Embed Size (px)
Citation preview
• 347 •Chin J Integr Med 2014 May;20(5):347-352
Type 2 diabetes mellilus (T2DM) is one of the most prevalent chronic diseases and it is the fourth major cause of mortality worldwide.(1) The World Health Organization (WHO) estimates that the number of people with diabetes in age range of 45–64 years old will be more than 140 million in developing countries and more than 30 million in developed countries by 2030.(2)
Patients with T2DM are at high risk of developing chronic diseases like atherosclerosis and coronary heart and renal diseases.(3) Development of chronic diseases in these patients has been hypothesized to be accelerated by increased oxidative stress.(4) Poor glycemic control may also lead to reduce antioxidant defense mechanisms which can cause cellular enzymes damage, increased lipid peroxidation, and development of insul in resistance. (5) The results of previous studies showed that antioxidant supplementation such as vitamin E and C may improve oxidative stress and glycemic control in patients with T2DM.(6-9)
Royal jelly (RJ) is a viscous and milky substance
secreted by the hypopharyngeal and mandibular glands of worker honeybees (Apis mellifera) and is an essential food for both the queen and her larvae.(10) RJ comprises 60%–70% water, 10%–12% carbohydrates, 12%–15% proteins, and 3%–7% lipids.(11) It has been suggested that RJ may have antioxidant properties, El-Neekety, et al(12) reported that RJ decreased malondialdehyde (MDA) levels and enhanced antioxidants enzyme activity in fumonisin rats. Also it has been noted that RJ prolongs life span in mice through decreasing oxidative stress.(13) In addition, findings of in vivo and in vitro studies indicated that
ORIGINAL ARTICLE
Effects of Royal Jelly Supplementation on Glycemic Control and Oxidative Stress Factors in Type 2 Diabetic
Female: A Randomized Clinical Trial
Samira Pourmoradian1, Reza Mahdavi1, Majid Mobasseri2, Elnaz Faramarzi3, and Mehrnoosh Mobasseri4
©The Chinese Journal of Integrated Traditional and Western Medicine Press and Springer-Verlag Berlin Heidelberg 2014Support by the Nutrition Research Center, Tabriz University of Medical Sciences1. Nutrition Research Center, Tabriz University of Medical Sciences, Tabriz, Iran; 2. Endocrinology Department of Medicine Faculty, Tabriz University of Medical Sciences, Tabriz, Iran; 3. Student Research Committee, Faculty of Nutrition, Tabriz University of Medical Sciences, Tabriz, Iran; 4. Faculty of Medicine, Tabriz University of Medical Sciences, Tabriz, IranCorrespondence to: Dr. Reza Mahdavi, Tel: 98-4113341113, Fax: 98-4113363430, E-mail: [email protected]: 10.1007/s11655-014-1804-8
ABSTRACTABSTRACT ObjectiveObjective: It has been proposed that royal jelly has antioxidant properties and may improve : It has been proposed that royal jelly has antioxidant properties and may improve
oxidative stress and glycemic control. Therefore, we investigated the effects of royal jelly supplementation in oxidative stress and glycemic control. Therefore, we investigated the effects of royal jelly supplementation in
diabetic females. diabetic females. MethodsMethods: In this pilot, parallel design randomized clinical trial, 50 female volunteers with type : In this pilot, parallel design randomized clinical trial, 50 female volunteers with type
2 diabetes were randomly allocated to the supplemented (25, cases) and placebo (25, cases) groups, based on 2 diabetes were randomly allocated to the supplemented (25, cases) and placebo (25, cases) groups, based on
random block procedure produced by Random Allocation Software, given a daily dose of 1,000 mg royal jelly random block procedure produced by Random Allocation Software, given a daily dose of 1,000 mg royal jelly
soft gel or placebo, respectively, for 8 weeks. Before and after intervention, glycemic control indices, antioxidant soft gel or placebo, respectively, for 8 weeks. Before and after intervention, glycemic control indices, antioxidant
and oxidative stress factors were measured. and oxidative stress factors were measured. ResultsResults: After royal jelly supplementation, the mean fasting blood : After royal jelly supplementation, the mean fasting blood
glucose decreased remarkably (163.05±42.51 mg/dL glucose decreased remarkably (163.05±42.51 mg/dL vsvs. 149.68±42.7 mg/dL). Royal jelly supplementation . 149.68±42.7 mg/dL). Royal jelly supplementation
resulted in significant reduction in the mean serum glycosylated hemoglobin levels (8.67%±2.24% resulted in significant reduction in the mean serum glycosylated hemoglobin levels (8.67%±2.24% vsvs. .
