Embed Size (px)
Citation preview

Intl. Journal of Clinical and Experimental Hypnosis, 64(4): 434–455, 2016Copyright © International Journal of Clinical and Experimental HypnosisISSN: 0020-7144 print / 1744-5183 onlineDOI: 10.1080/00207144.2016.1209039
EFFECTS OF A HYPNOTIC INDUCTION ANDAN UNPLEASANTNESS-FOCUSED
ANALGESIA SUGGESTION ON PAINCATASTROPHIZING TO AN EXPERIMENTAL
HEAT STIMULUS: A Preliminary Study
Tomonori Adachi
Graduate School of Human Sciences, Osaka University, Osaka, Japan
Aya Nakae
Immunology Frontier Research Center, Osaka University, Osaka, Japan
Jun Sasaki
Graduate School of Human Sciences, Osaka University, Osaka, Japan
Abstract: Pain catastrophizing is associated with greater levels ofpain. While many studies support the efficacy of hypnosis for pain,the effect on pain catastrophizing remains unclear. The present studyevaluated the effect of hypnosis on pain catastrophizing using exper-imental heat stimulation. Twenty-two pain patients engaged in 3 con-ditions: baseline (no suggestion), hypnotic induction, and hypnoticinduction plus analgesia suggestion. Participants with higher baselinepain showed a significant reduction in rumination following hyp-notic induction plus analgesia suggestion and significant reductionsin pain due to both the hypnotic induction alone and the hyp-notic induction plus analgesia suggestion. The findings suggest thatunpleasantness-focused hypnotic analgesia reduces pain via its effecton the rumination component of pain catastrophizing.
Pain catastrophizing is one of the primary psychological factors thatinfluences the experience of pain (Keefe, Rumble, Scipio, Giordano,& Perri, 2004; Linton, 2000). It has been defined as “an exaggeratednegative mental set brought to bear during actual or anticipated painexperience” (Sullivan et al., 2001, p. 53) and has been consistently and
Manuscript submitted December 1, 2014; final revision accepted March 21, 2016.Address correspondence to Tomonori Adachi, MA, Shinri-Kyouiku Soudansitsu,
Graduate School of Human Sciences, Osaka University, 1-2 Yamadaoka, Suita, Osaka565-0871, Japan. E-mail: [email protected]
434

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 435
significantly associated with more pain, more psychological dysfunc-tion, and more physical dysfunction across a wide variety of painpopulations (e.g., Leung, 2012; Quartana, Campbell, & Edwards, 2009).Significant associations between pain catastrophizing and pain havealso been found in laboratory situations (e.g., Gilliam et al., 2010;Roelofs, Peters, van der Zijden, & Vlaeyen, 2004; Sullivan, Thorn,Rodgers, & Ward, 2004).
Although a wide variety of theoretical models of paincatastrophizing have been proposed, including the appraisal model,the attentional model, the communal coping model, and the schema-activation model (Leung, 2012; Quartana et al., 2009; Sullivan et al.,2001), Flink, Boersma, and Linton (2013) have recently proposedviewing pain catastrophizing as a type of repetitive negative thinking.This view is consistent with the idea of catastrophizing as a type ofrepetitive thought process that is intrusive and from which it is difficultto disengage (Ehring et al., 2011). In this model, pain catastrophizingmay be viewed as consisting of two dimensions, that is, both a style ofthinking as well as the content of thoughts. Indeed, the three subscalesof the Pain Catastrophizing Scale (PCS; Sullivan, Bishop, & Pivik,1995)—the most commonly used self-report scale for measuring paincatastrophizing—appear to fall into one of these two dimensions (Flinket al., 2013). The Rumination subscale (“I keep thinking about howmuch it hurts”) can be viewed as a style of thinking, while both theHelplessness subscale (“There’s nothing I can do to reduce the intensityof the pain”) and the Magnification subscale (“I become afraid thatthe pain will get worse”) can be viewed as assessing the content ofthought. Distinguishing these two dimensions provides an alternativeframework for evaluating the effect of specific treatment strategieson catastrophizing, as well as for examining the influence of thesecatastrophizing domains on other pain-related factors.
Although cognitive restructuring (Ehde & Jensen, 2004; Richter et al.,1986; Thorn, Boothby, & Sullivan, 2002) is probably the most com-mon therapeutic strategy for reducing pain-related catastrophizing,researchers have begun to examine the effects of both hypnoticanalgesia (Pukall, Kandyba, Amsel, Khalifé, & Binik, 2007) and hyp-notic cognitive therapy (Ehde & Jensen, 2007; Jensen et al., 2011) oncatastrophizing. Pukall and colleagues conducted a preliminary clin-ical trial of hypnosis for 8 females suffering from vulvar vestibulitissyndrome (VVS). Their hypnotic treatment consisted of six sessionswith suggestions related to relaxation, hypnotic analgesia, and sexualpleasure. An example of a hypnotic analgesia suggestion is “imag-ining the pain as a bright red ball, and then reducing the pain bydulling the color” (Pukall et al., 2007, p. 421). The researchers usedthe PCS to measure participants’ catastrophizing with respect to VVSpain. As a result of the hypnotic treatment, catastrophizing of VVS

436 TOMONORI ADACHI ET AL.
pain decreased significantly between pretreatment and 1-month, and6-month follow-ups. Jensen and his colleagues also conducted a prelim-inary clinical trial investigating the effects of hypnotic cognitive therapyin 15 multiple sclerosis patients with chronic pain. Participants weregiven 16 sessions of the treatment that included four sessions each offour different treatment modules: an education control, self-hypnosistraining, cognitive restructuring, and a combined hypnosis-cognitiverestructuring intervention. Representative suggestions used in theself-hypnosis training module consisted of decreased unpleasantness,increased pain acceptance, decreased awareness of uncomfortable sen-sations, imagined anesthesia, and increased awareness of comfort andcomfortable sensations. The combined intervention module used thefollowing suggestions: increased comfort with ambiguity about con-clusions regarding pain and its impact, focused attention to alterpain-related catastrophizing into more reassuring and realistic cogni-tions and to ponder these types of more adaptive cognitions, and ageprogression to increase the participants’ sense of control over pain andits impact on their lives. In the educational control module, partici-pants were given information about the effect of pain on individualswith multiple sclerosis, the neurophysiology of pain, sleep hygiene,and activity management. Therapists were instructed not to teach anyspecific pain-coping skills such as a relaxation, self-hypnosis, or cogni-tive restructuring skills during the session. The cognitive restructuringmodule consisted of the following four primary components: educationabout the role of cognition in pain, cognitive coping skills acquisition,rehearsal of cognitive coping skills, and encouragement of mainte-nance and generalization of skills. Participants were taught a methodof recording and evaluating catastrophic pain thoughts. Examinationof core beliefs about chronic pain and instructions relating to thought-stopping skills were also provided. Catastrophizing cognition wasmeasured using the PCS. Results of their study showed that lower levelsof catastrophizing occurred after the self-hypnosis training module, thecognitive restructuring module, and the combined intervention moduleas compared with the pretreatment status. The level of catastrophizingafter the combined intervention module was lowest among all fourtreatment modules.
Moreover, a large number of studies support the efficacy of hypno-sis for both acute (Landolt & Milling, 2011; Montgomery, DuHamel,& Redd, 2000; Patterson & Jensen, 2003; Tomé-Pires & Miró, 2012)and chronic pain (Adachi, Fujino, Nakae, Mashimo, & Sasaki, 2014;Elkins, Jensen, & Patterson, 2007; Jensen, 2009; Jensen & Patterson,2006; Montgomery et al., 2000; Patterson & Jensen, 2003; Tomé-Pires& Miró, 2012). Evidence also shows that hypnotic pain treatments canresult in a large number of beneficial “side effects,” such as an increase

