Embed Size (px)
Citation preview

Effects of Relapse Forces on PeriodontalStatus of Mandibular Incisors FollowingOrthognathic SurgeryArzu Ari-Demirkaya* and Isil Ilhan*
Background: In this case-control study, the relationship be-tween the relapse forces and periodontal changes in the man-dibular incisor region were investigated following orthognathicsurgery.
Methods: Mucogingival and alveolar changes in 36 sub-jects with mandibular prognathism were analyzed by clinicaland roentgenographic methods just before mandibular set-back surgery and 7.4 months postoperatively. The resultswere compared to two control groups: 36 subjects with no or-thodontic history and 33 orthodontic patients. The mean ageof the 105 subjects was 20.21 years.
Results: The intergroup comparisons showed significantdifferences in all parameters, except for the plaque index andalveolar height measurements. By an incisor proclination of3.3 mm and a tipping of +8.5� (postoperative relapse: 0.8 mmand 0.14�), the surgery group revealed significant changes insingle parameters of both alveolar height and sulcus depthmeasurements.
Conclusions: Compared to both control groups, the preop-erative periodontal condition of the surgery patients was lessacceptable than in the orthodontically treated patients, whereassubjects without braces presented the most ideal hygienic con-ditions. In the short term, the decompensation process priorto mandibular setback surgery did not affect periodontal struc-tures significantly, and the current study did not find anynegative effects of early postoperative relapse forces on themandibular incisor area. J Periodontol 2008;79:2069-2077.
KEY WORDS
Maxillofacial surgery; periapical tissue; prognathism;stability; tooth movement.
Severe skeletal discrepancies, suchas mandibular overgrowths, areoften camouflaged by dental com-
pensations, resulting in proclined upperincisors and retroclined lower incisors.Preoperative correction of these incisorpositions often becomes necessary toachieve proper postoperative occlusion,without which there is an increased riskfor postoperative relapse. However, theresulting pre- and postoperative labio-lingual movements may become a riskfactor for localized gingival recession ordecreased crestal alveolar bone levels.
The definition of orthodontic relapse isthe loss of any correction achieved by or-thodontic treatment.1 However, postop-erative relapse is not limited to toothmovement; it also occurs as a result ofaltered muscular force moments actingon the temporomandibular joint (TMJ),such as trying to adapt to the new shapeand location of the bone. According tothe hierarchy of stability for surgical pro-cedures, mandibular setback is consid-ered to be less stable than maxillaryimpaction, maxillary advancement, ormandibular advancement procedures.2
This makes the stomatognathic systemsusceptible to the effects of the relapsingforces up to 1 year postoperatively, untilthe physiologic adaptation is completedand morphologic changes are settled.3
During the first few weeks following set-backoperations,theinterdigitationissome-times ensured by a splint, acting similarto class III elastics on the dentoalveolar
* Department of Orthodontics, Faculty of Dentistry, Marmara University, Istanbul, Turkey.
doi: 10.1902/jop.2008.070576
J Periodontol • November 2008
2069

system. The resulting lingual inclination of the mandibu-lar incisors,alongwith labial rootmovement,may lead toperiodontal problems despite the preventive measurestaken preoperatively (e.g., thickest possible archwireor lingual root torque).Therefore, it is important to recog-nize the risk factors for a timely intervention.
According to some studies,4-6 a thin or non-exis-tent labial plate of bone in the presence of bacterialplaque can easily result in attachment loss, which
may lead to gingival recession. In orthodontic pa-tients, it may become difficult to pinpoint or controlthese problems. Although one study7 suggested lim-iting labiolingual tooth movement in patients with nar-row alveolar bone width, other investigators8 found noconclusive evidence as to the damage or benefit toperiodontal structures from orthodontic treatment.
The effect of excessive proclination of the mandib-ular incisors on periodontal tissues is also controver-sial. In two studies,9,10 no relationship was foundbetween gingival recession and the amount of incisorproclination or the clinical crown length, whereas ananimal study by Steiner et al.11 revealed significantgingival recession, as well as connective tissue andmarginal bone loss, following 3.05 mm of labial inci-sor movement. Wennstrom12 also investigated therelationship between incisor movement and muco-gingival changes, pointing out two important factorsrelated to gingival defects: direction of tooth move-ment and the bucco-lingual thickness of the gingiva.
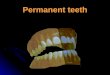
Figure 1.Alveolar height and root length changes. a = distance between thealveolar crest and the root apex; b = tooth length; c = distancebetween incisor edge and cemento-enamel junction.
