Embed Size (px)
Citation preview
DP
CD
tmt
p
vc
H
3a
c
ato
Clinical Therapeutics/Volume 35, Number 5, 2013
Effects of Injectable HP�CD-Diclofenac on the Humanelayed Rectifier Potassium Channel Current In Vitro and onroarrhythmic QTc In Vivo
Daniel B. Carr, MD1; Tara McDonnell Moorehead, BA1; Annie Bouchard, MSc2;raig R. Sprenger, MD3; Douglas A. Hamilton, MBA1; Eric Lang, MD1;onna Madden, MS1; Peter G. Lacouture, PhD4; and Curtis Wright IV, MD, MPH1
1Javelin Pharmaceuticals, Inc (now Hospira, Inc), Cambridge, Massachusetts; 2IPS Therapeutique,Sherbrooke, Quebec, Canada; 3Cetero Research, Fargo, North Dakota; and 4Hospira, Inc, Lake Forest,Illinois
sa
ABSTRACTBackground: Novel formulations and administra-
ion routes of established drugs may result in higheraximum concentrations or total exposures and po-
entially cause previously unrecognized adverse events.Objective: This study evaluated the proarrhythmic
otential of hydroxypropyl-�-cyclodextrin (HP�CD)-diclofenac, a novel injectable diclofenac formulation solubi-lized with hydroxypropyl-�-cyclodextrin (HP�CD), onentricular electrical conduction in preclinical and clini-al models.
Methods: We assessed the effects of diclofenac,P�CD, and HP�CD-diclofenac on the human delayed
rectifier potassium channel (IKr) using human embryonickidney (HEK) 293 cells transfected with a human ether-à-go-go–related gene (hERG) using whole-cell patch-clamp. In a single-dose, active- and placebo-controlled,4-period crossover, thorough QT in vivo study, 70healthy volunteers (mean age, 23.3 years; range, 18–49years; 55.75% male) received HP�CD-diclofenac at7.5- and 75-mg doses, inactive vehicle (placebo), and anctive control (moxifloxacin).
Results: In vitro, diclofenac produced no statisti-ally significant effect on IKr. Significant, non–dose-
dependent effects were observed in the presence ofHP�CD or HP�CD-diclofenac of similar magnitudecross the 300-fold dose range of concentrationsested, suggesting an artifact due to the detergent effectf HP�CD in this in vitro model. In vivo, neither
HP�CD-diclofenac dose resulted in QTc prolongation�2 ms (�5 ms is the threshold of clinical concern). Nocorrelation was evident between changes in QTc andplasma concentrations of diclofenac or HP�CD. Con-firming study sensitivity, moxifloxacin produced a
mean QTc prolongation �10 ms.646
Conclusions: The findings from the present studysuggest that HP�CD-diclofenac does not have a dose-dependent effect in the in vitro hERG assay system anddoes not produce proarrhythmic QTc prolongation invivo. ClinicalTrials.gov identifier: NCT01812538.(Clin Ther. 2013;35:646–658) © 2013 Elsevier HSJournals, Inc.
Key words: cyclodextrin, diclofenac, pain, QTinterval.
INTRODUCTIONSince its introduction in 1974, diclofenac has become themost commonly prescribed nonselective nonsteroidal anti-inflammatory drug (NSAID) worldwide1–3 and has demon-trated a consistent record of efficacy and tolerability incute and chronic pain.3,4 Diclofenac can be administered
by multiple routes, although an injectable form is not cur-rently available in the United States. For acute postoperativepain, the rapid onset of relief of intravenous analgesics isuseful; however, a previous formulation of diclofenac forinjection requires prolonged intravenous infusion times.5 Arecently developed parenteral diclofenac formulation em-ploys hydroxypropyl-�-cyclodextrin (HP�CD) to solubilizediclofenac, allowing for low-volume intravenous bolus ad-ministration. HP�CD-diclofenac is well tolerated and effi-cacious in dental surgery,6,7 abdominal/pelvic surgery,8 and
Portions of this work were presented at the International Association forthe Study of Pain 13th World Congress on Pain, Montreal, Quebec,Canada, August 29–September 2, 2010.
Accepted for publication March 18, 2013.http://dx.doi.org/10.1016/j.clinthera.2013.03.0140149-2918
Open access under CC BY-NC-ND license.
© 2013 Elsevier HS Journals, Inc.
Volume 35 Number 5
Open access under CC BY-NC-ND license.

k
FldwTtIsttd(dc
cHd
Tvpt
atcpnwt
c
T
D.B. Carr et al.
orthopedic surgery9 and shows less platelet inhibition thanetorolac or acetylsalicylic acid.10
Novel formulations, novel routes of administration,and different infusion rates of marketed drugs may resultin greater maximum observed plasma concentrations(Cmax) or total exposures (AUC). When HP�CD-diclofe-nac is administered by intravenous bolus, Cmax is 4- to8-fold greater than the Cmax of oral diclofenac. The USood and Drug Administration suggests that new formu-
ations of previously approved drugs undergo testing toetermine their proarrhythmic potential, in accordanceith the International Conference on Harmonisation ofechnical Requirements for Registration of Pharmaceu-
icals for Human Use guideline known as E14 (ICH E14).n particular, proarrhythmic potential is assessed by mea-uring changes in the duration of the QT interval in ahorough QT (TQT) study, in which ECG interval dura-ions and wave morphology analysis are conducted onata from healthy volunteers. Prolonged repolarizationincreased QT interval) may be associated with torsadese pointes, a polymorphic ventricular tachycardia thatan result in sudden death.11
The studies described here evaluate the proarrhyth-mic potential of HP�CD-diclofenac. The potential fora product to demonstrate proarrhythmic effects maybe evaluated by in vivo or in vitro experiments. Non-clinical estimates of arrhythmogenic potential includein vitro end points of ion channel inhibition or altera-tion of measured cellular action potential duration.12
As an in vitro screening and predictive tool to assaypotential effects on human cardiac function, humanembryonic kidney (HEK) 293 cells stably transfectedwith a human ether-à-go-go–related gene (hERG)13,14
were employed to assess the effect of the study drug onthe human potassium channel current (IKr). The hERGgene (KCNH2) encodes the � subunit of the potassiumion channel, which carries the delayed rectifier potas-sium current involved in the repolarization of the ac-tion potential in ventricular cardiac myocytes.14 Thisstudy evaluated the individual effects of diclofenac,HP�CD-diclofenac, and HP�CD on this potassiumurrent and found that HP�CD-diclofenac andP�CD inhibited the hERG current in vitro, whileiclofenac alone did not.
To further investigate this phenomenon in vivo, thisQT clinical trial quantified potential QT/QTc inter-al prolongations and established the proarrhythmicotential of HP�CD-diclofenac. The findings suggest
hat there was no net effect of HP�CD-diclofenac onMay 2013
ventricular repolarization in healthy subjects by ECGanalysis. The implications of these results for the use ofin vitro models are discussed.
