OGTT] and lipid infusion/ISO [L-ISO]). In participants withdiabetes, the two tests were repeated after the ingestion ofacipimox (Olbetam, Pfizer, Rome, Italy) (250 mg) 2 h beforeglucose administration and 1 h into each study (OGTT follow-ing acipimox [Acp-OGTT], ISO following acipimox [Acp-ISO]).
Measurements Fat-free mass was measured by electricalbioimpedance at both sites. Bedside plasma glucose concen-trations were measured at 10 min intervals throughout thestudies using the glucose oxidase technique (YSI 2300 StatPlus Glucose Analyser, Yellow Springs, OH, USA, at theUniversity of Campinas; Beckman Glucose Analysers,Fullerton, CA, USA, at the University of Pisa); plasma insulinand C-peptide concentrations were all measured by chemi-luminescence (on a COBAS e411 instrument, Roche,Indianapolis, IN, USA). In both centres, total plasmaglucagon-like peptide 1 (GLP-1) and gastric inhibitory poly-peptide (GIP) were assayed using the same ELISA kit (Merck
Table 1 Anthropometric and metabolic characteristics of the studyparticipants
Characteristic Healthy Type 2 diabetes
n (women/men) 10 (4/6) 13 (10/3)
Age (years) 34 ± 11 55 ± 8
Duration (<1/<10/≥10 years) - 2/7/4
Body weight (kg) 68 ± 22 88 ± 16
BMI (kg/m2) 23.8 ± 5.9 32.8 ± 5.6
Fat-free mass (kg) 52 ± 15 51 ± 10
Fat mass (%) 23 ± 3 39 ± 6
Energy expenditure (kJ/24 h) 6592 ± 548 6772 ± 302
HbA1c (mmol/mol) – 55.2 ± 4.3
HbA1c (%) – 7.2 ± 0.5
Triacylglycerols (mmol/l) 1.05 ± 0.27 1.77 ± 0.74
Insulin sensitivity (ml min−1 m−2) 402 ± 22 291 ± 60
Data are mean ± SD
4
6
8
10
12
14
-120 -90 -60 -30 0 30 60 90 120 150 1804
5
6
7
8
9
10
-120 -90 -60 -30 0 30 60 90 120 150 180
0
1000
2000
3000
4000
5000
-120 -90 -60 -30 0 30 60 90 120 150 180
Pla
sma
NE
FA
(µm
ol/l)
0
200
400
600
800
1000
-120 -90 -60 -30 0 30 60 90 120 150 180
c
Pla
sma
gluc
ose
(m
mol
/l)
Time (min)
b
Time (min)
d
a
Pla
sma
gluc
ose
(m
mol
/l)P
lasm
a N
EF
A (
µmol
/l)
Time (min) Time (min)
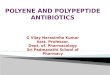
Fig. 1 Plasma NEFA (a) and glucose concentrations (b) in non-diabeticvolunteers in OGTT and ISO control studies and with lipid infusion.Black squares, OGTT; white squares, ISO; black triangles, L-OGTT;white triangles, L-ISO. Plasma NEFA (c) and glucose concentrations(d) in participants with type 2 diabetes in OGTT and ISO control studies
and after acipimox ingestion. Black circles, OGTT; white circles, ISO;black diamonds, Acp-OGTT; white diamonds, Acp-ISO. Data are pre-sented as mean ± SEM for n = 10 non-diabetic participants and n = 13type 2 diabetic participants
Diabetologia (2018) 61:1829–1837 1831

Millipore, Billerica, MA, USA), plasma NEFA by a standardcolorimetric method (WAKO Chemicals, Neuss, Germany),and plasma glucagon by ELISA (RD System, Minneapolis,MN, USA; Campinas) and by Mercodia Glucagon ELISA(Mercodia, Uppsala, Sweden; Pisa).
