Embed Size (px)
Citation preview

Effects of the Support Surface Condition
on Muscle Activity of Abdominalis
and Erector Spinae During
Bridging Exercise
Youngju Hong
The Graduate School
Yonsei University
Department of Rehabilitation Therapy

Effects of the Support Surface Condition
on Muscle Activity of Abdominalis
and Erector Spinae During
Bridging Exercise
Youngju Hong
The Graduate School
Yonsei University
Department of Rehabilitation Therapy

Effects of the Support Surface Condition
on Muscle Activity of Abdominalis
and Erector Spinae During
Bridging Exercise
A Masters Thesis
Submitted to the Department of Rehabilitation Therapy
and the Graduate School of Yonsei University
in partial fulfillment of the
requirements for the degree of
Master of Science
Youngju Hong
June 2009

This certifies that the master’s thesis of Youngju Hong
is approved.
Thesis Supervisor: Ohyun Kwon
Chunghwi Yi
Hyeseon Jeon
The Graduate School
Yonsei University
June 2009

Acknowledgements
As I finish my work on the thesis, memories from the graduate school days rush
back to me with swelling joy in the heart and many dear faces. First of all, I would
like to dedicate my accomplishment to the glory of God, who always guided me to
a right path, leading me to this point.
I extend my deepest gratitude to Professor Ohyun Kwon who expanded my
perspectives on the world and became my beacon even though I lacked so many
abilities and caused concern. My sincere gratitude also goes to Professor Chung-
hwi Yi who embraced me with wonderful kindness even when I made mistakes. I
would like to thank Professor Hyeseon Jeon for giving me encouragement and love
with her warm smile and heart. I also thank Professor Sanghyun Cho for giving me
clear guidelines in study and Professor Seunghyun Yoo for awakening spirit of
academic exploration in me.
I am much indebted to Jonghyuck Weon for taking care of me during my
graduate school years, as well as to Taeho Kim, Heonseock Cynn and KEMA
members.
My appreciation goes to Jaeseop Oh, Wonhwee Lee, Sungmin Ha, Sujeong Kim
and Kyuenam Park, all of whom are on the same path with me. I would also like to
thank Minhee Kim who is even more attentive than me in taking care of my work,

and to Jungran Kim for her generous advice and encouragement, and to Sujin
Hwang.
I bow my head deeply to show my appreciation to Father Hakgeun Lee who
became my spiritual support, gave me lessons of life, and enriched my life while I
worked at the KEMA center. Also, my gratitude goes to Yeonggil Jung, godmother,
sisters at nunnery, Professor Myoungbok Kim, Hyunsoon Cynn and other families
of the KEMA center.
Love that I receive from my greatest supporters, grandparents and parents,
nourishes my life. It becomes a solid ground when I go through difficult moments,
and I respect and love them for helping me to take root more strongly. I am also
thankful to sister Jeongwon who is my family and friend that extends helping hands
to me without hesitation, to my aunts and niece Doyun, my valuable friends whom
I can laugh with freely even when work is hectic and stressful, and the juniors at
the school who helped me greatly with experiments.
I will always remember my blessing and try to live up to the trust people have
shown in me. Thank you.

i
Table of Contents
List of Figures ·························································································· ⅱ
List of Tables ···························································································· iii
Abstract ···································································································· iv
Introduction ······························································································· 1
Method ······································································································ 5
1. Subjects ····························································································· 5
2. Experimental Equipments ·································································· 6
2.1 Electromyography System ··························································· 6
2.2 Apparatus of the Support Surface Conditions ······························· 8
3. Experimental Procedures ··································································· 9
3.1 Bridging Exercise ······································································· 10
3.2 Unilateral Bridging Exercise ······················································· 10
4. Statistical Analysis ··········································································· 13
Results ····································································································· 14
Discussion ································································································ 23
Conclusion ······························································································· 28
References ······························································································· 29
Abstract in Korean ··················································································· 35

ii
List of Figures
Figure 1. Surface conditions ········································································ 8
Figure 2. Bridging exercise under the three different support surface
conditions ··················································································· 11
Figure 3. Unilateral bridging exercise under the three different support
surface conditions ······································································· 12
Figure 4. EMG activities during the bridging exercise using three
different support surfaces ···························································· 17
Figure 5. EMG activities during the unilateral bridging exercise
using three different support surfaces ··········································· 19

iii
List of Tables
Table 1. Descriptive data for participants in this study ······························· 5
Table 2. Comparison of EMG activities according to the support
surface conditions during the bridging exercise ··························· 16
Table 3. Comparison of EMG activities according to the support
surface conditions during the unilateral bridging exercise ············ 18
Table 4. Comparison of EMG activities between the bridging exercise
and unilateral bridging exercise ··················································· 20
Table 5. Comparison of EMG activities between the right and left
sides during the bridging exercise ··············································· 21
Table 6. Comparison of EMG activities between the right and left
sides during the unilateral bridging exercise ······························ 22
iv
ABSTRACT
Effects of the Support Surface Condition
on Muscle Activity of Abdominalis and
Erector Spinae During Bridging Exercise
Youngju Hong
Dept. of Rehabilitation Therapy
(Physical Therapy Major)
The Graduate School
Yonsei University
Various exercise protocols have been designed to improve trunk stability in the
fields of rehabilitation and sport. Bridging exercise on the floor, foam roll, or gymball
is often prescribed for improving trunk stability.
The aim of this study was to determine the muscle activity of the abdominalis and
erector spinae during bridging and unilateral bridging exercises on a firm surface, on
the sit-fit, and on a foam roll. Eighteen healthy young subjects with no medical

v
history of lower-extremity or lumbar spine disease were recruited for this study.
Muscle activity was recorded using surface EMG electrods from the both sides of the
rectus abdominalis, external obliques, internal obliques, and erector spinae muscles
during bridging and unilateral bridging exercises. A one-way repeated analysis of
variance was used to compare the EMG activity of each muscle according to the
support surface condition. Differences in the EMG activities between the bridging
and unilateral bridging exercises, and between the right side and left side were
assessed using a paired t-test, and the level of statistical significance was set at 0.05.
The study showed that the EMG activities of the both rectus abdominalis, both
external obliques, and the right internal oblique were significantly higher when the
bridging exercise was performed using the foam roll than when using the sit-fit. The
EMG activities of the both external obliques, both internal obliques, and both erector
spinae during bridging exercise using the foam roll were significantly higher than that
using the firm surface. The EMG activities of the left rectus abdominis, both external
obliques, and the right internal oblique were significantly higher during unilateral
bridging exercise using the foam roll than when using the sit-fit. The EMG activities
of the right external oblique, right internal oblique, and both erector spinae during
unilateral bridging exercise using the foam roll were significantly higher than when
using the firm surface. The EMG activity of the left erector spina was significantly
higher when using the sit-fit than when using the firm surface during the unilateral
bridging exercise. The EMG activities of all of the muscles were significantly higher
during the unilateral bridging exercise than during the bridging exercise. There was