MATERIALS AND METHODShERG Inhibition AssayCell Culture
HEK 293 cells stably transfected with the hERGgene were selected as the test system based on the doc-umented robustness of the gene expression in HEK 293cells and the sensitivity of the current to IKr inhibi-tors.13–16 The HEK 293 cell line was maintained inminimum essential medium complemented with 10%fetal bovine serum (Wisent Inc, St. Bruno, Quebec,Canada), 1% minimum essential medium sodium py-ruvate, 1% nonessential amino acids, 1% L-glutamine,1% penicillin/streptomycin, and 400 �g/mL G-418(Geneticin) as the selection agent (all ingredients fromGibco/Invitrogen, Burlington, Ontario, Canada), andused between passages 12 and 16. Those cells fromwhich a gigaohm (G�) seal could not be obtained orthat did not generate currents with a distinctive tailcurrent were eliminated during the equilibrationperiod.
ReagentsConcentrations of each constituent (diclofenac or
HP�CD) of HP�CD-diclofenac were selected to reflectrange calculated to exceed the anticipated clinical
herapeutic exposure and provide a safety margin ex-eeding 30 times the expected maximal therapeuticlasma concentration. The 4 concentrations of diclofe-ac sodium (Esteve Quimica, S.A., Barcelona, Spain)ere 1.58, 15.8, 158, and 474 �g/mL. The 4 concen-
rations of HP�CD (Roquette America, Inc., Water-loo, Ontario, Canada) were 14, 140, 1400, and 4200�g/mL. The 4 concentrations of HP�CD-diclofenacontained 1.58-, 15.8-, 158-, and 474-�g/mL diclofe-
nac and 14-, 140-, 1400-, and 4200-�g/mL HP�CD.he active control, the IKr inhibitor E-4031 (N-[4-[[1-
[2-(6-methyl-2-pyridinyl)ethyl]-4-piperidinyl]carbon-yl]phenyl]methane sulfonamide dihydrochloride anhy-drous, Sigma-Aldrich Co LLC, St. Louis, Missouri),was used at 500 nM.
The internal pipette solution was composed of140-mM KCl, 1.0-mM MgCl2, 4.0-mM Mg-ATP,5.0-mM EGTA, 10-mM HEPES, and 10-mM sucrose,pH 7.4 � 0.05. The hERG external solution was com-
posed of 140.0-mM NaCl, 5.0-mM KCl, 1.8-mM647

H
cs
edr
Clinical Therapeutics
CaCl2, 1.0-mM MgCl2, 10.0-mM HEPES, and10.0-mM dextrose, pH 7.3 � 0.05. Diclofenac and
P�CD stock solutions were prepared in hERG exter-nal solution. HP�CD-diclofenac solution was made byombination of the appropriate volumes of diclofenactock solution and HP�CD stock solution.
ProcedureThe whole-cell patch-clamp technique was used to
functionally evaluate drug interactions with the ionicchannels.17 HEK 293 cells plated onto 35-mm petridishes were washed twice with 1 mL of hERG externalsolution followed by the addition of 2 mL of hERGexternal solution. The petri dish was mounted on thestage of an inverted phase contrast microscope andmaintained at constant temperature (35°C � 2°C). Aborosilicate glass micropipette filled with the internalpipette solution was positioned above a single cell us-ing an Eppendorf PatchMan micromanipulator (Ep-pendorf Canada, Mississauga, Ontario, Canada). Themicropipette was lowered to the cell until a close con-tact was achieved. The G�-range membrane-pipetteseal was then created by applying a slight negative pres-sure (resistances were measured using a 5-mV squarepulse). Cell capacitance was immediately measured toevaluate cell surface area, using a conversion factor of1 pF/�m2. This cell surface area was later used to cal-culate net current density.
All currents were recorded following analog filter-ing using a 4-pole Bessel filter (Frequency Devices,Haverhill, Massachusetts) set at 1 kHz. Through thecomputer-controlled amplifier, the cell was depolar-ized to a maximum value of �25 mV, starting at �5mV, in 10-mV increments, for 2 seconds each. Themembrane potential was then returned to �55 mV for2 seconds, and finally repolarized to the holding poten-tial of �60 mV. This allowed the channels to go fromactivated to inactivated mode, and back to activatedmode, to measure robust tail currents. All K� selectivecurrents passing through hERG channels were re-corded using Axopatch-1D or Axopatch 200B ampli-fiers and digitized with Digidata 1322A or 1440AAD-DA interfaces (Axon Instruments Inc, Foster City,California, now Molecular Devices Inc). The recordingof the cell current started 500 ms before cell depolar-ization to �5/�15/�25 mV and lasted for 500 ms afterthe cell had been repolarized to �60 mV.
After baseline recordings were obtained, the in-
creasing concentrations of diclofenac, HP�CD, or648
HP�CD-diclofenac were added in 20-�L aliquots di-rectly to the experimental chamber and were allowedto disperse through a closed-circuit perfusion systemusing a mini-peristaltic pump (MP-1, Harvard Instru-ments, Holliston, Massachusetts). Exposure times foreach concentration were limited to 2.5 to 5 minutes.Following the recording of currents in the presence ofall concentrations of diclofenac, HP�CD, or HP�CD-diclofenac, a flow-through perfusion system was usedto wash out the test article and obtain postexposurehERG currents in the same manner as previously de-scribed. Finally, an aliquot of E-4031 (final concentra-tion, 500 nM) was added after the washout recordingsto verify the sensitivity of the system.
The hERG currents generated by heterologous ex-pression systems such as HEK 293 cells are known torun down over long periods of recording. Therefore,parallel experiments were run in the absence of diclofe-nac, HP�CD, or HP�CD-diclofenac and in the pres-nce of the solvent to correct for the time-dependentecrease in current density, known as currentundown.
Statistical AnalysisThe correction for the time-dependent decrease in
current density involved averaging the changes in cur-rent density associated with time and solvents, andmultiplying the “test-article” results with the resultingcorrection factor. All results appearing in this reporthave been corrected for the effect of the vehicle and fortime-dependent changes in current density.
hERG current amplitudes are expressed as currentdensity (in nanoamperes/picofarad [nA/pF]) to correctfor variations in cell size within the population of cellsused for this study. Currents were analyzed using theClampfit 10.0 module of the pClamp 10.0 software(Axon Instruments Inc).
The results obtained in the presence of each concen-tration were expressed as net current density, normal-ized against current density measured in baselineconditions.
The amplitude of the IKr tail current was calculatedas the difference between the average current recordedbefore the depolarizing pulse to �15 mV and the max-imum transient current recorded at the beginning ofthe repolarizing pulse to �55 mV. Paired t tests wereperformed to determine the statistical significance ofthe differences in current density obtained before and
after the exposure of the cells to the test article. Signif-Volume 35 Number 5

wmfsot
lt
s
bthnadoihcacbmQjcraewFpuc
onneyoaH(aoopcmaJafkodd
Qsecdtjtmr
D.B. Carr et al.
icance was set at P � 0.05, where P is the probabilitythat the difference in current density levels is due tochance alone.