Data analysis Insulin sensitivity was estimated from the plas-ma glucose and insulin responses to oral glucose using theOGTT-derived index of insulin sensitivity (OGIS) [20].AUCs were calculated using the trapezoid rule. Plasma C-peptide deconvolution was used to calculate insulin secretionrate (ISR) and TIS, and mathematical modelling to quantify
beta cell function and the incretin effect [21]. The main vari-ables in the beta cell model are glucose sensitivity (β-GS), i.e.the slope of the ISR/glucose dose–response curve obtainedduring the ISO test. Glucose-induced potentiation (PGLU), atime-dependent modulation of the dose–response calculatedduring the ISO test, was parameterised as the ratio of the valueat 3 h to the fasting value; incretin-induced potentiation(PINCR) was calculated as the time-dependent fold ISR incre-ment during OGTT compared with ISO glucose, and wasparameterised as its integral over the 3 h of the tests. Theincretin effect was also calculated using conventional model-independent indices (per cent difference ([(OGTT TIS − ISO
0
0.5
1.0
1.5
2.0
2.5
OGTT L-OGTT
0
30
60
90
120
150
180
OGTT ISO L-OGTT L-ISO
0
1000
2000
3000
4000
5000
OGTT ISO L-OGTT L-ISO
0
30
60
90
120
150
ISO L-ISOβ-G
S (
pmol
min
-1 m
-2 [m
mol
/l]-1
)R
ate
sens
itivi
ty (
pmol
m-2
mm
ol-1
) P
INC
R (f
old)
PIN
CR
(fol
d)
TIS
(nm
ol/m
2 )
β-G
S (
pmol
min
-1 m
-2 [m
mol
/l]-1
)R
ate
sens
itivi
ty (
pmol
m-2
mm
ol-1
) T
IS (
nmol
/m2 )
a
b
c
d
e
f
g
h
†
† *
*
0
30
60
90
120
150
180
OGTT ISO Acp-OGTT Acp-ISO
0
1000
2000
3000
4000
5000
OGTT ISO Acp-OGTT Acp-ISO
0
30
60
90
120
150
ISO Acp-ISO
0
0.5
1.0
1.5
2.0
2.5
OGTT Acp-OGTT
**†
**
†
†
*
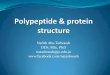
Fig. 2 TIS (a,e), β-GS (b,f),PINCR (c,g) and rate sensitivity(d,h) in non-diabetic volunteers(a–d) and participants with type 2diabetes (e–h). *p < 0.05 for ISOvs OGTT, L-ISO vs L-OGTT orAcp-ISO vs Acp-OGTT.†p < 0.05 for treatment (lipid oracipimox) vs corresponding(OGTT or ISO) control study.Data are presented as mean ±SEM for n = 10 non-diabeticparticipants and n = 13 type 2diabetic participants
1832 Diabetologia (2018) 61:1829–1837

TIS)/OGTT TIS] × 100) and the ratio (OGTT TIS/ISO TIS)between oral and i.v. glucose insulin secretory response), asdescribed by Nauck et al [13, 14].
Statistical analysis Data from healthy participants and thosewith diabetes were analysed separately. Within-group treat-ment responses were analysed by paired t test or Wilcoxonsigned rank test for normally or non-normally distributed var-iables, respectively. A p value ≤0.05 was considered statisti-cally significant.
Results
Lipid infusion in non-diabetic volunteersWhile plasmaNEFAlevels were markedly suppressed during saline (154 mmol/lNaCl) infusion, exogenous lipid infusion increasedmean plas-ma NEFA from 0.20 ± 0.08 to 3.55 ± 1.29 mmol/l during theL-OGTT, and from 0.23 ± 0.08 to 3.77 ± 1.10 mmol/l duringthe L-ISO study (p < 0.001 for both) (Fig . 1a) .Correspondingly, mean triacylglycerol rose from 0.7 ± 0.3 to3.1 ± 1.3 mmol/l and from 0.6 ± 0.2 to 3.2 ± 1.3 mmol/l duringthe L-OGTT and L-ISO, respectively (p < 0.005 for both).Plasma glucose profiles were matched between the oral andi.v. studies. Lipid infusion caused a marked deterioration ofglucose tolerance (glucose incremental AUC 0.44 ± 0.04 vs0.30 ± 0.03 mol/l × h, p < 0.05) that was particularly evident
during the second half of the test (Fig. 1b). As expected, totalinsulin release was greater with oral than i.v. glucose with bothsaline (Figs 2a, 3a) and lipid (Figs 2a, 3b); in addition, therelative hyperglycaemia induced by lipid infusion producedan increase in ISR and TIS, which was particularly pro-nounced (and statistically significant) during i.v. glucose ad-ministration (Table 2 and Fig. 2a). Neither β-GS (Fig. 2b) norglucose potentiation (PGLU) (Fig. 4) were significantly affect-ed by the rise in NEFA, while rate sensitivity was approxi-mately doubled (Table 2 and Fig. 2d) in both the oral and i.v.tests. In contrast, lipid infusion induced a marked decrease inincretin potentiation (PINCR) (Table 2; Figs 2c, 4b), as well asin incretin effect calculated by conventional formulae(Table 2).
