Embed Size (px)
Citation preview

Kidney International, Vol. 60 (2001), pp. 2367–2376
Effects of uremic serum on isolated cardiac myocyte calciumcycling and contractile function.
SANKARIDRUG M. PERIYASAMY, JIE CHEN, DEREK COONEY, PATRICIA CARTER, EIAD OMRAN,JIANG TIAN, SNIGDHA PRIYADARSHI, ALEXEI BAGROV, OLGA FEDOROVA,DEEPAK MALHOTRA, ZIJIAN XIE, and JOSEPH I. SHAPIRO
Departments of Medicine and Pharmacology, Medical College of Ohio, Toledo, Ohio, and National Institute of Aging, NationalInstitutes of Health, Bethesda, Maryland, USA
concentration as well as impaired relaxation. As these effectsEffects of uremic serum on isolated cardiac myocyte calciumare similar to that seen with ouabain and can be prevented bycycling and contractile function.co-incubation with an antibody fragment to digitalis, whichBackground. Diastolic dysfunction occurs in patients withalso attenuates the sodium pump inhibitory effect, we suggestchronic renal failure. Moreover, serum from uremic patientsthat this (these) substance(s) circulating in uremic sera andcontains one or more inhibitors of the plasmalemmal Na,K-inhibiting the sodium pump also causes the acute diastolicATPase (sodium pump). We hypothesized that a circulatingdysfunction seen in our system.substance present in uremic sera contributes to both sodium
pump inhibition and diastolic dysfunction.Methods. Serum samples were obtained from six patients
Patients with renal failure develop cardiac complica-with chronic renal failure and diastolic dysfunction.Results. Their serum samples caused marked inhibition of tions extremely frequently. In end-stage renal disease
Na,K-ATPase purified from dog kidney at all concentrations (ESRD) patients treated with hemodialysis in the Unitedstudied (all P � 0.01) and also impaired ouabain-sensitive States, mortality rates exceed 20% per year with morerubidium uptake by myocytes isolated from Sprague-Dawley
than 50% attributed to cardiac mortality [1]. Althoughrats (P � 0.01). These cardiac myocytes were studied for theirthe term “uremic cardiomyopathy” had previously beencontractile function with video-edge detection and calcium me-used to refer to a dilated cardiomyopathy complicatingtabolism with indo-1 fluorescence spectroscopy after exposure
to these uremic sera. These uremic sera caused increases in renal failure, more recent studies suggest that the mostmyocyte fractional shortening (P � 0.01) as well as an increase common form of heart disease in renal failure patientsin the time constant of relengthening (P � 0.01). Examining is one characterized by diastolic dysfunction and leftthe calcium transient, the time constant for calcium recovery ventricular hypertrophy [2]. Although several putativewas also increased (P � 0.01). Exposure of these cells to sera
mechanisms for the diastolic dysfunction have been sug-from age- and sex-matched healthy subjects did not result ingested, its pathogenesis is still unclear [3].significant changes in contraction or calcium cycling. Extracts
of uremic serum samples inhibited isolated Na,K-ATPase For many years, it has been known that a substance(s)whereas extracts of normal serum samples did not. The effect is (are) present in the serum of patients with ESRDof uremic serum extracts on contractile function and calcium that inhibit(s) the function of sodium potassium ATPasecycling were quite similar to that of intact serum or the addition (Na,K-ATPase) in vitro [4–7]. Since the transmembraneof ouabain. Co-incubation of uremic serum extract with an
sodium gradient drives calcium extrusion through so-antibody fragment directed against digoxin markedly attenu-dium–calcium exchange in the myocyte, and because thisated the inhibition of Na,K-ATPase activity and completely
prevented any effects on calcium cycling or contractile func- mechanism may account for about 30 to 40% of calciumtion. removal from the cytosol following stimulation (de-
Conclusion. These data show that one or more substances pending on species) [8, 9], we hypothesized that sodiumare present in uremic sera that acutely cause increased force of pump inhibition produced by this (these) substance(s)contraction and impaired recovery of cardiac myocyte calcium
in uremic serum could contribute to impaired ventricularrelaxation. To examine this concept further, the follow-ing studies were performed.Key words: sodium pump, potassium, ATPase, ventricular dysfunction,
myocardial calcium, diastolic dysfunction, Na,K-ATPase, uremic car-diomyopathy.
METHODSReceived for publication March 26, 2001
Patient serum samplesand in revised form July 5, 2001Accepted for publication July 11, 2001 Serum samples were collected from six patients with
ESRD treated with hemodialysis for more than one year. 2001 by the International Society of Nephrology
2367

Periyasamy et al: Uremic sera and diastolic dysfunction2368
Table 1. Clinical characteristics of uremic patients was added to the assay medium with enzyme to bring thetotal volume to 1.0 mL; the mixture was then incubated atControl Uremic37�C for five minutes before starting the reaction. En-Age 21, 25, 39, 22, 28, 35,
46, 51, 55 44, 52, 55 zyme assays were carried out in triplicate for each serumSex 4 M 2 F 4M 2 F sample, and the average value assigned to each patientCause of ESRD Diabetes (3)
or control.Hypertension (2)Polycystic kidney (1)
Systolic blood pressure Isolation and culture of cardiac myocytesmm Hg 152�5
Cardiac myocytes were isolated from the ventricle ofDiastolic blood pressuremm Hg 82�6 rat as described previously [11] with minor modifications.
