Embed Size (px)
Citation preview

Effects of Vasoactive Agents on
Intestinal Oxygen Consumption and Blood Flow in Dogs
WIEsLAw PAwUK, A. P. SmUpHmD,and EUGENED. JACOBSON
From the Department of Physiology, The University of Texas Medical School
at Houston, Houston, Texas 77025
A B S T R A C T A comparison study of several vaso-constrictor and vasodilator agents was conducted mea-suring changes in intestinal blood flow and oxygenconsumption during 10-min periods of intra-arterialinfusion. Blood flow was measured in a branch of thesuperior mesenteric artery of anesthetized dogs withan electromagnetic blood flow meter, and the arterio-venous oxygen content difference across the gut seg-ment was determined photometrically. Vasopressin (4X 10' and 7 X 10' U/kg-min) diminished blood flow60 and 28% and reduced oxygen consumption 54 and22%, respectively (all P < 0.001). In a dose whichdid not lower blood flow, vasopressin still caused adecline in oxygen consumption (P < 0.01). Epinephrine(5 X 10'2 /g/kg-min) decreased blood flow 19% (P< 0.001) but did not reduce oxygen consumption.After 8-adrenergic blockade, however, the same doseof epinephrine decreased blood flow 41% and oxygenconsumption 33% (both P <0.001). Responses to an-giotensin II, calcium chloride, and prostaglandin F2.resembled effects of vasopressin rather than those ofepinephrine, namely decreased blood flow and decreasedoxygen consumption. The vasodilator agents, prosta-glandin E1, isoproterenol, and histamine, increased (P<0.001) both blood flow (130, 80, and 98%, respec-tively) and oxygen consumption (98, 64, and 70%, re-
spectively). Vasopressin, angiotensin II, calcium chlo-ride, and prostaglandin F2. appear to contract arteriolarand precapillary sphincteric smooth muscle indiscrimi-nately to evoke both intestinal ischemia and hypoxia.Epinephrine is the exceptional constrictor in this case,producing diminished blood flow without a reductionin oxygen uptake.
Dr. Pawlik's present address is the Institute of Physiol-ogy, Medical Academy of Krakow, Krakow, Poland; Dr.Shepherd's present address is Department of Physiology,The University of Texas Medical School at San Antonio,San Antonio, Tex. 78284.
Received for publication 1 November 1974 and in revisedform 5 March 1975.
INTRODUCTIONRecently, vasoconstrictor drugs, most notably intra-arterial vasopressin, have been employed in the man-agement of massive gastrointestinal hemorrhage, es-pecially from esophageal varices (1). The objective ofsuch therapy is to reduce blood flow through thesplanchnic vessels to minimize or stop bleeding. Suchtherapy in hemorrhagic states is associated with highmortality rates and with intestinal infarction (2). Onepossible explanation for the deleterious effects of vaso-pressin is that it could reduce the delivery of oxygento intestinal tissues. If intestinal blood flow is reducedby mechanical means rather than by vasoconstrictors(e.g. by reducing perfusion pressure), a concomitantincrease in oxygen extraction occurs so that oxygen up-take (the product of arteriovenous oxygen differenceand blood flow) is unaltered except at critically lowblood flow rates (3). Reducing blood flow with vaso-constrictors is not equivalent to reducing blood flowmechanically. Vasoconstrictors produce other micro-vascular effects besides a greater resistance to bloodflow.