TQT StudySubjects
To calculate the appropriate sample size for thisstudy, an SD of 10 ms (�) for mean QTc prolongation
as assumed for the primary end point, and a maxi-um difference of no more than 3 ms (�) was assumed
or the active arm compared with placebo. A sampleize of 64 evaluable subjects was selected to provide anverall power of 85% for the primary hypothesis usinghe following formula18:
N � �2�2�Z1�� Z�1 � ��1⁄k�2� ⁄ �10 � �2,
where k is the number of assessments, and Z1 – � andZ
(1 – �)
1/k are normal-distribution quantiles. The calcu-ation assumed � to be equal to 0.05, and 1 – � wasaken to be 0.85.
To allow for the possibility of 10% dropouts, 72ubjects were to be randomized to receive study drug.
Following approval by the institutional reviewoard (PRACS Institute, Fargo, North Dakota), writ-en informed consent was obtained from 171 screenedealthy subjects. The 72 subjects, approximately equalumbers of men and women, were to be enrolled anddmitted to the clinical research unit for a period of 13ays. Eligible subjects were required to be healthy menr women, 18 to 50 years of age, with a body mass
ndex (BMI) between 18 and 30 kg/m2, in good generalealth, and having a normal or non–clinically signifi-ant ECG at screening (QTc interval �450 ms in mennd �470 ms in women, consistent sinus rhythm, nolinically significant conduction disorders, PR intervaletween 120 and 230 ms, heart rate [HR] �100 beats/in [bpm] and �40 bpm, QRS interval �110 ms, andT intervals that could be consistently analyzed). Sub-
ects were also required to have normal or non–clini-ally significant results of physical examination, labo-atory screening, and vital-sign assessment and thebsence of any systemic illness, history of cardiac dis-ase, or a family history of QT prolongation thatould increase the risk of participation in this study.emale subjects were also required to have a negativeregnancy test and either remain sexually abstinent orse an appropriate form of birth control during the
ourse of study participation. pMay 2013
Exclusion criteria consisted of a history or presencef significant cardiovascular, pulmonary, hepatic, re-al, hematologic, gastrointestinal, endocrine, immu-ologic, dermatologic, neurologic, or psychiatric dis-ase; history of invasive cancer within the previous 5ears (excluding nonmelanoma skin cancers); historyf hypersensitivity or allergy to the quinolone class ofntibiotics, to diclofenac or other NSAIDs, or toP�CD or other excipients in HP�CD-diclofenac
monothioglycerol, sodium hydroxide, hydrochloriccid, and water for injection); a significant clinical lab-ratory test or ECG abnormality at screening; historyr presence of alcoholism or drug abuse within 2 yearsrior to the study; history of clinically significant syn-ope; and use of any prescription or over-the-counteredications, including topical medications, vitamins,
nd herbal or dietary supplements/remedies (eg, Stohn’s wort or milk thistle) within 14 days of studydmission. Subjects with a history of additional riskactors for torsades de pointes (eg, heart failure, hypo-alemia, history of drowning survival, family historyf long QT syndrome, family history of short QT syn-rome, family history of unexplained early suddeneath) were also precluded from study participation.
ProcedureThe TQT study was of randomized, single-dose,
comparative, active- and placebo-controlled, 4-waycrossover design and evaluated the effect of HP�CD-diclofenac on QTc intervals in healthy subjects. Therewas 1 period of confinement of 13 days, with subjectsadmitted to the clinic on study day �2 (2 days prior tothe start of dosing) and discharged on study day �11(day 11 after first dosing). All subjects completed afollow-up visit 7 � 3 days after clinic discharge.
The effect of HP�CD-diclofenac 37.5 mg on theTc interval was compared to that of placebo (normal
aline). A 75-mg dose of HP�CD-diclofenac was alsovaluated because it was the highest dose tested in thelinical program. The active control, moxifloxacin hy-rochloride 400 mg, was used to validate the trial ando demonstrate the expected QTc response in the sub-ects. The expected effect of the 400-mg moxifloxacinablet on the QTc intervals was a mean increase of �5s, which is the effect that represents the threshold of
egulatory concern.Subjects received a single bolus dose of HP�CD-
diclofenac 37.5 mg IV, HP�CD-diclofenac 75 mg IV,
lacebo (normal saline) IV, and moxifloxacin tablet649

�
diHpdadtetmmi
tHtwectptrIsc
waihlabwwvh
n
s
mapTaidwst2
dipctmo
difuQ
Clinical Therapeutics
400 mg PO (active control) once, in accordance withthe randomization sequence, during the 13-day admis-sion, with a 72-hour washout period between eachdosing. Subjects were dosed on study days �1, �4,�7, and �10. Study days �2 and �3, �5 and �6, and
8 and �9 were designated as study drug washoutays. On each day of dosing, 12-lead ECGs for QT-
nterval analysis were acquired from a continuousolter recording flashcard at selected nominal timeoint intervals: ��1.5, �1.0, and �0.5 hours (pre-ose); 5, 10, 15, and 30 minutes (2-minute window);nd 1, 2, 4, 6, 8, 12, and 23.5 hours (5-minute win-ow). The ECGs were 15 seconds in duration and ex-racted in triplicate. Time-matched ECGs were alsoxtracted in triplicate for the same 24-hour period onhe day prior to dosing. The QT-interval measure-ents were obtained by averaging 3 to 5 QT intervalseasured from raw waveforms in a single lead, primar-
ly lead II.Subjects were to be kept resting in the supine posi-
ion for 10 minutes before the intense cluster of ECGolter recordings at the nominal time points during
he first hour postdose. After the first hour, the subjectsere to resume supine resting for 10 minutes prior to
ach ECG nominal time point. Subject ambulation, in-luding use of toilet facilities, was prohibited duringhe 10 minutes prior to each of the ECG nominal timeoints. Throughout the Holter recording procedure,he use of cellular phones, handheld music players,eading material, or computer devices was prohibited.n addition, subjects were not permitted to engage intrenuous exercise while under observation at thelinic.
Because meals can prolong the QT interval, subjectsere kept to fasting on study days �1, �1, �4, �7,
nd �10 during the hours of frequent ECG collectionn the morning. A midday meal could be given 4 to 6ours postdose and concluded within 30 minutes, al-
owing for 1.5 hours before the next ECG acquisitiont 6 hours postdose. The evening meal was scheduledetween 8 and 12 hours postdose. Identical lunchesere served to each subject on all dosing days. Onashout days, standard meals and beverages were pro-ided as per the clinic’s usual policy, and subjects couldave these meals at their preferred times.
Blood was drawn from each subject for the determi-ation of diclofenac, HP�CD, and moxifloxacin phar-
macokinetic properties at time 0 (predose), and �5,
650
10, 15, 20, and 30 minutes and 1, 1.5, 2, 2.5, 3, 4, 6, 8,12, 18, and 23.5 hours after dosing.