7.05%±1.45%, 7.05%±1.45%, P=0.001) and signifi cant elevation in the mean insulin concentration (70.28±29.16 pmol/L =0.001) and signifi cant elevation in the mean insulin concentration (70.28±29.16 pmol/L vsvs. .
86.46±27.50 pmol/L, 86.46±27.50 pmol/L, P=0.01). Supplementation significantly increased erythrocyte superoxidase dismutase =0.01). Supplementation significantly increased erythrocyte superoxidase dismutase
and glutathione peroxidase activities and decreased malondialdehyde levels (and glutathione peroxidase activities and decreased malondialdehyde levels (P<0.05). At the end of study, the <0.05). At the end of study, the
mean total antioxidant capacity elevated insignifi cantly in both groups. mean total antioxidant capacity elevated insignifi cantly in both groups. ConclusionsConclusions: On the basis of our fi ndings, : On the basis of our fi ndings,
it seems that royal jelly supplementation may be benefi cial in controlling diabetes outcomes. Further studies with it seems that royal jelly supplementation may be benefi cial in controlling diabetes outcomes. Further studies with
larger sample size are warranted. larger sample size are warranted.
KEYWORDSKEYWORDS glycemic control, oxidative stress, Royal jelly, type 2 diabetes glycemic control, oxidative stress, Royal jelly, type 2 diabetes
• 348 • Chin J Integr Med 2014 May;20(5):347-352
RJ has hypotensive,(14) anti-hypercholesterolemic,(15) anti-infl ammatory,(16) anti-tumor,(17) antioxidant,(18) and hypoglycemic functions.(19) It has insulin like peptide activity which may improve insulin resistance.(20,21)
To the best of our knowledge, there are few reports about the effects of RJ on oxidative stress and glycemic control in diabetic patients, therefore, the aim of this study was to determine the effects of RJ supplementation in diabetic females.
METHODS
Trial Design This pilot, parallel design randomized clinical
trial was approved by the Ethics Committee of Tabriz University of Medical Sciences (code: 8939) with WHO registered randomized clinical trial number: IRCT201011131197N5 (available at: http://www.who.int/trialsearch) and the written consent obtained from all participants.
Participants Fifty female volunteers with T2DM, recruited
from the outpatient endocrine Clinic of Sina Hospital in Tabriz from December 2010 to March 2011.
Inclusion CriteriaStudy inclusion criteria were: patients who had
been diagnosed with type 2 diabetes at least one year ago, age 30–65 years, body mass index (BMI) 25–30 kg/m2, taken glucose-lowering medications for T2DM but without insulin injection.
Exclusion CriteriaExclusion criteria included: consuming trace
element and antioxidants supplements in the previous 6 months, pregnancy and lactation; having acute renal disease; endocrine dysfunction and allergy.
Case SelectionThe eligible participants were randomly allocated
to intervention and placebo groups based on random block procedure produced by Random Allocation Software. A computer-generated random sequence was kept in a remote secure location and administered by an independent third party who was not involved with the clinical conduct of study until all study data were collected and verifi ed. Patients and those involved in enrolling participants, administering interventions and assessing outcomes were blind to group assignments.
InterventionsThe patients were randomly assigned to the
supplemented group (25, cases), based on random block procedure produced by Random Allocation Software, receiving RJ soft gel (each soft gel include 1,000 mg lyophilized RJ providing 1 g fresh RJ) once a day after breakfast and placebo group (25, cases) receiving one placebo soft gel for 8 weeks. The RJ and placebo soft gels had an identical appearance. The participants were asked to keep their usual dietary intake, physical activity and medication during the study period. Patients were monitored weekly for any side effects of RJ supplementation.
Items and Methods of ObservationAt the onset and the end of the intervention, 5 mL
venous blood samples were collected after an overnight fast of 12 h. The serum samples of patients were kept at –80 ℃ until biochemical analysis.
Serum fasting blood glucose (FBG) and insulin concentration were determined by the enzymatic colorimetric method and enzyme-linked immunosorbent assay (ELISA) methods using Monobind ki ts respectively. Glycosylated hemoglobin (HbA1c) was assessed by immune turbidimetric method.