Exogenous vasoconstrictors and sympathetic stimula-tion constrict all three of the functionally defined series-coupled elements within the intestinal microvasculature:the resistance vessels (4, 5), the capacitance vessels(4, 6), and the precapillary sphincters which determinethe number of capillaries or exchange vessels perfusedat a given moment (4-7). However, the response ofone of these functionally defined "effectors" to an ex-ogenous vasoconstrictor may be antagonized by localblood flow-controlling mechanisms such as vasodilatormetabolites or tissue hypoxia (7). Thus, the resistance-exchange-capacitance response pattern produced by ex-
ogenous vasoconstrictors depends upon the balancereached between the vasoconstrictor and the local vaso-
dilator factors at each vascular effector.By means of a computer model of the intestinal
microcirculation (7), we recently predicted that nor-
The Journal of Clinical Investigation Volume 56 August 1975s 484-490484

epinephrine and sympathetic stimulation would constrictprecapillary sphincters to such an extent that the blood-to-tissue flux of oxygen would be limited by the dif-fusion parameters, e.g., capillary surface area and capil-lary-to-cell diffusion distance (7, 8). We tested thisprediction in animal experiments by perfusing isolatedloops of canine small bowel at a constant rate of bloodflow (9). Sympathetic stimulation and intra-arterialnorepinephrine depressed oxygen extraction in a fre-quency- or dose-dependent manner. When the extrac-tion of the nonmetabolizable tracer, 8Rb, was deter-mined, rubidium extraction and oxygen extraction weresynchronously depressed by these adrenergic constric-tors (9, 10). Since rubidium extraction is a valid indexof the relative number of perfused capillaries (11), weconcluded that norepinephrine and sympathetic stimu-lation reduced the density of the perfused capillary bedto such an extent that intestinal extractions of oxygenand rubidium were depressed despite constant flowperfusion.
Although these studies (9, 10) and more recent onesfrom our laboratory (12, 13) have shown that vaso-constrictors (sympathetic stimulation, norepinephrine,epinephrine, and vasopressin) reduce intestinal oxygenextraction, our data are not comparable to that frompatients receiving vasoconstrictor therapy since our ex-periments were performed in denervated gut loops per-fused at constant flow. We performed previous studiesunder constant flow to show clearly that these agentscan alter intestinal oxygen uptake independently of theireffects on blood flow, and because the rubidium tech-nique requires constant flow (11). Constant blood flow,however, obscures the antagonism which local factorsoffer to vasoconstrictors since the accumulation of vaso-dilator metabolites or tissue hypoxia is minimized byconstant flow. Thus, it is unwise to extrapolate fromour data at constant flow to the more physiologicalcondition of constant pressure perfusion.
The purpose of the present work has been to deter-mine if vasoconstrictors reduce the oxygen uptake ofintestinal loops perfused at constant pressure, and, ifso, to determine to what extent the reduction in bloodflow and the alterations in oxygen extraction accountfor the changes in oxygen uptake. Wehave investigatedin particular the effects of vasopressin on intestinalhemodynamics and oxygen consumption and comparedits effects with those of other mesenteric vasoconstric-tor drugs (epinephrine, angiotensin II, calcium chlo-ride, and prostaglandin F.>) and with effects of vaso-dilator agents (prostaglandin E1, isoproterenol, andhistamine).
METHODSSubjects of our experiments were 50 fasted mongrel dogs ofeither sex weighing 15-20 kg each. Animals were anesthe-
tized with intravenous pentobarbital sodium (30 mg/kg).Supplemental doses of the agent were administered to main-tain deep levels of anesthesia throughout all experiments.
Both femoral arteries and veins were exposed, one veinfor injection of supplemental anesthetic and one artery forcannulation to monitor systemic arterial blood pressure,using a strain gauge transducer (Hewlett-Packard Co., PaloAlto, Calif., model 1280 C). Before the onset of experi-ments, arterial pressure exceeded 100 mmHg in all animals.
A terminal trunk of the superior mesenteric artery sup-plying a segment of distal ileum (50-100 g weight) wasexposed via a midline laparotomy. The ends of the gut seg-ment supplied by the vessel were ligated to block intra-mural collateral vessels. The probe of an electromagneticblood flow transducer (Micron Instruments Inc., Los An-gles, Calif.) of 1.5-2.0 mmsize (ID) was implanted aboutthe exposed artery and connected to an amplifier (MicronInstruments Inc.). A lateral branch of the artery was can-nulated proximal to the probe for intra-arterial infusion ofthe vasoactive agents. No attempt was made to denervatethe perfused gut segment.