Statistical AnalysisAll clinical data were analyzed using the SAS System
version 8.2 or higher (SAS Institute Inc, Cary, NorthCarolina). The primary ECG end point was the time-matched active drug–placebo difference in baseline-ad-justed QTc interval (predose baseline-adjusted) usingthe Fridericia correction formula (QTcF) evaluated atthe time point at which the maximum mean baseline-and placebo-adjusted QTcF was observed for each ac-tive treatment arm. The QTcF was defined as QT/RR0.333, where RR is the time elapsing between 2 con-ecutive R waves on the ECG.
For measurements at each time point, an ANOVAodel for a crossover design was fit to the baseline-
djusted QTcF data, including effects for treatment,eriod, and subject, with subject as a random effect.he time point at which the time-matched placebo-nd baseline-adjusted QTcF had the highest mean wasdentified separately for each of the HP�CD-diclofenacose arms and the moxifloxacin arm. In accordanceith ICH E14, the study was deemed to have demon-
trated no clinically meaningful QT interval prolonga-ion if the 1-sided 95% upper confidence limits for theHP�CD-diclofenac doses were �10 ms.The washout period between treatment arms was 2
ays to prevent treatment carryover effects from 1 dos-ng period to the next. This was tested formally for therimary end point only by the addition of a 1-periodarryover effect (effect of treatment in prior period) tohe ANOVA crossover model with effects for treat-ent, period, and subject (random effect). The carry-ver for the first period was defined as zero.
As secondary end points, time-matched activerug–placebo difference in baseline-adjusted QTcntervals were evaluated using the Bazett correctionormula (QTcB), which has been more frequentlysed in previous literature. The QTcB was defined asT/RR0.5.The QTcB was evaluated at the time point at which
the maximum mean baseline- and placebo-adjustedQTcB was observed for each active treatment arm.
A population-specific regression model was con-structed for the QT correction (QTcP) at the timepoint(s) at which the maximum mean baseline- andplacebo-adjusted QTcB and QTcP, respectively, were
observed for each active treatment arm. For this adjust-Volume 35 Number 5

id
f�ce(wCtaowii
D
crtnhs
t3
D.B. Carr et al.
ment, all of the paired drug-free QT and RR intervalmeasurements taken on study day �1 for all subjects inthe trial were plotted (QT vs RR). A linear regressionof the QT and RR relationship was modeled, and theslope estimate from this regression model, m, was usedn the HR correction of the QT interval. The QTcP waserived as QT � m(1 – RR).
Relationships between the placebo-corrected changesrom baseline in QTcF, QTcB, and QTcP (��QTcF,�QTcB, and ��QTcP, respectively) and the plasmaoncentrations of diclofenac and HP�CD were alsoxplored graphically using SigmaPlot version 11.0Systat Software, Inc, Chicago, Illinois). PK parametersere calculated using noncompartmental analysis.
max and Tmax were taken directly from the data. Theerminal elimination rate constant, �z, was calculateds the negative slope of the terminal log-linear segmentf the plasma concentration–time curve. The t1⁄2 valueas calculated as 0.693/�. AUC0–t was calculated us-
ng the linear trapezoidal method and extrapolated tonfinity using the formula AUC0–� � Ctf/�z, where Ctfis the last measurable concentration. Total plasma
Table I. Effects of injectable diclofenac* and HP�CDunless otherwise noted).
Corrected NormalizedCurrent Density
Diclofenac
Mean (SEM) P
1 1.159 (0.107) 0.1910 1.289 (0.188) 0.18100 0.914 (0.128) 0.53300 0.941 (0.095) 0.56Washout 1 1.136 (0.22)§ 0.57E-4031 0.301 (0.039)§ 0.02‡
Washout 2 0.229 (0.099)¶ 0.83
hERG human ether-à-go-go–related gene; HP�CD hyd*Diclofenac 1 1.58 �g/mL.†HP�CD 1 14 �g/mL.‡Statistical significance at P � 0.05 versus current density ractive control (E-4031) were compared to the currents recsecond washout period were compared to the current mea
§n 5.�n 6.¶n 3.#n 4.
clearance (CL) was calculated as Dose/AUC, and ter- n
May 2013
minal volume of distribution (Vz) was calculated asose/(�z AUC).
RESULTShERG Channel Assay
Diclofenac, at concentrations up to 474 �g/mL,aused no significant inhibition of the hERG currentecorded by patch-clamp from HEK 293 cells stablyransfected with hERG (Table I). None of the diclofe-ac concentrations tested significantly inhibited theERG current compared with the baseline current den-ity measured at I�15 (n 7).
Testing of varying concentrations of the formula-tion vehicle, HP�CD, produced statistically significantbut non–dose-dependent effects on hERG current. The4 HP�CD concentrations tested (14, 140, 1400, and4200 �g/mL) produced similar effects in the test sys-em, causing, respectively, 22.5%, 39.3%, 43.5%, and6.5% inhibition of the hERG current density for I�15
(n 7).HP�CD-diclofenac produced effects similar to
those observed with the vehicle HP�CD, causing sig-
ERG current density (N 7 responsive cells patched
HP�CD HP�CD-Diclofenac
ean (SEM) P Mean (SEM) P
75 (0.042) 0.002‡ 0.807 (0.038) 0.1407 (0.058) 0.001‡ 0.547 (0.051) 0.002‡
65 (0.047) 0.0001‡ 0.522 (0.066) 0.001‡
35 (0.059) 0.001‡ 0.590 (0.068) 0.018‡
71 (0.135) 0.019‡ 0.397 (0.181)� 0.002‡
08 (0.034) 0.007‡ 0.154 (0.045)� 0.05291 (0.052) 0.082 0.053 (0.030)# 0.007‡
opyl �-cyclodextrin.
d after the baseline condition. Currents recorded after theafter the first washout period; currents measured after thefollowing exposure of the cells to the active control.