Response to oral glucose of plasma glucagon (0.76 ± 0.34vs 0.68 ± 0.25 mol/l × h, OGTTAUC vs L-OGTTAUC, respec-tively) (data not shown), GLP-1 (7.8 ± 2.2 vs 7.6 ± 2.1 nmol/l × h, respectively) and GIP (9.4 ± 1.1 vs 9.4 ± 1.4 nmol/l × h,respectively) were not different (electronic supplementary ma-terial [ESM] Fig. 1). Lipid infusion induced mild insulin re-sistance (OGIS = 355 ± 28 vs 402 ± 22 ml min−1 m−2, L-OGTT vs OGTT, respectively, p < 0.01).
Type 2 diabetic participants Plasma glucose profiles weresuperimposable on the paired oral and the i.v. tests.Acipimox administration was associated with a marked de-crease in NEFAAUC (55 ± 14%, p < 0.01), which was similar
0
100
200
300
400
500
600
700
Time (min) Time (min)
ISR
(pm
ol m
in-1
m-2
)
0
100
200
300
400
500
600
700
0
100
200
300
400
500
600
700
0
100
200
300
400
500
600
700
0 30 60 90 120 150 180
00 30 60 90 120 150 180
0 30 60 90 120 150 180
0 30 60 90 120 150 180
a
b
c
dTime (min) Time (min)
ISR
(pm
ol m
in-1
m-2
)
ISR
(pm
ol m
in-1
m-2
)IS
R (
pmol
min
-1 m
-2)
Fig. 3 ISR in non-diabetic volunteers during control studies, OGTT andcorresponding ISO test (a), and during the lipid infusion studies, L-OGTTand L-ISO (b). Black squares, OGTT; white squares, ISO; black triangles,L-OGTT; white triangles, L-ISO. ISR in people with type 2 diabetes
during (c) control studies and after acipimox ingestion (d). Black circles,OGTT; white circles, ISO; black diamonds, Acp-OGTT; white diamonds,Acp-ISO. Data are presented as mean ± SEM for n = 10 non-diabeticparticipants and n = 13 type 2 diabetic participants
Diabetologia (2018) 61:1829–1837 1833

in the oral and i.v. tests (Fig. 1c), and an improved glucosetolerance (glucose AUC = 0.74 ± 0.16 vs 0.90 ± 0.26 mol/l ×h, p = 0.04) (Fig. 1d). Lowering plasma NEFAwith acipimoxreduced TIS during the OGTT, without significant changes inβ-GS or rate sensitivity (Table 2 and Fig. 2e,h). Similarly, inthe control (Fig. 3c) and the acipimox study (Fig. 3d), insulinsecretion was lower in response to i.v. than oral glucose, par-ticularly during the first 2 h of the tests. Neither PGLU (Fig. 4c)nor PINCR (Figs 2g,4d) (or the incretin effect indices [Table 2])were changed by acipimox. PINCR was ~30% lower in theseparticipants with diabetes than in the control group (p < 0.05).
Acipimox administration did not change theAUCs of plasmaglucagon (4.58 ± 0.92 vs 4.47 ± 0.63 nmol/l × h) (data notshown), GLP-1 (9.0 ± 3.2 vs 9.2 ± 4.3 nmol/l × h) or GIP(16.9 ± 7.4 vs 16.3 ± 5.5 nmol/l × h) (all p =NS) (ESM Fig. 1).Insulin sensitivity was slightly, but significantly, improved byacipimox (OGIS: 326 ± 44 vs 291 ± 60ml min−1 m−2, p = 0.01).