A vein draining the intestinal segment was cannulatedalong with a femoral artery. A constant flow pump with-drew blood from each vessel, passed the blood through thevenous and arterial cuvettes of an arteriovenous oxygendifference analyzer, and then returned the blood to thecirculation via a femoral vein. This preparation has beendescribed previously in detail (13).
Blood flow through the branch of the mesenteric arterywas measured with precalibrated transducers. At the begin-ning and end of each experiment, we occluded the vesseldistal to the transducer to provide a transient zero flow(14). At the end of each experiment the gut segment wasexcised and weighed. In 43 animals, mean flow (±SE) was34±7 ml/min per 100 g of tissue before the onset of druginfusion. Intestinal oxygen consumption was calculated asthe product of the simultaneously measured arteriovenousoxygen content difference and the mean blood flow (10, 13).The mean rate of oxygen consumption was 2.4±0.5 ml oxy-gen/min per 100 g tissue in these animals. These intestinalblood flow and oxygen consumption values agree withthose reported elsewhere (3, 15).
Each drug was infused into the mesenteric artery for 10min in each animal. The drugs employed, their com-mercial sources and doses, and the number of separate ani-mal experiments are indicated in Table I. With vasocon-strictor agents a dose was usually selected which wouldreduce blood flow about 20-25%o; with vasopressin a morepotent and a less potent dose were also studied. With thevasodilator drugs doses were selected to double blood flowapproximately. In experiments with epinephrine and iso-proterenol, we used propranolol comparing responses ofintestinal oxygen consumption and blood flow with eachcatecholamine alone and with the same dose of epinephrineor isoproterenol after j8-blockade with propranolol (0.1-0.3mg injected intra-arterially). A total of 88 separate ex-periments were conducted in 43 dogs. No dogs were usedtwice for the same dose of a drug, except in experimentswith propranolol.
Since each agent was infused directly into the mesentericartery in small doses, there was far less effect upon sys-temic arterial pressure than upon mesenteric artery bloodflow. The vasoconstrictor agents either increased systemicarterial pressure slightly (< 10 mmHg) or had no effect,and the vasodilator drugs either decreased blood pressureslightly or had no effect. Therefore, the primary effect ofeach agent was considered to be a direct one upon the
Vasoactive Drugs and Intestinal Oxygen Uptake 485

I-150 -
100 -
50 L
VASOPRESSIN
80
10
A - V&02(ml /lO0ml ) S -
O _I min 10 min
FIGUit 1 Effect of vasopressin infusion on systemic arterial pressure, mesenteric artery branchblood flow and arteriovenous oxygen difference across the intestinal circulation in one experi-ment. Since arterial pressure changed little, the effect of vasopressin on the local circulationis that of a direct constrictor agent. Note the reciprocal response of A-V,02 to the changein blood flow.
vascular bed under study rather than a reflex-induced effect.Furthermore, our data have not been expressed in terms
TABLE IAgents Used in the Present Study
Number ofIntra-arterlal separate dog
Agent dose experiments
per kg bodywi/min
VasoconstrictorsVasopressin 4 X 10- U 8
(Pitressin tannate,Parke, Davis & Co.,Detroit, Mich.)
Vasopressin 7 X 10-4 U 7Vasopressin 3 X 10-4 U 6Epinephrine 50 ng 9
(Adrenalin chloride,Parke, Davis & Co.)
Epinephrine after 9propranolol hydrochloride(Inderal, AyerstLaboratories, NewYork)
Angiotensin II 25 ng 7(Hypertensin, CIBAPharmaceutical Company,Summit, N. J.)