Hypertensive medications None Calcium channel Sprague-Dawley rats weighing between 250 and 300 gantagonist (3)
were anesthetized with sodium pentobarbital (60 mg/kgBeta-blocker (3)Converting enzyme IP) and the hearts were rapidly removed and attached
inhibitor (3) to an aortic cannula. The heart was retrograde perfusedCentrally acting
for 15 minutes with medium (A) containing Joklik mini-antagonist (2)mum essential medium (MEM; Sigma, St. Louis, MO,Results for blood pressure determined predialysis (for Uremic patients) are
expressed as mean � SEM. All uremic patients were receiving at least one USA), 24 mmol/L NaHCO3 and 1.25 mmol/L CaCl2 toantihypertensive agent, and most were on more than one. wash out blood, followed by medium (A) without Ca2�
for five minutes. The heart was then perfused with JoklikMEM containing 24 mmol/L NaHCO3 and 0.2 mg/mLcollagenase type 2 (Worthington Corp., Freehold, NJ,The clinical features of these six patients are summarizedUSA), and the perfusate was recirculated for 20 to 30in Table 1. Of note, each of these patients had left ven-minutes until the heart became soft and flaccid. To disso-tricular hypertrophy and diastolic dysfunction found onciate the myocytes, the left ventricle was cut out fromroutine Doppler echocardiography by the clinician read-the heart, minced with scissors in MEM containing 24ing the study. Predialysis blood pressure values weremmol/L NaHCO3 and 0.1 mg/mL collagenase and 2%transcribed from routine dialysis flow sheets. Blood sam-wt/vol bovine serum albumin (BSA; Sigma), and gentlyples from these patients and six age- and sex-matchedagitated for five minutes in the same buffer. The myo-controls were obtained, and the serum was frozen andcytes were harvested by drawing off the supernatant,kept at �80�C until subsequent study. In some cases,filtered through gauze and centrifuged at 200 rpm forthe serum samples were deproteinized and extracts weretwo minutes.
produced using the method of Stokes et al [4]. InformedTo make the myocytes Ca2� tolerant after isolation in
consent was obtained prior to drawing blood samples in Ca2�-free medium, the pellet was resuspended in Joklikaccordance with the Medical College of Ohio Institu- MEM with a gradual increase in the concentration oftional Review Board. Ca2� from 10 to 100 �mol/L. Finally, the isolated myo-
cytes were suspended in medium (c) containing M199Measurement of Na,K-ATPase activity(Sigma) supplemented with 24 mmol/L NaHCO3, 0.1%
To study the effect of sera on Na,K-ATPase activity, BSA, 2 mmol/L l-carnitine, 5 mmol/L creatine and 5purified dog kidney Na,K-ATPase with specific activity mmol/L taurine at 37�C for one hour. The calcium con-in the range of 800 to 1000 �mol of adenosine 5�-triphos- centration of this medium is 1.8 mmol/L. All the mediaphate (ATP) hydrolyzed/mg of protein/h was used [10]. used for isolation were adjusted to pH 7.3 and myocytesNa,K-ATPase activity was measured using a reaction were maintained at 37�C and gassed with 95% O2 � 5%mixture containing 50 mmol/L Tris-HCl, pH 7.4, 4 mmol/L CO2 throughout the isolation period. This method ofMgCl2, 2 mmol/L egtazic acid (EGTA), 100 mmol/L isolation produced a good yield of rod-shaped (70 toNaCl, 10 mmol/L KCl, 3 mmol/L (�-32P)-ATP and 3-5 80%) myocytes. For attachment of myocytes to cov-�g of purified enzyme; reactions were measured in the erslips, the myocyte suspension was plated onto lamininpresence and absence of 1 mmol/L ouabain. Enzymatic (Sigma) coated coverslips that were then placed in 60reaction was initiated by the addition of (�-32P)-ATP and mm dishes and incubated at 37�C for one hour.terminated five minutes later by the addition of ice-cold
Measurement of ouabain-sensitive 86Rb� uptake8% perchloric acid. Released inorganic (32P)-phosphatewas measured as described by Askari, Huang and Anti- Ouabain-sensitive 86Rb� uptake was measured in du-eau [10]. The difference between ATPase activity in the plicate at 37�C using adult myocytes isolated as describedpresence and absence of 1 mmol/L ouabain was consid- previously [11]. The uptake of 0.5 �mol/L 86RbCl (1.5ered to be Na,K-ATPase activity. To study the effect of to 2 106 cpm) by myocytes (105 cells) was studied using
an uptake medium (140 mmol/L NaCl, 4 mmol/L KCl,sera on Na,K-ATPase, serum (25, 50, 75 and 100 �L)

Periyasamy et al: Uremic sera and diastolic dysfunction 2369
1 mmol/L MgCl2, 0.1 mmol/L CaCl2, 10 mmol/L glucose, The cells were then washed twice with medium (c) to re-move extracellular dye. The coverslip with the attachedand 10 mmol/L Hepes, pH 7.4, and 5 �mol/L monensin);
the 86Rb� uptake was determined in the presence and indo-1 loaded myocytes was placed in the chamber filledwith 1 or 2 mL of medium (c). The chamber was thenabsence of 1 mmol/L ouabain. Uptake was initiated by
adding 86RbCl and was terminated 20 minutes later by mounted on the stage of an inverted microscope (NikonDiaphot) equipped with an objective lens (40 Fluar/rapid vacuum filtration through a nitrocellulose filter
with a pore size of 5 �m (Millipore Corporation, Bed- 1.30 oil; Carl Zeiss Instruments, Zurich, Switzerland).The cell was field stimulated at 0.5 Hz (5-ms pulse dura-ford, MA, USA). The filter was washed five times with
3 mL of ice-cold uptake medium. Each filter was trans- tion) by a pair of platinum electrodes connected to aGrass stimulator. For stimulation, myocytes that wereferred to a glass vial containing 5.0 mL of scintillation
fluid (Cytocint; ICN Biochemicals, Cleveland, OH, USA). rod-shaped with clear striations, unattached to eitheradjacent cells or debris, and without spontaneous con-The radioactivity retained on the filter was determined
by using a Beckman liquid scintillation counter. To study tractions were used. An adjustable iris was used tochoose the optical image of only one myocyte in eachthe effect of sera on 86Rb� uptake, serum (50 �L) was
added to the uptake medium containing myocytes (total experiment to minimize background fluorescence. Themyocytes loaded with indo-1 were excited by a 75 Wvolume 1 mL) and incubated at 37�C for five minutes
before initiating the 86Rb� uptake. Under our experimen- xenon lamp at 355 nm (2 mm slit width) and the emittedfluorescence derived from within a single cell was splittal conditions, the specific activity of ouabain–sensitive
86Rb� uptake was in the range of 25-35 nmol/mg of into two beams. One of the beams passed through a 405nm filter and the other passed through a 485 nm filterprotein/h.