In the data from the diabetes group, changes in ISR weredirectly related to changes in NEFA (ρ = 0.62, p = 0.03).
Discussion
In this study, we show that the acute effects of NEFA oninsulin secretion are asymmetric. While in non-diabetic vol-unteers NEFA elevation caused a marked impairment ofincretin-induced potentiation, in individuals with type 2 dia-betes the impaired incretin effect was not improved by acutelylowering plasma NEFA. Of note, in the non-diabetic partici-pants raising NEFA induced all the expected metabolic chang-es [9, 22]: mild deterioration of glucose tolerance and insulinsensitivity, increased insulin secretion and enhanced early in-sulin response (i.e. rate sensitivity) without any changes in β-GS. Conversely, acipimox administration in diabetic partici-pants was associated with reduced insulin secretion and plas-ma glucose excursions and improved insulin sensitivity, butneither beta cell glucose sensitivity nor incretin-induced po-tentiation was changed. Of interest is that the effects of plasmaNEFA modulation were observed in both the oral and i.v.tests; this rules out a role for the entero–insular axis or the
Table 2 Beta cell function innon-diabetic volunteers and indi-viduals with type 2 diabetes
Variable OGTT ISO L-OGTT L-ISO
No diabetes
Fasting plasma glucose (mmol/l) 5.11 ± 0.28 5.33 ± 0.42* 5.19 ± 0.50 5.08 ± 0.41†
Fasting NEFA (μmol/l) 630 ± 121 595 ± 152* 554 ± 109† 607 ± 310
Fasting ISR (pmol min−1 m−2) 81 [19] 73 [43] 103 [25] 105 [24]††
TIS (nmol/m2) 61 [26] 29 [26]** 78 [31]† 57 [30]**, †
β-GS (pmol min−1 m−2 [mmol/l]−1) – 62 [34] – 61 [50]
Rate sensitivity (nmol m−2 mM−1) 0.85 [0.94] 0.28 [0.59] 2.02 [2.05]† 0.70 [0.92]*
PGLU (fold) – 1.04 [0.38] – 1.19 [0.73]
PINCR (fold)a 1.61 [1.10] 1.30 [0.10]†
Incretin effect (ratio)a 1.79 [0.69] 1.41 [0.21]†
Incretin effect (%)a 44 [19] 29 [12]†
Type 2 diabetes OGTT ISO Acp-OGTT Acp-ISO
Fasting plasma glucose (mmol/l) 6.91 ± 0.97 6.97 ± 0.91 6.78 ± 0.74 6.91 ± 0.86
Fasting NEFA (μmol/l) 716 ± 262 749 ± 231 748 ± 348 763 ± 349
Fasting ISR (pmol min−1 m−2) 129 [40] 134 [39] 130 [43] 113 [53]
TIS (nmol/m2) 64 [24] 58 [17]** 60 [26]† 49 [10]**
β-GS (pmol min−1 m−2 [mmol/l]−1) – 26 [14] – 29 [15]
Rate sensitivity (nmol m−2 mmol−1) 0.65 [0.58] 0.23 [0.04]** 0.85 [1.39] 0.00 [0.00]**
PGLU (fold) – 1.61 [0.82] – 1.38 [0.50]
PINCR (fold)a 1.15 [0.21] 1.10 [0.24]
Incretin effect (ratio)a 1.22 [0.26] 1.22 [0.35]
Incretin effect (%)a 18 [18] 18 [24]
Data are mean ± SD or median [interquartile range]a These values were determined using oral and i.v. glucose results. For a further explanation of these variables,please refer to the ‘Data analysis’ section of the Methods* p < 0.05 and ** p < 0.01 by Wilcoxon test for oral vs i.v. glucose: ISO vs OGTT in non-diabetic and in type 2diabetic participants; L-ISO vs L-OGTT in non-diabetic and Acp-ISO vs Acp-OGTT in type 2 diabeticparticipants† p < 0.05 and †† p < 0.01 by Wilcoxon test for the comparison of lipid infusion or acipimox vs respective controlstudy
1834 Diabetologia (2018) 61:1829–1837

taste receptors/cerebral–insular axis. In support of this, neitherlipid infusion nor acipimox was associated with any changesin plasma glucagon, GLP-1 or GIP responses in the partici-pants with or without diabetes. The absence of short-termchanges in gut hormones agrees with studies in normal volun-teers subjected to 1 week of high-fat overeating, in whomglucose tolerance deteriorated, plasma insulin increased butGLP-1 and GIP responses were not modified [23].