vi
no significant difference in the EMG activity of each muscle between the right side
and the left side during the bridging exercise. In the unilateral bridging exercise, the
EMG activity of the right rectus abdominis was significantly higher than that of the
left rectus abdominis in all three support surface conditions. In addition, the EMG
activity of the right erector spina was significantly higher than that of the left erector
spina when performing the unilateral bridging exercise using the firm surface and the
sit-fit.
Based on these fidings, performing the unilateral bridging exercise using the sit-fit
or the foam roll is a useful method for facilitating trunk-muscle strength and hence
lumbar stability.
Keywords: Abdominal muscles, Bridging exercise, Electromyography, Erector
spinae, Trunk stabilization exercise, Unstable support surface.

- 1 -
Introduction
Low back pain (LBP) is common, with 60% - 90% of the adult population being at
risk of developing LBP at some point in their lifetime (Smeal et al. 2004). Of those
who develop acute LBP, 30% develop chronic LBP (Khadilkar et al. 2005), which
has a significant impact on functional status and occupational activities, and marked
socioeconomic repercussions (Hagen et al. 2000; Philadelphia Panel 2001; Strand,
Moe-Nilssen, and Ljunggren 2002). Chronic LBP is the most frequent cause of
workers’ compensation claims and a major reason for visits to healthcare
professionals (Philadelphia Panel 2001).
The trunk muscles provide core stability to the trunk, which allows the trunk to
maintain a static posture even under the influence of destabilizing external torques
(Akuthota and Nadler 2004). LBP is caused by instability of the lumbar segment with
weakness of the trunk stabilizer muscles, and a lack of back muscle endurance (Hall
and Brody 2005; Neumann 2002). Poor coordination of the muscle corset around the
lumbar spine may also contribute to LBP (Andersson et al. 1997; Cholewicki and
VanVliet 2002).
Panjabi (1992) introduced an innovative model of a spinal stabilization system.
Spine stability is dependent on three subsystems: passive (spinal column), active
(spinal muscles), and control (neural control). Lumbar spine stability can be achieved
via coordinated force feedback from both the active and the passive structures, with

- 2 -
appropriate levels of activation to the contracting muscles in order to balance any
destabilizing force (Kavcic, Grenier, and McGill 2004). It is therefore essential that
stability is precisely controlled by lumbar and abdominal muscles to produce the
stiffness required to optimize the loading on the lumbar spine, and to prevent
overload injury (Arokoski et al. 2004).
Lumbar stability is increased with abdominal and paraspinal muscle coactivation,
which increases intra-abdominal pressure and produces an abdominal spring force
(McGillet et al. 2003). The abdominal muscles serve as a vital component of the core.
The internal oblique (IO) has a similar fiber orientation to the transverse abdominis,
thus increasing the intra-abdominal pressure together with the transverse abdominis.
Thus, the IO imparts functional stability to the lumbar spine (McGill 2002). The
external oblique (EO), the largest and most superficial of the abdominal muscles, acts
as an evaluator of anterior pelvic tilt. It is recruited to enhance spine stability,
generating lateral bending and twist torque of the trunk (Pool-Goudzwaard et al.
1998). The rectus abdominis (RA) is a paired, strap-like muscle of the anterior
abdominal wall contraction of which predominantly causes flexion of the lumbar
spine. The erector spinae (ESs) in the lumbar region act on the lumbar spine via a
long tendon that is attached to the pelvis. Contraction of the ESs extends the trunk, a
movement that is controlled largely by the opposing activity of the RA muscles. The
role of the multisegmental back muscle is to provide general trunk stabilization and to
balance external loads, thereby helping to minimize the forces acting on the spine
(Ebenbichler et al. 2001). The function and coordination of the muscles that stabilize

- 3 -
the lumbar spine are often impaired in patients with LBP (Cholewicki and VanVlient
2002).
During the past decade, many physical therapy rehabilitation interventions have
been used in the management of LBP (Khadilkar et al. 2005). Exercises are effective
in decreasing the intensity of LBP and the associated functional disability, and in
improving back extension strength, mobility, and endurance (Vezina and Hubley-
Kizey 2000). Recently the focus of lumbar stabilization exercises has been on
protecting the spinal joint structure from further repetitive microtrauma and restoring
dynamic stability to the trunk (Stevens et al. 2006). The lumbar stabilization exercises
include the so-called dying bug, quadruped, pelvic tilt, abdominal hollowing, and
bridging exercises (Barnett and Gilleard 2005; Hubley-Kozey and Vezina 2002). The
bridging exercise is commonly used for improving lumbopelvic stabilization. It is a
comfortable and typically painless posture for improving the coordination of the trunk
muscles (Hyde and Gengenbach 2007; Lehman, Hoda, and Oliver 2005; Stevens et al.
2006). The use of unstable support surfaces increases muscle activity and coactivation
for trunk and lumbar stability (Vera-Garcia, Grenier, and McGill 2000). Unstable
support surfaces such as gym balls, rollers, wobble boards, slings, and disks are often
used for stability exercises (Akuthota and Nadler 2004). According to a study by
Marshall and Murphy (2005), performing tasks on a Swiss ball leads to the abdominal
and spinal muscle activities being higher than those on a stable surface (Vera-Garcia,
Grenier, and McGill 2000). However, the Swiss ball has been the only type of
unstable surface examined in previous studies. Trunk and ESs EMG activities were

- 4 -
recently investigated during bridging stabilization exercises, ball bridging exercises,
and bridging exercises with leg movements (Stevens et al. 2006). However, the EMG
activities of the abdominal muscles and ESs during bridging and unilateral bridging
exercises under different support surface conditions were not analyzed. Therefore, in
the present study determined the effects of three different surface conditions (firm
surface, sit-fit, and foam roll) on abdominal muscles and ESs EMG activities during
bridging and unilateral bridging exercises.