Epithelial cells from rat kidney (NRK) and from pig (corresponding to the peak emission of Ca2� bound andCa2� free forms of the indicator, respectively) and thekidney (LLC-PK1) were obtained from American Type
Culture Collection (Rockville, MD, USA) and were emerging lights were then directed to two separate pho-tomultiplier tubes. The indo-1 emission ratio (R) of 405/grown in 12-well plates containing Dulbecco’s modified
Eagle’s medium (DMEM; Sigma), 5% fetal bovine se- 485 was acquired by using the Felix software programand stored in a personal computer for later off-line analy-rum (FBS; Sigma), 100 U/mL penicillin and 100 �g/mL
streptomycin at 37�C in 5% CO2 and 95% air. After sis. In cases where the effects of acute sodium pumpinhibition with ouabain or deproteinized serum extractsreaching subconfluence (80%), the cells were washed
twice with serum-free DMEM and were maintained in were studied, calculations of cytosolic calcium concentra-tion ([Ca2�]i) were made using the formula:the same medium for six hours. For 86Rb� uptake, the
method described above was followed with modification.[Ca2�]i Kd Dfree/Dbound (R � Rmin)/(Rmax � R)
Briefly, the cells maintained on serum free medium werewashed once and incubated at 37�C in the same medium where the Kd was assumed to be 250 nmol/L, the Dfree
and Dbound represent the intensity of the fluorescence atcontaining 2.5 �mol/L monensin and different concen-trations of ouabain or different volumes of deproteinized 485 nm following EGTA (4 mmol/L) and ionomycin
(10�6 mol/L) treatment of the cell, respectively, and Rminserum. After 30 minutes of incubation with ouabain ordeproteinized serum, 86Rb� uptake was started by the and Rmax were the ratios obtained under these conditions
as well as previously described by Bers, Bassani andaddition of 86RbCl (106 cpm/well), and 30 minutes laterthe uptake was terminated by washing the wells three Bassani [12]. Because the addition of human serum (ei-
ther 100 or 250 �L of media was added to make a totaltimes with 3 mL of ice-cold 0.1 mol/L MgCl2. The 86Rb�
taken up by the cells was extracted by shaking the cells volume of 2.5 mL) caused a marked and unpredictablechange in the autofluorescence of the sample, we didwith 10% ice-cold trichloroacetic acid (TCA) for 60 min-
utes, and the TCA extracted 86Rb� was counted. TCA not calculate [Ca2�]i in cells to which human serum wasadded, but rather restricted our analysis of these cellsprecipitated cellular protein was dissolved in 0.1 N
NaOH and the protein content was determined by bicin- to the determination of the time to maximal calciumfrom baseline and the time constant (� value) for thechoninic acid (BCA) assay using bovine serum albumin
as standard. exponential decay from peak calcium [9]. Fluorescencemeasurements made prior to addition of serum (or oua-
Measurement of Ca2� transient: bain) were compared with those made five minutes after-wards.The Ca2� transient was measured by using the Ca2�
selective fluorescent dye indo-1 and spectrofluorimeterMeasurement of contractility(Photon Technology International, Monmouth Junction,
NJ, USA). After attachment of cells to the coverslips, Myocyte contractility was measured by using the edgedetector device (Crystal Biotech, Northboro, MA, USA).myocytes were loaded with 5 �mol/L indo-1-AM (Molec-
ular Probes, Eugene, OR, USA) at 37�C for 30 minutes. To monitor and record myocyte contraction (cell length)

Periyasamy et al: Uremic sera and diastolic dysfunction2370
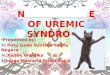
simultaneously, indo-1 loaded cells were illuminatedwith bright light from a 50 W standard light source ofthe microscope passed through a red filter (650 nm)while being stimulated at 0.5 Hz, and monitored withfluorescence spectroscopy as described above. The imageof the contracting myocyte was deflected by a custombuilt dichroic filter that was placed in the C-arm of themicroscope proximal to the adjustable iris that localizedfluorescence to within a single cell. The dichroic filterreflected red light 90 degrees but allowed the wave-lengths of less than 550 nm to pass through to the fluo-rescence detection system. The myocyte image was mon-itored continuously using a video camera (FTM800Image Sensor Module, Philips Imaging Technology, The Fig. 1. Relationship between amount of serum and inhibition of puri-Netherlands) connected to a video-edge detector. The fied NaK-ATPase activity. Symbols are: (�) control patients; (�) ure-
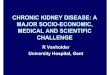
mic patients. **P � 0.01 vs. control.cell image scanned by the camera at 60 Hz was displayedon a TV monitor and also was recorded on a video tape.The shortening and relengthening of myocytes were ac-quired using a Felix software program and stored in a ent from ouabain on the rubidium uptake of the cellpersonal computer for later off-line analysis. Again, edge lines studied. LLC-PK1 cells (derived from porcine kid-detection measurements obtained before altering experi- ney) were chosen to represent a cell type in which themental conditions were compared to those made five expressed Na,K-ATPase isoform is quite ouabain sensi-minutes afterwards. tive whereas NRK cells (derived from rat kidney) were
chosen because they are much less ouabain sensitive.Statistical analysisThe uremic serum extracts inhibited ouabain-sensitive
Data obtained were compared using the unpaired orrubidium uptake in dose dependent manner quite simi-paired Student t test with Scheffe’s correction for multi-larly in both cell lines whereas the dose dependence ofple comparisons depending on the unpaired or pairedouabain induced inhibition was, as expected, markedlynature or the data [13]. Statistical analysis was performeddifferent between the LLC-PK1 and NRK cells (Fig. 2).using Sigmastat� software. All animal experimentation
described in the manuscript was conducted in accord with Effect of uremic sera on contraction, relaxation andthe NIH Guide for the Care and Use of Laboratory Ani- the calcium transientmals using protocols approved by the Medical College
Uremic sera (both 1:24 and 1:9 dilutions) had a veryof Ohio Institutional Animal Use and Care (IACUC)significant effect on both contractile and relaxation func-Committee.tions of the isolated myocytes as determined by edgedetection analysis as well as on calcium metabolism,
RESULTS whereas control sera did not have a significant effect onany of the parameters examined. Uremic sera causedEffect of uremic sera on Na,K-ATPase activity and
ouabain-sensitive rubidium uptake increases in the amount of cell contraction and the timeconstant for relaxation (both P � 0.01) but did not sig-Both uremic sera and control sera were found to in-nificantly affect the time to peak contraction (Table 2).hibit purified Na,K-ATPase enzyme activity at each ofBecause of significant and unpredictable effects of serathe doses studied. These data are summarized in Figureon background autofluorescence, we could not reliably1. The amount of sodium pump inhibition was consider-calculate the effects of serum samples on [Ca2�]i; how-ably higher with the uremic sera as compared to controlever, uremic but not normal sera were found to signifi-sera at any all dilutions studied. Uremic sera also inhib-cantly increase the time constant for calcium normaliza-ited ouabain-sensitive rubidium uptake to a greater de-tion following stimulation (P � 0.01) whereas controlgree than control sera (58.6 � 4.3 vs. 28.6 � 3.2% whensera did not have demonstrable effects on these measure-studied at a concentration of 5% in the reaction media,ments (Table 2). The time to peak calcium concentrationP � 0.01). After deproteinization of the serum samples,was not affected by either control or uremic sera. Anuremic extracts (5%) still produced significant inhibitionexcellent correlation was observed between the changesof the purified Na,K-ATPase activity whereas controlin � values as assessed by edge detection and fluorescenceextracts essentially did not inhibit it (46.0 � 1.7 vs. 3.3 �spectroscopy induced by the serum samples (R2 0.55,1.1%, P � 0.01).
The effects of uremic serum extract were quite differ- P � 0.01).

Periyasamy et al: Uremic sera and diastolic dysfunction 2371
Table 2. Effect of uremic serum on contraction and calciummetabolism of isolated myocytes
Control Uremic UremicMeasurement (10%) (4%) (10%)
Contractile functionFractional shortening pre % 11.6 �1.9 7.4�1.2 8.5�0.5Fractional shortening post % 10.8 �2.4 17.2�2.5b,c 14.7�0.5a
Time to peak (Edge)pre msec 165 �8 160�7 189�6
Time to peak (Edge)post msec 170 �5 180�2 214�7
� (Edge) pre msec 184 �14 161�20 174�5� (Edge) post msec 210 �20 209�24c 256�8a,b
Calcium metabolismTime to peak (Ca) pre msec 57�2 54 �4 59�1Time to peak (Ca) post msec 59�2 58 �7 59�2� (Ca) pre msec 376 �36 394�17 363�27� (Ca) post msec 381 �30 531�34a,c 537�48a,c
Data are expressed as mean � SEM.a P � 0.01 vs. pre by paired t testb P � 0.05 vs. Control, c P � 0.01 vs. Control by unpaired t test
uremic serum extract, but both uremic serum extract andouabain caused a significant prolongation of the timeconstant for the recovery phase of the caffeine transientcompared with controls (N 10; 8.4 � 1.2 and 6.4 �
Fig. 2. Relationships between the concentration of ouabain (A) and 0.8 vs. 3.7 � 0.2 seconds, both P � 0.05). High doses ofuremic serum extract (B) and inhibition of 86Rb uptake in LLCPK-1
the uremic serum extract (10%) or 1 mmol/L ouabain(�) and NRK (�) cells.caused rapid and marked elevations in cytosolic calciumand irreversible contracture of the cell (both N 3). Avery low dose of uremic extract (0.5%) did not signifi-
Effect of uremic serum extracts on contraction, cantly alter cardiac contractile function or calcium cy-relaxation and the calcium transient cling to a significant degree (N 3).
The effects of deproteinized uremic serum extractEffects of Fab fragment of digitalis antibody onwere compared with those of control serum extract anduremic serum extract effects100 �mol/L ouabain. A representative experiment show-
ing the effects of uremic serum extract on myocyte con- In these studies, deproteinated extract samples pooledtraction and indo-1 fluorescence is shown in Figures 3 from four of our five uremic patients were mixed withand 4. Deproteinized uremic—but not control—serum a commercially-available Fab fragment of antibody toextracts caused increases in fractional shortening, dia- digoxin (Digibind; Jackson ImmunoResearch Labora-stolic and systolic calcium as well as prolongation of the tories, Inc., West Grove, PA, USA) for 30 minutes attime constant for relengthening and calcium transient 37�C and then added to the reaction media or studyrecovery in a similar fashion to 100 �mol/L ouabain
media for isolated enzyme, rubidium uptake (of LLC-(Table 3).PK1 cells) or isolated myocytes. Digoxin antibody frag-To examine the mechanism behind the prolongationment was added in a ratio of 1 or 10 �L (1.3 or 13 �g)of the calcium transient, cells were pretreated with eitherto 50 �L of uremic extract. We observed that the loweruremic serum extract (3.75%, N 14) or ouabain (100dose of the Fab fragment had no effect whereas the�mol/L, N 14) for five minutes prior to the generationhigher dose markedly attenuated the effects of the serumof a caffeine transient produced by the bolus administra-extract on inhibiting the sodium pump activity in vitrotion of 10 mmol/L caffeine. Caffeine causes the sarco-(Table 4). Moreover, the Fab fragment blocked the inhi-plasmic reticulum to release calcium and prevents thebition of uremic serum extract (10%) on LLC-PK1 86Rb�reuptake of calcium via the sarcoplasmic reticulum cal-uptake in a dose dependent fashion as shown in Figurecium ATPase. In this setting, the time constant for the5. Finally, the addition of 10 �L of Fab fragment (torecovery of cytosolic calcium is mostly dependent onneutralize 35 �L of extract) blocked essentially all of theplasmalemmal sodium calcium exchange [12]. The mag-observed effects of 3.5% uremic extract on myocardialnitude of the caffeine transient was not significantly dif-
ferent following the administration of either ouabain or contraction, relaxation and calcium cycling (Fig. 6).

Periyasamy et al: Uremic sera and diastolic dysfunction2372
Fig. 3. Representative responses of cellularcontraction and Indo-1 fluorescence to addi-tion of uremic extract 1.5%. Effects of calibra-tion with ionomycin and EGTA also areshown.
Fig. 4. Representative cell length (A) and cy-tosolic calcium (B) measurements obtainedfrom cardiac myocytes exposed to deprotei-nized normal and uremic serum extracts(3.75%) during field stimulation at 0.5 Hz.

Periyasamy et al: Uremic sera and diastolic dysfunction 2373
Table 3. Effect of uremic serum extract on contraction and calcium metabolism of isolated myocytes
Control Uremic Uremic OuabainMeasurement (3.75%) (1.5%) (3.75%) 100 �mol/L
Contractile functionFractional shortening pre % 8.2�1.4 10.0�2.2 9.9�1.2 8.7�2.2Fractional shortening post % 8.8�2.0 14.2�1.2bc 13.2 �1.5a 14.0�1.8bc
Time to peak (Edge) pre msec 177�10 170�12 162�6 165�15Time to peak (Edge) post msec 182�9 192�15 183�12 175�7� (Edge) pre msec 162�12 154�18 161�8 179�21� (Edge) post msec 171�10 235�25b 266 �8bd 296�17bd
Calcium metabolismDiastolic [Ca] pre nmol/L 66�7 58�7 49�10 58�19Diastolic [Ca] post nmol/L 72�6 99�16b 112 �14bc 109�29b
Systolic [Ca] pre nmol/L 189�15 198�16 209�18 233�16Systolic [Ca] post nmol/L 192�14 247�30b 254 �22ac 274�51a
Time to peak (Ca) pre msec 62�5 60�4 62�7 58�6Time to peak (Ca) post msec 69�5 58�7 69�5 59�4� (Ca) pre msec 382�22 394�17 382�16 361�24� (Ca) post msec 391�17 531�34bd 567 �27bd 472�12bd
Data expressed as mean � SEM. Based on the extraction procedure, 100 �L of serum yields approximately 30 �L of extract.a P � 0.05 vs. pre, b P � 0.01 vs. pre by paired t test.cP � 0.05 vs. Control, d P � 0.01 vs. Control by unpaired t test
Table 4. Effect of Digibind on isolated Na,K-ATPase activity sodium pump activity as assessed by isolated enzymeactivity and cardiac myocyte ouabain-sensitive rubidiumNa,K-ATPase activity
Experimental group % control uptake; however, the uremic samples caused substan-Extract (50 �L alone, N4) 47.5�3.1b tially greater degrees of sodium pump inhibition thanAb (1 �L alone, N3) 98.0�1.0 the control samples. The observation that uremic seraAb (10 �L alone N 4) 88.3�0.9b
inhibited purified enzyme isolated from dog kidney con-Ab (1 �L)� 50 �L extract (N3) 47.7�1.3b
Ab (10 �L) � 50 �L extract (N4) 68.0�2.1ab firms previous work [23, 24]. However, it was somewhatData expressed as mean � SEM. surprising to see such an excellent correlation betweena P � 0.01 vs. extract alone inhibition of isolated enzyme and rat myocyte ouabain-b P � 0.01 vs. Control by unpaired t test
sensitive rubidium uptake, as there is substantial differ-ence between species in the sensitivity of the predomi-nant isoform to cardiac glycosides [25, 26]. The isolated
DISCUSSION enzyme used in our studies was derived from dog kidney,which is predominantly alpha 1 isoform and has muchAlthough the term “uremic cardiomyopathy” has beengreater ouabain sensitivity than the Na,K-ATPase pres-used for many years, our concept of the clinical featuresent in rat cardiac myocytes [27]. This strong correlationhas changed dramatically [14]. Foley et al have demon-between isolated enzyme (dog kidney) inhibition andstrated that, while systolic dysfunction is demonstrablerubidium uptake (rat cardiomyocyte) that we observedin the minority of chronic renal failure patients [15],argues that the circulating sodium pump inhibitor pres-hospitalization for fluid overload or congestive heart fail-ent in uremic patients cannot be ouabain. This point alsoure is a common occurrence [16]. Recent work suggestsis supported by the effects of the deproteinized extractsthat echocardiographically demonstrable diastolic dys-of the uremic serum on the rubidium uptake of LLC-function is extremely common in ESRD patients treatedPK1 and NRK cells; the similar degrees of inhibition ofwith hemodialysis [17]. This is certainly a potential mech-uremic serum on both cell types contrast dramaticallyanism for why admissions for congestive heart failurewith the marked difference in the sensitivity of ouabainare so common in this patient population [18]. As severaldemonstrated by these cell lines.studies have demonstrated that acute inhibition of the
Examining the effects on isolated myocyte contractilesodium pump with digitalis glycosides can cause diastolicfunction and calcium cycling, the uremic sera (4% anddysfunction in the in vitro preparations and in vivo ani-10%) had very similar effects to that of a significantmals and human subjects [19–22], we sought to examineamount of ouabain (for example, 100 �mol/L), whereaswhether uremic serum might cause diastolic dysfunctionthe normal samples (10%) did not alter any measure-as well as establish whether this occurred through alter-ment performed. Deproteinization of the serum samplesations in calcium metabolism.did not alter the observed effects of either the uremic orOur study found that serum samples from both uremic
patients and age- and sex-matched controls inhibited control serum on contractile function or calcium cycling;

Periyasamy et al: Uremic sera and diastolic dysfunction2374
Fig. 5. Effect of Fab fragment directedagainst digitalis (D) on the uremic extractpooled from 4 of the 5 patients (UE, 10%)inhibition of 86Rb uptake in LLCPK-1 cells.Each data point was derived from N 3 ex-periments. D is Fab fragment alone (10, 20and 40 �L data pooled). Final reaction volumewas approximately 1 mL. *P � 0.05 and **P �0.01 vs. UE alone. D alone not compared withUE alone.
Fig. 6. Effect of Fab fragment (D) on uremicextract (UE 3.5%) effects on myocyte contrac-tion, relaxation and calcium cycling. Data arepresented as percent change from baselineafter 5 minutes following addition of UE aloneor UE mixed with D. Each data point wasobtained from N 4 replicants. Symbols are:(�) fractional shortening; ( ) diastolic [Ca];( ) systolic [Ca]; ( ) � edge; ( ) � calcium.*P � 0.05 and **P � 0.01 vs UE alone.
moreover, since actual cytosolic calcium quantification response relationship with respect to contractile functioncannot be seen with either the original serum samplescould be made with the addition of the uremic extracts
(but not the original serum samples), the similarity to or the protein free extracts at the doses that we reported,we feel this is probably a reflection of the variabilityouabain was even more apparent. Specifically, the ure-
mic serum extracts (1.5% and 3.75%) caused significant inherent in this measurement. It should be stressed thathigh doses of the uremic extracts caused irreversibleincreases in diastolic and systolic [Ca2�]i, fractional short-
ening, as well as the � values for relengthening and cal- contracture of myocytes in a similar fashion to that whichwe’ve seen with very high doses of ouabain (for example,cium recovery, whereas control extracts (3.75%) did not
alter any of these measurements. These findings with the 1 mmol/L; data not shown). We note that although someof these uremic patients received antihypertensive medi-uremic extracts were, again, very similar to significant
doses of ouabain (100 �mol/L). Although a clear dose cations that conceivably could alter calcium metabolism,

Periyasamy et al: Uremic sera and diastolic dysfunction 2375
the combination of an increase in � values (both relax- We did not measure these substances in these serumsamples, but when commercially available antibodies toation and calcium recovery) and an increase in contractil-
ity as assessed by fractional shortening and systolic and these substances become more available, it should berelatively simple to examine which (if any) of these sub-diastolic [Ca2�]i cannot be ascribed to any of these agents
[28–31]. Finally, the role of sodium pump inhibition from stances are responsible for the alterations in contractilefunction and calcium metabolism that we observed.the uremic serum samples in the physiological effects of
these samples is further supported by the data obtained In summary, we observed that serum samples obtainedfrom patients with chronic renal failure treated with he-studying the caffeine transient as well as data obtained
with the addition of a Fab fragment directed against modialysis contained a substance(s) that inhibited Na,K-ATPase in vitro, and acutely caused alterations in myo-digitalis. In short, it appears that the uremic serum con-
tains a substance(s) that inhibits the sodium pump with cyte relaxation and calcium metabolism. We suggest thatthe diastolic dysfunction of chronic renal failure may bevery different isoform selectivity than is displayed by
ouabain, but alters cardiac calcium cycling and physio- caused, at least in part, by this (these) substance(s).logical function in a virtually identical manner.
