Embed Size (px)
Citation preview

Early Human Development, 23 ( 1990) 109- 115 Elsevier Scientific Publishers Ireland Ltd.
109
EtiD 01080
Effects of behavioural states on cardiac output in the healthy human fetus at 36-38 weeks
of gestation
Giuseppe Rizzo, Domenico Arduini, Herbert Valensise and Carlo Romanini
Laboratory of Fetal Physiology, Department of Obstetrics and Gynecology, Universit& Cattolica S. Cuore, Largo A. Gemelli 8, 00168 Rome and Department of Obstetrics and Gynecology, Universitd di
Ancona (Italy)
(Received 27 February 1990; revision received 7 May 1990; accepted 22 May 1990)
Summary
Doppler velocity waveforms from atrioventricular valves were recorded in 20 healthy fetuses at 36-38 weeks of gestation during both behavioural states 1F (quiet sleep) and 2F (active sleep). No significant changes were found in the ratios between the velocities during early passive ventricular filling and active ventricular filling (E/ A ratios) at the level of both mitral and tricuspid valves when the measurements obtained during states 1F and 2F were compared. Moreover, during state 2F the left ventricular output increased and the right ventricular output decreased, resulting in a marked modification of the right to left cardiac output ratio. Our data suggest a redistribution of cardiac output in favour of the left side of the heart during state 2F.
Doppler echocardiography; fetal behavioural states; fetal circulation; fetal cardiac output.
Introduction
Several studies have suggested the use of Doppler echocardiography in the evalu- ation of cardiac output in the human fetus [2,6,8,10] and this technique has been recently applied to the study of fetal haemodynamics in different pathological con- ditions such as congenital heart diseases [ 151, intrauterine growth retardation [ 1,131 and anemia [5,19]. However, the studies so far performed have shown wide varia- tions between the measurements obtained. This variability might be explained on the basis of differences either in the techniques followed or in the behavioural condi- tions of the fetuses studied [2].
It has been reported that regional blood flow is altered by behavioural states [7,11,16,17] but there is no account on the influence of these states on cardiac out-
0378-3782/90/%03.50 0 1990 Elsevier Scientific Publishers Ireland Ltd. Published and Printed in Ireland

110
put and on its distribution in the human fetus. The purpose of this study was to investigate whether behavioural states affect cardiac output in healthy fetuses.
Subjects and Methods
Twenty healthy pregnant women with a gestational age between 36 and 38 weeks of gestation gave their informed consent to participate in the study. All pregnancies were singleton and with a certain gestational age as confirmed by early ultrasonic measurement of fetal crown-rump length or biparietal diameter. Normal pregnancy and fetal outcome confirmed the good health of the fetuses considered. Fetal birth- weight ranged between the 10th and 90th centiles for Italian population standards.
Recordings were carried out in the afternoon 2 h after a standardized lunch of 1500 kcal. The techniques of behavioural states and cardiac blood flow analysis have been reported in detail elsewhere [3,13]. Briefly, behavioural states were identified by simultaneous recording of fetal heart rate (FHR), gross body movements (FM) and eye movements (FEM). FHR was obtained by means of a Hewlett Packard 8040 cardiotocograph equipped with an external ultrasound transducer (carrier frequency 1 MHz). FEM and FM were determined by two different observers using two real time ultrasound equipments positioned to obtain a parasagittal section through the fetal face (Toshiba Sal 20, 3.5 MHz linear transducer) and a transverse section at the level of the upper fetal abdomen (Ansaldo color Doppler Esacord 81,5.0 MHz con- vex transducer).
In the presence of a stable (> 3 min) association between FHR, FM and FEM, resembling either the behavioural states 1F (quiet sleep) or 2F (active sleep) described by Nijhuis [9], the ultrasound transducer positioned over the fetal abdo- men was moved slightly towards the fetal chest in order to obtain an apical four chamber view of the fetal heart. The color flow mapping function was then superim- posed and the trans-mitral and trans-tricuspid flow observed. The sample volume of the pulsed Doppler was placed immediately below either the mitral or tricuspid valves in the point of maximum flow velocity, as expressed by the color brightness, and velocity waveforms were then recorded keeping an angle of insonation lower than 20°. Sample volume length was between 1 and 4 mm. Velocity waveforms anal- ysis was limited to periods of fetal apnea.
Doppler and two-dimensional images were recorded on standard l/2 inch video- tapes for subsequent analysis. In order to avoid interferences the cardiotocograph was switched off during the Doppler recording. The maximum amount of time required to obtain velocity waveforms from both tricuspid and mitral valves was 3 min. At the end of the Doppler measurements the persistence of the same stable association between FHR, FEM and FM was checked and the behavioural observa- tion continued. In the absence of this condition the Doppler recordings obtains were discarded. When a different behavioural state was evidenced the Doppler measure- ments were resumed.
Atrio-ventricular valve diameters were evaluated from the two-dimensional images obtained from optimal apical four chamber views. The analysis was per- formed in play-back on videorecorded images frozen during diastole when showing

111
the maximized diameters. Measurements were repeated on 10 different cycles for each valve and the values obtained averaged. Repeated diameter measurements var- ied less than 0.6 mm for either valves. Valvular area was calculated assuming a circu- lar cross section. As no differences were found in the valve measurements obtained during states 1F and 2F, the same area value was considered for both behavioural states.
Permanent records of all the velocity waveforms were obtained from the video- tape by means of a strip chart recorder. The printouts were labeled with random numbers. The investigator involved in the later analysis was not informed of the sequence of the printouts. Ten consecutive velocity waveforms were selected for
’ each time interval from either atrio-ventricular valve, and measurements of the fol- lowing variables were obtained with the digitizing tablet of a computer (Cardio 800, Kontron, Oxford, U.K.): (1) peak velocities during early ventricular filling (E wave) and atria1 contraction (A wave), (2) mean temporal velocity (MTV), (3) FHR.
For each time interval a ratio between E peak and A peak velocities (E/A) at the ’ level of both atrio-ventricular valves was calculated. Absolute right (RVO) and left
(LVO) ventricular outputs (ml/min) were derived by multiplying tricuspid or mitral MTV, valvular area and FHR. The combined ventricular output (CVO = RVO + LVO) and the ratio between RVO and LVO (RVO/LVO) were then calculated. All the echocardiographic recordings were performed by one operator (G.R.). In our laboratory the intra-observer coefficient of variation for all the measurements con- sidered is less than 12%. ,
Data are expressed as mean value f S.D. A two-tailed paired t-test was used for statistical analysis. A P value less than or equal to 0.05 was considered significant.
Results
Reliable recordings from either atrio-ventricular valve during states 1F and 2F were obtained in 14 patients. In the remaining cases fetal position or difficulties in
TABLE I
Comparison of Doppler echocardiographic parameters (mean + 1 SD.) measured during behavioural states 1F and 2F.
E/A mitral valve E/A tricuspid valve Mitral MTV (cm/s) Tricuspid MTV(cm/s) FHR @pm)
d LVO (ml/mm) RVO (ml/min) CVO (ml/mm) RVO/LVO
1F 2F
0.85 + 0.05 0.88 + 0.04
14.42 f 0.91 15.89 f 1.03
135.34 f 12.26 568.71 f 80.64 136.51 + 94.50
1304.92 + 154.48 1.30 + 0.18
0.86 + 0.05 0.87 + 0.05
16.16 + 1.34 14.26 k 1.42
138.47 f 14.98 650.43 rf: 96.25 689.71 f 90.16
1340.50 + 144.44 1.07 + 0.16
n.s. n.s. 0.01 0.02 n.s. 0.002 0.02 n.s. 0.001
‘Two-tailed paired r-test.

112
1 m 1 1 ,oo
1 0,95 -
f 5 0,90-
‘ij L z 0,85-
E q 0,80- w
0,75-
1F 2F
Y 0,95 -
F * 0,90- m .r c5
: 0,85- .,o ,L : 0,80-
w 0,75-
0,70-
0,65-1 1F 2F
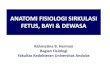
Fig. 1. E/A ratio values from mitral and tricuspid valves recorded during states 1F and 2F.
the identification of behavioural states did not allow reliable Doppler recordings to be obtained in all the experimental conditions and patients were therefore excluded from further analysis. No significant differences were found in FHR values meas- ured from left and right heart side (mean paired difference 2.14 bpm, P n.s.). Simi- larly no differences were evidenced when the values of FHR obtained during state 1F and 2F were compared (Table I).
Figure 1 shows the E/A values measured at the level of both atrioventricular valves during states 1F and 2F. No significant modifications were evidenced with the change of behavioural state. Moreover a significant increase of mitral MTV with a concomitant decrease of tricuspid MTV was evidenced during state 2F (Table I).
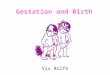
When cardiac output was calculated, a significant increase of LVO was evidenced during state 2F associated with decreased RVO values resulting in a markedly decreased RVO/LVO ratio (Fig. 2, Table I). No significant changes were found for CVO (Fig. 2, Table I).
Discussion
In the fetal heart right and left ventricles eject into the systemic circulation in par- allel: the output of the left ventricle is directed through the ascending aorta to the upper body organs, including brain and heart, whereas the output of the right ven- tricle is directed to the pulmonary circulation and through the patent ductus arterio- sus to the lower body and placenta slightly [14]. Doppler echocardiography has allowed the measurement of LVO and RVO in the human fetus. However, this analysis may be prone to errors, mainly caused by inaccuracies in the determination of valve diameters being their dimensions near the limits of ultrasound resolution. In