Calcium chloride 300 pg 7Prostaglandin Fua 250 ng 7
(The Upjohn Company,Kalamazoo, Mich.)
VasodilatorsProstaglandin Et 500 ng 7
(The Upjohn Company)Isoproterenol 500 ng 7
(Isuprel, WinthropLaboratories, NewYork)
Isoproterenol 7after propranolol hydrochloride
Histamine acid phosphate 500 ng 7(Eli Lilly and Company,Indianapolis, Ind.)
of resistance, since resistance values would be approxi-mately reciprocal to changes in blood flow.
Significance of changes was determined using the pairedt test with a confidence level of 5%o or less. For each agentresults have been presented graphically as a percent changeof blood flow and of oxygen consumption from the controlvalue obtained in the last minute before starting infusionof the drug (Figs. 2-5). The paired t test was used toevaluate significance of changes from control.
RESULTS
Vasopressin was infused intra-arterially at three dif-ferent dose rates: 4 X 10V, 7 X 10-4, and 3 X 10 U/kg-min. Results from one experiment using the highestdose of vasopressin are reproduced in Fig. 1. Thehighest dose caused a 60% decrease (P < 0.001) inblood flow and a 54% decrease (P <0.001) in oxygenconsumption. The lowest dose caused no change in
blood flow; however, oxygen consumption declined 6%(P < 0.01) with the lowest dose of vasopressin. These
results appear in Fig. 2. Values indicated in this and
succeeding figures were obtained during the steady-state phase of the infusion.
Intra-arterial epinephrine decreased intestinal blood
flow 19% (P < 0.001). Oxygen consumption was un-
changed by epinephrine. After ,B-blockade with pro-pranolol the same dose of epinephrine decreased bloodflow 41% (P < 0.001 ) and decreased oxygen con-
sumption 33% (P < 0.001). These results appear in
Fig. 3.
486 W. Pawlik, A. P. Shepherd, and E. D. Jacobson
ARTERIALPRESSURE
(mmHg)
BLOODFLOW
(ml /min)-
OXYGENCONSUMPTION BLOOD FLOW
EPINEPHRINE ALONE
i EPINEPHRINE AFTERPROPRANOLOL
4.0 mU/kg-min
m0.7 mU/kg-min
* 0.3 mU/kg-min
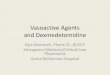
FIGURE 2 Effects of three doses of vasopressin on bloodflow and oxygen consumption of the intestinal segment.Bars represent mean values (- +SE) from each series ofexperiments. Note that the lowest dose of vasopressin sig-nificantly (P < 0.05) reduced oxygen consumption withoutaltering blood flow. The values indicated are those obtainedduring the steady-state phase of the infusion.
Angiotensin II reduced blood flow and oxygen con-
sumption 26 and 18%, respectively (both P < 0.001).Calcium chloride diminished both blood flow and oxy-gen consumption by 12% (P < 0.05 and 0.001, respec-tively). Prostaglandin F2. lowered blood flow 27%and oxygen consumption 21% (both <0.001). Valuesobtained with these constrictor agents are depictedin Fig. 4.
Prostaglandin E1 increased blood flow 130% andoxygen consumption 98% (P < 0.001 for both). Iso-proterenol raised blood flow 80% and oxygen con-
sumption 64% (both P < 0.001). After propranololblockade, both responses to the same dose of isopro-terenol were not significantly different from control.Histamine augmented blood flow 98% and oxygen con-
sumption 70% (P < 0.001 for both). Values obtainedwith dilator drugs are indicated in Fig. 5.