† on h
M
0.70.60.50.60.50.10.1
roxypr
ecordeordedsured
ificant and dose-independent current inhibition. The
651

rt
H
t7v
Tm
Clinical Therapeutics
3 highest concentrations of HP�CD-diclofenac testedespectively caused 45.3%, 47.8%, and 41% inhibi-ion of the hERG tail current density (n 7). The IKr
selective inhibitor E-4031 induced respective decreasesof 73.5%, 81.1%, and 61.2% compared with the av-eraged I�15 tail current remaining after diclofenac,
P�CD, or HP�CD-diclofenac washout. The inhibi-tory effect of E-4031 was consistent with publishedpotency and was irreversible. The observed irrevers-ibility of this inhibition was consistent with previousobservations.13
TQT StudyOf the 171 screened subjects, 74 were randomized
and 70 received study drug. Four randomized subjectswere withdrawn just prior to dosing, as 2 withdrewconsent, 1 had an abnormal vital signs assessment atbaseline, and 1 had an abnormal laboratory result atbaseline. Among the 70 subjects who completed thestudy, 39 were male (55.7%) and 31 were female(44.3%). The treatment-sequence groups were compa-rable with respect to all demographic and baseline
Table II. Baseline- and placebo-adjusted QTcF at mclofenac or moxifloxacin in each active-treat
HP�CD-D37.5
Maximum mean, msNominal time after dosing 1Adjusted mean* 1SE 190% CI* �0.45
At subject-specific Tmax of diclofenacAdjusted mean* �0SE 190% CI* �2.27
At subject-specific Tmax of HP�CDAdjusted mean* �0SE 190% CI* �2.13
HP�CD hydroxypropyl �-cyclodextrin; QTcF Fridericia*Adjusted mean (baseline-adjusted QTcF for active – baselin
an ANOVA model with effects for subject, period, and trea
characteristics. The mean age was 23.3 years (range, l
652
18–49 years), and the mean BMI was 24.7 kg/m2
(range, 18.3–29.8 kg/m2).Evaluation of the primary ECG end point indicated
hat exposure to HP�CD-diclofenac at the 37.5- and5-mg doses produced no clinically meaningful QT inter-al prolongation. Administration of HP�CD-diclofenac
did not cause mean QTc prolongation beyond 5 ms, thethreshold of regulatory safety concern (Table II). Thetime points at which the time-matched placebo- andbaseline-adjusted QTcF had the highest means were 1hour postdosing in both the HP�CD-diclofenac 37.5-and 75-mg treatment arms and 4 hours postdosing inthe moxifloxacin 400-mg treatment arm. The upperlimits of 1-sided 95% upper confidence limits, equal tothe 90% CI boundary, were 3.68 and 3.42 ms withHP�CD-diclofenac 37.5 and 75 mg, respectively. Inaddition, mean QTc prolongation was �5 ms whenmeasured at subject-specific Tmax of diclofenac andHP�CD. The upper limits of the 90% CI of the ad-justed mean for each HP�CD-diclofenac dose at the
max of diclofenac and the Tmax of HP�CD were all �2s, providing further evidence that QTcF is not pro-
m mean and subject-specific Tmax with HP�CD-di-arm (n 70 per arm).
enac HP�CD-Diclofenac75 mg IV
Moxifloxacin400 mg PO
1 h 4 h1.36 10.621.25 1.28
68 �0.70 to 3.42 8.50 to 12.73
�0.22 —1.18 —
55 �2.17 to 1.74 —
0.04 —1.18 —
73 �1.91 to 1.99 —
ted QT interval.sted QTcF for placebo), SE, and 90% CI were obtained from, with subject as a random effect.
aximument
iclofmg IV
h.62.25to 3.
.36
.16to 1.
.20
.17to 1.
-correce-adjutment
onged by HP�CD-diclofenac. The moxifloxacin
Volume 35 Number 5

fl
td
vmQQHclwdl
D.B. Carr et al.
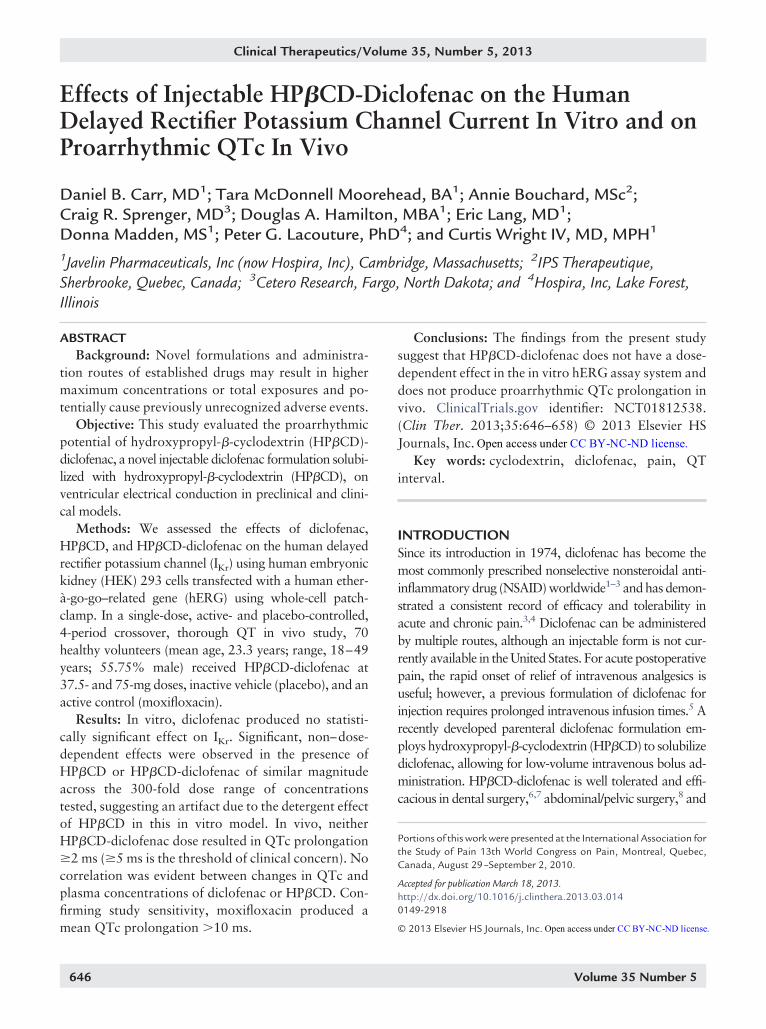
group had a mean maximum effect of 10.62 ms, andthe lower limit of the 90% CI (8.50–12.73) was �5ms, establishing the study’s sensitivity to detect ameaningful drug-induced prolongation of QTc. Ad-justed means of the time-matched active drug–placebodifferences in baseline-adjusted QTcF with the 37.5-and 75-mg doses of HP�CD-diclofenac and moxi-oxacin 400 mg are presented in Figure 1.