Serum total ant ioxidant capaci ty (TAC), erythrocyte superoxide dismutase (SOD) and glutathione peroxidase (GSH-PX) activities were measured by autoanlyzer with randox kits. Serum MDA level was assessed by colorimetric method.
Statistical AnalysisDescriptive statistics were obtained for all
study variables for each study group. The normality of variables was tested by the Kolmogorov-Smirnov test. Differences between two treatment groups were analyzed using independent t-test. Paired t-test and wilcoxon was used to compare the differences within a group when it's appropriate. ANCOVA test was used to adjust for the effects of confounding factors (basel ine values of MDA levels). A P value less than 0.05 was considered statistically signifi cant.
RESULTS
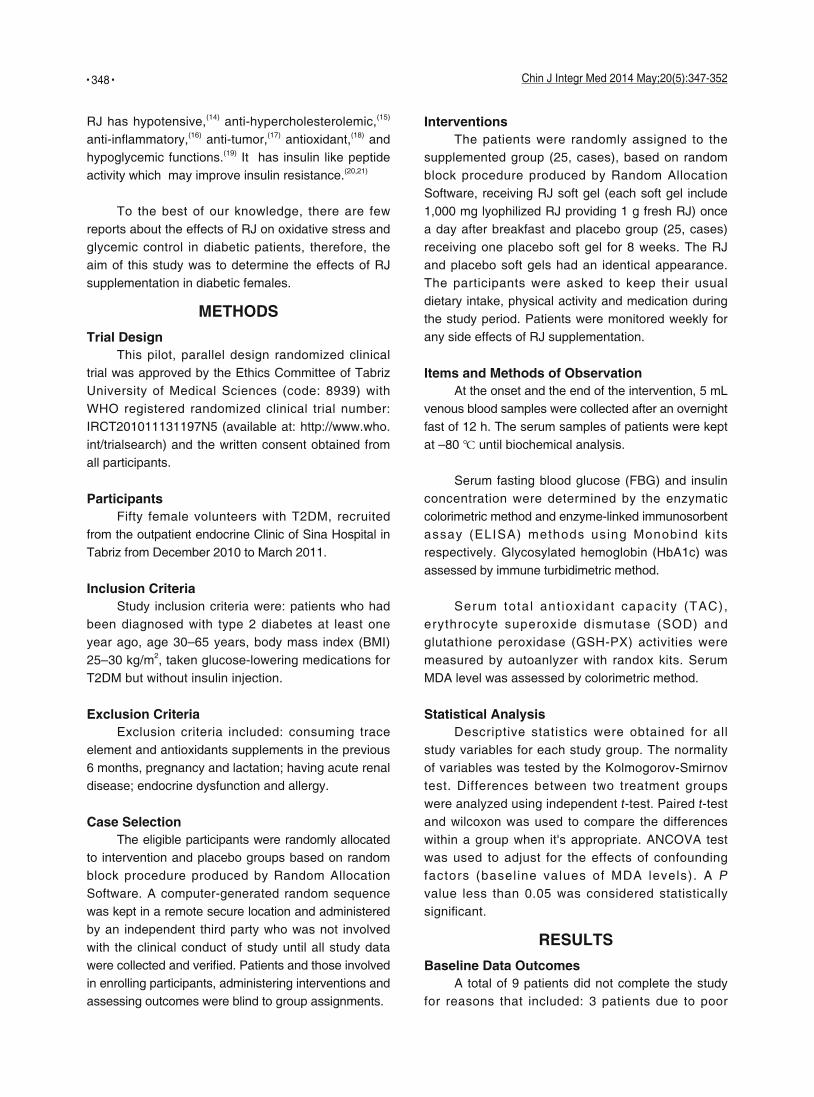
Baseline Data OutcomesA total of 9 patients did not complete the study
for reasons that included: 3 patients due to poor
• 349 •Chin J Integr Med 2014 May;20(5):347-352
(71.00±6.44 kg) and BMI (28.40±1.06 kg/m2), however after intervention slight elevation in the mean body weight (73.52±6.80 kg) and BMI (28.80±1.36 kg/m2) were observed in the placebo group.
Comparison of the Results of Glycemic Control Factors between Groups
Glycemic control parameters of study groups at the onset and the end of intervention are presented in Table 2. The mean serum FBG levels decreased in both groups but reduction in supplemented group
Figure 1. Study Flow Diagram
Allocated to RJ group (n=25)• Biochemical factors was measured• Received 1,000 mg/day RJ soft gel for 8
weeks (n=25)
Lost to follow-up (personal reason, n=2)Discontinued intervention:• Poor compliance with study protocols (n=2)
• Biochemical factors was measured• Analysed (n=21)
Allocated to placebo group (n=25)• Biochemical factors was measured• Received 1,000 mg/day placebo soft gel for
8 weeks (n=25)
Lost to follow-up (personal reason, n=3)Discontinued intervention:• Poor compliance with study protocols (n=1)• Gastrointestinal disturbances (n=1)
• Biochemical factors was measured• Analysed (n=20)
Enrollment
Allocation
Follow-up
Analysis
Assessed for eligibility (n=240)
Excluded (n=190)• Not meeting inclusion criteria (n=135)• Declined to participate (n=40)• Other reasons (n=15)
Randomized (n=50)
compliance with study protocols, 1 patient due to gastrointestinal disturbances, and 5 patients due to personal reasons (Figure 1).
Baseline characterist ics of patients were presented in Table 1, at the beginning of the study, the two groups were similar based upon the mean age, weight, BMI, diabetes duration a n d b i o c h e m i c a l p a r a m e t e r s e x c e p t M D A levels. At the end of study, supplementation of RJ did not increase in the mean body weight
Table 1. Baseline Characteristics of Patients ( ±s)
Group Case Age (Year) Weight (kg) BMI (kg/m2) Duration of diabetes (Year)
RJ 21 51.7±6.3 72.45±4.42 28.98±1.10 5.2±3.1
Placebo 20 51.4±9.6 73.07±6.44 28.80±1.36 5.1±2.8
P value 0.91 0.71 0.64 0.87
Notes: BMI: body mass index; Independent t-test value
Table 2. Comparison of Glycemic Control Measurements in Both Groups before and after Intervention ( ±s)
Group Case Time FBG (mg/dL) HbA1c (%) Insulin (pmol/L)
RJ 21 Before 163.05±42.50 8.67±2.24 70.28±29.16
After 149.68±42.75 7.05±1.45 27.50±86.46
P 0.08 0.001 0.001
Placebo 20 Before 145.06±44.23 7.80±1.03 34.03±86.74
After 39.49±139.06 7.03±1.00 34.09±81.11
P 0.54 0.01 0.35
Note: compared with before intervention in the same group; paired t-test
• 350 • Chin J Integr Med 2014 May;20(5):347-352