DISCUSSION
The two most important structures of the intestinalmicrocirculation which regulate total blood flow to thegut and capillary blood flow, respectively, are the ar-
teriolar smooth muscle and the muscle of the precapil-lary sphincters. More than half of the resistance to thetotal flow of blood through the gut occurs duringpassage of the blood through the arterioles (16). Smallchanges in the diameter of these vessels are translated
FIGuRE 3 Effects of epinephrine before and after propra-nolol on blood flow and oxygen consumption of the gut seg-ment in nine experiments. After p-blockade epinephrine in-duced more severe vasoconstriction, and the oxygen-sparingcapacity of the catecholamine was lost. The values indicatedare those obtained during the steady-state phase of theinfusion.
into large changes in blood flow through the superiormesenteric artery. However, it is also true under''resting" conditions that only one-third to one-fourthof the capillaries are open to the flow of blood at anymoment in time (17). Thus, by identifying the diffu-sion parameters (surface area and diffusion distance),it becomes apparent that the density of the perfusedcapillary bed is a critical determinant of tissue oxygenextraction. Furthermore, our calculations indicate thatchanges in the density of the perfused capillary bed
BLOOD FLOW
z
I -
C.)
z
C;
-50-
OXYGENCONSUMPTION
it~~~~~ANGIOTENSIN 11
0 CaC12
PROSTAGLANDINF2
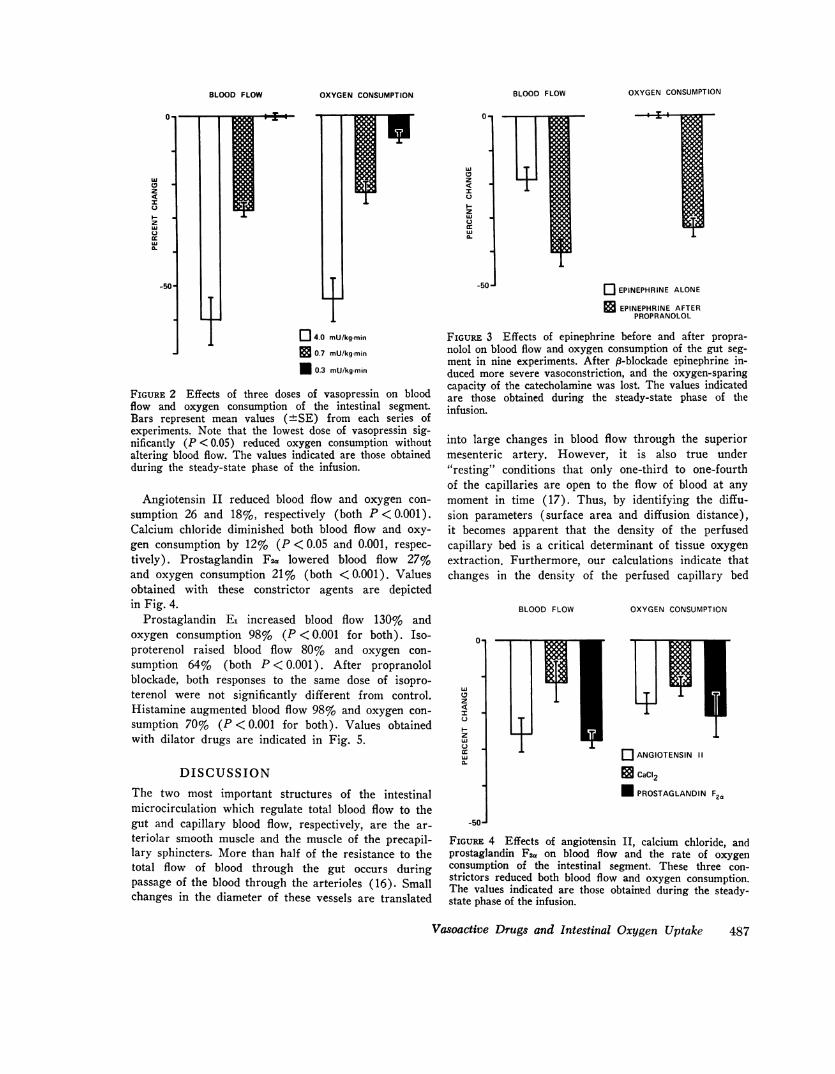
FIGURE 4 Effects of angiotensin II, calcium chloride, andprostaglandin F2, on blood flow and the rate of oxygen
consumption of the intestinal segment. These three con-
strictors reduced both blood flow and oxygen consumption.The values indicated are those obtained during the steady-state phase of the infusion.