- 5 -
Method
1. Subjects
A cohort of eighteen healthy young subjects (9men and 9women) without
neurological, musculoskeletal, or cardiopulmonary diseases, or back or lower-limb
pathology were recruited from the Department of Physical Therapy, Yonsei
University, Korea (Table 1). The subjects were assessed for their ability to perform
the bridging exercise and unilateral bridging exercise without pain. Prior to the study,
the principal investigator explained all of the procedures to the subjects in detail, and
obtained their written informed consent to participate.
Table 1. Descriptive data for participants in this study. (N=18)
Parameter Mean ± SD Range
Age (years) 23.17 ± 2.09 21~26
Body mass (㎏) 61.33 ± 9.89 46~81
Height (㎝) 170.56 ± 9.19 156~190
- 6 -
2. Experimental Equipments
2.1 Electromyography System
EMG data were collected using a Noraxon TeleMyo 2400 system (Noraxon Inc.,
Scottsdale, AZ, USA.) and analyzed using MyoResearch Master Edition 1.06 XP
software (Noraxon Inc., Scottsdale, AZ, USA). The skin was prepared by shaving the
hair and then rubbing it with sandpaper and an alcohol/water solution to decrease the
skin impedance. Surface electrode pairs and the adhesive skin interfaces were
separated by 2 cm. The reference electrode was attached to the right anterior superior
iliac spine (ASIS). The eight electrode sites on both sides were as follows: the RA
(parallel to approximately 3cm lateral and superior to the umbilicus, arranged along
the longitudinal axis, over the muscle belly), IO (halfway between the ASIS of the
pelvis and the midline, just superior to the inguinal ligament), EO (halfway between
the ASIS of the pelvis and the inferior border of the rib cage at a slightly oblique
angle, running parallel to the underlying muscle fibers), and lumbar ES (parallel to
the spine, approximately 2 cm lateral to the L4 - L5 spinous process for the lumbar
ES, over the muscle belly) (Cram, Kasman, and Holtz 1998).
The raw signal was full-wave rectified and filtered using a Lancosh FIR digital
filter. The bandpass filter was set between 20 and 500 Hz and the notch filter at 60 Hz.
The sampling rate was 1000 Hz. The EMG data were processed into the root mean
square (RMS) value, which was calculated from 300-ms windows of data points. For
- 7 -
normalization of the EMG data, the mean RMS of three trials of 5-second maximal
voluntary isometric contractions (MVICs) was calculated for each muscle. The
manual muscle testing positions selected for the MVIC were those recommended by
Kendall et al. (2005). For the testing of the bridging and unilateral bridging exercises,
the EMG signal was collected for 5 seconds while the subject’s pelvis was maintained
level with the hip in a neutral position. The data for each trial are expressed as a
percentage of the MVIC (%MVIC), and the mean value of three trials was used for
analysis.

- 8 -
2.2 Apparatus of the Support Surface Conditions
The exercises were performed using three different support surfaces: firm surface,
sit-fit, and round foam roll (Figure 1). The height of the 14 cm diameter foam roll was
matched with the firm surface and sit-fit height. The subjects laid supine on the floor
with their feet flat on the experimental surface.
Figure 1. Surface conditions. A: Firm surface, B: Sit-fit, C: Foam roll.
A B C

- 9 -
3. Experimental Procedures
All subjects attended an orientation (practice) session that lasted at least 30 minutes
before testing to familiarize themselves with the bridging and unilateral bridging
exercises using the different support surface conditions. The start position of all
exercises was hook-lying with the feet flat on the support surface. The positions of
both the subject and the equipment were standardized by placing markers on the floor.
Tests were performed in a random order. The bridging position was held for five
seconds, and three trials were performed for each exercise. A 30-second rest period
was allocated between the trials, and a 3-minute rest period was allocated between the
different support surface conditions.

- 10 -
3.1 Bridging Exercise
The subjects assumed a supine position on the floor with the head, upper trunk, and
pelvis in a straight line. The knees were bent to 60° and the hands were placed onto
the chest. The feet were placed shoulder-width apart on the support surface being
tested. The subjects lifted their pelvis until the hip joint reached a neutral position
(Figure 2). At the beginning of each exercise, a neutral lumbar spine position was
determined by the examiner and the subjects were encouraged to hold this position
during the course of the exercise. Feedback from the examiner was given in order to
achieve a consistent spine and lower-limb posture during the bridging exercise.
3.2 Unilateral Bridging Exercise
This testing procedure was similar to that of the bridging exercise, except that the
right knee joint was extended during the bridging exercise position (Figure 3), and
also took place using the three different support surfaces. The target bar was placed at
the level of 0° of knee extension, and subjects were instructed to extend their knee
without hip adduction, abduction, or pelvic tilt until the tiptoe region of the right side
touched the target bar.

- 11 -
Figure 2. Bridging exercise under the three different support
surface conditions. A: Firm surface, B: Sit-fit, C: Foam roll.
A
B
C

- 12 -
Figure 3. Unilateral bridging exercise under the three different
support surface conditions. A: Firm surface, B: Sit-fit, C: Foam roll.
A
B
C