Taken together, these findings make it possible to concludethat the direction of the impact of NEFA on incretin effectdepends, essentially, on beta cell function: raising NEFA canimpair the incretin effect on a normal beta cell but loweringNEFA cannot rescue the incretin effect on a dysfunctional betacell. In line with the latter result, lipid-induced impairment ofbeta cell function is not observed in frankly diabetic animalsor humans [12]. Obviously, our conclusions apply only toacute changes in NEFA concentration and to the experimentalconditions created by these protocols, i.e. they provide proofof concept. In the longer term, the impact of NEFA on beta cellfunction may be more heterogeneous. For example, Kashyapet al [9] reported that in normal participants a prolonged(4 day) l ipid infusion led to mild meal- inducedhyperglycaemia and insulin hypersecretion, which was asso-ciated with a marked improvement in first-phase insulin se-cretion. In contrast, opposite responses were observed in
individuals with a family history of diabetes [9]. However,in a similar study, 48 h acipimox treatment improved the acuteinsulin response to i.v. glucose in individuals with a familyhistory of type 2 diabetes [24]. It must be observed, however,that these studies did not directly assess the incretin effect,which, by definition, requires performing an isoglycaemicprotocol. On the other hand, it is pertinent to recall that chronictreatment with a dipeptidyl peptidase IV (DPP-IV) inhibitor,sitagliptin [25] or metformin [26], in diabetic individuals didnot improve the incretin effect.
The current results align with those of a previous studycarried out in a large cohort of non-diabetic individuals [27],which indicated that relatively higher NEFA levels, such asare typically found in type 2 diabetic individuals, are associ-ated with enhanced absolute ISRs and reduced insulin action,but they do not interfere with β-GS, which is the strongestdeterminant of glucose tolerance.
Several cellular mechanisms may be involved in the im-pairment of incretin function caused by NEFA exposure.Kang et al reported that, in rat insulinoma INS-1E cells andin isolated islets of db/dbmice, palmitate decreases the expres-sion and levels of the GLP-1 receptor; this was associated toimpairment of: cAMP production, protein phosphorylation ofcAMP-responsive elements binding protein (p-CREB) andinsulin secretion [18]. A recent very elegant study investigated
PIN
CR (
fold
)
PIN
CR (
fold
)
PG
LU (
fold
)
PG
LU (
fold
)
Time (min)Time (min)
0.8
1.2
1.6
2.0
2.4
0.6
0.8
1.0
1.2
1.4
0 30 60 90 120 150 180
0 30 60 90 120 150 180 0 30 60 90 120 150 180
0 30 60 90 120 150 180
0.8
1.2
1.6
2.0
2.4
0.6
0.8
1.0
1.2
1.4a
b
c
d
Time (min)Time (min)
Fig. 4 PGLU during ISO test and L-ISO in non-diabetic volunteers (a),and during ISO test and Acp-ISO study in participants with type 2 dia-betes (c). PINCR during the control studies and during the lipid infusionstudies in non-diabetic volunteers (b) and during control studies andacipimox studies in participants with type 2 diabetes (d). Non-diabetic
participants: white squares, ISO; white triangles, L-ISO; black squares,OGTT; black triangles, L-OGTT. Diabetic participants: white circles,ISO; white diamonds, Acp-ISO; black circles, OGTT; black diamonds,Acp-OGTT. Data are presented as mean ± SEM for n = 10 non-diabeticparticipants and n = 13 type 2 diabetic participants
Diabetologia (2018) 61:1829–1837 1835