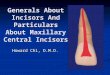
Figure 2.Cephalometric landmarks and planes used in the study: S = sella;N = nasion; Go = gonion; Me = menton; 1 = sella-nasion (SN);2 = horizontal reference (HR) plane (SN+7�); 3 = vertical reference(VR) plane (perpendicular to HR); 4 = mandibular plane (MP);5 = nasion-B point (NB).
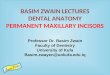
Figure 3.Measurements of symphyseal morphology. Me = menton; w = width ofthe symphysis; h = height of the symphysis; CEJ = cemento-enameljunction.
Table 1.
Cephalometric Measurements inthe S Group
Measurement
Initial Preoperative Postoperative
Mean SD Mean SD Mean SD
IMPA (�) 79.11 8.36 87.67 4.82 87.53 5.68
L1?VR (mm) 75.14 9.04 78.44 8.97 76.22 8.64
L1?MP (mm) 42.72 3.75 43.39 3.51 43.14 3.51
SNB (�) 81.25 3.91 81.25 3.93 80.03 3.87
Symphysis height (mm) 33.11 3.13
Symphysis width (mm) 14.69 1.94
Symphysis ratio 2.29 0.36
L1?MP = perpendicular through lower incisor edge to mandibular plane.
Periodontal Implications After Orthognathic Surgery Volume 79 • Number 11
2070

One of the few studies on surgically treated patientswas performed by Artun and Krogstad,13 who re-ported increased clinical crown length and recessionafter excessive proclination. However, they statedthat most of these periodontal changes occurred inthe short-term, and the long-term prognosis was ac-ceptable. In another surgical study, Foushee et al.14
found a significant decrease in the keratinized and at-tached gingiva in the mandibular anterior region, withone-fourth of subjects displaying significant gingivalrecession postoperatively. In a long-term, follow-upstudy from Cheung and Lo,15 3.9% of the subjectsdeveloped gingival recession with mildly increasedprobing depth 3 to 12 years after mandibular steposteotomy.
Because of the small number of studies and theconflicting results, this study analyzed and evaluatedthe periodontal effects of preoperative mandibularincisor proclination and subsequent postoperativelingual tilting due to interincisal locking caused byanteriorly directed relapse forces on the mandible.
MATERIALS AND METHODS
The current study was conducted on 133 patients,who were referred to a university clinic for orthodontictreatment between 2000 and 2007. The number ofdrop-outs was 28: 14 subjects with inadequate oralhygiene, four patients with fillings in the incisor region,six patients with low-quality records, and four subjectswho failed to show for recall. One study group and twocontrol groups were formed to compare the findings ofnon-treated and otherwise orthodontically treated pa-tients to the surgery patients.
The surgery (S) group consisted of 36 skeletallyclass III non-growing patients (15 males and 21females). During the preoperative period, proclina-tion of lower incisors and subsequent mesializationof the remaining posterior teeth were performed, with-out any expansion of the mandibular arch. The sur-gery protocol included double jaw surgery (bilateral
sagittal split and Le Fort 1 osteotomies) and rigid-fix-ation methods (titanium miniplates for the maxillaand triple titanium screws at the gonial region forthe mandible). Maxilla underwent sagittal changesonly, and 30 of 36 patients had additional chin aug-mentation. Postoperative retention involved an aver-age of 10 days of intermaxillary fixation with elasticsand an acrylic splint to stabilize the occlusion. Toothmovements after this period were limited to minor rootadjustments. The mean age of the group was 19.62years (range: 17.42 to 26.67 years).
The first control (C1) group consisted of 36 sub-jects (14 males and 22 females) selected from 613consecutively examined candidates who were ex-amined in 1 month. The selection criteria were adultsubjects with no history of orthodontic treatment,presence of a malocclusion, and ‡20 permanent teethto permit adequate periodontal examination. Themean age of the group was 20.47 years (range:16.42 to 31.17 years).
For the second control (C2) group, a random fileselection of all actively treated patients with variousmalocclusions was performed at the same time asthe C1 group selection. Following a clinical examina-tion, 33 patients (18 males and 15 females) were in-corporated into the study. The criterion for the C2group was adults with no extractions and completedleveling of the mandibular incisors at the time of theexamination. The mean age of the group was 20.57years (range: 16.83 to 31.50 years).
Data Collection and AnalysisTo eliminate dental plaque as a possible etiologic fac-tor for periodontal changes, dental awareness of thepotential subjects was evaluated with a questionnairethat contained the following inquiries: 1) regularity ofdental visits: irregular (score 1), every 12 months (score2), every 6 months (score 3); 2) regularity of tooth-brushing: irregular (score 1), once daily (score 2),twice daily (score 3); and 3) use of dental floss: never(score 1), irregular (score 2), once daily (score 3).