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 437
in perceived control over pain, stress reduction, and enhanced well-being (Jensen et al., 2006). These studies support the use of hypnosisfor treating chronic pain in general and perhaps specifically for paincatastrophizing.
However, it is not yet clear how hypnosis reduces paincatastrophizing. Two possible mediating mechanisms are via mindful-ness and one’s style of thinking. It has been pointed out that hypnosisshares some similarities with mindfulness-based treatments such aspromoting acceptance and focusing attention (Lynn, Das, Hallquist, &Williams, 2006), and that mindfulness-based treatments appear to besimilar to the induction phase of hypnosis (Jensen, 2011). For example,both a mindfulness-based approach and a hypnotic induction instruct aparticipant to focus his or her attention on a single sensory experience,such as that of breathing. It has also been reported that mindfulness-based treatments can reduce maladaptive styles of thought in avariety of conditions. For example, Querstret and Cropley (2013)identified 19 studies that demonstrated the efficacy of mindfulness forreducing rumination and worry. In these studies, mindfulness-basedtreatments were effective for reducing rumination in patients withcancer (Campbell, Labelle, Bacon, Faris, & Carlson, 2012), depression(Van Aalderen et al., 2012), and otherwise healthy university students(Jain et al., 2007; Shapiro, Oman, Thoresen, Plante, & Flinders, 2008).From this research, it seems reasonable to hypothesize that a hypnoticinduction alone could reduce the thought style dimension of paincatastrophizing (that is, scores on the Rumination subscale) via itsinfluence on general mindfulness.
Several factors could potentially moderate the effects of hypnosis,including both baseline pain intensity and the specific content of hyp-notic suggestions. For example, Patterson and colleagues found thatindividuals with burns who report higher baseline levels of pain inten-sity (5 or greater on a scale of 1 = no pain to 10 = worst possible pain)experience significant pain reductions following a hypnotic interven-tion, as compared to their pretreatment status and in comparison withpain in a control group (Patterson, Everett, Burns, & Marvin, 1992;Patterson & Ptacek, 1997). The hypnotic intervention in their studiesused a modified version of the Rapid Induction Analgesia procedure(Barber, 1977) for burn wound debridement (Patterson, Questad, &de Lateur, 1989). The suggestions included deepening the hypnoticexperience by using imagery of 20 staircases, feelings of comfort andrelaxation, a suggestion of amnesia, and an analgesia suggestion thatthe body part undergoing debridement would become heavy andnumb. A posthypnotic suggestion of comfort and relaxation during asubsequent dressing change was also provided. In the control group,the patient was told that they received a hypnotic intervention and thatit would be useful to close one’s eyes, count to 20, and imagine oneself

438 TOMONORI ADACHI ET AL.
in a relaxing place prior to burn debridement. With respect to the impor-tance of hypnotic suggestions, De Pascalis and colleagues have shownthat a hypnotic induction plus a glove anesthesia suggestion producedgreater reduction of pain intensity than a hypnotic induction alone (DePascalis, Cacace, & Massicolle, 2004, 2008).
The current study sought to understand better the effects of hypnoticanalgesia on pain catastrophizing in a sample of patients with chronicpain, using an induced noxious heat stimulation model. Based onthe available research, we hypothesized the following: (a) Individualswith higher baseline pain intensity would report significant reduc-tions in both pain intensity and the thought style dimension ofpain catastrophizing (as assessed by the Rumination subscale of thePCS) following a hypnotic induction alone and a hypnotic inductionplus analgesia suggestion, when compared to a no-hypnotic sugges-tion condition; and (b) among individuals with higher baseline painintensity, reductions in pain intensity and the thought style of paincatastrophizing following hypnotic induction plus analgesia suggestionwould be greater following hypnotic induction alone. If the two hypno-sis conditions reduced the thought style of pain catastrophizing, we alsoanticipated that they would reduce pain via the effects of hypnosis onthe thought style.
Method
ParticipantsThe study participants consisted of a convenience sample of outpa-
tients at a university hospital pain clinic. Study inclusion criteria werethe following: (a) attending the pain clinic with pain as the primarypresenting problem; (b) age 16 years or older; (c) ability to read andwrite Japanese; and (d) willingness to participate in the present study.Participants were classified as high baseline pain intensity (HBP) or lowbaseline pain intensity (LBP), based on pain-intensity ratings using aVisual Analogue Scale anchored with 0 = No pain and 10 = Worst possi-ble pain. The participants with scores greater than or equal to 5.0 in thebaseline condition were assigned to the HBP group and the remainingparticipants with scores less than 5.0 were assigned to the LBP group.The study was approved by the Institutional Review Board for ClinicalResearch at Osaka University Hospital, and written informed consentwas obtained from all participants prior to participation.
MaterialsPain catastrophizing: The Pain Catastrophizing Scale (PCS). The Pain
Catastrophizing Scale (PCS) is a 13-item self-report questionnairethat measures maladaptive thoughts regarding pain (Sullivan et al.,1995). Each item is rated on a 5-point Likert-type scale. The PCS is