the effect of palmitate on the recruitment, by GLP-1, of thebeta cell network, which is essential to synchronise rapid in-creases in glucose-induced insulin secretion. Gap junctions inhuman beta cells, through connexin 36 (Cx36), are importantfor incretin-stimulated but not for GSIS [19]. In these humanislet preparations, palmitate reduced Cx36 expression and thecoordinated secretory activity in response to GLP-1 and GIP,thereby reducing insulin release. Thus, elevated NEFA mightdisrupt the GLP-1-sensitive syncytium. Chronic mechanismsmay involve accumulation of malonyl-coenzyme A (CoA)and long-chain fatty acyl-CoAs, increased fatty acid esterifi-cation and activation of endoplasmic reticulum stress in betacells (reviewed in Giacca et al [12] and Poitout and Robertson[28]). Decreased free fatty acid receptor 1 (GPR40) expressionin the beta cell, or its downregulation by NEFA, may contrib-ute to the impaired incretin action observed in diabetes. It isnoteworthy that our diabetic participants had higher fastingglucose and marginally higher fasting NEFA concentrations(700 [352] vs 588 [220], p = 0.12), a combination that seemsto be synergistically toxic to islets [12], where itdownregulates GPR40 expression in all cell types [29].Similar insulin secretion impairment was observed in humanislets exposed to palmitate or oleate for 48 h [30]. GPR40 ishighly expressed in islets from young normoglycaemic, hy-perlipidaemic and prediabetic Zucker diabetic fatty (ZDF) rats(fa/fa) even before diabetes development [29]. Furthermore,in rats maintained under hyperglycaemic conditions for 96 h,GLP-1 receptor expression is reduced, and GIP receptor ex-pression is increased [31]. While these mechanisms, alone orin combination, may underlie the effect of raising NEFA intothe millimolar range we observed in our non-diabetic partici-pants, a role for the mild but chronic NEFA elevations, com-monly found in individuals with type 2 diabetes, to the loss ofincretin effect remains to be conclusively demonstrated. Theabsence of changes in gut hormones across our NEFA manip-ulations implies that an impaired incretin effect—whether in-duced in non-diabetic participants or spontaneous in diabe-tes—is coupled with a degree of cellular resistance to incretins[32]. Interestingly, in a recent study in type 2 diabetic individ-uals, the clinical efficacy of liraglutide, a GLP-1 receptor ag-onist, was related to the baseline plasma triacylglycerols andC-peptide levels [33].
Limitations and strengths These studies were carried out intwo centres and the general phenotypes of the two participantgroups were different. We chose a very healthy group to testthe effects of NEFA, and typical individuals with type 2 dia-betes to evaluate a possible improvement in incretin effectafter NEFA reduction. The results were not meant to be com-pared across groups but within groups. Another limitation isthe sample size, but the incretin effect, i.e. the main outcomevariable of the protocol, was very different after lipid infusionin the non-diabetic participants, and very similar after
acipimox ingestion in the diabetic participants. On the otherhand, this is the first study to evaluate the effect of NEFA onthe incretin effect in humans with an appropriate protocol. Themathematical model yielded the dynamic characteristics ofbeta cell function, including the time course of glucose poten-tiation and the incretin potentiation of insulin secretion.
Acknowledgements We warmly thank F. K. Saraiva and S. Rodovalho,Faculdade de Medicina, Pontificia Universidade Catolica de Campinas,for their valuable collaboration. We also thank LC Oliveira and RFCastilho from the Department of Patologia Clinica at the University ofCampinas for the laboratory assays.
The results were presented at the EASD 2017 Annual Meeting as oralpresentation 197 and poster 512.
Data availability The datasets generated and analysed during the currentstudy are available from the corresponding author on reasonable request.
Funding European Foundation for the Study of Diabetes (EFSD)/SanofiCollaborative Program 2015 award to EM; partial support was also pro-vided by a EuropeanMedical Information Framework (EMIF) grant (IMIJU GA 115372-2) for Pisa participation. The study sponsors were notinvolved in: the design of the study; the collection, analysis nor the inter-pretation of data; writing the report; nor the decision to submit the reportfor publication.