- 13 -
4. Statistical Analysis
The data are expressed as mean ± standard deviation (SD) values. Repeated one-
way analysis of variance (ANOVA) was used to compare the EMG activities of the
abdominalis and ESs according to the support surface condition. The Bonferroni’s
post-hoc test was used to determine the differences in EMG activities of the
abdominalis and ESs between the different support surface conditions. The
significance of differences in the EMG activity between the bridging and unilateral
bridging exercises, and between the right side and left side were assessed using a
paired t-test. Data analysis was performed using SPSS version 12.0 software, and the
level of statistical significance was set at 0.05.
- 14 -
Results
The EMG activities of all of the abdominalis and the ESs differed significantly
among the different support surfaces during the bridging exercise (p < 0.05) (Table 2).
Post-hoc testing revealed that the EMG activities of both RAs, both EOs, and the
right IO were significantly higher when performing the bridging exercise using the
foam roll than when using the sit-fit. The EMG activities of both EOs, both IOs, and
both ESs when performing the bridging exercise were significantly higher when using
the foam roll than when using the firm surface. None of the muscle EMG activities
when performing the bridging exercise differed significantly between using the firm
surface and the sit-fit (Figure 4).
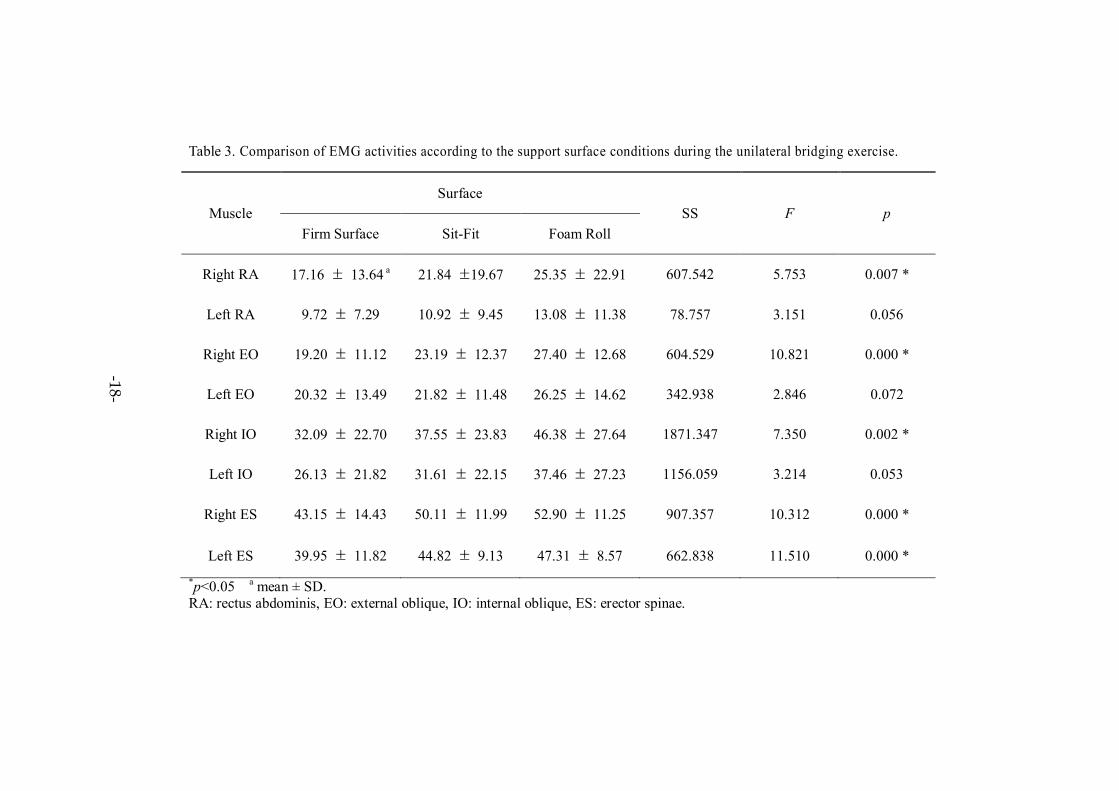
The EMG activities of the right RA, right EO, right IO, and both ESs differed
significantly among the different support surfaces during the unilateral bridging
exercise (p < 0.05) (Table 3). Post-hoc testing revealed that the EMG activities of the
left RA, both EOs, and the right IO when performing the unilateral bridging exercise
were significantly higher when using the foam roll than when using the sit-fit. The
EMG activities of the right EO, right IO, and both ESs when performing the unilateral
bridging exercise were significantly higher when using the foam roll than when using
the firm surface. The EMG activity of the left ES when performing the unilateral
bridging exercise was significantly higher when using the sit-fit than when using the
firm surface (p < 0.05) (Figure 5).
- 15 -
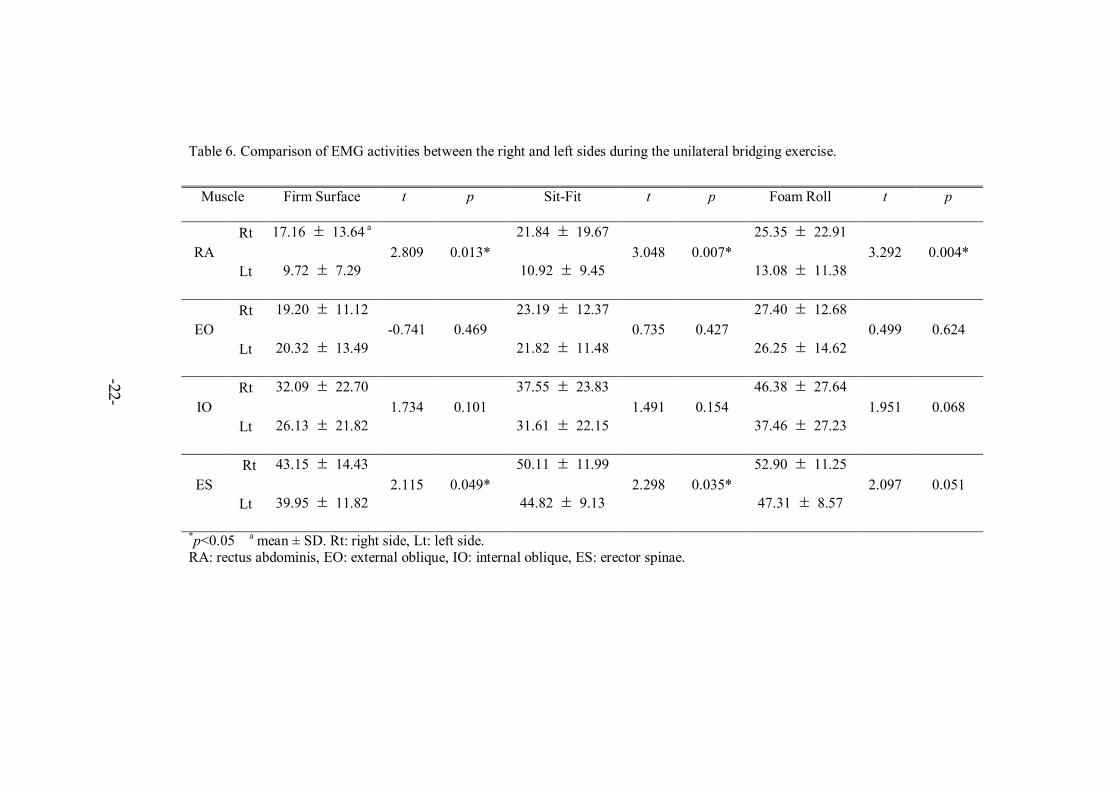
The EMG activity of each individual muscle was significantly higher during the
unilateral bridging exercise than during the bridging exercise (Table 4). There was no
significant difference in the EMG activity of each muscle between the right and the
left sides during the bridging exercise (Table 5). However, when performing the
unilateral bridging exercise the EMG activity of the right RA was significantly higher
than that of the left RA in all three support surface conditions. The EMG activity of
the right ES was also significantly higher than that of the left ES when performing the
unilateral bridging exercise using the firm surface and the sit-fit (Table 6).