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 439
scored on three subscales assessing helplessness, magnification, andrumination. The Japanese version of the PCS used in this study has beenshown to have excellent reliability for the Helplessness (Cronbach’salpha = .81) and Rumination (Cronbach’s alpha = .80) scales, andmarginal reliability for the Magnification scale (Cronbach’s alpha = .65;Matsuoka & Sakano, 2007). In the Japanese version of the PCS, Item1, which is usually scored as a part of the Helplessness scale whenadministered to English-speaking individuals, is scored as a part of theRumination scale.
Pain intensity: Visual Analogue Scale (VAS). The Visual Analogue Scale(VAS) for measuring pain intensity consisted of a 10-centimeter lineanchored by two extremes of pain intensity, namely 0 = No pain and10 = Worst possible pain. The participants were asked to make a mark onthe line that best represented their recalled level of pain intensity aftercompletion of one condition. The scale was scored by measuring the dis-tance from the No pain end of the line to participant’s mark. A large bodyof evidence supports the validity of the VAS for assessing pain intensity(Jensen, Karoly, & Braver, 1986; Price, McGrath, Rafii, & Buckingham,1983; Rainville, Carrier, Hofbauer, Bushnell, & Duncan, 1999).
ProcedureThe participants were asked to engage in all three experimental con-
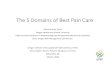
ditions using a within-participants design (see Figure 1). The threeexperimental conditions were baseline (B), hypnotic induction (HI), andhypnotic induction plus analgesia suggestion (HI+AS). A shortenedversion of the B condition was also carried out as a practice trial in orderto accustom participants to an experimental task before starting thethree conditions. Details of the experimental task are described later inthe section explaining the heat stimulation. All participants received theB condition first to control for the residual effect of hypnosis (Hofbauer,Rainville, Duncan, & Bushnell, 2001; Rainville et al., 1999; Rainville,Duncan, Price, Carrier, & Bushnell, 1997). After the B condition, halfof the participants received the HI condition followed by the HI +AS condition. The other half of the participants received the HI + AScondition followed by the HI condition. The two orders of conditions(B→HI→HI+AS and B→HI+AS →HI) were counterbalanced.
Experimental ConditionsDetails of each condition’s procedures are described below. Hypnotic
suggestions and instructions regarding each experimental task wererecorded in advance and provided to the participants during eachcondition via headphones.

440 TOMONORI ADACHI ET AL.
Figure 1. A flowchart of procedure. Note. PCS = Pain Catastrophizing Scale; VAS = VisualAnalogue Scale.
Baseline condition. The participants were asked to sit on a comfort-able, reclining chair with armrests. Before receiving heat stimulation,participants were instructed (a) to detect and count target heat stimuliwithout speaking or taking any action and (b) to look at a mark (sil-ver magnet) placed on the upper part of a wall in front of them and tokeep their eyes open during the heat stimulation as much as they could.No hypnotic suggestions were provided in the B condition. Once theheat stimulation was over, the participants were asked to get up fromthe chair and to rate their catastrophizing and pain intensity during theheat stimulation of the B condition, using the PCS and the VAS.
Hypnotic-induction condition. First, a hypnotic induction was appliedto the participants, who were seated as in the B condition (sitting ona comfortable, reclining chair). We used the eye closure and hand-lowering items of the Japanese version of the Stanford HypnoticSusceptibility Scale, Form A (SHSS:A; Saitoh, 2004; approximately

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 441
20–25 minutes) as suggestions for hypnotic induction. The participantswere instructed to look at the mark on the wall during the initialphase of a hypnotic induction, and then the eye closure suggestionwas followed by the hand-lowering suggestion. After completion of thetwo hypnotic induction suggestions, the participants were instructedto count the target heat stimuli without speaking or taking any spe-cific actions when they would receive the heat stimulation. Then, theywere asked to open their eyes and to keep them open. At the sametime, it was suggested to the participants that they would continueto feel relaxed, calm, and comfortable when they opened their eyes.Subsequently, the heat stimuli were delivered without an analgesia sug-gestion. After receipt of the heat stimuli, the participants were asked toclose their eyes again and to relax. Then, a dehypnotization procedurewas conducted using the dehypnotization procedure of the SHSS:A.In the dehypnotization procedure, an experimenter (audiotape in thepresent experiment) counted back from 20 to 1 and suggested that theparticipants would feel refreshed when the count reached one. Aftercompletion of the dehypnotization procedure, the participants wereasked to complete the PCS and the VAS.
Hypnotic induction plus analgesia suggestion condition. After provid-ing the same hypnotic induction procedure and instructions as theHI condition regarding counting the heat stimuli, a suggestion ofdecreased pain unpleasantness was given. As in the analgesia sug-gestion, the participants received the suggestion that a sensation ofcomfort and well-being would sweep through their arm and spreadto their whole body. They were also given the suggestion that theycould feel the intensity and quality of the heat stimulation while itwas provided, but they would primarily feel comfortable with a senseof well-being. The suggestion used in this study was based on thatof Rainville et al. (1999). The first author (TA) translated the sugges-tion into Japanese and added minor changes to fit the experimentalsituation (e.g., changing “the stimulation” in the original suggestioninto “heat”). We chose the unpleasantness-focused analgesia suggestionbecause pain catastrophizing is particularly associated with the activityof brain regions involved in processing pain unpleasantness (Gracelyet al., 2004; Rainville, 2002). After providing the analgesia suggestion,the participants were asked to open their eyes and to keep them open.They were also provided with the suggestion that feelings of relaxation,calmness, and comfort would continue when they opened their eyes.As in the HI condition, the heat stimulation was followed by the instruc-tions to the participants to reclose their eyes and relax. Immediatelythereafter, the same dehypnotization procedure as in the HI conditionwas conducted, after which the participants completed the PCS and theVAS.

442 TOMONORI ADACHI ET AL.
Heat StimulationHeat stimuli were delivered using a computerized thermal contact
stimulator (Contact-Heat Evoked Potential Stimulator [CHEPS]; MedocAdvanced Medical Systems Ltd., Ramat Yishai, Israel). The CHEPS gen-erates a rapid temperature change (heating rate of 70◦C/sec and coolingrate of 40◦C/sec) via a combination of a heating foil (27 mm in diameter)and a Peltier element for active back-cooling. The probe was attachedto the left forearm with a strap and heat stimuli were delivered to thatlocation, except for 1 participant who had clinical pain in the left fore-arm. This participant received heat stimuli to the right forearm. In eachexperimental condition, heat stimuli were applied using an oddball task(De Pascalis, Magurano, & Bellusci, 1999; Duncan-Johnson & Donchin,1977). The participants completed a block of 70 heat stimuli for eachexperimental condition and a block of 27 stimuli for a practice trial.Two types of heat stimuli were delivered. Infrequent (16% of stimuli)54◦C noxious heat stimuli (target stimuli) were interspersed amongfrequently occurring (84% of stimuli) 44◦C nonnoxious heat stimuli(standard stimuli) in a block of heat stimuli. Target stimulus presen-tation order was pseudorandomized with the criterion that two targetstimuli could not be presented in succession. The interstimulus intervalwas set at a constant 3 seconds. The baseline temperature of the probewas 30◦C. Before the heat stimulation was delivered, participants wereinstructed that they were to count silently the number of target heatstimuli delivered and to keep their eyes open during heat stimulationin all conditions.
Somatosensory Event-Related Potential (SERP) data in response toheat stimulation and hypnosis were recorded additionally, but thesedata are not reported here.
Statistical AnalysesThe statistical analyses were conducted using the Statistical Package
for the Social Sciences 21.0 (IBM Corp, 2012). The dependent vari-ables (rumination, helplessness, magnification, and pain intensity) wereanalyzed using four separate two-way repeated-measures analyses ofvariance (ANOVAs) to examine their changes according to the experi-mental manipulations. Post hoc comparisons were performed using theHolm-Bonferroni method (Holm, 1979), which sets a p value of .05 assignificant. A t test was used to assess differences in age between theHBP and LBP groups.