Table 2.
Pearson Correlations Between Vertical Pattern and Incisor Locations at Various Times
L1?VR 1 L1?VR 2 L1?VR 3 L1?MP 1 L1?MP 2 L1?MP 3 IMPA1
SN-MP (�) r -0.314 -0.324 -0.124 0.060 0.120 0.038 -0.340P 0.062 0.054 0.470 0.727 0.485 0.827 0.043*
IMPA 2 IMPA 3 SNB1 SNB2 SNB3 h w R
SN-MP (�) r -0.306 -0.196 -0.530 -0.541 -0.255 0.211 -0.191 0.331P 0.070 0.252 0.001† 0.001† 0.134 0.217 0.264 0.048*
L1?MP = perpendicular through lower incisor edge to mandibular plane; 1 = initial visit; 2 = preoperative visit; 3 = postoperative visit; r = Pearson coefficient;P = level of significance; bold type = statistically significant; h = height of symphysis; w = width of symphysis; R = symphysis ratio (h/w).* P <0.05.† P <0.001.
J Periodontol • November 2008 Ari-Demirkaya, Ilhan
2071

Subjects with a total score between 6 and 9 wereincluded in the study. Subjects with smoking habitsor a history of allergy were excluded to prevent anypossible alterations in the gingival response duringthe course of the study.
To control the oral hygiene status throughoutthe study, the patients in the S and C2 groups re-ceived instructions at the beginning of treatment,which were repeated at 3-month intervals. Surgerycandidates received additional instructions just priorto and 1 week after the operation. The C1 group wasnotgiven instructionsat the timeof their examination.
All subjects were examined clinically, and periapi-cal radiographs were taken. Clinical and radiographicrecords of the S group were taken twice during activetreatment (prior to the operation and 7.4 months post-operatively), whereas both control groups were ex-amined once. The initial and pre- and postoperativecephalograms were added to the records of the S
group. A written consent form was obtained fromall patients or their guardians, and the research wasconducted in accordance with the fifth revision ofthe Helsinki Declaration.
Changes in clinical crown length were measuredwith a ruler, and the incidence of gingival recessionwas determined clinically. Plaque accumulation atthe gingival margins was evaluated using the plaqueindex, described by Silness and Loe.16 The presenceor absence of bleeding from mesial, mid-facial, distal,and lingual surfaces was noted after gentle probing ofthe gingival margin for plaque and scored accordingto the gingival index, described by Loe and Silness.17
For both indices, individual measurements were aver-aged to determine one value for each tooth, giving atotal score. To evaluate the periodontal condition,probing depth was measured from the gingival freemargin to the bottom of the pocket. Measurements>0.5 mm were rounded up to the nearest millimeter.
Table 3.
Intergroup Comparisons of Parametric Measurements
S Group (n = 36) C1 Group (n = 36) C2 Group (n = 33)
F PMean SD Mean SD Mean SD
Clinical crown (mm)Tooth #26 9.61 1.18 9.04 0.94 9.11 1.52 2.295 0.106Tooth #25 9.68 1.29 8.85 1.04 9.09 1.45 4.105 0.019*Tooth #24 9.96 1.14 9.01 1.11 9.13 1.30 6.491 0.002†
Tooth #23 9.58 1.44 8.90 0.98 9.00 1.33 3.033 0.053
Alveolar height (%)Distal aspect of tooth #26 0.58 0.05 0.59 0.04 0.58 0.06 0.241 0.786Mesial aspect of tooth #26 0.64 0.05 0.65 0.05 0.65 0.05 0.352 0.704Distal aspect of tooth #25 0.60 0.06 0.60 0.05 0.59 0.06 0.188 0.829Mesial aspect of tooth #25 0.61 0.06 0.62 0.05 0.61 0.07 0.366 0.694Mesial aspect of tooth #24 0.61 0.05 0.62 0.05 0.60 0.07 0.915 0.404Distal aspect of tooth #24 0.59 0.05 0.61 0.05 0.60 0.07 1.709 0.186Mesial aspect of tooth #23 0.65 0.05 0.67 0.04 0.65 0.05 3.088 0.050Distal aspect of tooth #23 0.59 0.06 0.62 0.04 0.59 0.05 2.588 0.080
Sulcus depth (mm)Mesial aspect of tooth #26 2.61 0.99 2.36 0.83 2.67 0.78 1.215 0.301Vestibule of tooth #26 1.35 0.53 1.28 0.51 1.45 0.79 0.705 0.497Distal aspect of tooth #26 2.61 0.80 2.36 0.76 2.94 1.00 3.940 0.022*Mesial aspect of tooth #25 2.68 0.65 2.39 0.84 2.85 0.97 2.763 0.068Vestibule of tooth #25 1.39 0.55 1.28 0.45 1.52 0.80 1.302 0.277Distal aspect of tooth #25 2.75 0.81 2.31 0.95 2.85 1.33 2.712 0.071Mesial aspect of tooth #24 2.79 0.73 2.25 0.94 2.72 1.28 3.054 0.052Vestibule of tooth #24 1.21 0.48 1.22 0.42 1.47 0.57 2.974 0.056Distal aspect of tooth #24 2.82 0.76 2.19 0.92 2.63 1.21 3.821 0.025*Mesial aspect of tooth #23 2.81 0.75 2.28 0.81 2.48 1.09 3.199 0.045*Vestibule of tooth #23 1.28 0.51 1.42 0.55 1.55 0.62 1.961 0.146Distal aspect of tooth #23 2.82 0.72 2.36 0.80 2.60 1.22 2.188 0.117
F = analysis of variance; P = level of significance; bold type = statistically significant.* P <0.05.† P <0.01.