The results using QTcB and QTcP were comparable tohe primary end point (QTcF). The time-matched active
12
10
8
6
4
2
0
–2
0 2 4 6 8 10Ti
Adj
uste
d M
ean
QTc
F (m
s)
12
10
8
6
4
2
0
–2
0 2 4 6 8 10Ti
Adj
uste
d M
ean
QTc
F (m
s)
A
B
Figure 1. Adjusted means of the time-matched activecorrected QT interval (QTcF). Overlays ofconcentrations (open symbols) of (A) dicfollowing administration of intravenous Hcontrol).
rug–placebo difference in baseline-adjusted QTc inter- Q
May 2013
al using QTcB and QTcP at the time point of the maxi-um mean baseline- and placebo-adjusted QTcB andTcP, respectively, were similar. The adjusted meanTcB (baseline – mean QTcB) was 0.83 ms withP�CD-diclofenac 37.5 mg, 0.99 ms with HP�CD-di-
lofenac 75 mg, and 11.92 ms with moxifloxacin. Theower limit of the 90% CI of the adjusted mean QTcBith moxifloxacin was �5 ms, as expected, again vali-ating the assay sensitivity. Using the population-derivedinear regression line and the slope of the line to calculate
Mea
n P
lasm
a C
once
ntra
tion
(ng
/mL)
14 16 18 20 22 24
3000
6000
9000
12,000
15,000cF
sma]
HPβCD-diclofenac 37.5 mg IVHPβCD-diclofenac 75 mg IV
HPβCD-diclofenac 37.5 mg IVHPβCD-diclofenac 75 mg IV
Moxifloxacin 400 mg
Mea
n P
lasm
a C
once
ntra
tion
(ng
/mL)
14 16 18 20 22 24
20,000
40,000
60,000
80,000
100,000
–placebo differences in baseline-adjusted Fridericia-sted QTcF values (solid symbols) and mean plasmaac and (B) hydroxypropyl �-cyclodextrin (HP�CD)-diclofenac 37.5 or 75 mg or moxifloxacin (active
12me (h)
QT
[Pla
12me (h)
-drugadjulofenP�CD
TcP, the adjusted mean QTcP (baseline – mean QTcP)
653

wmlH
w
ttetwdwQami
vaiwm
cm
H
paM
3
v
H
Clinical Therapeutics
was 1.80 ms with HP�CD-diclofenac 37.5 mg, 1.57 msith HP�CD-diclofenac 75 mg, and 10.75 ms withoxifloxacin. With both corrective methods, the upper
imit of the 90% CI of the adjusted mean of eachP�CD-diclofenac dose was �10 ms, indicating no clin-
ically meaningful QTcB or QTcP prolongation. AbsoluteQTcF values of �450 ms occurred with similar frequency
ith placebo and HP�CD-diclofenac, and there were nochanges of �30 ms in these groups.
Subset evaluations of the male and female subpopula-ions were consistent with the overall results. Applyinghe primary analysis for HP�CD-diclofenac, there was novidence of QTcF prolongation in the men or women. Inhe men (n 39), the adjusted mean QTcFs were 1.76 msith HP�CD-diclofenac 37.5 mg, 0.51 ms with HP�CD-iclofenac 75 mg, and 9.15 ms with moxifloxacin. In theomen (n 31), the corresponding adjusted meanTcFs were 1.52, 3.69, and 12.44 ms. In both the men
nd women, the upper limit of the 90% CI of the adjustedean with each HP�CD-diclofenac dose was �10 ms,
ndicating no clinically meaningful QTcF prolongation.None of the male subjects (n 39) had a mean QTcF
alue of �450 ms or an increase of �30 ms from baseline atny time point. Values of �470 ms were considered normaln women. Mean QTcF values between 470 and 480 msere observed in 1 female subject following placebo and
Table III. Mean pharmacokinetic properties of diclofeunless otherwise noted). Values are arithm
Parameter
HP�CD-Diclofenac 37
Diclofenac H
Cmax, ng/mL 6493 (1363) 4957Tmax, h* 0.083AUC0–t, h · ng/mL 1984 (399) 5957AUC0–�, h · ng/mL 2017 (397)† 6035�z, h�1 0.421 (0.075)† 0.40t1⁄2, h 1.70 (0.33)† 1.7CL, mL/min 299 (57.9)† 95.Vz, L 43.4 (9.3)† 14.
�z terminal elimination rate constant; CL total plasmavolume of distribution.*Median.†n 66.‡n 69.
oxifloxacin treatments. One female subject had an in-
654
rease from baseline QTcF between 30 and 60 ms followingoxifloxacin treatment.The PK data confirmed that exposures to diclofenac,
P�CD, and moxifloxacin were consistent with theknown PK properties of each compound. A summaryof mean the PK properties of diclofenac and HP�CD isresented in Table III. For diclofenac, dose proportion-lity is evident on examination of these parameters.ean values of Cmax and AUC0–� increased 2-fold be-
tween the 37.5- and 75-mg HP�CD-diclofenac doses,and the mean values for CL, Vz, and t1⁄2 were similarwith both doses. Dose proportionality was also ob-served for the HP�CD PK parameters. The mean val-ues of Cmax and AUC0–� increased 2-fold between the7.5-mg (333.3-mg HP�CD) and 75-mg (666.7-mg
HP�CD) HP�CD-diclofenac doses, whereas the meanalues for CL, Vz, and t1⁄2 were similar between the 2
doses. The mean plasma concentrations of diclofenacand HP�CD following intravenous administration of
P�CD-diclofenac are presented in Figure 1.No relationship between ��QTcF and the plasma
concentration of either diclofenac or HP�CD was ap-parent (Figure 2). Because there was no apparent rela-tionship between any ��QTc and the correspondingplasma concentrations of diclofenac or HP�CD, no
nd HP�CD measured in thorough QT study (N 70ean (SD) unless otherwise noted.
IV HP�CD-Diclofenac 75 mg IV
D Diclofenac HP�CD
553) 12102 (2146) 99039 (21709)0.083 0.083
737) 3943 (788) 130497 (27384)563)‡ 3967 (789) 131163 (27377)
045)‡ 0.389 (0.067) 0.382 (0.059)23)‡ 1.84 (0.35) 1.86 (0.32).5)‡ 304 (62.1) 88.2 (17.3)
5)‡ 48.1 (11.2) 14.1 (3.2)
nce; HP�CD hydroxypropyl �-cyclodextrin; Vz terminal
nac aetic m
.5 mg
P�C
0 (110.0831 (105 (104 (0.4 (0.1 (183 (3.
cleara
PK/PD models were fitted to the data.
Volume 35 Number 5

p
D.B. Carr et al.
TolerabilityHP�CD-diclofenac was well tolerated in this
healthy adult population. The prevalences of treat-ment-emergent adverse events (TEAEs), defined as anyevents not present before exposure to the study drug orany events already present that worsened in either in-
50
40
30
20
10
0
–10
–20
–30
–400 5000
Diclofenac
∆∆∆∆Q
TcF
(ms)
50
40
30
20
10
0
–10
–20
–30
–400 50,000
HPββCD Co
∆∆∆∆Q
TcF
(ms)
A
B
Figure 2. A. Relationship between placebo-corrected(��QTcF) and plasma concentrations o(HP�CD) after intravenous administration(HP�CD 333.3 and 666.7 mg, respectively
tensity or frequency following exposure to study drug,
May 2013
were 8.6% with HP�CD-diclofenac 37.5 mg and withlacebo, 10.0% with HP�CD-diclofenac 75 mg, and
12.9% with moxifloxacin. The most frequent TEAEswere nervous system disorders (ie, dizziness and head-ache), followed by administration-site conditions (in-cluding injection-site pain and hematoma). The fre-
ntration (ng/mL)000 15,000 20,000
ation (ng/mL)00 150,000 200,000
ge from baseline in Fridericia-corrected QT intervaldiclofenac and (B) hydroxypropyl �-cyclodextrin
�CD-diclofenac 37.5 (triangles) and 75 mg (circles)ealthy subjects.