Duality of interest The authors declare that there is no duality of interestassociated with this manuscript.
Contribution statement EF, EM, AN and BA designed the protocol.VBC, EM, ALS, BA, RP-M and SMA performed the experimental stud-ies, and acquired the data and participated in its interpretation. VBC, BAand EM wrote the manuscript. AM and AT performed the mathematicalmodelling. EF and AN discussed and revised the manuscript. All authorsreviewed the manuscript critically and approved the final manuscriptversion. EF and EM are the guarantors of this work.
References
1. Randle PJ, Garland PB, Hales CN, Newsholme EA (1963) Theglucose fatty-acid cycle. Its role in insulin sensitivity and the met-abolic disturbances of diabetes mellitus. Lancet 1:785–789
2. Boden G, Chen X, Iqbal N (1998) Acute lowering of plasma NEFAlowers basal insulin secretion in diabetic and non diabetic subjects.Diabetes 47:1609–1612
3. Sako Y, Grill VE (1990) A 48-hour lipid infusion in the rat time-dependently inhibits glucose-induced insulin secretion and β-celloxidation through a process likely coupled to fatty acid oxidation.Endocrinology 127:1580–1589
4. Amery CM, Round RA, Smith JM, Nattrass M (2000) Elevation ofplasma fatty acids by ten-hour intralipid infusion has no effect onbasal or glucose-stimulated insulin secretion in normal man.Metabolism 49:450–454
5. Felber JP, Vannotti A (1964) Effects of fat infusion on glucosetolerance and insulin plasma levels. Med Exp Int J Exp Med 10:153–156
6. Pelkonen R,Miettinen TA, TaskinenMR, Nikkila EA (1968) Effectof acute elevation of plasma glycerol, trygliceride and NEFA levelson glucose utilization and plasma insulin. Diabetes 17:76–82
7. Paolisso G, Gambardella A, Amato L et al (1995) Opposite effectsof short- and long-term fatty acid infusion on insulin secretion inhealthy subjects. Diabetologia 38:1295–1299
1836 Diabetologia (2018) 61:1829–1837

8. Boden G, Chen X, Rosner J, Baron M (1995) Effects of a 48-hourfat infusion on insulin secretion and glucose utilization. Diabetes44:1239–1242
9. Kashyap S, Belfort R, Gastaldelli A et al (2003) A sustained in-crease in plasma free fatty acids impairs insulin secretion in nondi-abetic subjects genetically predisposed to develop Type 2 diabetes.Diabetes 52:2461–2474
10. Salgin B, Marcovecchio ML, Humphreys SM et al (2009) Effectsof prolonged fasting and sustained lipolysis on insulin secretion andinsulin sensitivity in normal subjects. Am J Physiol EndocrinolMetab 296:E454–E461
11. PaolissoG, TagliamonteMR, RizzoMR et al (1998) Lowering fattyacids potentiates acute insulin response in first degree relatives ofpeople with type II diabetes. Diabetologia 41:1127–1132
12. Giacca A, Xiao C, Oprescu AI, Carpentier AC, Lewis GF (2011)Lipid-induced pancreatic β-cell dysfunction: focus on in vivo stud-ies. Am J Physiol Endocrinol Metab 300:E255–E262
13. Nauck MA, Homberger E, Siegel E et al (1986) Incretin effects ofincreasing glucose loads in man calculated from venous insulin andC-peptide responses. J Clin Endocrinol Metab 63:492–498
14. Nauck M, Stöckmann F, Ebert R, Creutzfeldt W (1986) Reducedincretin effect in type 2 (non-insulin-dependent) diabetes.Diabetologia 29:46–52
15. Muscelli E, Mari A, Natali A et al (2006) Impact of incretin hor-mones on β-cell function in subjects with normal or impaired glu-cose tolerance. Am J Physiol Endocrinol Metab 291:E1144–E1150
16. Muscelli E, Mari A, Casolaro A et al (2008) Separate impact ofobesity and glucose tolerance on the incretin effect in normal sub-jects and type 2 diabetic patients. Diabetes 57:1340–1348