Vasoactive Drugs and Intestinal Oxygen Uptake 487
Al:
z
IC)
z
0-
Lu
z
I
zC)
MU
-50-
OXYGENCONSUMPTIONBLOOD F LOW

BLOOD FLOW OXYGENCONSUMPTIONQ
PROSTAGLANDINEl
+150 0 ISOPROTERENOLALONE
_ ISOPROTERENOLAFTER PROPRANOLOL
HISTAMINECDz
+100-zT
+50-
FIGURE 5 Effects of prostaglandin E1, isoproterenol (before and after propranolol), and his-tamine on blood flow and oxygen consumption of perfused intestinal segments. The valuesindicated are those obtained during the steady-state phase of the infusion.
are as significant to oxygen delivery as are the changesin blood flow (7, 8, 10). It also follows that a drugmay cause a sizeable decrease in the total flow of bloodto the gut without reducing the delivery of oxygen tothe tissue, since extraction of oxygen can increase tocompensate for the reduced total blood flow. If theagent constricts arteriolar smooth muscle selectively,without affecting the ability of the precapillary sphinc-ters to regulate the diffusion parameters so as to in-crease oxygen extraction, intestinal oxygen consump-tion will not suffer until total blood flow is reducedto a critically low level (3, 7, 10). Use of a drug witha selective constrictive action on arterioles would per-mit production of ischemia without imperiling theviability of the gut with hypoxia.
Unfortunately, the present study has shown that themost commonly employed vasoconstrictor in cases ofsevere gastrointestinal hemorrhage, namely vasopres-sin, may not possess this selectivity. Vasopressin re-
duced the oxygen uptake of gut loops perfused bothat constant flow (12) and, as the present study shows,at constant pressure. In the present study, the lowestdose of vasopressin reduced oxygen uptake withoutlowering blood flow, whereas higher doses reducedboth blood flow and oxygen consumption (Fig. 2).The changes in blood flow and oxygen uptake occurredquite rapidly (Fig. 1) and we interpret them as a
vascular effect of vasopressin to lower oxygen delivery.However, an alternative explanation is that vasopressinmight reduce the tissue demand for oxygen via a
direct metabolic effect since vasopressin is known to
depress electrolyte transport in vivo (18). We feelthe metabolic explanation is less likely than the vascular
one because the changes in oxygen consumption whichoccur when sugar-electrolyte or dinitrophenol solutionsare placed in the lumen are much slower than arethe vasopressin-induced changes in oxygen uptake (un-published observations from our laboratory). In addi-tion, vasopressin stimulates both the electrolyte absorp-tion (19, 20) and the oxygen consumption (20) rateof isolated epithelia in which the vascular mechanismhas been eliminated. Because reports conflict concerningvasopressin's transport effect in vivo (18, 21), it is notunlikely that vasopressin lowers blood flow and oxygendelivery. This, in turn, could lead to the diminishedelectrolyte transport seen in vivo.
In the present study all intestinal vasoconstrictors,except epinephrine, reduced both total blood flow to thegut and intestinal oxygen consumption. Thus, vasopres-sin, angiotensin II, calcium chloride, and prostaglandinF2a each evoked ischemia and hypoxia, approximatelyin parallel. In other studies we have found that cardiacglycosides (13), epinephrine, vasopressin (12), nor-epinephrine, and electrical stimulation of splanchnicsympathetic nerves (9, 10) depress oxygen extractiondespite constant flow perfusion. In terms of identifyingthe responsive structures in the intestinal microcircu-lation which regulate total blood flow and the densityof the perfused capillary bed, the aforementioned vaso-
constrictors seemed to act on smooth muscle of botharterioles and precapillary sphincters, since rubidiumextraction was also depressed.
