Embed Size (px)
Citation preview
Effects of a mindfulness-based smoking cessation program for anadult with mild intellectual disability
Nirbhay N. Singh a,*, Giulio E. Lancioni b, Alan S.W. Winton c, Ashvind N.A. Singh a,Judy Singh a, Angela D.A. Singh a
a American Health and Wellness Institute, Verona, VA, USAb University of Bari, Italyc Massey University, Palmerston North, New Zealand
1. Introduction
It has been estimated that 1.3 billion people in the world currently smoke cigarettes or tobacco related products (Guindon& Boisclair, 2003). In the United States, about 20% of the population (i.e., 43 million people) smoked cigarettes in 2007.Smoking is the most frequently occurring preventable cause of disability and death. In the United States, at least 30% of allcancer deaths are attributed to tobacco use, with smoking causing about 87% of lung cancer deaths. In addition, smoking isresponsible for many non-cancerous lung diseases, such as chronic bronchitis, emphysema, and chronic obstructivepulmonary disease. Long-term smoking may also cause heart disease, aneurysms, bronchitis, emphysema and stroke, andworsen pneumonia and asthma, negatively impact the immune system, and increase the risk of sexual impotence in malesmokers. Short-term smoking may result in poor lung function (which may cause shortness of breath and nagging coughs),reduced ability to smell and taste, premature aging of the skin, bad breath, and stained teeth.
The prevalence of smoking in individuals with intellectual disabilities varies widely across studies, depending on thesample size, community versus institution versus clinical samples, living arrangements, age range, gender, degree ofintellectual disabilities, and comorbid mental illness. For example, in chronological order, a comprehensive sample of studiesreported the following smoking prevalence rates: 7.6% in an institution and 25.6% in group homes (Rimmer, Braddock, &Marks, 1995); 36% in individuals with mild intellectual disabilities in independent community living settings (Tracy &Hosken, 1997); 18% in clinic-referred adults with severe to borderline intellectual disabilities (Hymowitz, Jaffe, Gupta &
Research in Developmental Disabilities 32 (2011) 1180–1185
A R T I C L E I N F O
Article history:
Received 31 December 2010
Accepted 6 January 2011
Available online 1 February 2011
Keywords:
Smoking
Mindfulness-based smoking cessation pro-
gram
Intention
Mindful observation of thoughts
Meditation on the Soles of the Feet
A B S T R A C T
Smoking is a major risk factor for a number of health conditions and many smokers find it
difficult to quit smoking without specific interventions. We developed and used a
mindfulness-based smoking cessation program with a 31-year-old man with mild
intellectual disabilities who had been a smoker for 17 years. The mindfulness-based
smoking cessation program consisted of three components: intention, mindful observa-
tion of thoughts, and Meditation on the Soles of the Feet. A changing-criterion analysis
showed that this man was able to fade his cigarette smoking from 12 at baseline to 0
within 3 months, and maintain this for a year. Follow-up data, collected every 3 months
following the maintenance period, showed he was able to abstain from smoking for 3
years. Our study suggests that this mindfulness-based smoking cessation program merits
further investigation.
� 2011 Elsevier Ltd. All rights reserved.
* Corresponding author at: American Health and Wellness Institute, P.O. Box 5419, Midlothian, VA, USA. Tel.: +1 804 743 3121; fax: +1 804 743 3448.
E-mail address: [email protected] (N.N. Singh).
Contents lists available at ScienceDirect
Research in Developmental Disabilities
0891-4222/$ – see front matter � 2011 Elsevier Ltd. All rights reserved.
doi:10.1016/j.ridd.2011.01.003

Feuerman, 1997), 4% of an adult institutional population (Peine, Darvish, Blakelock, Osborne, & Jenson, 1998); 12.7% of stateand community residences in Massachusetts (Minihan, 1999); 2%, 8% and 12% of adults with intellectual disabilities residingin village communities, residential campuses, and dispersed housing in the United Kingdom (Robertson et al., 2000); 6.2% ofadults attending four social services day centers (Taylor, Standen, Cutajar, Fox, & Wilson, 2004); 14% self-reported smokingin adolescents with intellectual disabilities (Emerson & Turnbull, 2005); 26% of adolescents with mild intellectual disabilitieswere occasional or regular smokers (Kalyva, 2007). As these studies show, smoking is a reasonably common activity formany individuals with intellectual disabilities.
Only a single published study could be located that attempted to reduce or eliminate smoking in individuals withintellectual disabilities. Peine et al. (1998) used a spinning wheel, similar to that in the Wheel of Fortune TV program, toreduce smoking by two adults in a developmental disabilities center. Prior to the intervention, if the individuals did notengage in maladaptive behavior (e.g., aggression) for an hour, they could get a cigarette. While this reduced maladaptivebehavior, it resulted in high numbers of cigarettes smoked. During intervention, absence of maladaptive behavior for anhour now led to the opportunity to spin the wheel that offered various choices including cigarettes, coffee, tea, diet sodapop, diet candy, fruit juices and magazines. The probability of the spin landing on a cigarette choicereduced the opportunity to get a cigarette each hour, and this led to a 50% reduction in smoking by the end of the3-year study.
The aim of our study was to assess the effectiveness of a mindfulness-based smoking cessation program for an individualwith mild intellectual disability whose smoking had proved intractable to treatment with other approaches (e.g., nicotinereplacement therapy, pharmacotherapy, etc.).
2. Method
2.1. Participant
Paul was a 31-year-old man who had been institutionalized for 10 years from the age of 9 years. He was admitted tothe developmental center because his family could not manage his severe aggressive and destructive behaviors, and hehad been refused attendance at a special school for the same reasons. When admitted to the developmental center, hewas assessed as functioning at a mild level of intellectual disability, with uncontrolled maladaptive behaviors. He wasnot diagnosed with a psychiatric disorder, but the admitting psychiatrist noted that his behavior was very impulsive. Hewas included in the developmental center’s token economy program and put on a behavior modification program tocontrol his aggressive and destructive behaviors. His maladaptive behaviors were substantially controlled by the age of18. By the time he was transitioned to a community group home at the age of 19, he had been a smoker for almost 5years. In the developmental center, he smoked as many cigarettes as staff gave him, usually between 15 and 20 a day. Inthe first group home he was transitioned to he was allowed to purchase and smoke as many cigarettes as he wished. Hissmoking increased to an average of 30 cigarettes a day. When transitioned to a second group home, which was closer tohis work, his smoking was restricted to 12 cigarettes a day, and he was not allowed to smoke indoors. At this grouphome, the staff enrolled him in health wellness classes at the local wellness center, and he slowly began to adapt hislifestyle to incorporate wellness activities into his daily schedule. At the age of 25, he began a series of programs to quitsmoking. These included abrupt stopping of smoking, nicotine replacement therapy, pharmacotherapy (i.e., bupropion),contingency management, and other informal approaches. At best, over the 6-year period of trying to quit smoking, hewas able to abstain from smoking for a maximum of 49 consecutive days. At age 31, when he was offered anopportunity to live independently if he could quit smoking, his group home staff requested treatment for Paulusing mindfulness-based strategies. Paul consented to the treatment and agreed to adhere to the treatment protocol.
2.2. Therapist
Mindfulness training was provided by a therapist who had extensive experience in mindfulness meditation practice aswell as clinical expertise and experience in service delivery to individuals with intellectual disabilities.
2.3. Procedure
2.3.1. Design
We used a changing criterion design (Barlow, Nock, & Hersen, 2009). Following baseline, the mindfulness practice wasintroduced, with the individual being responsible for determining each successive criterion during the intervention(mindfulness practice) phase. This was followed by a 12-month maintenance period and follow-up for 3 years after thetermination of maintenance procedures.
2.3.2. Assessment
Interviews with group home staff and Paul indicated that he was allowed and smoked 12 cigarettes a day, regardless ofwhether it was a workday or weekend. Interviews at his work place showed that he did not smoke extra cigarettes at work,and that he adhered to his 12-a-day limit.
N.N. Singh et al. / Research in Developmental Disabilities 32 (2011) 1180–1185 1181
2.3.3. Reliability
Staff and Paul independently tracked his smoking during all phases of the study. During follow-up, only staff at his work sitetracked his smoking because he was in an independent living situation, and care staff was not present. Informal inquiries weremade periodically with Paul’s neighbors about whether they ever saw him smoking during the follow-up period. The overallreliability across experimental conditions was 100% during the times that both Paul and an independent rater were present.
2.3.4. Mindfulness procedures
Three mindfulness procedures were taught to Paul. These were:
2.3.4.1. Mindfulness practices. I. Intention. Right intention is one of the foundations of mindfulness practice (Shapiro & Carlson,2009), because it sets the context for the changes that follow. Paul was taught to verbally self-affirm his intention to quitsmoking and to give directionality to his conscious decision to stop smoking. This affirmation was to assist him to overcomeinertia to give up smoking, motivate himself to continue working daily on his intention to gradually stop smoking, and to remindhimself that he wanted to do it. Paul chose the statement, ‘‘I will not smoke today. I will not smoke anymore’’ as his affirmation.
2.3.4.2. Mindfulness practices. II. Mindful observation of thoughts. Paul was taught a standard mindfulness procedure forobserving his thoughts, individualized in terms of language, idiom and explanation of practice to match his ability tounderstand and engage in the meditation practice. He was taught that he was not his thoughts, and that desires were merelythoughts, so he could observe his ‘‘desire’’ thoughts, and let them go. This was adapted to deal with his desire to smoke. Paulwas taught a four-part, inter-related series of mindfulness procedures that would enable him to disengage himself from histhoughts. The mindfulness procedures required him to (1) focus on successive thoughts, (2) observe the beginning, middle,and end of each thought, (3) observe his thoughts as clouds (‘‘thought clouds’’) passing through his awareness, and (4)observe the desire to smoke as thought clouds without (a) pushing the thoughts away, (b) engaging with the thoughts, or (c)becoming emotionally attached to the thoughts. The procedures are presented in Table 1.
2.3.4.3. Mindfulness practices. III. Meditation on the Soles of the Feet (SoF). If the desire thoughts were too strong, and Paulcould not let them go, he was taught this procedure to rapidly move the focus of his attention from the craving to smoke to aneutral point on his body, the soles of his feet (Singh, Wahler, Adkins, & Myers, 2003). The procedure is presented in Table 2.To ensure fidelity of training, we used a SoF training manual (Singh, Singh, Adkins, Singh, & Winton, 2008), but theprocedures were individualized to suit Paul’s cognitive capability.
2.4. Experimental conditions
2.4.1. Prebaseline
Four months prior to the baseline, staff at Paul’s group home contacted the senior author requesting assistance for Paul inhis efforts to reduce and eliminate his smoking. They explained that he was highly motivated to quit smoking, had triedvarious methods but none had worked well for him, and he was seeking a method which would enable him to control his
Table 1
Outline of the standard mindful observation of thoughts procedure for desire to smoke.
Part I
1. Sit comfortably, preferably with your back straight and feet flat on the floor.
2. Close your eyes and continue to sit, quietly.
3. Focus your attention on the flow of your breath as it moves in through your nostrils into your body, back up, and out through your nostrils.
4. Keep your attention on your breath.
5. Stay with your breath for about 5 min.
Part II
6. Focus your attention on your breath until you feel settled and centered.
7. Now focus on your mind.
8. Observe your thoughts arising, lingering, and departing one after another.
9. Notice how your mind engages the thoughts and one thought gives rise to another, and another.
10. Do not try to stop the thoughts. Just observe the play of the thoughts in your mind.
Part III
11. Focus your attention on your breath until you feel settled and centered.
12. Imagine your mind as the sky, with clouds rolling by in the blue sky.
13. When you observe a thought arising, imagine the thought as a cloud passing by.
14. Observe your thought clouds drift through the sky and out of your attention.
15. Do not respond to the thought clouds; just observe.
Part IV
16. Focus your attention on your breath until you feel settled and centered.
17. At the first sign of a desire to smoke (i.e., desire), think of it as a thought cloud.
18. Let the thought clouds drift out of your attention.
19. When the thoughts return, repeat the same process over and over again.
20. Practice observing the thought clouds of desire until they have no physical effect on you.
N.N. Singh et al. / Research in Developmental Disabilities 32 (2011) 1180–11851182
smoking urges so that he could quit smoking. They explained that they had read about mindfulness, and were interested ininvestigating whether it could be taught to them as well as to Paul. Three months prior to the baseline, Paul and his grouphome staff met with the senior author for 2 h, during which he explained the nature of mindfulness, daily meditationpractice, customized mindfulness practices, and data collection requirements. He taught the staff and Paul a basic breathingmeditation that they could practice twice a day for 10–15 min each time. They were instructed to practice this meditation for3 months, before interventions would be initiated for Paul’s smoking.
2.4.2. Baseline
Paul was instructed to keep a log of his smoking for 14 days, including time and number of cigarettes smoked. He was told tocontinue smoking as he had done before he volunteered to participate in this study. On the first day of baseline, Paul was trained onPart I of the mindful observation of thoughts procedure, then 4 days later on Part II, and 6 days after that on Part III. Daily trainingsessions lasted 5–7 min on Part I, about 10 min with the addition of Part II, and about 15 min with the addition of Part III. On the lastday of baseline, Paul was also taught the right intention procedure, through discussion and practice, in a 45-min session.
2.4.3. Intervention
On the first day of intervention, Paul began using the affirmation every morning before getting out of bed, and wheneverhe had a desire to smoke. In addition, he practiced saying the affirmation, discussing it with his group home staff for a week,and using and practicing it independently thereafter.
Paul was trained on Part IV of the mindful observation of thoughts procedure on the first day of intervention and, fromthen on, he was required to practice all four parts of this meditation for 20 min each morning. In addition, he began trainingon SoF during 30-min supervised role play and practice sessions, twice a day for 5 days. During the following 10 days, he wasgiven practice assignments, after which he was instructed to use the procedure to control his desire to smoke. Paul wasrequired to practice SoF throughout the rest of the intervention period.
2.4.4. Criterion changes
Criterion changes were arranged when Paul and his group home staff met with the senior author. Paul decided that hewould decrease smoking by one cigarette every time he was able to maintain 3 consecutive days on his previous number ofcigarettes (Singh & Leung, 1988). That is, because he consistently smoked 12 cigarettes a day during baseline, he would set atarget of smoking 11 cigarettes a day for 3 consecutive days before reducing it to 10 cigarettes a day, and so on. Criterionchanges were to be made when there were three stable data points equal to or immediately below the criterion. However,this was set as a minimum requirement and Paul was free to maintain his smoking at criterion level until he was ready todecrease to a lower level. Criterion changes were made until Paul reached zero cigarettes per day for 3 consecutive days. Theintervention period lasted 82 days.
2.4.5. Maintenance
During maintenance, the criterion was set at zero cigarettes per day, and Paul was required to continue with hismindfulness practices for 12 months.
2.4.6. Follow-up
There was no requirement to engage in mindfulness practices during the 3-year follow-up period. Paul and his reliabilityraters at work were contacted once every 3 months during this time.
3. Results
Fig. 1 presents Paul’s smoking (i.e., frequencies of cigarette smoked), daily during baseline and intervention, monthlyduring maintenance, and yearly during follow-up. The data show that Paul smoked 12 cigarettes each day during baseline.
Table 2
Outline of the standard Meditation on the Soles of the Feet training for desire to smoke.
Steps of the skill:
1. If you are standing, stand in a natural manner, with the soles of your feet flat on the floor.
2. If you are sitting, sit comfortably with the soles of your feet flat on the floor.
3. Just breathe naturally.
4. Think of times when you really wanted to have a smoke.
5. Fully attend to the desire to smoke.
6. Now, shift all your attention immediately to the soles of your feet.
7. Slowly, move your toes, feel your shoes covering your feet, feel the texture of your socks, the curve of your arch, and the
heels of your feet against the back of your shoes. If you do not have shoes on, feel the floor or carpet with the soles of your feet.
8. Keep breathing naturally and focus on the soles of your feet until you are free from the desire to smoke.
9. Practice this mindfulness exercise until you can use it wherever you have a desire to smoke that you feel you cannot control through
your mindful observation of thoughts meditation practice.
10. Remember that once you are free from the desire to smoke, you can refocus your attention on whatever you choose. Eventually, you may
experience a desire to smoke, but will not give in to that desire.
N.N. Singh et al. / Research in Developmental Disabilities 32 (2011) 1180–1185 1183
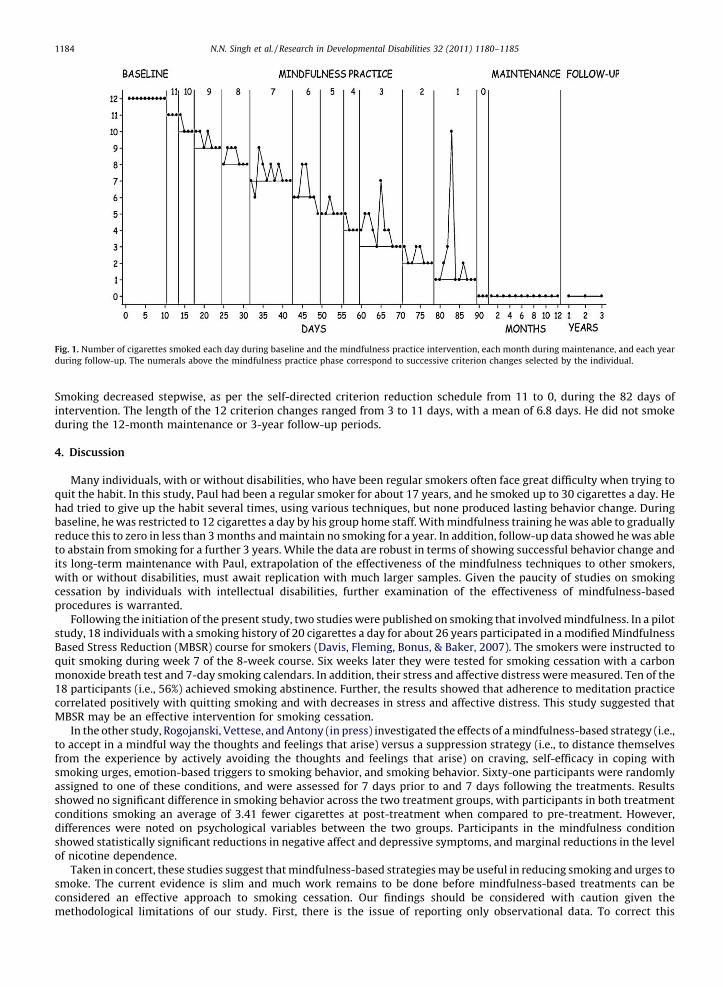
Smoking decreased stepwise, as per the self-directed criterion reduction schedule from 11 to 0, during the 82 days ofintervention. The length of the 12 criterion changes ranged from 3 to 11 days, with a mean of 6.8 days. He did not smokeduring the 12-month maintenance or 3-year follow-up periods.
4. Discussion
Many individuals, with or without disabilities, who have been regular smokers often face great difficulty when trying toquit the habit. In this study, Paul had been a regular smoker for about 17 years, and he smoked up to 30 cigarettes a day. Hehad tried to give up the habit several times, using various techniques, but none produced lasting behavior change. Duringbaseline, he was restricted to 12 cigarettes a day by his group home staff. With mindfulness training he was able to graduallyreduce this to zero in less than 3 months and maintain no smoking for a year. In addition, follow-up data showed he was ableto abstain from smoking for a further 3 years. While the data are robust in terms of showing successful behavior change andits long-term maintenance with Paul, extrapolation of the effectiveness of the mindfulness techniques to other smokers,with or without disabilities, must await replication with much larger samples. Given the paucity of studies on smokingcessation by individuals with intellectual disabilities, further examination of the effectiveness of mindfulness-basedprocedures is warranted.
Following the initiation of the present study, two studies were published on smoking that involved mindfulness. In a pilotstudy, 18 individuals with a smoking history of 20 cigarettes a day for about 26 years participated in a modified MindfulnessBased Stress Reduction (MBSR) course for smokers (Davis, Fleming, Bonus, & Baker, 2007). The smokers were instructed toquit smoking during week 7 of the 8-week course. Six weeks later they were tested for smoking cessation with a carbonmonoxide breath test and 7-day smoking calendars. In addition, their stress and affective distress were measured. Ten of the18 participants (i.e., 56%) achieved smoking abstinence. Further, the results showed that adherence to meditation practicecorrelated positively with quitting smoking and with decreases in stress and affective distress. This study suggested thatMBSR may be an effective intervention for smoking cessation.
In the other study, Rogojanski, Vettese, and Antony (in press) investigated the effects of a mindfulness-based strategy (i.e.,to accept in a mindful way the thoughts and feelings that arise) versus a suppression strategy (i.e., to distance themselvesfrom the experience by actively avoiding the thoughts and feelings that arise) on craving, self-efficacy in coping withsmoking urges, emotion-based triggers to smoking behavior, and smoking behavior. Sixty-one participants were randomlyassigned to one of these conditions, and were assessed for 7 days prior to and 7 days following the treatments. Resultsshowed no significant difference in smoking behavior across the two treatment groups, with participants in both treatmentconditions smoking an average of 3.41 fewer cigarettes at post-treatment when compared to pre-treatment. However,differences were noted on psychological variables between the two groups. Participants in the mindfulness conditionshowed statistically significant reductions in negative affect and depressive symptoms, and marginal reductions in the levelof nicotine dependence.
Taken in concert, these studies suggest that mindfulness-based strategies may be useful in reducing smoking and urges tosmoke. The current evidence is slim and much work remains to be done before mindfulness-based treatments can beconsidered an effective approach to smoking cessation. Our findings should be considered with caution given themethodological limitations of our study. First, there is the issue of reporting only observational data. To correct this
[()TD$FIG]
Fig. 1. Number of cigarettes smoked each day during baseline and the mindfulness practice intervention, each month during maintenance, and each year
during follow-up. The numerals above the mindfulness practice phase correspond to successive criterion changes selected by the individual.
N.N. Singh et al. / Research in Developmental Disabilities 32 (2011) 1180–11851184

limitation, it is becoming increasingly common to verify observational data via carbon monoxide breath tests, plasmanicotine levels, or other indices (Davis et al., 2007; Schnoll, Patterson, Wileyto, Tyndale, Benowitz, & Lerman, 2009). Second,we report data from only a single participant, who could be an atypical example. Nonetheless, our study underscores thepotential value of using mindfulness-based strategies for smoking cessation. The data were reported from a study using arobust changing criterion design, with an extensive follow-up that is a rarity in the smoking cessation field.
References
Barlow, D. H., Nock, M. K., & Hersen, M. (2009). Single case experimental designs: Strategies for studying behavior change. Boston, MA: Allyn & Bacon.Davis, J. M., Fleming, M. F., Bonus, K. A., & Baker, T. B. (2007). A pilot study on mindfulness based stress reduction for smokers. BMC Complementary and Alternative
Medicine, 7, 2doi:10.1186/1472-6882-7-2.Emerson, E., & Turnbull, L. (2005). Self-reported smoking and alcohol use among adolescents with intellectual disabilities. Journal of Intellectual Disabilities, 9, 58–
69.Guindon, G. E., & Boisclair, D. (2003). Past, current, and future trends in tobacco use Available at URL: http://www1.worldbank.org/tobacco/publications.asp.Hymowitz, M., Jaffe, F. E., Gupta, A., & Feuerman, M. (1997). Cigarette smoking among patients with mental retardation and mental illness. Psychiatric Services, 48,
100–102.Kalyva, E. (2007). Prevalence and influences on self-reported smoking among adolescents with mild learning disabilities, attention deficit hyperactivity disorder,
and their typically developing peers. Journal of Intellectual Disabilities, 11, 267–279.Minihan, P. M. (1999). Smoking policies and practices in a state-supported residential system for people with mental retardation. American Journal on Mental
Retardation, 104, 131–142.Peine, H. A., Darvish, R., Blakelock, H., Osborne, J. G., & Jenson, W. R. (1998). Non-aversive reduction of cigarette smoking in two adult men in a residential setting.
Journal of Behavior Therapy and Experimental Psychiatry, 29, 55–65.Rimmer, J. H., Braddock, D., & Marks, B. (1995). Health characteristics and behaviors of adults with mental retardation residing in three living arrangements.
Research in Developmental Disabilities, 16, 489–499.Robertson, J., Emerson, E., Gregory, N., Hatton, C., Turner, S., Kessissoglou, S., et al. (2000). Lifestyle related risk factors for poor health in residential settings for
people with intellectual disabilities. Research in Developmental Disabilities, 21, 469–486.Rogojanski, J., Vettese, L. C., & Antony, M. M. (in press). Coping with cigarette cravings: Comparison of suppression versus mindfulness-based strategies.
Mindfulness.Schnoll, R. A., Patterson, F., Wileyto, E. P., Tyndale, R. F., Benowitz, N., & Lerman, C. (2009). Nicotine metabolic rate predicts successful smoking cessation with
transdermal nicotine: A validation study. Pharmacology, Biochemistry and Behavior, 92, 6–11.Shapiro, S. L., & Carlson, L. E. (2009). The art and science of mindfulness: Integrating mindfulness into psychology and the helping professions. Washington, DC:
American Psychological Association.Singh, N. N., & Leung, J. P. (1988). Smoking cessation through cigarette-fading, self-recording, and contracting: Treatment, maintenance and long-term followup.
Addictive Behaviors, 13, 101–105.Singh, N. N., Singh, J., Adkins, A. D., Singh, A. N., & Winton, A. S. W. (2008). A trainer’s manual for Meditation on the Soles of the Feet: A mindful method for anger
management. Midlothian, VA: ONE Publications.Singh, N. N., Wahler, R. G., Adkins, A. D., & Myers, R. E. (2003). Soles of the feet: A mindfulness-based self-control intervention for aggression by an individual with
mild mental retardation and mental illness. Research in Developmental Disabilities, 24, 158–169.Taylor, N. S., Standen, P. J., Cutajar, P., Fox, D., & Wilson, D. N. (2004). Smoking prevalence and knowledge of associated risks in adult attenders at day centres for
people with learning disabilities. Journal of Intellectual Disability Research, 48, 239–244.Tracy, J., & Hosken, R. (1997). The importance of smoking education and preventive health strategies for people with intellectual disability. Journal of Intellectual
Disability Research, 41, 416–421.
N.N. Singh et al. / Research in Developmental Disabilities 32 (2011) 1180–1185 1185




![Mindfulness Meditation for Chronic Pain: Systematic Review ... · [9], tobacco cessation [10], stress reduction [11], and treat-ment of chronic pain [12–14]. Early mindfulness studies](https://img.pdfslide.us/doc/110x75/5f908b9fe6af09458b2cf1c8/mindfulness-meditation-for-chronic-pain-systematic-review-9-tobacco-cessation.jpg)