Periodontal Implications After Orthognathic Surgery Volume 79 • Number 11
2072

To assess the overall periodontal condition of theindividual, the Ramfjord index was calculated, as de-scribed in previous studies.18-20
Mesial and distal alveolar bone levels were mea-sured from periapical radiographs for each mandibu-lar incisor with a digital caliper that was sensitive toone-hundredth of a millimeter. A decrease in alveolarheight was calculated by the ratio a/b, whereas thechanges in root length were measured by the ratioc/b (Fig. 1).
For the S group, the shape of the symphysis and theamount of incisor movement was assessed from lat-eral cephalograms (Figs. 2 and 3). The amount ofdental relapse was determined from the linear dif-ference of the perpendicular through lower incisoredge to the vertical reference line (L1?VR) and per-pendicular through B point to vertical reference line(B?VR) parameters.
The method error was calculated for radiographicmeasurements only by using the Dahlberg equa-tion.21 Second measurements were performed on10 periapical radiographs within 15 days of the firstmeasurements.
All statistical data were analyzed with a softwareprogram,† and the level of significance for all statisticaltests was predetermined at P <0.05. The significance ofthe differences among the three groups was evaluatedby one-way analysis of variance and the post hocTukey test for parametric data, whereas the Kruskal-Wallis test was used for nominal data. For evaluationswithin the S group, comparisons of parametric datawere accomplished with paired t tests, whereas nom-
inal data were compared to the Wilcoxon test. Therelationship between vertical pattern, incisor move-ments, and symphysis shape was determined withthe Pearson correlation test.
RESULTS
In the current study, the calculated method errorranged between 0.024 and 0.062. The results wereidentical in 13% of the double measurements. The testfor homogeneity of variances revealed significant dif-ferences in only four of the parameters; therefore, thestatistical evaluation continued with parametric tests.
Cephalometric measurements of the S groupshowed an increase of lower incisor-mandibular planeangle (IMPA) of 8.56�, by an incisor proclination of 3.3mm and extrusion of 0.67 mm. During the postoper-ative phase, IMPA decreased 0.14�, whereas the inci-sors retroclined 0.8 mm and intruded 0.25 mm (Table1). The increase in IMPA was 3.15� in orthodonticallytreated subjects. Comparisons of vertical pattern,symphysis morphology, and incisor movements re-vealed a positive correlation between the mandibularplane angle (SN-MP) and symphysis ratio (r = 0.331;P = 0.048). Results also indicated a negative correla-tion between SN-MP and the initial lower incisor-man-dibular plane angle (IMPAI) (r = -0.340; P = 0.043), theinitial SN-B point angle (SNB1) (r = -0.530; P = 0.001),and the preoperative SN-B point angle (SNB2) (r =-0.541; P = 0.001) parameters (Table 2).
Table 4.
Intergroup Comparisons of Nominal Measurements
S Group (n = 36) C1 Group (n = 36) C2 Group (n = 33)
x2 PMed. Min. Max. Med. Min. Max. Med. Min. Max.