Epinephrine is an exceptional vasoconstrictive agent.One explanation for the action of this agent would be
that epinephrine constricted mesenteric arteriolarsmooth muscle, thereby increasing the vascular re-
488 W. Pawlik, A. P. Shepherd, and E. D. Jacobson

sistance and reducing total blood flow to the gut, butin the dose used did not constrict the precapillarysphincters. Consequently, the nutrient circulation waspreserved, and oxygen consumption was not depressedby epinephrine. In support of this possibility are find-ings of Zweifach (22) who showed in the rat mesen-teric circulation under direct visualization that ar-teriolar smooth muscle contracted brickly to topicalepinephrine but that precapillary sphincters were un-responsive.
An alternative explanation for effects observed withthis catecholamine would be that epinephrine constrictedprecapillary sphincters but also increased tissue metabo-lism and lowered intracellular Po2, thereby increasingthe capillary-to-cell oxygen gradient. This would ex-plain our finding that epinephrine caused no decreasein oxygen consumption. This possibility is consistentwith our finding in gut loops perfused at constant flow(12) that small doses of epinephrine caused an in-crease in both oxygen consumption and in the clear-ance of 'Rb. At this time, the mechanism wherebyepinephrine maintained normal levels of oxygen con-sumption in the face of reduced blood flow to the gutis uncertain.
The ability of the P-adrenergic antagonist, propra-nolol, to abolish the oxygen-sparing properties of epi-nephrine was not unexpected, since norepinephrine re-duced oxygen consumption in a constant-flow prepara-tion (9, 10). In addition, when epinephrine increasedoxygen uptake in gut loops at constant flow, propranololcaused the same dose of epinephrine to reduce oxygenconsumption (12). One inference from our results isthat the precapillary sphincter may contain a greaterdensity of P-adrenergic receptors than does the ar-teriole. Thus, epinephrine, which can stimulate both a-constrictor and P8-dilator receptors, is able in someconcentrations to constrict the arterioles without con-stricting and perhaps even dilating the precapillarysphincters. After propranolol, epinephrine reduced oxy-gen consumption and depressed total blood flow moreintensely (Fig. 3).
The oxygen-sparing capacity of epinephrine sets itapart from all other vasoconstrictors that we havestudied in the canine intestine. It alone could reduceblood flow without impairing oxygen delivery. Un-fortunately, epinephrine has other undesirable effectsin patients including a vasodilatory action in low dosesthat could intensify the hemorrhage it was intended tocheck. Therefore, if gastrointestinal hemorrhage is tobe managed effectively with vasoconstrictor drugs, asearch should be undertaken to identify a safer drugor drug combination which can also lower intestinalblood flow without depressing oxygen consumption bythe gut.
ACKNOWLEDGMENTSThe authors are grateful to Ms. Paula Leis for technicalassistance.
This research was supported in part by U. S. PublicHealth Service grant AM 15997.
REFERENCES
1. Conn, H. O., G. R. Ramsby, and E. H. Storer. 1972.Selective intraarterial vasopressin in the treatment ofupper gastrointestinal hemorrhage. Gastroenterology. 63:634-645.
2. Renert, W. A., K. F. Button, W. J. Casarella, and S. L.Fuld. 1972. Mesenteric venous thrombosis and smallbowel infarction following infusion of vasopressin intothe superior mesenteric artery. Radiology. 102: 299-302.
3. Johnson, P. C. Autoregulation of intestinal blood flow.1960. Am. J. Physiol. 199: 311-318.
4. Mellander, S., and B. Johansson. 1968. Control of re-sistance, exchange, and capacitance functions in theperipheral circulation. Pharmacol. Rev. 20: 117-196.