was remarkable (P=0.08). The mean HbA1C levels significantly decreased in both groups but changes were dramatic in the RJ group (P=0.001). In contrast to the placebo group, the mean serum insulin concentrations was significantly increased in the supplemented group (P<0.05).
Comparison of the Results of Oxidative Stress Factors between Groups
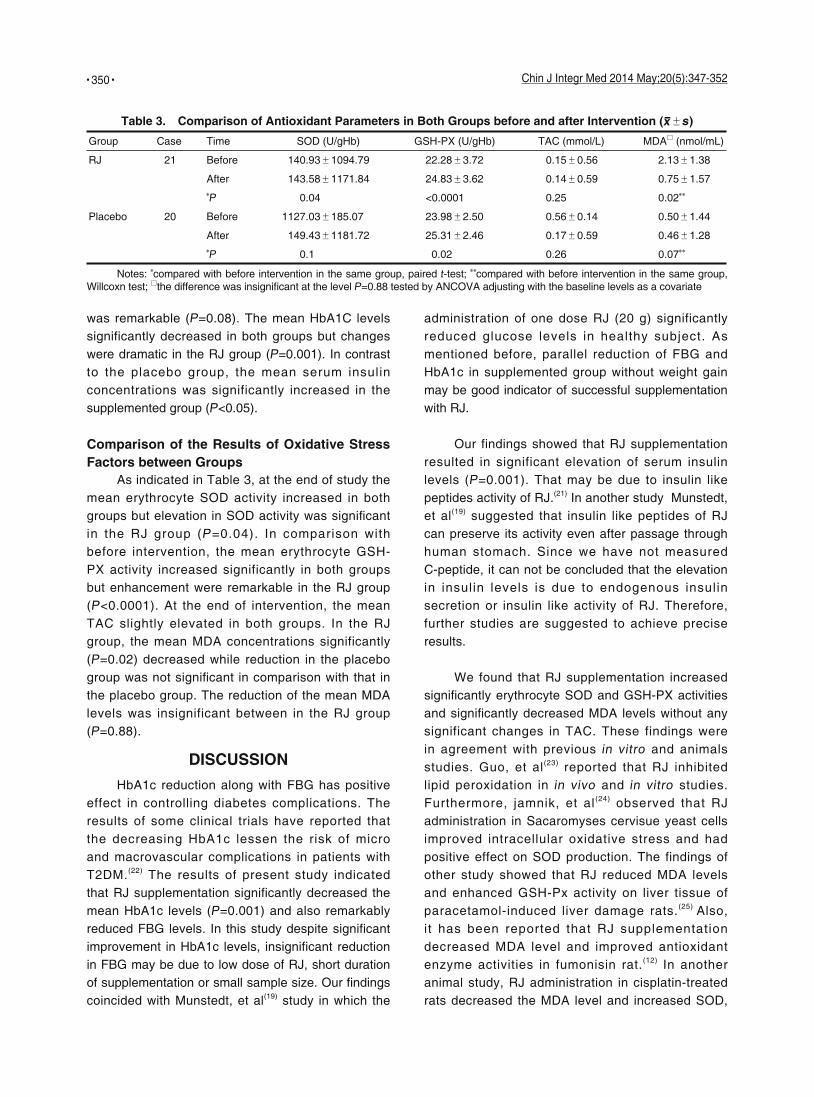
As indicated in Table 3, at the end of study the mean erythrocyte SOD activity increased in both groups but elevation in SOD activity was signifi cant in the RJ group (P=0.04). In comparison with before intervention, the mean erythrocyte GSH-PX activity increased significantly in both groups but enhancement were remarkable in the RJ group (P<0.0001). At the end of intervention, the mean TAC slightly elevated in both groups. In the RJ group, the mean MDA concentrations significantly (P=0.02) decreased while reduction in the placebo group was not signifi cant in comparison with that in the placebo group. The reduction of the mean MDA levels was insignificant between in the RJ group (P=0.88).
DISCUSSION
HbA1c reduction along with FBG has positive effect in controlling diabetes complications. The results of some clinical trials have reported that the decreasing HbA1c lessen the risk of micro and macrovascular complications in patients with T2DM.(22) The results of present study indicated that RJ supplementation significantly decreased the mean HbA1c levels (P=0.001) and also remarkably reduced FBG levels. In this study despite significant improvement in HbA1c levels, insignificant reduction in FBG may be due to low dose of RJ, short duration of supplementation or small sample size. Our fi ndings coincided with Munstedt, et al(19) study in which the
administration of one dose RJ (20 g) significantly reduced glucose levels in healthy subject. As mentioned before, parallel reduction of FBG and HbA1c in supplemented group without weight gain may be good indicator of successful supplementation with RJ.
Our findings showed that RJ supplementation resulted in significant elevation of serum insulin levels (P=0.001). That may be due to insulin like peptides activity of RJ.(21) In another study Munstedt, et al(19) suggested that insulin like peptides of RJ can preserve its activity even after passage through human stomach. Since we have not measured C-peptide, it can not be concluded that the elevation in insulin levels is due to endogenous insulin secretion or insulin like activity of RJ. Therefore, further studies are suggested to achieve precise results.
We found that RJ supplementation increased signifi cantly erythrocyte SOD and GSH-PX activities and signifi cantly decreased MDA levels without any significant changes in TAC. These findings were in agreement with previous in vitro and animals studies. Guo, et al(23) reported that RJ inhibited lipid peroxidation in in vivo and in vitro studies. Furthermore, jamnik, et al(24) observed that RJ administration in Sacaromyses cervisue yeast cells improved intracellular oxidative stress and had positive effect on SOD production. The findings of other study showed that RJ reduced MDA levels and enhanced GSH-Px activity on liver tissue of paracetamol-induced liver damage rats.(25) Also, it has been reported that RJ supplementation decreased MDA level and improved antioxidant enzyme activities in fumonisin rat.(12) In another animal study, RJ administration in cisplatin-treated rats decreased the MDA level and increased SOD,
Table 3. Comparison of Antioxidant Parameters in Both Groups before and after Intervention ( ±s)
Group Case Time SOD (U/gHb) GSH-PX (U/gHb) TAC (mmol/L) MDA□ (nmol/mL)
RJ 21 Before 140.93±1094.79 22.28±3.72 0.15±0.56 2.13±1.38
After 143.58±1171.84 24.83±3.62 0.14±0.59 0.75±1.57
P 0.04 <0.0001 0.25 0.02
Placebo 20 Before 1127.03±185.07 23.98±2.50 0.56±0.14 0.50±1.44
After 149.43±1181.72 25.31±2.46 0.17±0.59 0.46±1.28
P 0.1 0.02 0.26 0.07
Notes: compared with before intervention in the same group, paired t-test; compared with before intervention in the same group, Willcoxn test; □the difference was insignifi cant at the level P=0.88 tested by ANCOVA adjusting with the baseline levels as a covariate

• 351 •Chin J Integr Med 2014 May;20(5):347-352
catalase, and GSH-PX activities.(26) Our findings supported the result of previous studies. (23-26) Researchers suggested that possible mechanism for antioxidant activity of RJ may be due to: (1) Three tyrosyl dipeptides (Lys-Tyr, Arg-Tyr, and Tyr-Tyr) of RJ have high antioxidant activity in in vitro which scavenge the free radicals by hydroxyl group of their hydrogen atom.(27) (2) RJ downregulated cytochrome P450 4A14 enzymes and detoxifying enzymes genes which catalyzed peroxidation of endogenous lipids and upregulated of glutathione-s-transferase and glutathione peroxides genes.(28) We thought that the improvement in antioxidant status and oxidative stress in supplemented group can be justified by mentioned mechanisms.
In conclusion, our findings revealed that RJ supplementation led to remarkable reduction in HbA1c and FBG levels and significant increase in insulin concentrations. Also, supplementations decreased oxidative stress via improvement of MDA levels, erythrocyte SOD and GSH-PX activities. On the basis of positive results of present study, supplementation with RJ may be beneficial for diabetic patients. However, further studies with large sample size, long-term period and high dose of RJ supplementation in diabetic patients are needed to achieve more precise results.
AcknowledgmentsThe authors are deeply indebted to all patients who
participated in this study. The results of this paper are from
Pourmoradian's MSc thesis which was registered in Tabriz
University of Medical Sciences.
REFERENCES 1. Khuwaja AK, Khowaja LA, Cosgrove P. The economic
costs of diabetes in developing countries: some concerns
and recommendations. Diabetologia 2010;53:389-390.
2. Wild S, Roglic G, Green A, Sicree R, King H. Global
prevalence of diabetes: estimates for the year 2000 and
projections for 2030. Diabetes Care 2004;27:1047-1053.
3. Glugliano D, Paolisso G, Ceriello A. Oxidative stress
and diabetes vascular complications. Diabetes Care
1996;19:257-267.
4. Roussel A, Kerkeni, Zouari N, Mahjoub S, Matheau J,
Richard A. Antioxidant effects of zinc supplementation in
Tunisians with type 2 diabetes mellitus. J Am Coll Nutr
2003;22:4:316-321.
5. Bonnefont-roussel D, Batrad JP, Jaudon MC, Delattre
J. Consequences of the diabetic status on the oxidant/
antioxidant balance. Diabetes Metab 2000;26:163-176.
6. Johansen JS, Harris AK, Rychly DJ, Ergul A. Oxidative
stress and the use of antioxidants in diabetes: linking
basic science to clinical practice. Cardiovasc Diabetol
2005;4(1):5.
7. Neri S, Signorelli SS, Torrisi B, Pulvirenti D, Mauceri B,
Abate G, et al. Effects of antioxidant supplementation on
postprandial oxidative stress and endothelial dysfunction:
a single-blind, 15-day clinical trial in patients with untreated
type 2 diabetes, subjects with impaired glucose tolerance,
and healthy controls. Clin Ther 2005;27:1764-1773.
8. Vega-Lopez S, Devaraj S, Jialal I. Oxidative stress and
antioxidant supplementation in the management of diabetic
cardiovascular disease. J Investig Med 2004;52:24-32.
9. Lee DH, Falsom AR, Harnack L, Halliwell B , Jacobs Jr
DR. Does supplemental vitamin C increase cardiovascular
disease risk in women with diabetes? Am J Clin Nutr
2004;80:1194-1200.
10. Fujii A, Kobayashi S, Kuboyama N, Furukawa Y, Kaneko Y,
Ishihama S, et al. Augmentation of wound healing by royal
jelly (RJ) in streptozotocin-diabetic rats. Jpn J Pharmacol
1990;53:331–337.
11. Suzuki KM, Isohama Y, Maruyama H, Yamada Y, Narita
Y, Ohta SH, et al. Estrogenic activities of fatty acids and a
sterol isolated from Royal Jelly. Evid Based Complement
Alternat Med 2008;5:295-302.
12. El-Nekeety AA, El-Kholy W, Abbas NF, Ebaid A, Amra
HA, Abdel-Wahhab MA. Efficacy of royal jelly against
the oxidative stress of fumonisin in rats. Toxicon
2007;50:256-269.
13. Inoue SI, Koya-Miyata S, Ushio S, Iwak K, Ikeda M,
Kurimoto M. Royal jelly prolongs the life span of C3H/H3J
mice: correlation with reduced DNA damage. Exp Gerontol
2003;38:965-969.
14. Tokunaga KH, Yoshida CH, Suzuki KM, Maruyama H,
Futamura Y, Araki Y, et al. Antihypertensive effect of
peptides from Royal Jelly in spontaneously hypertensive
rats. Biol PharmBull 2004;27:189-192.
15. Gou H, Sagia A, Sato M, Miyazawa I, Shibata M,
Takahata Y, et al. Royal jelly supplementation improve
lipoprotein metabolism in humans. J Nutr Sci Vitaminol
2007;53:354-348.
16. Kohno K, Okamoto I, Sano O, Arai N, Iwaki K, Ikeda M, et
al. Royal jelly inhibits the production of proinflammatory
cytokines by activated macrophages. Biosci Biotechnol
Biochem 2004;68:138-145.
17. Towsend GF, Morgan JF, Hazlett B. Activity of 10-hydro-
xydecenoic acid from royal jelly against experimental
leuacemia and ascitic tumors. Nature 1959;183:1270-1271.
18. Nagai T, Inoue R. Preparation and the functional properties

• 352 • Chin J Integr Med 2014 May;20(5):347-352
of water extract and alkaline extract from royal jelly. Food
Chem 2004;84:181-186.
19. Munstedt K, Baregello M, Hauenschild A. Royal jelly reduce
the serum glucose levels in healthy subjects. J Med Food
2009;12(5):1-3.
20. Dixit PK, Patel NG. Insulin-like activity in larval foods of the
honeybee. Nature Lond 1964; 202:189-190.
21. Kramer KJ, Tager HS. Insul in- l ike and glucagon-
like peptides in insect hemolymph Insect. Biochem
1980;10:179-182.
22. Woerle HJ, Neumann Ch, Zschau S, Tenner S, Irsigler A,
Schirra J, et al. Impact of fasting and postprandial glycemia
on overall glycemic control in type 2 diabetes importance
of postprandial glycemia to achieve target HbA1c levels.
Diabetes Res Clin Pract 2007;77:280-285.
23. Gou H, Ekusa A, Iwai K, Yonekura M, Takahata Y,
Morimatsu F. Royal jelly peptides inhibit lipid peroxidation in
in vitro and in vivo. J Nutr Sci Vitaminol 2008;54:191-195.
24. Jamnik P, Goranovic D, Raspor P. Antioxidative action of
royal jelly in the yeast cell. Exp Gerontol 2007;42:594-600.
25. Kanbur M, Eraslan G, Beyaz L. The effects of royal jelly on
liver damage induced by paracetamol in mice. Exp Toxicol
Pathol 2009;61:123-132.
26. Si l ic i S, Ekmekcioglu O, Eraslan G, Demir tas A.
Antioxidative effect of Royal Jelly in cisplatin-induced testes
damage. Urology 2009;74:545-551.
27. Gou H, Yoshiaki A, Yonekura M. Structures and properties
of antioxidative peptides derived from royal jelly protein.
Food Chem 2009;113:238-245.
28. Kanbur M, Eraslan G, Silici S, Karababack M. Effects of
sodium fl uoride exposure on some biochemical parameters
in mice: Evaluation of the ameliorative effect of royal jelly
applications on these parameters. Food Chem Toxicol
2009;47:1184-1189.
(Received January 18, 2012)Edited by ZHANG Wen