16
Table 2. Comparison of EMG activities according to the support surface conditions during the bridging exercise.
*p<0.05 a mean ± SD. RA: rectus abdominis, EO: external oblique, IO: internal oblique, ES: erector spinae.
Muscle
Surface
SS F p
Firm Surface Sit-Fit Foam Roll
Right RA 4.38 ± 3.42 a 4.90 ± 4.54 6.42 ± 6.00 40.645 3.893 0.03 *
Left RA 4.30 ± 3.48 4.40 ± 3.42 6.69 ± 6.29 65.711 5.531 0.002 *
Right EO 4.96 ± 4.20 5.60 ± 3.78 8.72 ± 6.98 146.056 10.211 0.000 *
Left EO 5.60 ± 4.06 5.93 ± 3.62 9.93 ± 7.22 209.608 10.819 0.000 *
Right IO 5.03 ± 4.07 6.80 ± 6.70 11.44 ± 10.53 394.211 6.709 0.003 *
Left IO 5.91 ± 4.11 7.97 ± 6.82 13.86 ± 12.06 611.662 7.958 0.001 *
Right ES 31.02 ± 10.77 34.55 ± 8.86 35.74 ± 9.08 216.936 5.361 0.009*
Left ES 32.27 ± 10.14 35.35 ± 8.01 37.25 ± 7.76 227.154 7.660 0.002 *
-16-

17
Right RA Left RA Right EO Left EO Right IO Left IO Right ES Left ES0
10
20
30
40
50
FS SF FR
* * *
* *
*
*
* * *
*
%M
VIC
Figure 4. EMG activities during the bridging exercise using three different support surfaces. FS; firm surface, SF:
sit-fit, FR: foam roll. RA: rectus abdominis, EO: external oblique, IO: internal oblique, ES: erector spinae. *p<0.05 (mean ± SD).
-17-
18
Table 3. Comparison of EMG activities according to the support surface conditions during the unilateral bridging exercise.
*p<0.05 a mean ± SD. RA: rectus abdominis, EO: external oblique, IO: internal oblique, ES: erector spinae.
Muscle
Surface
SS F p
Firm Surface Sit-Fit Foam Roll
Right RA 17.16 ± 13.64 a 21.84 ±19.67 25.35 ± 22.91 607.542 5.753 0.007 *
Left RA 9.72 ± 7.29 10.92 ± 9.45 13.08 ± 11.38 78.757 3.151 0.056
Right EO 19.20 ± 11.12 23.19 ± 12.37 27.40 ± 12.68 604.529 10.821 0.000 *
Left EO 20.32 ± 13.49 21.82 ± 11.48 26.25 ± 14.62 342.938 2.846 0.072
Right IO 32.09 ± 22.70 37.55 ± 23.83 46.38 ± 27.64 1871.347 7.350 0.002 *
Left IO 26.13 ± 21.82 31.61 ± 22.15 37.46 ± 27.23 1156.059 3.214 0.053
Right ES 43.15 ± 14.43 50.11 ± 11.99 52.90 ± 11.25 907.357 10.312 0.000 *
Left ES 39.95 ± 11.82 44.82 ± 9.13 47.31 ± 8.57 662.838 11.510 0.000 *
-18-

19
Right RA Left RA Right EO Left EO Right IO Left IO Right ES Left ES0
5
10
15
20
25
30
35
40
45
50
55
60
65
70
75
*
*
*
*
*
*
*
* *
FS FRSF
%M
VIC
Figure 5. EMG activities during the unilateral bridging exercise using three different support surfaces. FS; firm surface,
SF: sit-fit, FR: foam roll. RA: rectus abdominis, EO: external oblique, IO: internal oblique, ES: erector spinae. *p<0.05 (mean ± SD).
-19-

20
Table 4. Comparison of EMG activities between the bridging exercise and unilateral bridging exercise.
* p<0.05 a mean ± SD. R: right, L: left.
RA: rectus abdominis, EO: external oblique, IO: internal oblique, ES: erector spinae. B: bridging exercise UB: unilateral bridging exercise.
Muscle Firm Surface t p Sit-Fit t p Foam Roll t p
RRA B
UB
4.38 ± 3.42 a
17.16 ± 13.64 -4.529 0.000*
4.90 ± 4.54
21.84 ± 19.67 -4.151 0.001*
6.42 ± 6.00
25.35 ± 22.91 -4.113 0.001*
LRA B
UB
4.30 ± 3.48
9.72 ± 7.29 -5.046 0.001*
4.40 ± 3.42
10.92 ± 9.45 -4.130 0.001*
6.69 ± 6.29
13.08 ± 11.38 -4.354 0.001*
REO B
UB
4.96 ± 4.20
19.20 ± 11.12 -6.358 0.001*
5.60 ± 3.78
23.19 ± 12.37 -6.869 0.001*
8.72 ± 6.98
27.40 ± 12.68 -7.703 0.001*
LEO B
UB
5.60 ± 4.06
20.32 ± 13.49 -5.622 0.001*
5.93 ± 3.62
21.82 ± 11.48 -6.756 0.001*
9.93 ± 7.22
26.25 ± 14.16 -5.803 0.001*
RIO B
UB
5.03 ± 4.07
32.09 ± 22.70 -5.627 0.001*
6.80 ± 6.70
37.55 ± 23.83 -6.225 0.001*
11.44 ± 10.53
46.38 ± 27.64 -6.147 0.001*
LIO B
UB
5.91 ± 4.11
26.13 ± 21.82 -4.307 0.001*
7.97 ± 6.82
31.61 ± 22.15 -4.980 0.001*
13.86 ± 12.06
37.46 ± 27.23 -4.354 0.001*
RES B
UB
31.02 ± 10.77
43.15 ± 14.43 -7.183 0.001*
34.55 ± 8.86
50.11 ± 11.99 -12.914 0.001*
35.74 ± 9.08
52.90 ± 11.25 -9.105 0.001*
LES B
UB
5.60 ± 4.06
39.95 ± 11.82 -3.602 0.002*
35.35 ± 8.01
44.82 ± 9.13 -6.266 0.001*
37.25 ± 7.76
47.31 ± 8.57 -5.099 0.001*
-20-