Although our data as well as those of others clearly ACKNOWLEDGMENTSdemonstrate that acute sodium pump inhibition impairs Portions of this study were supported by the American Heart Asso-
ciation (National and Northwest Ohio Affiliate) and the National Insti-cardiac myocyte relaxation, the mechanism by whichtutes of Health (HL57144). Some of these data were presented inthis occurs has not been definitively established. Oneabstract form at the 1999 and 2000 American Society of Nephrology
mechanism that has been promoted is that inhibition of meetings. The authors thank Ms. Carol Woods for her excellent secre-tarial assistance.the sodium pump leads to increases in cytosolic sodium,
which in turn impair calcium extrusion via sodium cal-Reprint requests to Joseph I. Shapiro, M.D., Department of Medicine,
cium exchange. We observed that the caffeine transient Medical College of Ohio, 3120 Glendale Avenue, Toledo, Ohio 43614-5089, USA.was, in fact, prolonged with ouabain as well as uremicE-mail: [email protected] extracts; this is, of course, consistent with impaired
Na/Ca exchange causing or at least contributing to theREFERENCESdelayed myocyte relaxation induced by uremic sera [8].
Although this mechanism is appealing, studies of cy- 1. Causes of death: USRDS. United States Renal Data System. AmJ Kidney Dis 30(Suppl):S107–S117, 1997tosolic sodium concentration with the sodium sensi-
2. Parfrey PS, Harnett JD, Barre PE: The natural history of myo-tive fluorescence dye, SBFI have failed to demonstrate cardial disease in dialysis patients. J Am Soc Nephrol 2:2–12, 1991
3. Amann K, Ritz E: Cardiac disease in chronic uremia: Pathophysi-marked increases in cytosolic sodium unless very highology. Adv Ren Replace Ther 4:212–224, 1997doses of ouabain (for example, 500 �mol/L) are used
4. Stokes GS, Norris LA, Marwood JF, et al: Effect of dialysis on[32]. Blaustein proposed that changes in cellular sodium circulating Na,K ATPase inhibitor in uremic patients. Nephronconcentration limited to specific compartments could re- 54:127–133, 1990
5. Kariya K, Sano H, Yamanishi J, et al: A circulating Na�-sult in significant alterations in Na/Ca exchange andK�ATPase inhibitor, erythrocyte sodium transport and hyperten-cause significant increases in [Ca2�]i [33, 34]. Alterna- sion in patients with chronic renal failure. Clin Exp Hypertens
tively, signal transduction pathways induced by sodium 8:167–183, 19866. Bosch RJ, Hernando N, Casado S, Lopez-Novoa JM: Endoge-pump inhibition, which have recently described, also
nous digoxin-like immunoreactivity and erythrocyte sodium trans-could alter Na/Ca exchange and cardiac relaxation port in uraemic patients undergoing dialysis. Clin Sci 76:157–163,[35, 36]. Certainly, additional studies must be pursued 1989
7. Bricker NS, Bourgoignie JJ, Klahr S: A humoral inhibitor ofto resolve this important issue.sodium transport in uremic serum. A potential toxin? Arch InternThere are several candidates for the sodium pump Med 126:860–864, 1970
inhibitory substance(s) that is (are) present in the uremic 8. Bassani JW, Bassani RA, Bers DM: Relaxation in rabbit and ratcardiac cells: Species-dependent differences in cellular mecha-sera. While ouabain itself has been found in uremic sera,nisms. J Physiol 476:279–293, 1994the concentrations of ouabain found cannot account for 9. Bassani RA, Bassani JW, Bers DM: Relaxation in ferret ventricu-
the degree of sodium pump inhibition observed [37]. lar myocytes: Unusual interplay among calcium transport systems.J Physiol 476:295–308, 1994Marinobufagenin has been postulated to play an impor-
10. Askari A, Huang W, Antieau JM: Na�,K�-ATPase: Ligand-tant role in sodium pump inhibition caused by seruminduced conformational transitions and alterations in subunit inter-
or plasma isolated from patients with extracellular fluid actions evidenced by cross-linking studies. Biochem 19:1132–1140,1980volume expansion. The very low Ki of this substance for
11. Xie ZJ, Wang YH, Askari A, et al: Studies on the specificity ofthe predominant, alpha 1 isoform of the sodium pumpthe effects of oxygen metabolites on cardiac sodium pump. J Mol
present in adult rat cardiac myocytes makes it a potential Cell Cardiol 22:911–920, 199012. Bers DM, Bassani JW, Bassani RA: Na-Ca exchange and Caviable candidate [38]. Hypertension associated protein
fluxes during contraction and relaxation in mammalian ventricularmay be itself or may be associated with a small molecularmuscle. Ann NY Acad Sci 779:430–442, 1996
weight sodium pump inhibitor. This substance also is 13. Wallerstein S, Zucker CI, Fleiss JL: Some statistical methodsuseful in circulation research. Circ Res 47:1–9, 1980increased in patients with chronic renal failure [39, 37].