17. Nauck MA, Vardarli I, Deacon CF, Holst JJ, Meier JJ (2011)Secretion of glucagon-like peptide-1 (GLP-1) in T2D: what is up,what is down? Diabetologia 54:10–18
18. Kang ZF, Deng Y, Zhou Y et al (2013) Pharmacological reductionof NEFA restores the efficacy of incretin-based therapies throughGLP-1 receptor signalling in the β-cell in mouse models of diabe-tes. Diabetologia 56:423–433
19. Hodson DJ, Mitchell RK, Bellomo LA et al (2013) Lipotoxicitydisrupts incretin-regulated human β-cell connectivity. J Clin Invest123:4182–4194
20. Mari A, Pacini G, Murphy E, Ludvik B, Nolan JJ (2001) A model-based method for assessing insulin sensitivity from the oral glucosetolerance test. Diabetes Care 24:539–548
21. Tura A, Muscelli E, Gastaldelli A, Ferrannini E, Mari A (2014)Altered pattern of the incretin effect as assessed by modelling inindividuals with glucose tolerance ranging from normal to diabetic.Diabetologia 57:1199–1203
22. Ferrannini E, Barrett EJ, Bevilacqua S, DeFronzo RA (1983) Effectof fatty acids on glucose production and utilization in man. J ClinInvest 72:1737–1747
23. Parry SA, Smith JR, Corbett TR, Woods RM, Hulston CJ (2017)Short-term, high-fat overfeeding impairs glycaemic control butdoes not alter gut hormone responses to a mixed meal tolerance testin healthy, normal-weight individuals. Br J Nutr 117:48–55
24. Cusi K, Kashyap S, Gastaldelli A, Bajaj M, Cersosimo E (2007)Effects on insulin secretion and insulin action of a 48-h reduction ofplasma free fatty acids with acipimox in nondiabetic subjects ge-netically predisposed to T2D. Am J Physiol Endocrinol Metab 292:E1775–E1781
25. Muscelli E, Casolaro A, Gastaldelli A et al (2012) Mechanisms forthe antihyperglycemic effect of sitagliptin in patients with type 2diabetes. J Clin Endocrinol Metab 97:2818–2826
26. Vardarli I, Arndt E, Deacon CF, Holst JJ, NauckMA (2014) Effectsof sitagliptin and metformin treatment on incretin hormone andinsulin secretory responses to oral and “isoglycemic” intravenousglucose. Diabetes 63:663–674
27. Rebelos E, Seghieri M, Natali A et al (2015) Influence of endoge-nousNEFA on beta cell function in humans. Diabetologia 58:2344–2351
28. Poitout V, Robertson RP (2008) Glucolipotoxicity: Fuel excess andβ-cell dysfunction. Endocr Rev 29:351–366
29. Meidute Abaraviciene S, Muhammed SJ, Amisten S, Lundquist I,Salehi A (2013) GPR40 protein levels are crucial to the regulationof stimulated hormone secretion in pancreatic islets. Lessons fromspontaneous obesity-prone and non-obese type 2 diabetes in rats.Mol Cell Endocrinol 381:150–159
30. Zhou YP, Grill V (1995) Long term exposure to fatty acids andketones inhibits B cell functions in human pancreatic islets ofLangerhans. J Clin Endocrinol Metab 80:1584–1590
31. Xu G, Kaneto H, Laybutt DR et al (2007) Downregulation of GLP-1 and GIP receptor expression by hyperglycemia: possible contri-bution to impaired incretin effects in diabetes. Diabetes 56:1551–1558
32. Tura A, Bagger JI, Ferrannini E et al (2017) Impaired beta cellsensitivity to incretins in type 2 diabetes is insufficiently compen-sated by higher incretin response. Nutr Metab Cardiovasc Dis 27:1123–1129
33. Tanabe A, Kaneto H, Kamei S et al (2016) Clinical effects ofliraglutide are possibly influenced by hypertriglyceridemia and re-maining pancreatic β-cell function in subjects with type 2 diabetesmellitus. J Diabetes Complicat 30:1201–1203
Diabetologia (2018) 61:1829–1837 1837