21
Table 5. Comparison of EMG activities between the right and left sides during the bridging exercise.
*p<0.05 a mean ± SD. Rt: right side, Lt: left side. RA: rectus abdominis, EO: external oblique, IO: internal oblique, ES: erector spinae.
Muscle Firm Surface t p Sit-Fit t p Foam Roll t p
RA
Rt 4.38 ± 3.42 a
0.160 0.875
4.90 ± 4.54
0.688 0.500
6.42 ± 6.00
-0.309 0.761
Lt 4.30 ± 3.48 4.40 ± 3.42 6.69 ± 6.29
EO
Rt 4.96 ± 4.20
-1.058 0.305
5.60 ± 3.78
-0.555 0.586
8.72 ± 6.98
-1.513 0.149
Lt 5.60 ± 4.06 5.93 ± 3.62 9.93 ± 7.22
IO
Rt 5.03 ± 4.07
-1.262 0.224
6.80 ± 6.70
-1.730 0.102
11.44 ± 10.53
-1.283 0.217
Lt 5.91 ± 4.11 7.97 ± 6.82 13.86 ± 12.06
ES
Rt 31.02 ± 10.77
-1.021 0.321
34.55 ± 8.86
-0.771 0.451
35.74 ± 9.08
-1.361 0.191
Lt 32.27 ± 10.14 35.35 ± 8.01 37.25 ± 7.76
-21-
22
Table 6. Comparison of EMG activities between the right and left sides during the unilateral bridging exercise.
*p<0.05 a mean ± SD. Rt: right side, Lt: left side. RA: rectus abdominis, EO: external oblique, IO: internal oblique, ES: erector spinae.
Muscle Firm Surface t p Sit-Fit t p Foam Roll t p
RA
Rt 17.16 ± 13.64 a
2.809 0.013*
21.84 ± 19.67
3.048 0.007*
25.35 ± 22.91
3.292 0.004*
Lt 9.72 ± 7.29 10.92 ± 9.45 13.08 ± 11.38
EO
Rt 19.20 ± 11.12
-0.741 0.469
23.19 ± 12.37
0.735 0.427
27.40 ± 12.68
0.499 0.624
Lt 20.32 ± 13.49 21.82 ± 11.48 26.25 ± 14.62
IO
Rt 32.09 ± 22.70
1.734 0.101
37.55 ± 23.83
1.491 0.154
46.38 ± 27.64
1.951 0.068
Lt 26.13 ± 21.82 31.61 ± 22.15 37.46 ± 27.23
ES
Rt 43.15 ± 14.43
2.115 0.049*
50.11 ± 11.99
2.298 0.035*
52.90 ± 11.25
2.097 0.051
Lt 39.95 ± 11.82 44.82 ± 9.13 47.31 ± 8.57
-22-
-23-
Discussion
The stability of the lumbar spine requires both the passive stiffness provided by
the osseous and ligamentous structures, and the active stiffness provided by muscles
that are under the motor control of the central nervous system (Ebenbichler et al.
2001; McGill et al. 2003). The spinal structure plays a role, but damage to the spinal
segments can be compaensated by proper muscular function and adequate neural
control, which is why exercise training is the mainstay of treatment to improve
stabilization of the spine (Barr, Griggs, and Cadby 2005). Thus, trunk stabilization
exercises are often used in the rehabilitation of individuals with LBP. Unstable
surfaces have been commonly incorporated into trunk strengthening exercise regimes
and recommended as a means of more effectively training the stability of the
musculoskeletal system (Behm et al. 2005; Lehman, Hoda, and Oliver 2005).
Numerous studies have documented increased trunk muscle activity during a variety
of trunk muscle exercises on unstable surfaces such as gym balls, rollers, wobble
boards, slings, and disks (Arokoski et al. 2001; Lehman, Hoda, and Oliver 2005; Mori
2004; Stevens et al. 2006; Vera-Garcia, Grenier, and McGill 2000).
The effects of three different support surface conditions on abdominalis and ESs
muscle activities during bridging and unilateral bridging exercises were examined in
the present study. The EMG activities of both RAs, both EOs, and the right IO when
performing the bridging exercise were significantly higher when using the foam roll
-24-
than when using the sit-fit. In addition, the EMG activities of the both EOs, and both
IOs when performing the bridging exercise using the foam roll were approximately
two times higher than when using the firm surface. The EMG activities of the
contralateral RA, both EOs, and ipsilateral IO when performing the unilateral briging
exercise were significantly higher when using the foam roll than when using the sit-fit.
Those of the ipsilateral EO, ipsilateral IO, and both ESs when performing the
unilateral bridging exercise were significantly higher when using the foam roll than
when using the firm surface. The EMG activity of the contralateral ES was
significantly higher during the same exercise when using the sit-fit than when using
the firm surface. The findings of this study thus demonstrate that when performing
the bridging and unilateral bridging exercises, the EMG activities of the abdominalis
and ESs were significantly higher when using the sit-fit and foam roll (unstable
surfaces) than when using the firm surface (stable surface). These increased
abdominalis and ESs EMG activities when using an unstable surface are in
accordance with the findings of Arokosiki et al. (2001) and Vera- Garcia, Grenier,
and McGill (2000). Vera-Garcia and his colleagues (2000) reported that the EMG
activities of both RAs, EOs, and IOs were higher when performing exercises on a
gym ball than when using a stable surface. This increased EMG activity was
attributed to the increased need for spine and whole-body stability in order to reduce
the threat of falling off the unstable surface. A more unstable support area requires
more muscle activity to maintaining balance.

-25-
In the present study, the EMG activities of all of the abdominalis when performing
bridging exercise were significantly higher when using the foam roll than when using
the sit-fit. There are several possible explanations for this finding. First, the
cylindrical shape of the foam roll provides a smaller contact area on the floor and
moves easily from side to side; therefore, more challenging balancing reactions are
required during bridging exercise when using foam roll than when using the sit-fit,
with its flat lower surface (i.e. normal to the floor) (Creager 2006). Second, the
contact area between the subject’s foot and the support surface of the foam roll is
smaller than with the sit-fit. Finally, the smaller contact area between the foot and the
foam roll may have resulted in a reduced somatosensory input, and thus a
concomitant reduction in feedback, possibly causing an increase in the EMG
activities of the abdominalis (Shumway-Cook and Woollacott 2001).
In this study, the EMG activities of the abdominalis and ESs were significantly
higher during the unilateral bridging exercise than during the bridging exercise. The
contact area between the subject’s feet and the support is smaller when performing the
unilateral bridging exercise than when performing the bridging exercise. Thus,
maintaining a neutral spine without rotation during the unilateral bridging exercise is
a more challenging task, requiring more abdominalis contraction than the bridging
exercise (Behm and Anderson 2006; Shumway-Cook and Woollacott 2001).
Instability is induced not only by unstable surfaces, but also by destabilizing torque
such as that resulting from the unbalanced movement of lifting a leg (Behm et al.