113
800
'2 700 'C E \ F y
z
600
500
1600-
=1400- 'C E . F "1200-
E
IOOO-
it. iF
8OOh IF 2F
lOOO-
900-
c 'E 800- . z " 700- z a
600-
soo- m .
400 I 1 1F 2F
co 1 1,8 -
F 1,6 -
i 14- P '. u
1,2-
1,0-
0,8 -
“I” 1; iF
Fig. 2. Left ventricular output (LVO), right ventricular output (RVO), combined ventricular output (CVO) and RVO/LVO values recorded during states 1F and 2F.
this study, however, the flow orifice area is assumed to remain unmodified during the experimental design and therefore potential errors in valve diameters assessment similarly affect the measurements performed during the different behavioural states.
The results of this investigation show the dependence of cardiac output on behav- ioural states. During state 2F we found a significant increase of LVO associated with a concomitant decrease of RVO, which was primarily the result of modifications in stroke volume as, in agreement with previous reports [16,18], FHR did not change significantly between 1 F and 2F.

114
As no significant changes were found for the CVO. These results suggest a redis- tribution of cardiac output with a prevalence of LVO implying a preferential stream- ing of blood to the heart and the brain during state 2F. Possible explanations for these findings include modifications of the venous return to the heart (preload) or selective changes in the vascular resistance against which ventricles eject (afterload). The former hypothesis seems unlikely on the basis of the unchanged CVO and of the absence of evident modifications of E/A ratio, an index believed to be influenced by the preload of the heart [4,12,19]. On the other hand, the latter explanation is con- sistent with the results of animal studies which showed a significant increase of cere- bral blood flow during active sleep [7,1 l] associated with a reduction of flow in the ductus arteriosus [7]. Recent Doppler investigations in the human fetus further cor- roborate this hypothesis by showing a decrease of vascular resistance at cerebral level [17] and a reduction of peak flow velocity in the ductus arteriosus [18] during state 2F.
In the human fetus, RVO is usually higher than LVO resulting in a RVO/LVO greater than 1 [2,6,10] and this is in agreement with the “right ventricle dominance” previously found in animal studies [ 141. However, previous studies on human healthy fetuses have shown that in some subjects LVO values are equal or even higher than RVO values, resulting in a wide scatter of RVO/LVO ratios [2,6]. More- over, neither of the human studies so far performed took into account behavioural states, and the wide variations found in the distribution of cardiac output might merely reflect a difference in the fetal state in which recordings were performed.
In conclusion, behavioural states seem to influence fetal cardiac haemodynamics and this should be considered whenever these parameters are investigated.
Acknowledgements
This study was supported by the Italian National Council of Research (C.N.R. Grant No 89.03875. CT04).
References
Al-Ghazali, W., Chita, S.K., Chapman, M.G. and Allan, L.D. (1989): Evidence of a redistribution of cardiac output in asymmetrical growth retardation. Br. J. Obstet. Gynaecol., %, 607-704. Allan, L.D., Chita, S.K., Al-Ghazali, W., Crawford, D.C. and Tynan M. (1987): Doppler echocar- diographic evaluation of the normal human fetal heart. Br. Heart J., 57,528-533. Arduini, D., Rizzo, G., Caforio, L., Boccolini, M.R., Romanini, C. and Mancuso S. (1989): Behav- ioural state transitions in healthy and growth retarded fetuses. Early Hum. Dev., 19, 155-162. Choong, C.Y., Herrmann, H.C., Weyman, A.E. and Fifer, M.A. (1987): Preload dependence of Doppler-derived indices of left ventricular diastolic function in humans. J. Am. Coll. Cardiol., 10, 800-808. Copel, J.A., Grannum, P.A., Green, J.J., Belanger, K., Hanna, N., Jaffe, C.C., Hobbins, J.C. and Kleinman, C.S. (1986): Fetal cardiac output in the isoimmunized pregnancy: A pulsed Doppler- echocardiographic study of patients undergoing intravascular intrauterine transfusion. Am. J. Obstet. Gynccol., 161, 361-364. De Smedt, M.C.H., Visser, G.H.A. and Meijboom, E.J. (1987): Fetal cardiac output estimated by Doppler echocardiography during mid- and late gestation. Am. J. Cardiol., 60,338-342.

115
7
8
9
10
11
12
13
14
15
16
17
18
19
Jensen, A., Bamford, O.S., Dawes, G.S., Hofmeyer. G. and Parkes, M.J. (1985): Changes in organ blood flow between high and low voltage electrocortical activity and during isocapnic hypoxia in intacted and brain stem transected fetal lambs. In: The Physiological Development of the fetus and newborn, pp. 605-610. Editors: C.T. Jones and P.W. Nathanielsz. Academic Press, London. Kenny, J.F., Plappert, T., Saltzrnan, D.H., Cartire, M., Zollars, L., Leatherman, G.F. and St John Sutton, M.G. (1986): Changes in intracardiac blood flow velocities and right and left ventricular stroke volumes with gestational age in the normal human fetus: a prospective Doppler echocardi- ographic study. Circulation, 74, 1208-1216. Nijhuis, J.G., Prechtl, H.F.R., Martin, C.B. Jr. and Bots, R.S.G.M. (1982): Are there behavioural states in the human fetus? Early Hum. Dev., 6, 177-195. Reed, K.L., Meijboom, E.J., Sahn, D.J., Scagnelli, S.A., Valdes-Cruz, L.M. and Skenker, L. (1986): Cardiac Doppler flow velocities in human fetuses. Circulations 73,41-56. Richardson, B.S., Patrick, J.E. and Abduljabbar, H. (1985): Cerebral oxidative metabolism in the fetal lamb: relationship to electrocortical state. Am. J. Obstet. Gynecol., 153,426431. Riggs, T.W., Rodriguez, R., Snider, R.A., Batton, D., Pollock, J. and Sharp, E.J. (1989): Doppler echocardiographic evaluation of right and left ventricular diastolic function in normal neonates. J. Am. Coll. Cardiol., 13,700-805. Riuo, G., Arduini, D., Romanini, C. and Mancuso, S. (1988): Doppler echocardiographic assess- ment of atrioventricular velocity waveforms in normal and small for gestational age fetuses. Br. J. Obstet. Gynaecol., 95,65-69. Rudolph, A.M. (1985): Distribution and regulation of blood flow in the fetal and neonatal lamb. Circ. Res., 57, 811-821. Shenker, L., Reed, K.L., Marx, G.R., Donnerstein, R.L., Allen, H.D. and Anderson, C.F. (1988): Fetal cardiac Doppler flow studies in prenatal diagnosis of heart disease. Am. J. Obstet. Gynecol., 158,1267-1273. van Eyck, J., Wladimiroff, J.W., Noordam, M.J., Tonge, H.M. and Prechtl, H.F.R. (1985): The blood flow velocity waveform in the fetal descending aorta: its relationship to fetal behavioural states in normal pregnancy at 37-38 weeks. Early Hum. Dev., 12,137-143. van Eyck, J., Wladimiroff, J.W., van den Wijngaard, J.A.G.W., Noordam, M.J. and Prechtl, H.F.R. (1987): The blood flow velocity waveform in the fetal internal carotid artery and umbilical artery; its relationship to fetal behavioural states in normal pregnancy at 37-38 weeks of gestation. Br. J. Obstet. Gynaecol., 94,736-741. van der Mooren, K., van Eyck, J. and Wladimiroff, J.W. (1989): Human fetal ductal flow velocity waveforms relative to behavioural states in normal term pregnancy. Am. J. Obstet. Gynecol., 160, 371-374. Visser, G.H.A., De Smedt, M.C.H. and Meijboom, E.J. (1988): Altered fetal cardiac flow patterns in pure red cell anaemia (the Blackfan-Diamond syndrome). Prenat. Diagn., 8,525-529.