Plaque indexTooth #26 1.13 0 2.75 1.38 0 2.75 1.50 0 2.75 0.752 0.687Tooth #25 1.25 0 2.75 1.38 0 3.00 1.50 0 2.75 0.019 0.991Tooth #24 1.25 0 2.75 1.25 0 3.00 1.50 0 2.75 0.100 0.951Tooth #23 1.25 0 2.75 1.25 0 2.75 1.50 0 2.75 0.598 0.742Total 1.22 0 2.75 1.35 0 2.88 1.50 0 2.75 0.294 0.863
Gingival indexTooth #26 1.00 0 2.75 1.25 0 3.00 1.50 0 2.75 6.016 0.049*Tooth #25 1.25 0 2.75 1.38 0 3.00 1.50 0 2.75 3.923 0.141Tooth #24 1.38 0 2.75 1.25 0 3.00 1.63 0.75 2.75 3.752 0.153Tooth #23 1.38 0 2.75 1.25 0 3.00 1.50 0.75 2.75 2.111 0.348Total 1.25 0 2.75 1.25 0 3.00 1.50 0.75 2.75 3.138 0.208
Ramfjord index18-20 1.80 0 4 0 0 6 1.33 0 2.75 12.707 0.002†
Med. = median; Min. = minimum; Max. = maximum; P = level of significance; bold type = statistically significant.* P <0.05.† P <0.01.
† SPSS 12.0, SPSS, Chicago, IL.
J Periodontol • November 2008 Ari-Demirkaya, Ilhan
2073

According to the intergroup comparisons, the clin-ical crown height of teeth #25 (P = 0.019) and #24 (P =0.002) showed a significant difference among thethree groups (Table 3). For tooth #25, the differencebetween S and C1 groups was statistically significant(P = 0.017). For tooth #24, subgroup comparisonsshowed significant differences between S and C1groups (P = 0.003) and between S and C2 groups(P = 0.014).
With regard to the alveolar heights, no statisticallysignificant changes were observed in any of the pa-rameters in the three groups.
Sulcus depth for the distal aspect of tooth #26 (P =0.022), the distal aspect of tooth #24 (P = 0.025), andthe mesial aspect of tooth #23 (P = 0.045) showed sig-nificant differences among the three groups (Table 3).C1–C2 comparisons were statistically significant forthe distal aspect of tooth #26 (P = 0.017). However,for the distal aspect of tooth #24 and the mesial aspect
of tooth #23, subgroup comparisons revealed signif-icant differences between S and C1 groups (P = 0.022and P = 0.036, respectively).
No significant difference among the three groupswas detected for the plaque index. For the gingivalindex, the only significant intergroup difference wasfound for tooth #26 (P = 0.049). The results alsoshowed significant intergroup differences for theRamfjord index (P = 0.002).18-20 Details of the inter-group comparisons are shown in Table 4.
A comparison of preoperative and postoperativeclinical and radiographic parameters of the S grouprevealed that only the mesial surface of tooth #23showed a significant change in the alveolar heightratio (-0.02; P = 0.038) and sulcus depth (-0.37mm; P = 0.01). No other significant changes betweenpre- and postoperative measurements were detected.The intragroup comparisons are shown in Tables 5and 6.
Table 5.
Comparisons of Pre- and Postoperative Measurements Within the S Group (parametric data)
Preoperative Postoperative
t PMean SD Mean SD
Clinical crown (mm)Tooth #26 9.61 1.18 9.54 1.42 0.439 0.664Tooth #25 9.68 1.29 9.63 1.21 0.259 0.797Tooth #24 9.96 1.14 9.72 1.29 1.448 0.157Tooth #23 9.58 1.44 9.61 2.02 -0.083 0.934
Alveolar height (%)Distal aspect of tooth #26 0.58 0.05 0.59 0.05 -0.229 0.820Mesial aspect of tooth #26 0.64 0.05 0.62 0.05 2.004 0.053Distal aspect of tooth #25 0.60 0.06 0.59 0.05 0.767 0.448Mesial aspect of tooth #25 0.61 0.06 0.60 0.05 0.696 0.491Mesial aspect of tooth #24 0.61 0.05 0.60 0.05 1.069 0.293Distal aspect of tooth #24 0.59 0.05 0.59 0.05 0.579 0.566Mesial aspect of tooth #23 0.65 0.05 0.63 0.05 2.151 0.038*Distal aspect of tooth #23 0.59 0.06 0.58 0.06 1.473 0.150
Sulcus depth (mm)Mesial aspect of tooth #26 2.61 0.99 2.47 0.70 0.758 0.454Vestibule of tooth #26 1.35 0.53 1.25 0.44 0.894 0.378Distal aspect of tooth #26 2.61 0.80 2.44 0.61 1.063 0.295Mesial aspect of tooth #25 2.68 0.65 2.53 0.61 1.339 0.189Vestibule of tooth #25 1.39 0.55 1.25 0.50 1.221 0.230Distal aspect of tooth #25 2.75 0.81 2.61 0.84 0.896 0.377Mesial aspect of tooth #24 2.79 0.73 2.71 0.80 0.572 0.571Vestibule of tooth #24 1.21 0.48 1.26 0.45 0.529 0.600Distal aspect of tooth #24 2.82 0.76 2.53 0.75 1.768 0.086Mesial aspect of tooth #23 2.81 0.75 2.44 0.65 2.714 0.01†
Vestibule of tooth #23 1.28 0.51 1.31 0.52 -0.255 0.800Distal aspect of tooth #23 2.82 0.72 2.69 0.75 0.875 0.387
t = paired t test; P = level of significance; bold type = statistically significant.* P <0.05.† P <0.01.
Periodontal Implications After Orthognathic Surgery Volume 79 • Number 11
2074

DISCUSSION
The thin nature of the alveolar housing in the mandi-bular anterior area makes it difficult to predict theperiodontal implications of excessive incisor move-ments. Although some studies5,6,11,22-26 reported anincreased risk for breakdown of gingival attachment,other studies24,27-29 found no association between or-thodontic tooth movementand periodontal symptoms,such as increase in clinical crown height, gingival re-cession, or attachment loss.
In one such study from Yared et al.,30 no correlationamong labial incisor movement, recession, gingivalindex, and plaque index was reported. Similarly, a his-tologic study6 in monkeys showed that an incisor pro-clination of 2.9 mm did not result in periodontalbreakdown, provided the gingival tissue was kept freeof inflammation. The current study supports these find-ings; an incisor proclination of 3.3 mm had no adverseeffect on the periodontal status of the surgery patients.Only one tooth displayed a 2% decrease in alveolarheight and a 0.37-mm reduction in sulcus depth, whichcould be explained by minor positional changes oflower incisors during the intermaxillary fixation period.
Clinical crown height and plaque, gingival, andRamfjord indices did not differ significantly betweenpre- and postoperative measurements. The reasonfor this may have been that the amount of decompen-sation in the lower incisor region was within tolerancelevels and did not cause any periodontal problem inthe short-term. The dental awareness of the groupalso may have been increased by the extra oral hy-giene instructions given before and after the opera-tion. Finally, factors like gingival thickness and
morphology, alveolar thickness,12,30,31 the shape ofthe symphysis,23,31,32 as well as the direction and ex-tent of incisor movement12 contribute to the final con-dition of periodontal structures.
Changes in the alveolar bone height were deter-mined with a relative measuring technique, similarto those described by Bjorn et al. (Fig. 1).33 Althoughthe accuracy of this method can be affected by rootlength changes, only 2% of the subjects in the S andC2 groups presented with resorption >2 mm.
The shape of the symphysis and the amount ofproclination in surgery patients were assessed fromlateral cephalograms. According to the Pearson anal-ysis, the shape of the symphysis gets narrower andlonger with increasing vertical height (Table 2). Thecorrelations also indicated that long-faced individualsoften present with a steep IMPA, which, in turn, makesexcessive proclination necessary. Consequently, itcan be hypothesized that surgical patients with in-creased vertical height are more likely to develop peri-odontal problems compared to normal or short-facedsubjects.
Aside from the marked proclination of mandibularincisors, thesubsequent retroclinationdue toapossiblerelapsemayalsoresult inperiodontalbreakdownof thisregion with an already reduced adaptability. In a studyof 516 clinical patients, Geiger and Wassermann34 re-ported thatperiodontaldestructionwasassociatedwiththe lingual inclination of the mandibular incisors, ratherthan with a labial inclination. Because a postoperativedental relapse of 0.8 mm was found in this study, onecan assume that the periodontal changes were mostlyrelated to the preoperative incisor movements.
Table 6.
Nominal Data Comparisons Within the S Group
Preoperative Postoperative
z PMed. Min. Max. Med. Min. Max.
Plaque indexTooth #26 1.13 0 2.75 1.25 0 3.00 -0.143 0.886Tooth #25 1.25 0 2.75 1.00 0 3.00 -1.444 0.149Tooth #24 1.25 0 2.75 1.00 0 3.00 -0.914 0.361Tooth #23 1.25 0 2.75 1.00 0 3.00 -0.589 0.556Total 1.22 0 2.75 1.10 0 3.00 -0.876 0.381
Gingival indexTooth #26 1.00 0 2.75 1.25 0 2.75 -0.382 0.702Tooth #25 1.25 0 2.75 1.25 0 2.75 -0.330 0.741Tooth #24 1.38 0 2.75 1.00 0 2.75 -0.880 0.379Tooth #23 1.38 0 2.75 1.00 0 2.75 -0.580 0.562Total 1.25 0 2.75 1.13 0 2.75 -0.505 0.614
Ramfjord index18-20 1.80 0 4 2 0 3.33 -1.308 0.191
Med. = median; Min. = minimum; Max. = maximum; z = Wilcoxon signed-rank test; P = level of significance.
J Periodontol • November 2008 Ari-Demirkaya, Ilhan
2075

Generally, no relationship between postoperativerelapse movements and crestal alveolar bone levelswas found in the short-term. However, a retrospectivestudy35 pointed out that attachment and alveolar boneloss might increase the tendency for orthodontic re-lapse in the long-term.
The comparisons between the surgery and the twocontrol groups revealed significant differences in allparameters except the alveolar height and the plaqueindex. Although surgical patients presented with in-crease in IMPA nearly three times as much as inthe orthodontically treated group (8.56� and 3.15�,respectively), they showed lower scores for sulcusdepth, gingival index, and plaque index comparedto orthodontically treated patients. This may havebeen the result of controlled oral hygiene within theS group.
Nevertheless, the Ramfjord scores of the S groupwere higher than the C2 group, pointing to the greaterimpact of presurgical decompensation on generaloral hygiene than standard orthodontic treatment.Extra attachments (crimpable hooks and intermaxil-lary elastics) commonly used in surgical cases mayalso have contributed to increased plaque accumula-tion, increasing the Ramfjord index scores.
Comparing both control groups, although subjectswithout braces presented with slightly better periodon-tal conditions than orthodontically treated patients, thedifferences were not significant. This result may seemunexpected at first, because orthodontic appliancesare often considered risk factors for deteriorating gen-eral oral hygiene, by increasing plaque accumulation.However, the questionnaires used during patient selec-tion were intended to exclude subjects with low dentalawareness from the study.Thismethod of selection, to-gether with the hygiene instructions that the C2 groupreceived throughout the study, may explain the similarperiodontal conditions between the two control groups.In this regard, our findings confirmed results from sim-ilarstudies22,29thatstandardorthodontictreatmenthasminimal effect on the general condition of periodontalstructures.
CONCLUSIONS
The current study demonstrated that there was asignificant difference among the preoperative peri-odontal condition of class III surgery patients, otherorthodontically treated patients, and non-treated sub-jects. Surgical patients presented with periodontalstructures in the worst condition; the best were foundin non-treated subjects. However, there is no conclu-sive evidence that presurgical dental decompensa-tion, up to 3.5 mm, and the subsequent relapsemovementsaffected theperiodontalconditionofman-dibular setback patients negatively in the short-term.
ACKNOWLEDGMENT
The authors report no conflicts of interest related tothis study.
REFERENCES1. Moyers RE. Force systems and tissue responses to
forces in orthodontics and facial orthopedics. In:Marshall DK, Mitera MC, eds. Handbook of Orthodontics,4th ed. Chicago: Year Book Medical Publishers; 1988:326.
2. Bailey LJ, Cevidanes LHS, Proffit WR. Stability andpredictability of orthognathic surgery. Am J OrthodDentofacial Orthop 2004;126:273-277.
3. Proffit WR. Combined surgical and orthodontic treat-ment. In: Rudolph P, ed. Contemporary Orthodontics,3rd ed. St. Louis: Mosby; 2000:705.
4. Dorfman HS. Mucogingival changes resulting frommandibular incisor tooth movement. Am J Orthod1978;74:286-298.
5. Wainwright WM. Faciolingual tooth movement: Itsinfluence on the root and cortical plate. Am J Orthod1973;64:278-303.
6. Wingard CE, Bowers GM. The effects on facial bonefrom facial tipping of incisors in monkeys. J Periodon-tol 1976;47:450-455.
7. Handelman CS. The anterior alveolus: Its importancein limiting orthodontic treatment and its influence onthe occurrence of iatrogenic sequelae. Angle Orthod1996;66:95-111.
8. Sadowsky C, BeGole EA. Long-term effects of ortho-dontic treatment on periodontal health. Am J Orthod1981;80:156-172.
9. Ruf S, Hansen K, Pancherz H. Does orthodontic procli-nation of lower incisors in children and adolescentscause gingival recession? Am J Orthod DentofacialOrthop 1998;114:100-106.
10. Djeu G, Hayes C, Zawaideh S. Correlation betweenmandibular central incisor proclination and gingivalrecession during fixed appliance therapy. Angle Or-thod 2002;72:238-246.
11. Steiner GG, Pearson JK, Ainamo J. Changes of themarginal periodontium as a result of labial tooth move-ment in monkeys. J Periodontol 1981;52:314-320.
12. Wennstrom JL. Mucogingival considerations in ortho-dontic treatment. Semin Orthod 1996;2:46-54.
13. Artun J, Krogstad O. Periodontal status of mandibularincisors following excessive proclination: A study inadults with surgically treated mandibular prognathism.Am J Orthod Dentofacial Orthop 1987;91:225-232.
14. Foushee DG, Moriarty JD, Simpson DM. Effects ofmandibular orthognathic treatment on mucogingivaltissues. J Periodontol 1985;56:727-733.
15. Cheung LK, Lo J. The long-term clinical morbidity ofmandibular step osteotomy. Int J Adult OrthodonOrthognath Surg 2002;17:283-290.
16. Silness J, Loe H. Periodontal disease in pregnancy II.Correlation between oral hygiene and periodontalcondition. Acta Odontol Scand 1964;22:121-135.
17. Loe H, Silness J. Periodontal disease in pregnancy I.Prevalence and severity. Acta Odontol Scand 1963;21:533-551.
18. Ramfjord SP. Indices for prevalence and incidence ofperiodontal disease. J Periodontol 1959;30:51.
19. Ramfjord SP. The periodontal disease index (PDI).J Periodontol 1967;38:602-610.
Periodontal Implications After Orthognathic Surgery Volume 79 • Number 11
2076

20. Carranza FA, Newman MG. Epidemiology of gingivaland periodontal disease. In: Fermin A, Carranza, Jr.,Newman MG, eds. Clinical Periodontology, 8th ed.Philedelphia: W.B. Saunders; 1996:61-81.
21. Dahlberg G. Statistical Methods for Medical and Bio-logical Students. London: George Allen & Unwin;1940:122-132.
22. Hamp SE, Lundstrom F, Nyman S. Periodontal con-ditions in adolescents subjected to multiband ortho-dontic treatment with controlled oral hygiene. Eur JOrthod 1982;4:77-86.
23. Wehrbein H, Bauer W, Diedrich P. Mandibular incisors,alveolar bone, and symphysis after orthodontic treat-ment. A retrospective study. Am J Orthod DentofacialOrthop 1996;110:239-246.
24. Artun J, Grobety D. Periodontal status of mandibularincisors after pronounced orthodontic advancementduring adolescence: A follow-up evaluation. Am JOrthod Dentofacial Orthop 2001;119:2-10.
25. Batenhorst KF, Bowers GM, Williams JE Jr. Tissuechanges resulting from facial tipping and extrusion ofincisors in monkeys. J Periodontol 1974;45:660-668.
26. Wennstrom JL, Lindhe J, Sinclair F, Thilander B. Someperiodontal tissue reactions to orthodontic tooth move-ment in monkeys. J Clin Periodontol 1987;14:121-129.
27. Zhang XY, Liu DX, Gao X, Wang XY, Xi R. Periodontalstatus of mandibular incisors after pronounced ortho-dontic advancement during adolescence (text in Chi-nese, abstract in English). Shanghai Kou Qiang Yi Xue2002;11:297-299.
28. Pearson LE. Gingival height of lower central incisors,orthodontically treated and untreated. Angle Orthod1968;38:337-339.
29. Eliasson L, Hugoson A, Kurol J, Siwe H. The effects oforthodontic treatment of periodontal tissues in patientswith reduced periodontal support. Eur J Orthod 1982;4:1-9.
30. Yared KF, Zenobio EG, Pacheco W. Periodontal statusof mandibular central incisors after orthodontic procli-nation in adults. Am J Orthod Dentofac Orthoped2006;130:6.e1-6.e8.
31. Diedrich P. Problems and risks in the movement of themandibular anterior teeth (in German). Fortschr Kie-ferorthop 1995;56:148-156.
32. Mulie RM, Hoeve AT. The limitations of tooth move-ments within the symphysis studied with laminagra-phy and standardized occlusal films. J Clin Orthod1976;10:882-899.
33. Bjorn H, Halling A, Thyberg H. Radiographic assessmentof marginal bone loss. Odontol Revy 1969;20:165-179.
34. Geiger AM, Wasserman BH. Relationship of occlusionand periodontal disease. Part IX – Incisor inclinationand periodontal status. Angle Orthod 1976;46:99-110.
35. Sharpe W, Reed B, Subtelny JD, Polson A. Orthodonticrelapse, apical root resorption, and crestal alveolar bonelevels. Am J Orthod Dentofacial Orthop 1987;91:252-258.
Correspondence: Dr. Isil Ilhan, Department of Orthodon-tics, Faculty of Dentistry, Marmara University, GuzelbahceSok. No. 6 Nisantasi, Istanbul, Turkey. E-mail: [email protected].
Submitted November 7, 2007; accepted for publicationMay 8, 2008.
J Periodontol • November 2008 Ari-Demirkaya, Ilhan
2077