5. Dresel, P., B. Folkow, and I. Wallentin. 1966. Rubid-iumM clearance during neurogenic redistribution of in-testinal blood flow. Acta Physiol. Scand. 67: 173-184.
6. Cobbold, A., B. Folkow, 0. Lundgren, and I. Walletin.1964. Blood flow, capillary filtration coefficients, and re-gional blood volume responses in the intestine of the catduring stimulation of the hypothalamic 'defense' area.Acta Physiol. Scand. 61: 467475.
7. Shepherd, A. P., and H. J. Granger. 1973. Autoregula-tory escape in the gut: a systems analysis. Gastroen-terology. 65: 77-91.
8. Granger, H. J., and A. P. Shepherd. 1973. Intrinsicmicrovascular control of tissue oxygen delivery. Micro-vasc. Res. 5: 49-72.
9. Shepherd, A. P., D. Mailman, T. F. Burks, and H. J.Granger. 1973. Effects of norepinephrine and sympatheticstimulation on extraction of oxygen and MRb in per-fused canine small bowel. Circ. Res. 33: 166-174.
10. Shepherd, A. P., D. Mailman, T. F. Burks, and H. J.Granger. 1973. Sympathetic nervous control of intestinal02 extraction. In Oxygen Transport to Tissue: Instru-mentation, Methods, and Physiology. H. I. Bicher andD. F. Bruley, editors. Plenum Publishing Corp., NewYork. 423428.
11. Renkin, E. M., and S. Rosell. 1962. The influence ofsympathetic adrenergic vasoconstrictor nerves on trans-port of diffusible solutes from blood to tissues in skele-tal muscle. Acta Physiol. Scand. 54: 223-240.
12. Jacobson, E. D., D. Mailman, A. P. Shepherd, and W.Pawlik. 1974. Intestinal ischemia and hypoxia: vaso-pressin vs. epinephrine. Gastroenterology. 66: 715.(Abstr.)
13. Pawlik, W., A. P. Shepherd, D. Mailman, and E. D.Jacobson. 1974. Effects of ouabain on intestinal oxygenconsumption. Gastroenterology. 67: 100-106.
14. Jacobson, E. D., and K. G. Swan. 1966. Hydraulic oc-cluder for chronic electromagnetic blood flow determina-tions. J. Appl. Physiol. 21: 1400-1402.
15. Jacobson, E. D. 1965. The circulation of the stomach.Gastroenterology. 48: 85-109.
16. Selkurt, E. E. 1971. Peripheral blood pressures andpulses: venous pressure and venous return. In Physiol-ogy. E. E. Selkurt, editor. Little, Brown and Company,Boston. 3rd edition. 345-370.
Vasoactive Drugs and Intestinal Oxygen Uptake 489
17. Folkow, B. 1967. Regional adjustments of intestinal 20.blood flow. Gastroenterology. 52: 423-432.
18. Soergel, K. H., G. E. Whalen, J. A. Harris, and J. E.Geenen. 1968. Effect of antidiuretic hormone on humansmall intestinal water and solute transport. J. Clin. In- 21.vest. 47: 1071-1082.
19. Aulsebrook, K. A. 1961. Effect of vasopressin on sodium 22.transfer by rat colon in vitro. Endocrinology. 68: 1063-1065. (Abstr.)
Parisi, M., and P. J. Bentley. 1970. Effects of vaso-pressin, cyclic AMP, and theophylline on oxygen con-sumption of toad bladder 'sacs'. J. Endocrinol. 48: 117-124.Blickenstaff, D. D. 1954. Increase in intestinal absorp-tion of water from isosmotic saline following pitressinadministration. Am. J. Physiol. 179: 471472.Zweifach, B. F. 1961. Functional Behavior of the Mi-crocirculation. Charles C. Thomas, Publisher, Spring-field, Ill.
490 W. Pawlik, A. P. Shepherd, and E. D. Jacobson