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 443
Results
Demographic Characteristics of ParticipantsTwenty-four participants began the present study, but 2 declined to
continue the study after the practice trial. The mean age of the remain-ing 22 participants was 69.00 years (SD = 10.54, Range = 46–84). A totalof 55% of participants (n = 12) were female, 50% (n = 11) belonged to theHBP group, and 23% (n = 5) had previous experience of hypnosis. Painduration among the 22 participants was as follows: 6 months or less(n = 2; 9%), from 6 months to 1 year (n = 0; 0%), from 1 year to 3 years(n = 7; 32%), from 3 years to 5 years (n = 8; 36%), and over 5 years(n = 5; 23%). Most participants had chronic pain lasting over 6 months.Pain types included leg pain (n = 6; 27%), low back pain (n = 5; 23%),postherpetic neuralgia (n = 4; 18%), and other types of pain includ-ing rheumatoid arthritis and pain in a group of muscles (n = 7; 32%).The mean level of pain intensity among all participants as assessed bythe VAS in the B condition was 4.97 (SD = 2.55). No significant differ-ences in ages was present between the HBP and LBP participants (HBP:M = 65.91, SD = 10.76; LBP: M = 72.09, SD = 9.83), t (20) = 1.41, p = .175,d = 0.60.
Comparison of Experimental Conditions and Baseline Pain Intensity.Means and standard deviations of all dependent measures are pre-sented in Table 1. Repeated-measures ANOVAs revealed significantinteractions between the experimental condition and baseline painintensity for rumination, F(2, 40) = 5.97, p = .005, η2 = .22, andmagnification, F(2, 40) = 6.21, p = .004, η2 = .23. Post hoc analysisusing the Holm-Bonferroni method revealed a significant reduction ofrumination in the HI+AS condition (p = .014, d = 0.79) and a marginallysignificant reduction in the HI condition (p = .037, d = 0.62) as com-pared to the B condition among HBP participants. No significantdifference was found in rumination between the HI and HI+AS con-ditions among the HBP participants (p = .464, d = 0.14). The post hocanalysis also revealed that the HBP participants reported significantlygreater rumination (p = .008, d = 1.26) and magnification (p = .015,d = 1.14) than the LBP participants in the B condition. There were no sig-nificant interactions, F(2, 40) = 2.39, p = .105, η2 = 0.10, or main effects:experimental condition, F(2, 40) = 0.58, p = .566, η2 = .03; baseline painintensity, F(1, 20) = 1.31, p = .267, η2 = .06, for helplessness.
For pain intensity, repeated-measures ANOVAs revealed a signif-icant interaction between experimental condition and baseline painintensity, F(2, 40) = 5.14, p = .010, η2 = .17, and a main effect of experi-mental condition, F(2, 40) = 4.71, p = .015, η2 = 0.16, and baseline painintensity, F(1, 20) = 18.97, p = .000, η2 = .49. Post hoc analyses usingthe Holm-Bonferroni method revealed reductions in pain intensity in

444 TOMONORI ADACHI ET AL.
Tabl
e1
Mea
nsan
dSt
anda
rdD
evia
tion
sof
Dep
ende
ntV
aria
bles
(N=
22)
Bas
elin
eH
ypno
tic
Ind
ucti
on
Hyp
noti
cIn
duc
tion
+A
nalg
esia
Sugg
esti
on
Dep
end
ent
Var
iabl
es
Bas
elin
ePa
inIn
tens
ity
Mea
nSD
Mea
nSD
Mea
nSD
Con
dit
ion
Eff
ectF
(df)
Con
dit
ion
×B
asel
ine
Pain
Inte
nsit
yE
ffec
tF(d
f)
Rum
inat
ion
Hig
h11
.18 a
6.26
7.36
ab6.
156.
55bc
5.43
0.86
(2,4
0)5.
97∗∗
(2,4
0)L
ow4.
09a
4.91
6.82
a6.
945.
91a
6.14
Hel
ples
snes
sH
igh
6.18
a5.
535.
45a
4.66
4.82
a4.
810.
58(2
,40)
2.39
(2,4
0)L
ow2.
27a
3.47
4.36
a5.
613.
64a
3.47
Mag
nific
atio
nH
igh
3.55
a2.
422.
64a
2.50
2.27
a2.
870.
48(2
,40)
6.21
∗∗(2
,40)
Low
1.00
a2.
052.
09a
2.43
1.82
a2.
60Pa
inIn
tens
ity
Hig
h7.
09a
1.47
5.13
b2.
065.
11b
2.72
4.71
∗(2
,40)
5.14
∗(2
,40)
Low
2.85
a1.
243.
02a
1.47
2.76
a1.
73
Not
e.M
eans
wit
hd
iffe
rent
subs
crip
tsar
esi
gnifi
cant
lyd
iffe
rent
(p<
.05)
from
one
anot
her
for
expe
rim
enta
lcon
dit
ion
effe
cts.
∗ p<
.05.
∗∗p
<.0
1.