-26-
2005). Due to the instability of the unilateral bridging exercise, muscle crossing the
abdominal area needs to cocontract more to maintain the unilateral bridging exercise
without spine rotation, hip flexion, and pelvic tilt than in the bridging exercise. The
weight of the lifted leg produces torque about spine rotation, hip flexion, and pelvic
tilt. To counterbalance this rotation moment, the RA, EO, and IO muscles of the
contralateral side contract to maintain trunk stability (Pool-Goudzwaard et al. 1998).
This instability can be overcome by cocontraction of the abdominalis not by
contraction of a particular muscle. Spinal stability can be maintained during the
unilateral bridging exercise only by elevating the intra-abdominal pressure by
simultaneously contracting all of the trunk muscles (Ebenbichler et al. 2001; Hodges
and Richardson 1996; Hodges et al. 2005).
The major finding of this study was that the EMG activity of the right RA was
significantly higher than that of the left RA during the unilateral bridging exercise in
all three support surface conditions. In addition, the EMG activity of the right ES was
significantly higher than that of the left ES during the unilateral bridging exercise
using both the firm surface and the sit-fit. Both the RA and the EO muscles play a
role in stabilizing the trunk and pelvis (Mori 2004). The EOs stabilize the trunk by
preventing mediolateral rotation as a result of their attachment to the thoracolumbar
fascia. On the other hand, the RA muscles have a more longitudinal action on the
trunk, and are a better stabilizer of anteroposterior tilting of the pelvis (Neumann
2002). Performing the unilateral bridging exercise activated the right RA, and the

-27-
right ES, because the subjects were asked to maintain the static equilibrium of the
body during the unilateral bridging exercise (right knee extension).
The weight of the lifted leg causes a hip extension moment. This should be
counterbalanced by the activation of the hip flexors to maintain the neutral position of
trunk. Increased hip flexor muscle activation will cause anterior pelvic tilt of the right
side. Anterior pelvic tilt is prevented by contraction of the right RA. This may be why
the activity of the right RA was greater during the unilateral bridging exercise than
during the bridging exercise (Marshall and Murphy 2005). The activation of the right
ES may also be increased to counterbalance the activation of the right RA.
The support surface conditions influenced the activities of the abdominal muscles
and ESs during spine stabilizing exercises. The findings of this study should aid the
design of new trunk stabilization exercises.
There were some limitations to this study. First, our results cannot be generalized
to other populations because all of the subjects who participated in the study were
healthy and young. Therefore, the effects of surface condition on trunk muscles
during stabilizing exercises should be confirmed in a patient population. Second, the
activities of the deep muscles that are considered to be trunk stabilizers, such as the
transverse abdominis, multifidus, and pelvic floor muscles were not measured.

-28-
Conclusion
The effects of the support surface condition on the EMG activities of the
abdominalis and ESs during bridging and unilateral bridging exercises were
investigated. Overall, these exercises activated the abdominalis and ESs more when
they were performed using the sit-fit and foam roll (the unstable surfaces) than when
using the firm surface (the stable surface). In addition, the EMG activities of the
abdominalis and ESs were higher when performing the unilateral bridging exerise
than during the bridging exercise. The EMG activity of the right RA was significantly
higher than that of the left RA under all three support surface conditions during the
unilateral bridging exercise. The EMG activity of the right ES was significantly
higher than that of the left ES when performing the unilateral bridging exercise using
the firm surface and the sit-fit.

-29-
References
Akuthota V and Nadler SF. Core strengthening. Arch Phys Med Rehabil. 2004;85:86-
92.
Andersson EA, Nilsson J, Ma Z, and Thorstensson A. Abdominal and hip flexor
muscle activation during various training exercises. Eur J Appl Physiol Occup
Physiol. 1997;75:115-123.
Arokoski JP, Valta T, Airaksinen O, and Kankaanpaa. Back and abdominal muscle
function during stabilization exercises. Arch Phys Med Rehabil. 2001;82:1089-
1098.
Arokoski JP, Valta T, Kankaanpaa M, and Airaksinen O. Activation of lumbar
paraspinal and abdominal muscles during therapeutic exercises in chronic low
back pain patients. Arch Phys Med Rehabil. 2004;85:823-832.
Barr KP, Griggs M, and Cadby T. Lumbar stabilization: core concepts and current
literature, part 1. Am J Phys Med Rehabil. 2005;84:473-480.
Barnett F and Gilleard W. The use of lumbar spinal stabilization techniques during
the performance of abdominal strengthening exercise variations. J Sports Med
Phys Fitness. 2005;45:38-43.

-30-
Behm DG and Anderson KG. The role of instability with resistance training. J
Strength Cond Res. 2006;20:716-722.
Behm DG, Leonard AM, Young WB, Bonsey WA, and Mackinnon SN. Trunk
muscle electromyographic activity with unstable and unilateral exercises. J
Strength Cond Res. 2005;19:193-201.
Creager CC. Therapeutic Exercises using Foam Rollers.7th Ed. Berthoud, CO:
Executive Physical Therapy Inc, 2006.
Cholewicki J and VanVlient. Relative contribution of trunk muscles to the stability of
the lumbar spine during isometric exertions. Clin Biomech. 2002;17:99-105.
Cram JR, Kasman GS, and Holtz J. Introduction to Surface Electromyography.
Gaithersburg, Md: Aspen Publishers, 1998.
Ebenbichler GR, Oddsson LI, Kollmitzer J, and Erim Z. Sensory motor control of the
lower back: Implications for rehabilitation. Med Sci Sports Exerc. 2001;33:1889-
1898.
Hagen KB, Holte HH, Tambs K, and Bjerkedal T. Socioeconomic factors and
disability retirement from back pain: A 1983-1993 population-based prospective
study in Norway. Spine. 2000;25:2480-2487.
-31-
Hall CM and Brody LT. Therapeutic Exercise: Moving Toward Function. 2nd Ed.
Philadelphia: Lippincott Williams and Wilkins, 2005.
Hodges PW and Richardson CA. Inefficient muscular stabilization of the lumbar
spine associated with low back pain. A motor control evaluation of transversus
abdominis. Spine. 1996;21:2640-2650.
Hodges PW, Eriksson AE, Shirley D, and Gandevia SC. Intra-abdominal pressure
increases stiffness of the lumbar spine. J Biomech. 2005;38:1873-1880.
Hubley-Kozey CL and Vezina MJ. Muscle activation during exercises to improve
trunk stability in men with low back pain. Arch Phys Med Rehabil. 2002;83:1100-
1108.
Hyde TE and Gengenbach MS. Conservative Management of Sports Injuries. 2nd Ed.
Sudbury MA: Jones and Bartlett Publishers, 2007.
Kavcic N, Grenier S, and McGill SM. Quantifying tissue loads and spine stability
while performing commonly prescribed low back stabilization exercises. Spine.
2004;29:2319-2329.
Kendall FP, McCreary EK, Provance PG, Rodgers MM, and Romani WA. Muscles:
Testing and Function, with Posture and Pain. 5th Ed. Baltimore: Lippincott
Williams and Wilkins, 2005.

-32-
Khadilkar A, Milne S, Brosseau L, Wells G, Tugwell P, Robinson V, Shea B, and
Saginur M. Transcutaneous electrical nerve stimulation for the treatment of
chronic low back pain: A systematic review. Spine. 2005;30:2657-2666.
Lehman GJ, Hoda W, and Oliver S. Trunk muscle activity during bridging exercises
on and off a Swiss ball. Chiropr Osteopat. 2005;13:14-21.
Marshall PW and Murphy BA. Core stability exercises on and off a Swiss ball. Arch
Phys Med Rehabil. 2005;86:242-249.
McGill S. Low Back Disorders: Evidence-Based Prevention and Rehabilitation. 2nd
Ed. Champaign, IL: Human Kinetics, 2002.
McGill SM, Grenier S, Kavcic N, and Cholewicki J. Coordination of muscle activity
to assure stability of the lumbar spine. J Electromyogr Kinesiol. 2003;13:353-359.
Mori A. Electromyographic activity of selected trunk muscles during stabilization
exercises using a gym ball. Electromyogr Clin Neurophysiol. 2004;44:57-64.
Neumann DA. Kinesiology of the Musculoskeletal System. 1st Ed. St. Louis: Mosby,
2002.
Panjabi MM. The stabilizing system of the spine. Part І. Function, dysfunction,
adaptation, and enhancement. J Spinal Disord. 1992;5:383-389.

-33-
Philadelphia Panel. Philadelphia Panel evidence-based clinical practice guidelines on
selected rehabilitation interventions for low back pain. Phys Ther. 2001;81:1641-
1674.
Pool-Goudzwaard AL, Vleeming A, Stoeckart R, Snijders CJ. and Mens JM.
Insufficient lumbopelvic stability: A clinical, anatomical and biomechanical
approach to ‘a-specific’ low back pain. Man Ther. 1998;3:12-20.
Shumway-Cook A and Woollacott M. Motor Control: Theory and Practical
Applications. 2nd Ed. Baltimore: Lippincott Williams and Wilkins, 2001.
Smeal WL, Tyburski M, Alleva J, Prather H, and Hunt D. Conservative management
of low back pain, Part I. Discogenic/radicular pain. Dis Mon. 2004;50:636-669.
Strand LI, Moe-Nilssen R, and Ljunggren AE. Back performance scale for the
assessment of mobility-related activities in people with back pain. Phys Ther.
2002;82:1213-1223.
Stevens VK, Bouche KG, Mahieu NN, Coorevits PL, Vanderstraeten GG, and
Danneels LA. Trunk muscle activity in healthy subjects during bridging
stabilization exercises. BMC Musculoskelet Disord. 2006;7:75-82.
Vera-Garcia FJ, Grenier SG, and McGill SM. Abdominal muscle response during
curl-ups on both stable and labile surfaces. Phys Ther. 2000;80:564-569.

-34-
Vezina MJ and Hubley-Kozey CL. Muscle activation in therapeutic exercises to
improve trunk stability. Arch Phys Med Rehabil. 2000;81:1370-1379.

-35-
국 요약
각운동 수행 시 지지면 조건이 복근
척추 립근 근 도에 미 는 향
연 학 학원
재 학과( 리 료학 공)
주
재 스포 분야에 체간안 증진시키 하여 다양한
운동 실시하고 있다. 단단한 지지면, 폼 (foam roll), 료용 공(gym
ball) 이용한 각운동 체간안 운동 하나 히 행해진다.
본 연구 목 단단한 지지면, 싯핏(sit-fit), 원 폼 (foam roll)
3 가지 지지면에 각운동과 각운동 시 한쪽 다리를 편 운동 시 복근
척추 립근 근 도를 알아보 하여 실시하 다. 요통
과거 이 없는 건강한 인 18 명 상 실시하 다. 각운동과
각운동 시 한쪽 다리를 편 운동 수행 할 양 복직근, 외복사근,

-36-
내복사근, 척추 립근 근 도를 면 근 도 분 시스
이용하여 하 다. 각 근 근 도는 복 일원
분산분 (one-way repeated ANOVA) 사용하여 지지면 간 차이를
하 다. 각운동과 각운동 시 한쪽 다리를 편 운동 사이 근
도 각 근 좌∙우 근 도 차이는 짝 t-검 통하여
하 고, 수 α=0.05 하 다. 연구결과 각운동 시 양쪽
복직근, 외복사근, 른쪽 내복사근 근 도는 싯핏보다 폼 에
하게 높았다. 각운동 시 폼 에 양쪽 외복사근, 내복사근, 척추
립근 근 도는 단단한 지지면에 보다 하게 높았다. 각운동
시 한쪽 다리를 편 운동 시 왼쪽 복직근, 양쪽 외복사근, 른쪽
내복사근 근 도는 싯핏보다 폼 에 하게 높았다. 각운동 시
한쪽 다리를 편 운동 시 폼 에 른쪽 외복사근, 내복사근, 양쪽
척추 립근 근 도는 단단한 지지면에 하게 높았다. 각운동
시 한쪽 다리를 편 운동 시 왼쪽 척추 립근 근 도는 단단한
지지면에 보다 싯핏에 하게 높았다. 각운동 시행 보다 각운동
시 한쪽 다리를 편 운동 시행할 모든 복근 척추 립근 근
도가 하게 높았다. 각운동 시 복근 척추 립근 좌∙우
근 도는 한 차이가 없었다. 다른 3 가지 지지면에
각운동 시 한쪽 다리를 편 운동 시행 시 른쪽 복직근 근 도가
-37-
왼쪽 복직근 근 도보다 하게 높았다. 단단한 지지면과
싯핏에 각운동 시 한쪽 다리를 편 운동 시행 시 른쪽 척추
립근 근 도가 왼쪽 척추 립근 근 도보다 하게 높았다.
이러한 결과에 근거하여 싯핏이나 폼 에 각 운동시 한쪽 다리를
편 운동 실시하는 것 체간안 증진시키는데 효과 인 법이라고
할 수 있겠다.
핵심 는 말: 각운동, 근 도, 복근, 불안 한 지지면, 척추 립근,
체간안 운동.










![3 DeMenten ABIM2010.ppt [Kompatibilitätsmodus]€¦ · •Praon volucre •Aphelinus abdominalis. FresaProtect: Aphids-parasitoids relations Aphid/parasitoid A. ervi A. matricariae](https://img.pdfslide.us/doc/110x75/606b8794115a68079b644661/3-dementen-kompatibilittsmodus-apraon-volucre-aaphelinus-abdominalis-fresaprotect.jpg)

