Conce10,
ncentr100,0
chanf (A)of HP) in h
quencies of nervous system disorders were 4.3% with
655

ci
ttH
otowso
voai
mH
bcth
b
iQp
o
ta
Clinical Therapeutics
both HP�CD-diclofenac doses, 5.7% with moxifloxa-in, and 2.9% with placebo. The frequencies of admin-stration-site conditions were 2.9% with HP�CD-di-clofenac 37.5 mg, 4.3% with HP�CD-diclofenac 75mg, 2.9% with moxifloxacin, and 5.7% with placebo.No treatment-related TEAEs were reported with pla-cebo, whereas the frequencies were 2.9% withHP�CD-diclofenac 37.5 mg, 4.3% with HP�CD-di-clofenac 75 mg, and 7.1% with moxifloxacin. Themost frequent treatment-related TEAEs were dizzinessand nausea, which were reported only with HP�CD-diclofenac 75 mg (1.4% and 2.9%, respectively) andmoxifloxacin (5.7% and 4.3%, respectively).
At baseline and study completion, all mean hema-tology and chemistry measurements were within nor-mal limits. The most notable shifts were decreases inhematocrit, hemoglobin, neutrophils, and red bloodcell count, likely related to repeated blood draws dur-ing the study.
No deaths, discontinuations, or serious adverseevents were reported. None of the subjects reportedexperiencing episodes of ventricular tachycardia, fi-brillation, syncope, or seizure.
DISCUSSIONOur results demonstrate the tolerability of HP�CD-diclofenac in terms of an absence of proarrhythmicQTc prolongation, while highlighting some concernsand caveats related to the in vitro experimental systemused to evaluate that risk. The in vitro studies indicatethat diclofenac causes no significant inhibition of thehERG channel current recorded by patch-clamp fromHEK 293 cells, providing a safety margin exceeding30 times the anticipated plasma concentration ofHP�CD-diclofenac. In the presence of HP�CD alone,the hERG current was significantly inhibited, but in adose-independent manner. The inhibition of the hERGcurrent by HP�CD-diclofenac correlates closely withhat following exposure to HP�CD alone. Therefore,he authors conclude that the effect observed forP�CD-diclofenac resulted from the non–dose-de-
pendent effect of HP�CD with the hERG channel.The excipient HP�CD is a cyclic, glucose-derived
ligomer consisting of linked a-1 A-glucose units usedo enhance the solubility of diclofenac.19 These glucoseligomers form a cone-like cavity into which poorlyater-soluble compounds may enter, forming a water-
oluble complex. Cyclodextrins are used to solubilize
ver 35 drugs on the market today.20 Advantages of t656
solubilizing with HP�CD include a reduction in dosingolume, reduction in irritation from the high or low pHr the use of organic solvents needed for solubilization,nd avoidance of direct venous irritation from the drugtself. HP�CD has been employed to enhance the sol-ubility of poorly soluble drugs such as the marketedantifungal itraconazole, a novel formulation of propo-fol, and several other intravenous, oral, suppository,and eye-drop formulations.20–22
The lack of dose response in the hERG blockade forboth HP�CD-diclofenac and HP�CD suggests that the
echanism is a nonspecific, detergent-like artifact ofP�CD in this in vitro testing system. Supporting this
hypothesis, Mikhail et al23 reported a significant inhi-ition of hERG currents when measured by patch-lamp at 37°C on stably transfected HEK 293 cells inhe presence of cyclodextrins. The nonspecific effect onERG by HP�CD has been attributed to the an inter-
action of HP�CD with lipid rafts in the cell mem-rane,23,24 which is supported by data indicating that
other ion channels exhibit cholesterol-dependent activ-ity.25 Nonetheless, because hERG channel blockades not perfectly correlated with in vivo effects on theT interval,12,26 a thorough QT (TQT) study waserformed.
The data from the TQT study demonstrate that 37.5r 75 mg HP�CD-diclofenac is not likely to cause
proarrhythmic QTc prolongation. In general, womenare at greater risk for torsades de pointes27; however,results from the present study indicated that womenwere not more likely to show a prolonged QT intervalcompared with men. The different corrections for HRfor the QT interval were all in agreement in the presentresults. The Fridericia correction (QTcF) is more fre-quently used at present, whereas the Bazett correction(QTcB) has been used historically in the literature, al-though the latter may not correct as accurately for ex-treme values. The population-based estimations of theQT interval (QTcP) were also in accordance withQTcF and QTcB. The PK data from the study con-firmed that subjects were exposed to diclofenac andHP�CD as expected, but no apparent relationship be-tween the placebo-corrected cha nge from baseline inQTcF, QTcB, or QTcP and the plasma concentrationof either diclofenac or HP�CD was observed.
Thus, the results of the TQT study further supporthe conclusion that the hERG effect of HP�CD is anrtifact of the membrane-testing system employed, as
here was no indication that HP�CD-diclofenacVolume 35 Number 5

touom
1
D.B. Carr et al.
lengthened the QT interval. These results are consis-tent with those from other postmarketing clinical stud-ies of diclofenac, which have shown no evidence oftorsades de pointes.3,4,6,7
Preclinical models are increasingly used during thedrug development process to assess arrhythmogenicity,and are generally well correlated with results fromTQT studies.26 However, our results showing the non-specific effect of cyclodextrins highlight the limits in-herent in simplified in vitro systems. Poorly solubledrugs present a particular problem, as other types ofcarrier, such as organic solvents or nonionic surfac-tants, can also interfere with the hERG potassium cur-rent.24 The data from these studies suggest not onlyhat controls should be carefully selected when testingther drug formulations that use cyclodextrins as sol-bilization vehicles in this model system, but also thatther in vitro models should be considered and thatultiple methods should be employed.24,26
CONCLUSIONThe findings from the present study suggest thatHP�CD-diclofenac has no dose-dependent effect in thein vitro hERG assay system and does not produceproarrhythmic QTc prolongation in vivo.
ACKNOWLEDGMENTSThe authors thank IPS Therapeutique Inc, Sherbrooke,Quebec, Canada, for conducting the hERG study; BillKramer, PhD, for calculations and figures related to thein vivo results; Miganush Stepanians, PhD, for in vivostudy design and analysis; and Louis R. Cantilena,MD, PhD, for providing expert guidance during theearly phases of these studies. Drs. Carr and Lacouturewrote and edited the manuscript, and all other authorsprovided critical input and approval. Drs. Carr,Springer, Wright, and Lang were involved in study designand data interpretation, and P.G.L. provided interpreta-tion of the study data. Ms. Bouchard performed in vitroexperiments and provided interpretation of the data. Ms.McDonell Moorhead, Mr. Hamilton, and Ms. Maddenwere involved in the data collection.
CONFLICTS OF INTERESTThis research was funded by Javelin Pharmaceuticals,Inc, Cambridge, Massachusetts (Javelin was acquiredin July 2010 by Hospira, Inc). Dr. Carr, Dr. Lacouture,Ms. McDonnell Moorehead, Ms. Bouchard, Dr.
Sprenger, Mr. Hamilton, Dr. Lang, Dr. Wright, andMay 2013
Ms. Madden performed this work as a part of theiremployment by Javelin/Hospira or (for Ms. Bouchardand Dr. Sprenger) under contract thereto. Hospira, Incsponsored Fred Peyerl, PhD, and Michelle Merrigan,PhD of Boston Strategic Partners, Inc. for editorial sup-port. The authors have indicated that they have noother conflicts of interest with regard to the content ofthis article.
REFERENCES1. Cannon CP, Curtis SP, Bolognese JA, et al. Clinical trial
design and patient demographics of the MultinationalEtoricoxib and Diclofenac Arthritis Long-term (MEDAL)study program: cardiovascular outcomes with etoricoxibversus diclofenac in patients with osteoarthritis and rheuma-toid arthritis. Am Heart J. 2006;152:237–245.
2. Cannon CP, Curtis SP, FitzGerald GA, et al. Cardiovascularoutcomes with etoricoxib and diclofenac in patients withosteoarthritis and rheumatoid arthritis in the Multina-tional Etoricoxib and Diclofenac Arthritis Long-term(MEDAL) programme: a randomised comparison. Lancet.2006;368:1771–1781.
3. Catalano MA. Worldwide safety experience with diclofe-nac. Am J Med. 1986;80:81–87.
4. Willkens RF. Worldwide clinical safety experience withdiclofenac. Semin Arthritis Rheum. 1985;15(Suppl 1):105–110.
5. Voltarol ampoules (injectable diclofenac) [product charac-teristics]. Surrey, UK: Novartis Pharmaceuticals UK Ltd;2010.
6. Christensen K, Daniels S, Bandy D, et al. A double-blindplacebo-controlled comparison of a novel formulation ofintravenous diclofenac and ketorolac for postoperativethird molar extraction pain. Anesth Prog. 2011;58:73–81.
7. Leeson RM, Harrison S, Ernst CC, et al. Dyloject, a novelinjectable diclofenac formulation, offers greater safety andefficacy than Voltarol for postoperative dental pain. RegAnesth Pain Med. 2007;32:303–310.
8. Gan TJ, Daniels SE, Singla N, et al. A novel injectableformulation of diclofenac compared with intravenousketorolac or placebo for acute moderate-to-severe painafter abdominal or pelvic surgery: a multicenter, double-blind, randomized, multiple-dose study. Anesth Analg. 2012;115:1212–1220.
9. Daniels SE, Melson T, Hamilton DA, et al. Analgesicefficacy and safety of a novel injectable formulation ofdiclofenac compared with intravenous ketorolac and pla-cebo after orthopedic surgery: a multicenter, randomized,double-blinded, multiple-dose trial. Clin J Pain. In press:doi: 10.1097/AJP.0b013e318270f957.
0. Bauer KA, Gerson W, Wright CT, et al. Platelet function
following administration of a novel formulation of intrave-657

1
1
1
1
1
1
1
2
2
2
2
2
rabbit Purkinje fiber action poten-
2
2
2
JAMA. 1993;270:2590–2597.
Clinical Therapeutics
nous diclofenac sodium versus ac-tive comparators: a randomized,single dose, crossover study inhealthy male volunteers J Clin Anesth.2010;22:510–518.
11. Algra A, Tijssen JG, Roelandt JR, etal. QTc prolongation measured bystandard 12-lead electrocardiogra-phy is an independent risk factor forsudden death due to cardiac arrest.Circulation. 1991;83:1888–1894.
12. Picard S, Goineau S, Guillaume P, etal. Supplemental studies for cardio-vascular risk assessment in safetypharmacology: a critical overview.Cardiovasc Toxicol. 2011;11:285–307.
3. Zhou Z, Gong Q, Ye B, et al. Proper-ties of HERG channels stably ex-pressed in HEK 293 cells studied atphysiological temperature. Biophys J.1998;74:230–241.
4. Sanguinetti MC, Jiang C, CurranME, et al. A mechanistic link be-tween an inherited and an acquiredcardiac arrhythmia: HERG encodesthe IKr potassium channel. Cell.1995;81:299–307.
5. Hancox JC, Levi AJ, Witchel HJ. Timecourse and voltage dependence ofexpressed HERG current comparedwith native “rapid” delayed rectifierK current during the cardiac ventric-ular action potential. Pflugers Archiv:Eur J Physiol. 1998;436:843–853.
6. Zhang Y, Wang H, Wang J, et al.Normal function of HERG K� chan-nels expressed in HEK293 cells re-quires basal protein kinase B activ-ity. FEBS Lett. 2003;534:125–132.
7. Jurkat-Rott K, Lehmann-Horn F. Thepatch clamp technique in ion chan-nel research. Curr Pharm Biotechnol.2004;5:387–395.
8. Zhang J. Testing for positive controlactivity in a thorough QTc study.J Biopharm Stat. 2008;18:517–528.
9. Gould S, Scott RC. 2-Hydroxypropyl-beta-cyclodextrin (HP-beta-CD): atoxicology review. Food Chem Toxicol.2005;43:1451–1459.
0. Brewster ME, Loftsson T. Cyclodex-trins as pharmaceutical solubilizers.
Adv Drug Del Rev. 2007;59:645–666.658
1. Baker MT, Naguib M. Propofol: thechallenges of formulation. Anesthesi-ology. 2005;103:860–876.
2. Stevens DA. Itraconazole in cyclodex-trin solution. Pharmacotherapy. 1999;19:603–611.
3. Mikhail A, Fischer C, Patel A, et al.Hydroxypropyl beta-cyclodextrins: amisleading vehicle for the in vitrohERG current assay. J Cardiovasc Phar-macol. 2007;49:269–274.
4. Himmel HM. Suitability of com-monly used excipients for electro-physiological in-vitro safety phar-macology assessment of effects onhERG potassium current and on
tufts.edu
tial. J Pharmacol Toxicol Methods.2007;56:145–158.
5. O’Connell KM, Tamkun MM. Tar-geting of voltage-gated potassiumchannel isoforms to distinct cell sur-face microdomains. J Cell Sci. 2005;118:2155–2166.
6. Gintant G. An evaluation of hERGcurrent assay performance: translat-ing preclinical safety studies to clini-cal QT prolongation. Pharmacol Ther.2011;129:109–119.
7. Makkar RR, Fromm BS, SteinmanRT, et al. Female gender as a riskfactor for torsades de pointes associ-ated with cardiovascular drugs.
Address correspondence to: Daniel B. Carr, MD, Tufts Medical Center,#298, 800 Washington Street, Boston, MA 02111. E-mail: daniel.carr@
Volume 35 Number 5





