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 445
the HI (p = .003, d = 1.10) and HI+AS conditions (p = .002, d = 0.91),relative to the B condition among the HBP participants only. No sig-nificant difference was found between the HI and HI+AS conditionsamong the HBP participants (p = .961, d = 0.01). Post hoc analysesalso revealed that the HBP participants displayed significantly greaterpain intensity than the LBP participants in all three experimental con-ditions (B: p = .000, d = 3.12; HI: p = .012, d = 1.18; HI+AS: p = .025,d = 1.03).
Discussion
The present study sought to better understand the effects of a hyp-notic induction alone and hypnotic analgesia on pain catastrophizingusing an experimental pain model. As predicted, participants withhigher baseline pain intensity evidenced a significant reduction inrumination in the hypnotic induction plus analgesia suggestion con-dition as compared to the baseline condition. Inconsistent with ourhypothesis, the hypnotic induction condition did not produce a sig-nificant reduction in rumination. However, the effect of the hypnoticinduction condition on rumination approached significance and therewas a medium-to-large effect size for the reduction in rumination(d = 0.62), and sample size in the current study was relatively small.Therefore, we can assume that the hypnotic induction reduced therumination component of pain catastrophizing. With respect to painintensity, the participants with higher baseline pain intensity evidencedsignificant reductions in both the hypnotic induction and the hypnoticinduction plus analgesia suggestion conditions as compared to the base-line condition. However, no differences were found in rumination andpain intensity between the two hypnotic conditions.
The findings indicate that hypnotic analgesia suggestions that tar-get the affective component of pain (unpleasantness) have their pri-mary effects on rumination (thought style) and less profound effectson helplessness and magnification (thought content), and that theseeffects are limited to individuals with relatively higher baseline lev-els of pain intensity. Rumination is a particularly important compo-nent of pain catastrophizing, given its strong associations with painintensity (Sullivan & Neish, 1998) and disability (Sullivan, Stanish,Waite, Sullivan, & Tripp, 1998). In the attentional model of paincatastrophizing, Sullivan and colleagues have pointed out that catas-trophizers ruminate more about their pain, and their attentional per-formance is disrupted by anticipation of pain stimulus onset (Sullivanet al., 2001). Thus, attentional focus on pain has a close association

446 TOMONORI ADACHI ET AL.
with pain catastrophizing, especially rumination. In fact, several neu-roimaging studies have illustrated that an increase in activity in brainareas responsible for attention is associated with an increase in paincatastrophizing. Gracely and his colleagues (Gracely et al., 2004) con-ducted a functional magnetic resonance imaging (fMRI) study with29 fibromyalgia patients to examine the association between paincatastrophizing, as measured by the Coping Strategy Questionnaire(CSQ; Rosenstiel & Keefe, 1983), and the brain response to pressurepain stimuli. Results showed that pain-catastrophizing scores, aftercontrolling for self-reported depressive symptoms, were significantlyassociated with increased activity in brain areas related to antici-pation of pain (medial frontal cortex, cerebellum), attention to pain(dorsal anterior cingulate gyrus, dorsolateral prefrontal cortex), emo-tional aspects of pain (claustrum), and motor control (premotor cortex,lentiform nucleus). Seminowicz and Davis (2006) also conducted anfMRI study with 22 healthy volunteers to investigate the effect of paincatastrophizing as measured by the PCS on brain activity to two levelsof electric nerve stimulation (mild and moderate pain). In completingthe PCS, participants were instructed to consider their reactions to painexperiences in general and not to focus on one specific event. Resultsshowed that pain catastrophizing was associated with activity in corti-cal regions related to affective (insula, rostral anterior cingulate cortex),attentional (dorsolateral prefrontal cortex), and motor aspects (premo-tor cortices) of pain during mild pain. During moderate pain, paincatastrophizing was negatively correlated with activity in the dorsolat-eral prefrontal cortex, which is implicated in the top-down modulationof pain intensity. This small engagement of the dorsolateral prefrontalcortex was interpreted as the lack of control during more intense pain.Interestingly, some areas of the brain, which are impacted by hypnoticanalgesia, overlap with brain areas responsible for attentional mecha-nism such as anterior cingulate and prefrontal cortices (Faymonvilleet al., 2000; Hofbauer et al., 2001; Rainville et al., 1997; Wik, Fischer,Bragée, Finer, & Fredrikson, 1999). This overlap is consistent with thepresent results, suggesting that hypnotic suggestions focusing on theunpleasantness dimension of pain may act on the thought style dimen-sion of pain catastrophizing via its impact on the attentional function ofpain information processing.
Given the potential overlap between hypnosis and mindfulness, assuggested by a number of scientists (Holroyd, 2003; Jensen, 2011; Lynnet al., 2006), a hypnotic induction, namely so-called general hypnosis,may enhance a type of “decentering” from pain experience. Consistentwith this idea, we found a significant reduction in rumination inthe hypnotic induction plus analgesia suggestion condition and amarginally significant reduction in the hypnotic induction condition.

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 447
Mindfulness-based treatments have been shown to be effective treat-ments for reducing pain in a number of studies (Cramer, Haller, Lauche,& Dobos, 2012; Lakhan & Schofield, 2013). These considerations suggestthat “decentering” may mediate at least some of the beneficial effectsof both hypnosis and mindfulness-based treatments. Decentering is theability to observe one’s thoughts and feelings as temporary, objectiveevents in the mind, as opposed to reflections of self that are necessar-ily true (Fresco et al., 2007). It is regarded as one of the fundamentaltherapeutic mechanisms among mindfulness-based treatments (Allen,Bromley, Kuyken, & Sonnenberg, 2009; Bieling et al., 2012; Carmody,Baer, Lykins, & Olendzki, 2009; Teasdale et al., 2002). An individualengaged in decentering can observe one’s experience in a detachedmanner, and then excessive engagement in a repetitive negative thoughtstyle (e.g., rumination) may reduce. McCracken, Gutiérrez-Martínez,and Smyth (2013) reported that decentering, as measured with an 11-item subscale of the Experiences Questionnaire (EQ; Fresco et al., 2007),is significantly associated with the quality of functioning in the chronicpain population. Further investigations are needed to empirically exam-ine the extent to which hypnosis impacts decentering as measured bythe EQ, associations between decentering and specific hypnotic pro-cesses (e.g., absorption and dissociation), and whether the effect ofhypnosis on decentering results in pain reduction.
As predicted, people with higher baseline pain levels displayed sig-nificant alleviation of rumination and pain intensity in the two hypnoticconditions. The present results are consistent with Patterson and col-leagues (Patterson et al., 1992; Patterson & Ptacek, 1997). Patterson,Adcock, and Bombardier (1997) suggested that people who have higherbaseline levels of clinical burn pain may show greater pain reductionbecause of higher motivation to disengage from the pain experienceand a greater willingness to benefit from hypnotic analgesia. This moti-vational factor among individuals who have higher baseline levels ofpain might underlie the decrease in rumination and pain intensity inthe present study.
Generally, lower experimental baseline pain sensitivity consistentlypredicts a greater reduction of chronic pain after therapeutic interven-tions. For example, higher baseline heat pain thresholds were associatedwith a greater reduction of postherpetic neuralgia pain following anopioid treatment (Edwards, Haythornthwaite, Tella, Max, & Raja, 2006).Among female nonmalignant chronic pain patients, higher baselineischemic pain tolerance was associated with a greater improvement inpain due to a 4-week multidisciplinary treatment program including acognitive behavior therapy, graded exercise training, medication man-agement, and physical therapy (Edwards, Doleys, Lowery, & Fillingim,2003). Lower baseline heat pain intensity also predicted improvementsin pain in the vulvar vestibulitis syndrome following a variety of

448 TOMONORI ADACHI ET AL.
treatments such as a biofeedback, cognitive behavior therapy, applica-tion of a hypoallergic agent, and surgery (Granot, Zimmer, Friedman,Lowenstein, & Yarnitsky, 2004). It is reasonable that nonreactivity to atemporal painful stimulation predicts an improvement in distressingchronic pain responses because more extreme behavioral, cognitive, andemotional responses to acute pain can exacerbate and maintain chronicpain symptoms (Flor & Turk, 2011). However, the participants withlower baseline pain levels for experimental heat stimulation showedno significant reduction in catastrophizing and pain intensity for thesame experimental heat stimulation in the two hypnotic conditions.It would be interesting to replicate the present study focusing on clini-cal pain, rather than experimental pain. For patients with clinical pain,experimental pain in the current investigation might have been moretolerable because they could understand the source and duration oftheir experimental pain. They were unlikely to have appraised thatpain as dangerous. If we considered the participants’ clinical pain as adependent variable, significant reductions in catastrophizing and painmight be observed due to hypnosis among participants with lowerexperimental pain levels.
We found pain-intensity reductions in response to a hypnotic induc-tion alone, as well as a hypnotic induction plus an analgesia suggestion,at least among those with higher baseline pain intensity. The effect of thehypnotic induction condition on rumination approached significanceand there was a robust effect size for the reduction in rumination, andthe sample size in the present study was relatively small. Therefore,a hypnotic induction may reduce pain intensity via its effect on therumination component of pain catastrophizing. Further research isneeded with larger samples to examine whether a hypnotic inductionitself has a direct effect on pain intensity or an indirect effect via its effecton rumination.
As another explanation, it is possible that the relaxation suggestionthat was present in the hypnotic induction had an analgesic effect, givenprevious research showing that a hypnotic induction with relaxationsuggestions can reduce the pain intensity evoked by an experimen-tal electric stimulus (Sharav & Tal, 2004) and the pain intensity offibromyalgia patients (Castel, Pérez, Sala, Padrol, & Rull, 2007). Furtherresearch is needed to clarify the specific analgesic effects of relaxationsuggestions.
The present study had several limitations. First, the present resultsmay be attributable to a regression to the mean effect due to group-ing participants based on their baseline pain intensity. Participantswith higher baseline pain might become habituated to subsequentheat stimulation, and participants with lower baseline pain might pro-duce lower pain ratings to the stimulation in the baseline condition.To rule out this effect, it would be necessary to conduct another study

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 449
with a control group, in which participants take part in the baselinecondition repetitively. Second, we used retrospective reporting meth-ods to show changes in pain catastrophizing. Retrospective reportingmay reflect recalled experience rather than the actual extent of paincatastrophizing and pain intensity during each condition. A third limi-tation was that the analgesia suggestion focused only on reductions inpain unpleasantness. Different effects might have occurred if we alsoincluded suggestions for pain-intensity reductions, an increased abil-ity to ignore pain, or dissociation from pain sensations. Given that theresponse to hypnosis depends largely on the wording of the specificsuggestions (Crawford & Gruzelier, 1992; Kihlstrom, 2013; Oakley &Halligan, 2010), further research is needed to determine how differentsuggestions influence the different components of pain catastrophizing.A fourth limitation was the intensity of the experimental stimuli inthe present study. It is possible that the participants considered theheat stimulation relatively tolerable because it was not painful enough.The mean level of pain intensity in the baseline condition among allparticipants was 4.97. Maruo and his colleagues reported that meanclinical pain VAS scores in Japanese chronic neuropathic and non-neuropathic pain patients were lower than the value of the presentstudy (neuropathic pain: mean VAS = 3.8; nonneuropathic pain: meanVAS = 3.6; Maruo et al., 2014). Therefore, we can regard the heatstimulation in the present study as sufficiently painful because themean VAS score in the baseline condition was higher than the scoreof Japanese patients attending a hospital due to their difficulties withchronic pain. A fifth limitation was the lack of assessment of partic-ipants’ hypnotizability. Hypnotizability is one of the most influentialfactors in hypnosis and significantly correlates with hypnotic modu-lation of pain intensity as induced by experimental heat stimulation(Rainville et al., 1999). However, a meta-analysis by Montgomery andcolleagues reported that hypnotizability only accounts for 6% of thevariance in responsiveness to hypnotic interventions for clinical prob-lems, including medical procedural pain and headache (Montgomery,Schnur, & David, 2011). It is possible that effects of hypnotizability oncatastrophizing and pain intensity in the present study were relativelysmall because of the participants’ actual chronic pain.
In summary, our findings indicate that a hypnotic induction plusan unpleasantness-focused analgesia suggestion has a primary influ-ence on the rumination component of pain catastrophizing, but onlyamong those patients with relative high baseline levels of pain inten-sity. Further research is needed to determine if these findings apply toother pain models and when other analgesia suggestions are used, aswell as to determine the mechanisms of these effects.

450 TOMONORI ADACHI ET AL.
Acknowledgments
We would like to thank Dr. Mark Jensen for his helpful commentson an earlier version of this article, and Dr. Toshimasa Saitoh for hisencouragement to carry out the present study.
Funding
This research was supported by the Grant-in-Aid for Japan Societyfor the Promotion of Science (JSPS) Fellows (12J00483) of the JSPS,Japan.
References
Adachi, T., Fujino, H., Nakae, A., Mashimo, T., & Sasaki, J. (2014). A meta-analysis ofhypnosis for chronic pain problems: A comparison between hypnosis, standard care,and other psychological interventions. International Journal of Clinical and ExperimentalHypnosis, 62(1), 1–28.
Allen, M., Bromley, A., Kuyken, W., & Sonnenberg, S. J. (2009). Participants’ experi-ences of mindfulness-based cognitive therapy: “It changed me in just about every waypossible.” Behavioural and Cognitive Psychotherapy, 37, 413–430.
Barber, J. (1977). Rapid induction analgesia: A clinical report. American Journal of ClinicalHypnosis, 19(3), 138–147.
Bieling, P. J., Hawley, L. L., Bloch, R. T., Corcoran, K. M., Levitan, R. D., Young, L. T., &Segal, Z. V. (2012). Treatment-specific changes in decentering following mindfulness-based cognitive therapy versus antidepressant medication or placebo for preventionof depressive relapse. Journal of Consulting and Clinical Psychology, 80, 365–372.
Campbell, T. S., Labelle, L. E., Bacon, S. L., Faris, P., & Carlson, L. E. (2012). Impactof mindfulness-based stress reduction (MBSR) on attention, rumination and restingblood pressure in women with cancer: A waitlist-controlled study. Journal of BehavioralMedicine, 35, 262–271.
Carmody, J., Baer, R. A., Lykins, E. L. B., & Olendzki, N. (2009). An empirical study of themechanisms of mindfulness in a mindfulness−based stress reduction program. Journalof Clinical Psychology, 65, 613–626.
Castel, A., Pérez, M., Sala, J., Padrol, A., & Rull, M. (2007). Effect of hypnotic suggestionon fibromyalgic pain: Comparison between hypnosis and relaxation. European Journalof Pain, 11, 463–468.
Cramer, H., Haller, H., Lauche, R., & Dobos, G. (2012). Mindfulness-based stress reductionfor low back pain: A systematic review. BMC Complementary and Alternative Medicine,12, 162.
Crawford, H. J., & Gruzelier, J. H. (1992). A midstream view of the neuropsychophysi-ology of hypnosis: Recent research and future directions. In E. Fromm & M. R. Nash(Eds.), Contemporary hypnosis research (pp. 227–266). New York, NY: Guilford Press.
De Pascalis, V., Cacace, I., & Massicolle, F. (2004). Perception and modulation of pain inwaking and hypnosis: Functional significance of phase-ordered gamma oscillations.Pain, 112(1), 27–36.
De Pascalis, V., Cacace, I., & Massicolle, F. (2008). Focused analgesia in waking and hyp-nosis: Effects on pain, memory, and somatosensory event-related potentials. Pain, 134,197–208.

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 451
De Pascalis, V., Magurano, M. R., & Bellusci, A. (1999). Pain perception, somatosensoryevent-related potentials and skin conductance responses to painful stimuli in high,mid, and low hypnotizable subjects: Effects of differential pain reduction strategies.Pain, 83, 499–508.
Duncan-Johnson, C. C., & Donchin, E. (1977). On quantifying surprise: The variation ofevent-related potentials with subjective probability. Psychophysiology, 14, 456–467.
Edwards, R. R., Doleys, D. M., Lowery, D., & Fillingim, R. B. (2003). Pain toleranceas a predictor of outcome following multidisciplinary treatment for chronic pain:Differential effects as a function of sex. Pain, 106, 419–426.
Edwards, R. R., Haythornthwaite, J. A., Tella, P., Max, M. B., & Raja, S. (2006). Basalheat pain thresholds predict opioid analgesia in patients with postherpetic neuralgia.Anesthesiology, 104, 1243–1248.
Ehde, D. M., & Jensen, M. P. (2004). Feasibility of a cognitive restructuring interventionfor treatment of chronic pain in persons with disabilities. Rehabilitation Psychology, 49,254–258.
Ehde, D. M., & Jensen, M. P. (2007). Psychological treatments for pain management inpersons with spinal cord injury: Cognitive therapy and self-hypnosis training. Topicsin Spinal Cord Injury Rehabilitation, 13(2), 72–80.
Ehring, T., Zetsche, U., Weidacker, K., Wahl, K., Schönfeld, S., & Ehlers, A. (2011). ThePerseverative Thinking Questionnaire (PTQ): Validation of a content-independentmeasure of repetitive negative thinking. Journal of Behavior Therapy and ExperimentalPsychiatry, 42, 225–232.
Elkins, G., Jensen, M. P., & Patterson, D. R. (2007). Hypnotherapy for the management ofchronic pain. International Journal of Clinical and Experimental Hypnosis, 55, 275–287.
Faymonville, M. E., Laureys, S., Degueldre, C., DelFiore, G., Luxen, A., Franck, G.,& Maquet, P. (2000). Neural mechanisms of antinociceptive effects of hypnosis.Anesthesiology, 92, 1257–1267.
Flink, I. L., Boersma, K., & Linton, S. J. (2013). Pain catastrophizing as repetitive nega-tive thinking: A development of the conceptualization. Cognitive Behaviour Therapy,42, 215–223.
Flor, H., & Turk, D. C. (2011). Chronic pain: An integrated biobehavioral approach. Seattle, WA:IASP Press.
Fresco, D. M., Moore, M. T., Van Dulmen, M. H., Segal, Z. V., Ma, S. H., Teasdale, J. D.,& Williams, J. M. G. (2007). Initial psychometric properties of the experiences ques-tionnaire: Validation of a self-report measure of decentering. Behavior Therapy, 38,234–246.
Gilliam, W., Burns, J. W., Quartana, P., Matsuura, J., Nappi, C., & Wolff, B. (2010).Interactive effects of catastrophizing and suppression on responses to acute pain: Atest of an appraisal × emotion regulation model. Journal of Behavioral Medicine, 33,191–199.
Gracely, R. H., Geisser, M. E., Giesecke, T., Grant, M. A. B., Petzke, F., Williams, D. A., &Clauw, D. J. (2004). Pain catastrophizing and neural responses to pain among personswith fibromyalgia. Brain: A Journal of Neurology, 127, 835–843.
Granot, M., Zimmer, E. Z., Friedman, M., Lowenstein, L., & Yarnitsky, D. (2004).Association between quantitative sensory testing, treatment choice, and subsequentpain reduction in vulvar vestibulitis syndrome. The Journal of Pain, 5, 226–232.
Hofbauer, R. K., Rainville, P., Duncan, G. H., & Bushnell, M. C. (2001). Cortical represen-tation of the sensory dimension of pain. Journal of Neurophysiology, 86(1), 402–411.
Holm, S. (1979). A simple sequentially rejective multiple test procedure. ScandinavianJournal of Statistics, 6(2), 65–70.
Holroyd, J. (2003). The science of meditation and the state of hypnosis. American Journal ofClinical Hypnosis, 46(2), 109–128.
IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY:IBM Corp.

452 TOMONORI ADACHI ET AL.
Jain, S., Shapiro, S. L., Swanick, S., Roesch, S. C., Mills, P. J., Bell, I., & Schwartz, G. E.(2007). A randomized controlled trial of mindfulness meditation versus relaxationtraining: Effects on distress, positive states of mind, rumination, and distraction.Annals of Behavioral Medicine, 33(1), 11–21.
Jensen, M., & Patterson, D. R. (2006). Hypnotic treatment of chronic pain. Journal ofBehavioral Medicine, 29(1), 95–124.
Jensen, M. P. (2009). Hypnosis for chronic pain management: A new hope. Pain, 146,235–237.
Jensen, M. P. (2011). Psychosocial approaches to pain management: An organizationalframework. Pain, 152, 717–725.
Jensen, M. P., Ehde, D. M., Gertz, K. J., Stoelb, B. L., Dillworth, T. M., Hirsh, A. T., & Kraft,G. H. (2011). Effects of self-hypnosis training and cognitive restructuring on daily painintensity and catastrophizing in individuals with multiple sclerosis and chronic pain.International Journal of Clinical and Experimental Hypnosis, 59(1), 45–63.
Jensen, M. P., Karoly, P., & Braver, S. (1986). The measurement of clinical pain intensity: Acomparison of six methods. Pain, 27(1), 117–126.
Jensen, M. P., McArthur, K. D., Barber, J., Hanley, M. A., Engel, J. M., Romano, J. M., &Patterson, D. R. (2006). Satisfaction with, and the beneficial side effects of, hypnoticanalgesia. International Journal of Clinical and Experimental Hypnosis, 54, 432–447.
Keefe, F. J., Rumble, M. E., Scipio, C. D., Giordano, L. A., & Perri, L. M. (2004).Psychological aspects of persistent pain: Current state of the science. The Journal ofPain, 5, 195–211.
Kihlstrom, J. F. (2013). Neuro-hypnotism: Prospects for hypnosis and neuroscience. Cortex:A Journal Devoted to the Study of the Nervous System and Behavior, 49, 365–374.
Lakhan, S. E., & Schofield, K. L. (2013). Mindfulness-based therapies in the treatment ofsomatization disorders: A systematic review and meta-analysis. PloS One, 8, e71834.
Landolt, A. S., & Milling, L. S. (2011). The efficacy of hypnosis as an intervention forlabor and delivery pain: A comprehensive methodological review. Clinical PsychologyReview, 31, 1022–1031.
Leung, L. (2012). Pain catastrophizing: An updated review. Indian Journal of PsychologicalMedicine, 34, 204–217.
Linton, S. J. (2000). A review of psychological risk factors in back and neck pain. Spine, 25,1148–1156.
Lynn, S. J., Das, L. S., Hallquist, M. N., & Williams, J. C. (2006). Mindfulness, acceptance,and hypnosis: Cognitive and clinical perspectives. International Journal of Clinical andExperimental Hypnosis, 54, 143–166.
Maruo, T., Nakae, A., Maeda, L., Shi, K., Takahashi, K., Morris, S., & Saitoh, Y. (2014).Validity, reliability, and assessment sensitivity of the Japanese version of the short-form McGill Pain Questionnaire 2 in Japanese patients with neuropathic and non-neuropathic pain. Pain Medicine, 15, 1930–1937.
Matsuoka, H., & Sakano, Y. (2007). Assessment of cognitive aspect of pain: Development,reliability, and validation of Japanese version of pain catastrophizing scale (inJapanese). Japanese Journal of Psychosomatic Medicine, 47(2), 95–102.
McCracken, L. M., Gutiérrez-Martínez, O., & Smyth, C. (2013). “Decentering” reflects psy-chological flexibility in people with chronic pain and correlates with their quality offunctioning. Health Psychology, 32, 820–823.
Montgomery, G. H., DuHamel, K. N., & Redd, W. H. (2000). A meta-analysis of hypnoti-cally induced analgesia: How effective is hypnosis? International Journal of Clinical andExperimental Hypnosis, 48(2), 138–153.
Montgomery, G. H., Schnur, J. B., & David, D. (2011). The impact of hypnotic suggestibil-ity in clinical care settings. International Journal of Clinical and Experimental Hypnosis, 59,294–309.

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 453
Oakley, D. A., & Halligan, P. W. (2010). Psychophysiological foundations of hypnosis andsuggestion. In S. J. Lynn, J. W. Rhue, & I. Kirsch (Eds.), Handbook of clinical hypnosis(2nd ed., pp. 79–117). Washington, DC: American Psychological Association.
Patterson, D. R., Adcock, R. J., & Bombardier, C. H. (1997). Factors predicting hyp-notic analgesia in clinical burn pain. International Journal of Clinical and ExperimentalHypnosis, 45, 377–395.
Patterson, D. R., Everett, J. J., Burns, G. L., & Marvin, J. A. (1992). Hypnosis for thetreatment of burn pain. Journal of Consulting and Clinical Psychology, 60, 713–717.
Patterson, D. R., & Jensen, M. P. (2003). Hypnosis and clinical pain. Psychological Bulletin,129, 495–521.
Patterson, D. R., & Ptacek, J. T. (1997). Baseline pain as a moderator of hypnotic analgesiafor burn injury treatment. Journal of Consulting and Clinical Psychology, 65(1), 60–67.
Patterson, D. R., Questad, K. A., & de Lateur, B. J. (1989). Hypnotherapy as an adjunct tonarcotic analgesia for the treatment of pain for burn debridement. American Journal ofClinical Hypnosis, 31(3), 156–163.
Price, D. D., McGrath, P. A., Rafii, A., & Buckingham, B. (1983). The validation of visualanalogue scales as ratio scale measures for chronic and experimental pain. Pain, 17(1),45–56.
Pukall, C., Kandyba, K., Amsel, R., Khalifé, S., & Binik, Y. (2007). Effectiveness of hypnosisfor the treatment of vulvar vestibulitis syndrome: A preliminary investigation. TheJournal of Sexual Medicine, 4, 417–425.
Quartana, P. J., Campbell, C. M., & Edwards, R. R. (2009). Pain catastrophizing: A criticalreview. Expert Review of Neurotherapeutics, 9, 745–758.
Querstret, D., & Cropley, M. (2013). Assessing treatments used to reduce ruminationand/or worry: A systematic review. Clinical Psychology Review, 33, 996–1009.
Rainville, P. (2002). Brain mechanisms of pain affect and pain modulation. Current Opinionin Neurobiology, 12, 195–204.
Rainville, P., Carrier, B., Hofbauer, R. K., Bushnell, M. C., & Duncan, G. H. (1999).Dissociation of sensory and affective dimensions of pain using hypnotic modulation.Pain, 82, 159–171.
Rainville, P., Duncan, G. H., Price, D. D., Carrier, B., & Bushnell, M. C. (1997). Painaffect encoded in human anterior cingulate but not somatosensory cortex. Science, 277,968–971.
Richter, I. L., McGrath, P. J., Humphreys, P. J., Goodman, J. T., Firestone, P., & Keene, D.(1986). Cognitive and relaxation treatment of paediatric migraine. Pain, 25, 195–203.
Roelofs, J., Peters, M. L., van der Zijden, M., & Vlaeyen, J. W. (2004). Does fear of painmoderate the effects of sensory focusing and distraction on cold pressor pain in pain-free individuals? The Journal of Pain, 5, 250–256.
Rosenstiel, A. K., & Keefe, F. J. (1983). The use of coping strategies in chronic low back painpatients: Relationship to patient characteristics and current adjustment. Pain, 17(1),33–44.
Saitoh, T. (2004). The Japanese version of the Stanford Hypnotic Susceptibility Scale Form A.Kyoto, Japan: Dental-Psychological Association.
Seminowicz, D. A., & Davis, K. D. (2006). