-
J Clin Pathol 1986;39:1245-1249
Effects of N-methyl-thiotetrazole cephalosporin onhaemostasis in
patients with reduced serum vitaminK1 concentrationsI J MACKIE, K
WALSHE, H COHEN, P McCARTHY,* M SHEARER,*S D SCOTT,** S J KARRAN,**
S J MACHIN
From the Department ofHaematology, Middlesex Hospital, London,
the *Department ofHaematology, Guy'sHospital, London, and the
**Department ofSurgery, Southampton General Hospital
SUMMARY Two patients with low random serum vitamin K,
concentrations but with normal pro-thrombin times and normal
biological assays of the vitamin K dependent coagulation proteins
weretreated with an N-methyl-thiotetrazole cephalosporin
(cefotetan) postoperatively. Four to six dayslater both patients
developed a prolonged prothrombin time and a noticeable and
specific loweringof the clotting activities of factors II, VII, IX
and X, though the serum vitamin K, concentrationsremained
unchanged. Crossed immunoelectrophoresis of prothrombin showed the
appearance of asecond peak corresponding to descarboxyprothrombin
(PIVKA II). These abnormalities correctedafter vitamin K
administration. These data are consistent with the hypothesis that
cephalosporinswith an N-methyl-thiotetrazole side chain inhibit the
hepatic utilisation of vitamin K but that thisonly causes
hypoprothrombinaemia when liver reserves of vitamin K are low.
Cephalosporin antibiotics have been known for someyears to be
associated with reduced synthesis of thevitamin K dependent
clotting factors II, VII, IX andX and occasionally to be
responsible for clinicalbleeding episodes.' Clinical reports have
usuallyimplicated cephalosporins with N-methyl-thiotetrazole (NMTT)
side chains such as lat-amoxef,2 3 cefamandole,4 and cefoperazone.'
Theseevents occurred most in patients with renal failure,those who
are severely malnourished with chronicgastrointestinal disease, or
those who had beenreceiving prolonged parenteral nutrition.6 It has
beensuggested that NMTT cephalosporins may cause vita-min K
deficiency by suppressing the vitamin K pro-ducing micro-organisms
of the colonic microflora.78Contradicting this hypothesis is the
lack of evidencethat menaquinones (vitamin K2) can be absorbedfrom
the colon and the fact that other antibiotics suchas tetracyclines,
which also strongly suppress thebowel flora, are not known to be
associated with vita-min K deficiency. Another hypothesis is that
theNMTT side chain directly inhibits the vitamin Kdependent
y-carboxylation of clotting factors in theliver cell.9 10
Cefotetan (ICI) is a new compound in the cepha-mycin subdivision
of the cephalosporins with anAccepted for publication 21 May
1986
NMTT side chain." We investigated the effects ofthis new
cephalosporin on vitamin K, metabolismand hepatic synthesis of the
vitamin K dependentcoagulation factors after parenteral nutrition
givenover several days to two patients with a normal pro-thrombin
time and normal factor II, VII, IX and Xassays before treatment.
Both patients, however, hadsubnormal serum vitamin K,
concentrations beforetreatment was started.
Patients
CASE 1An 81 year old woman presented with a two monthhistory of
generalised abdominal pain and vomitingover the previous week. On
admission (day 1), a diag-nosis of a strangulated left femoral
hernia was madeand operative repair was carried out that day.
Pro-phylactic antibiotic cover was started with intra-venous
cefotetan (2 g) given every 12 hours; treatmentwas continued for
four days. She gave a history ofrecent weight loss, but routine
liver function and renalfunction tests were within normal limits.
On day four,after six doses of cefotetan, treatment was stoppedand
10 mg of vitamin K, was given intramuscularlylater that day when
the prothrombin time was foundto be prolonged.
1245
copyright. on M
arch 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.39.11.1245 on 1 N
ovember 1986. D
ownloaded from
http://jcp.bmj.com/
-
Mackie, Waishe, Cohen, McCarthy, Shearer, Scott, Karran,
MachinCASE 2A 74 year old man presented with a 24 hour history
ofgeneralised abdominal pain that later localised to theright iliac
fossa. On admission (day 1), peritonitis wasdiagnosed, and at
operation that day a perforatedgangrenous appendix was removed.
Prophylacticantibiotic cover was started preoperatively with
intra-venous cefotetan (2 g) given every 12 hours and con-tinued as
treatment because free pus was found atoperation. Liver function
and renal function testswere within normal limits on admission. On
day 6,after ten doses of cefotetan, treatment was stoppedand 10 mg
of vitamin K, was then given intra-muscularly because he was noted
to have a prolongedprothrombin time.
Methods
Blood was collected by clean venepuncture into plainglass tubes
for serum, or 0-106M trisodium citrate(9:1) for plasma.Serum
concentrations of Vitamin K1 were mea-
sured by high performance liquid chromatographywith dual
electrode electrochemical detection, asdescribed previously, 12
except that quantification wasmade by reference to an internal
standard(menaquinone-6) added at the extraction stage. Theinterrun
coefficient of variation for 37 replicate anal-yses of a plasma
pool (mean concentration 1100pg/ml) carried out over six months was
11-5%.
Prothrombin time was measured manually usingthe human brain
Manchester comparative reagent.Factor V and IX coagulant assays
were performed byone stage methods using congenitally deficient
sub-strate plasma.'3 One stage factor VII assay was car-ried out
with an artificially depleted substrate plasma.
Factor X was assayed using Russell's viper venomand "Diagen"
factor X deficient plasma (DiagnosticReagents Ltd). Prothrombin was
measured by a twostage clotting assay13 or by a chromogenic
substrateassay using Ecarin (Pentapharm Ltd) and S2238(Kabi Vitrum
Ltd).14 Factors II and IX antigenvalues were measured by
immunoelectrophoresis,using suitable antisera (Dako Ltd,
DiagnosticaStago Ltd). All factor II, VII, IX and X assays
werestandardised against a commercial reference plasma(Immuno Ltd)
with a normal range of 50-200 U/dl.Crossed immunoelectrophoresis of
prothrombinwas performed,16 using calcium lactate buffer toseparate
descarboxyprothrombin (PIVKA-II) fromy-carboxylated
prothrombin.
Results
Tables I and 2 show the results of assays for plasmacoagulation
factors and serum vitamin K,. Beforetreatment with antibiotics both
patients had normalprothrombin times (13-7 and 13-7 seconds,
normalrange 12-14 seconds) and normal activities in the bio-logical
assays for the vitamin K dependent clottingfactors II, VII, IX and
X, but serum concentration ofvitamin K1 (54 and 78 pg/ml) were
substantiallyreduced compared with those in the range
(170-680pg/mI) in 45 normal fasting adults using the
sameelectrochemical method. After four and six days oftreatment
with cefotetan the serum vitamin K, con-centrations remained
unchanged (52 and 73 pg/mI),but both patients developed a severe
hypo-prothrombinaemia, evidenced both by an increasedprothrombin
time (34.7 and 20-5 seconds) andclotting assays that showed a
specific lowering ofthe four vitamin K dependent factors. Hypo-
Table 1 Coagulation results (case 1) after six 12 hourly doses
ofcefotetan and then six and 24 hours after 10 mg vitamin K,given
intramuscularly
Vitamin K, Prothrombin V:C - VII:C IX:C IX:Ag X:C II:(C II Ag
Ecarin IIDay (pg/ml) time (seconds) (Uldi) (Uldl) (Uldi) (Uldi)
(Uldi) (Uldi) (Uldi) (Uldi)
1 54 13-7 52 59 180 76 77 87 78 774 52 34.7 47 3 2 46 36 30 59
72
+ 6 hours 1700 38-2 54 39 38 75 32 21 108 77+24 hours 36000 14-4
90 68 160 51 32 33 99 72
Table 2 Coagulation results (case 2) after ten 12 hourly doses
ofcefotetan and then 12 hours after 10 mg vitamin K,
givenintramuscularly
Vitamin K, Prothrombin V:C VII:C IX:C IX:Ag X:C II:C II Ag Ecars
IIDay (pg/ml) time (seconds) (Uldi) (Uldi) (Uldl) (Uldi) (UldI)
(Uldi) (Uldi) (Uldi)
1 78 13-7 50 65 150 88 90 50 108 636 73 20 5 72 37 38 80 18 29
135 77
+ 12 hours 27900 14 2 61 47 126 90 59 26 132 70
1246
copyright. on M
arch 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.39.11.1245 on 1 N
ovember 1986. D
ownloaded from
http://jcp.bmj.com/
-
Effects of N-methyl-thiotetrazole cephalosporin on
haemostasis
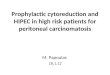
Figure Crossed immunoelectrophoresis ofprothrombin (case 1) Top
gel: day Ibefore treatment with Cefotetan. Middle gel: day 4 after
six doses of Cefotetan.Bottom gelt 24 hours after 10 mg vitamin
K1.
1247
copyright. on M
arch 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.39.11.1245 on 1 N
ovember 1986. D
ownloaded from
http://jcp.bmj.com/
-
Mackie, Waishe, Cohen, McCarthy, Shearer, Scott, Karran,
Machin
prothrombinaemia was most severe in the patienthaving the lower
serum vitamin K1, a serum concen-tration that was less than one
third the lower limit ofthe normal range. In this patient the
reduction inclotting factors was most noticeable for factors VIIand
IX (half lives four to six hours and 24 hours,respectively) than
for factors X and II, which havelonger circulating half lives (48
hours and 60 hours,respectively). Over the same period the clotting
activ-ity of factor V, which is also synthesised in the hepa-tocyte
but is not a vitamin K dependent protein, didnot change appreciably
in either patient. Factor IIactivity measured by the Ecarin method
and factors IIand IX antigenic activity, however, did not change
ineither patient. The Ecarin assay measured
bothdescarboxyprothrombin (PIVKA-II) and the biologi-cally active
fully y-carboxylated prothrombin: thesimilar values before and
after treatment withcefotetan indicate that the fall in biological
activity offactor II is due to an impaired vitamin K
dependenty-carboxylation rather than an impaired hepatic syn-thesis
of the core protein. This was confirmed bycrossed
immunoelectrophoresis, which showed thecharacteristic faster
migrating peak of non-carboxylated species of prothrombin after
treatmentwith cefotetan and a single peak of normal pro-thrombin
before treatment (case 1) (figure). Similarfindings were found in
case 2 by crossed immu-noelectrophoresis (results not shown).The
effect of 10 mg of vitamin K, given by intra-
muscular injection was most noticeable, producingafter 12 to 24
hours a substantial normalisation of theprolonged prothrombin time
and increased circu-lating concentration of biologically active
vitamin Kdependent factors.
Discussion
Vitamin K deficiency is usually identified by the pres-ence of a
prolonged prothrombin time that correctsafter vitamin K
administration. In vitamin Kdeficiency, or in the presence of
vitamin K antagonists(such as the coumarin anticoagulant warfarin),
thepostribosomal y-carboxylation of certain glutamicacid residues
of the vitamin K dependent clotting fac-tors (factors VII, IX, X
and II, proteins C and S) isinhibited.'7 Non y-carboxylated vitamin
Kdependent proteins are unable to bind calcium ionsand are inactive
in the blood coagulation cascade."8Patients with severe vitamin K
deficiency have abnor-mal inactive non -y-carboxylated proteins in
theirblood. These abnormal proteins have been calledPIVKAs or
descarboxyproteins.A feature of the investigations in these two
patients
was the measurement of their plasma concentrationsof vitamin K,
(phylloquinone). Until recently, such
measurements have been hampered by the analyticalproblems
associated with the detection of the low cir-culating
concentrations in blood: consequently, verylittle is known about
plasma concentrations of vita-min K in health and disease and
nothing about thoseconcentrations that may relate to an overt or
mar-ginal deficiency of vitamin K. Using a recently devel-oped
assay, based on high performance liquidchromatography with
electrochemical detection'2 butrefined for use with an internal
standard, the normalrange of plasma vitamin K, in 45 healthy
fastingadults was 170-680 pg/ml (median 372, mean 412pg/ml). The
plasma values of vitamin K1 in thepatients (54 and 52 pg/ml in case
1, 78 and 73 pg/mI incase 2) were notable in several respects.
Firstly, theywere well below the normal range; secondly, they
didnot change during the period of the study and;thirdly, although
low, the plasma vitamin K1 wassufficiently high to maintain normal
plasma concen-trations of the vitamin K dependent clotting
factorsuntil they were treated with cefotetan. The relationbetween
plasma concentrations of vitamin K1 and tis-sue reserves remains to
be established, but it seemsreasonable to assume that, as with
other fat solublevitamins, low plasma concentrations reflect low
bodystores. It is likely, therefore, that both these patientshad
low vitamin K reserves in the liver, which is thesite of synthesis
of the vitamin K dependent clottingfactors. Both patients had a
chronically poor nutri-tional state, and in the week or so before
hospitaladmission, their dietary intake had furtherdiminished due
to generalised abdominal pain andvomiting.
It has previously been suggested that cepha-losporins containing
the NMTT side chain such aslatamoxef and cefamandole cause
prolongation of theprothrombin time by inhibiting the action of the
vita-min K 2,3-epoxide reductase enzyme."9 This wouldseem to occur
after in vivo degradation of the anti-biotic and release of the
NMTT side chain.9 10 Thishas been confirmed using in vitro rat
liver systemsshowing partial inhibition of the epoxide
reductaseenzyme similar to the action of the oral
anticoagulantwarfarin.20 Previous studies with cefotetan in
wellnourished subjects with normal serum vitamin K,concentrations,
however, have shown no pro-longation in the prothrombin time or
decreased syn-thesis of the vitamin K dependent
coagulationfactors.2" In vivo degradation of the NMTT sidechain
occurs less readily in cefotetan than otherNMTT cephalosporins such
as latamoxef.22 Thusonly in clinical situations in which there is
chronicvitamin K deficiency such as elderly patients with apoor
dietary intake, patients receiving prolonged par-enteral feeding
without vitamin K supplements,23 orpatients with chronic
gastrointestinal malabsorption
1248
copyright. on M
arch 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.39.11.1245 on 1 N
ovember 1986. D
ownloaded from
http://jcp.bmj.com/
-
Effects of N-methyl-thiotetrazole cephalosporin on haemostasis
1249states24 is cefotetan likely to inhibit the vitamin Koxidation
reduction cycle and cause decreasedy-carboxylation of the K
dependent proteins. Obvi-ously in patients receiving warfarin and
antibioticswith a cephalosporin containing the NMTT sidechain,
there is a risk of a synergistic reaction with asudden decreased
y-carboxylation of the vitamin Kdependent factors and excessive
prolongation of theprothrombin time.
Although both these patients developed a pro-longed prothrombin
time, neither had any clinicalbleeding episode or spontaneous
bruising. OtherNMTT containing cephalosporins,
particularlylatamoxef2 3 have often been associated with a
clin-ical bleeding diathesis. These antibiotics, as well
asinhibiting the vitamin K epoxide-reductase activity;also
appreciably inhibit platelet function and prolongthe bleeding time
at standard therapeutic doses.25 Ce-fotetan does not inhibit
platelet function or prolongthe bleeding time21 and is thus much
less likely tocause bleeding events.
We thank Dr R Bax (ICI, Alderley Edge, Cheshire)for helpful
discussion and comments on this manu-script.
References
I Andrassy K, Bechtold H, Ritz E. Hypoprothrombinaemia causedby
cephalosporins. J Antimicrob Chemother 1985;15:133-6.
2 Weitekamp MR, Aber RC. Prolonged bleeding times and bleed-ing
diathesis associated with moxalactam administration.JAMA
1983;249:69-71.
3 Morris DL, Fabricius PJ, Ambrose NS, Scammell B, BurdonDW,
Keighley MRB. A high incidence of bleeding is observedin a trial to
determine whether addition of metronidazole isneeded with latamoxef
for prophylaxis in colorectal surgery. JHosp Infect
1984;5:398-408.
4 Clancy CM, Glew RH. Hypoprothrombinaemia and bleeding
as-sociated with cephamandole. Lancet 1983;i:250.
5 Weitekamp MR, Caputo GM, Al-Mondhiry HAB, Aber RC.The effects
of latamoxef, cefotaxime and cefoperazone onplatelet function and
coagulation in normal volunteers. J Anti-microb Chemother
1985;16:95-101.
6 Smith CR, Lipsky JJ. Hypoprothrombinaemia and platelet
dys-function caused by cephalosporin and oxalactam antibiotics.
JAntimicrob Chemother 1983;11:496-9.
7 Bang NU, Tessler SS, Heidenreich RO, Marks CA, Mattler
LE.Effects of oxalactam on blood coagulation and platelet
func-tion. Rev Infect Dis 1982;4 (supplement):5546-54.
8 Hochman R, Clark J, Rolla A, Thomas S, Kaldany A, D'Elia
J.Bleeding in patients with infections. Arch Intern
Med1982;142:1440-2.
9 Lipsky JJ. N-Methyl-thiotetrazole inhibition of the gamma
car-boxylation of glutamic acid: possible mechanism for
antibioticassociated hypoprothrombinaemia. Lancet 1983;i:192-3.
10 Lipsky JJ. Mechanism of the inhibition of the y-carboxylation
ofglutamic acid by N-methyl-thiotetrazole-containing anti-biotics.
Proc Nat! Acad Sci 1984;81:2893-7.
11 Phillips I, King A, Shannon K, Warren C. Cefotetan:
in-vitroantibacterial activity and susceptibility to B-lactamases.
J Anti-microb Chemother 1983;11 (Suppl A): 1-9.
12 Hart JP, Shearer MJ, McCarthy PT. Enhanced sensitivity for
thedetermination of endogenous phylloquinone (vitamin Kj) inplasma
using high-performance liquid chromatography withdual-electrode
electrochemical detection. Analyst 1985;110:1181-4.
13 Thompson J. Blood coagulation and haemostasis.
Edinburgh:Churchill Livingstone, 1980.
14 Bergstrom K, Egberg N. Determination of vitamin K
sensitivecoagulation factors in plasma. Studies of three methods
usingsynthetic chromogenic substrates. Thromb Res
1978;12:531-47.
15 Laurell CB. Quantitative estimation of proteins by
electro-phoresis in agarose gel containing antibodies. Anal
Biochem1966;15:45-68.
16 Laurell CB. Antigen-antibody crossed
immunoelectrophoresis.Anal Biochem 1965;10:358-62.
17 Friedman PA. Vitamin K dependent proteins. New EngI J
Med1984;310:1458-60.
18 Friedman PA, Shia MA, Gallop PM, Griep AE. Vitamin
K-dependent y-carbon-hydrogen bond cleavage and non-mandatory
concurrent carboxylation of peptide-boundglutamic acid residues.
Proc Natl Acad Sci USA1979;76:3 126-9.
19 Bechtold H, Andrassy K, Jahnchen E, et al. Evidence for
im-paired hepatic vitamin K, metabolism in patients treated
withN-methyl-thiotetrazole cephalosporins. Thromb Haemostas1984;51
(3):358-61.
20 Uotila L, Suttie JW. Inhibition of vitamin K-dependent
carbox-ylase in vitro by cefamandole and its structural analogues.
JInfect Dis 1983;148:571-8.
21 Machin SJ, Bowcock S, Mackie IJ, Ho D, Pozniak A.
Hae-mostatic parameters: pilot study with cefotetan compared
withother antibiotics. In: Lode H, Periti P, Strachan CJL, eds.
Ce-fotetan, a long acting antibiotic. Edinburgh: Churchill
Liv-ingstone 1985:138-42.
22 Wise R, Dent J. Stability of B-lactam antibiotics containing
N-methylthiotetrazole side chain. Lancet 1983;ii:624-5.
23 Hands LJ, Royle GT, Kettlewell MGW. Vitamin K requirementsin
patients receiving total parenteral nutrition. Br J
Surg1985;72:665-7.
24 Krasinski SD, Russell RM, Furie BC, Kruger SF, Jacques
PF,Furie B. The prevalence of vitamin K deficiency in
chronicgastrointestinal disorders. Am J Clin Nutr
1985;41:639-43.
25 Bowcock S, Mackie IJ, Ho D, Moulsdale M, Billings P,
MachinSJ. Effects of various doses of Latamoxef on haemostasis.
JHosp Infect (in press).
Requests for reprints to: Dr SJ Machin, Department of
Hae-matology, Middlesex Hospital, Mortimer Street, LondonWI,
England.
copyright. on M
arch 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.39.11.1245 on 1 N
ovember 1986. D
ownloaded from
http://jcp.bmj.com/