Periyasamy et al: Uremic sera and diastolic dysfunction2376
14. Venkatesan J, Henrich WL: Cardiac disease in chronic uremia: the properties of native and recombinant Na�/K�-ATPases. ArchBiochem Biophys 330:153–162, 1996management. Adv Ren Replace Ther 4:249–266, 1997
28. Xu YJ, Shao Q, Dhalla NS: Fura-2 fluorescent technique for15. Foley RN, Parfrey PS, Harnett JD, et al: The prognostic impor-the assessment of Ca2� homeostasis in cardiomyocytes. Mol Celltance of left ventricular geometry in uremic cardiomyopathy. J AmBiochem 172:149–157, 1997Soc Nephrol 5:2024–2031, 1995
29. Santi CM, Conner JA, Hernandez-Cruz A: A significant fraction16. Hospitalization: USRDS. United States Renal Data System. Amof calcium transients in intact guinea pig ventricular myocytes isJ Kidney Dis 30(Suppl):S145–S159, 1997mediated by Na(�)-Ca2� exchange. Cell Signal 7:803–820, 199517. Facchin L, Vescovo G, Levedianos G: et al: Left ventricular mor-
30. Yu JZ, Quamme GA, McNeill JH: Altered [Ca2�]i mobilizationphology and diastolic function in uraemia: Echocardiographic evi-in diabetic cardiomyocytes: Responses to caffeine, KCl, ouabain,dence of a specific cardiomyopathy. Br. Heart J 74:174–179, 1995and ATP. Diabetes Res Clin Pract 30:9–20, 199518. Kramer W, Wizemann V, Lammlein G, et al: Cardiac dysfunction
31. Auld AM, Aspinall J, Barritt GJ: Effects of verapamil, dibutyrylin patients on maintenance hemodialysis. II. Systolic and diastolic cyclic AMP, and extracellular calcium on intracellular free calciumproperties of the left ventricle assessed by invasive methods. Con- concentrations in myocytes isolated from rat ventricles. Cardiovasctrib Nephrol 52:110–124, 1986 Res 21:772–778, 1987
19. Bolognesi R, Cucchini F, Javernaro A, et al: Effects of acute 32. Borin ML, Goldman WF, Blaustein MP: Intracellular free Na�
K-strophantidin administration on left ventricular relaxation and in resting and activated A7r5 vascular smooth muscle cells. Am Jfilling phase in coronary artery disease. Am J Cardiol 69:169–172, Physiol 264:C1513–C1524, 19931992 33. Blaustein MP: Endogenous ouabain: physiological activity and
20. Bolognesi R, Manca C, Visioli O: Effects of digitalis on the pathophysiological implications. Clin Invest 72:706–707, 1994diastolic phase of the normal heart. Angiographic evaluation in 34. Blaustein MP: Physiological effects of endogenous ouabain: Con-man. Cardiologia 33:589–593, 1988 trol of intracellular Ca2� stores and cell responsiveness. Am J
21. Lorell BH, Isoyama S, Grice WN, et al: Effects of ouabain and Physiol 264:C1367–C1387, 199335. Haas M, Askari A, Xie Z: Involvement of src and epidermalisoproterenol on left ventricular diastolic function during low-flow
growth factor receptor in the signal-transducing function of Na�/ischemia in isolated, blood-perfused rabbit hearts. Circ Res 63:457–K�-ATPase. J Biol Chem 275:27832–27837, 2000467, 1988
36. Liu J, Tian J, Haas M, et al: Ouabain interaction with cardiac22. Little WC, Rassi A Jr, Freeman GL: Comparison of effects ofNa�/K�-ATPase initiates signal cascades independent of changesdobutamine and ouabain on left ventricular contraction and relax-in intracellular Na� and Ca2� concentrations. J Biol Chem 275:ation in closed-chest dogs. J Clin Invest 80:613–620, 198727838–27844, 200023. Calderaro V, Steffanini R, Matera MG, et al: Physiological
37. Gonick HC, Ding Y, Vaziri ND, et al: Simultaneous measurementand pharmacological properties of an endogenous sodium pumpof marinobufagenin, ouabain, and hypertension-associated proteininhibitor. Life Sci 61:1457–1468, 1997 in various disease states. Clin Exp Hypertens 20:617–627, 1998
24. Kolbel F, Schreiber V: The endogenous digitalis-like factor. Mol 38. Fedorova OV, Bagrov AY: Inhibition of Na/K ATPase from ratCell Biochem 160–161:111–115, 1996 aorta by two Na/K pump inhibitors, ouabain and marinobufagenin:
25. Lingrel JB: Na,K-ATPase: Isoform structure, function, and ex- Evidence of interaction with different alpha-subunit isoforms. Ampression. J Bioenerg Biomembr 24:263–270, 1992 J Hypertens 10:929–935, 1997
26. Sweader KJ: Isozymes of the Na� K� ATPase. Bioch Biophys 39. Weiler EW, Khalil-Manesh F, Gonick HC, et al: Na-K-ATPaseActa 998:185–220, 1989 inhibitor dissociated from hypertension-associated plasma protein.
Am J Hypertens 12:364–373, 199927. Xie Z, Wang Y, Liu G, et al: Similarities and differences between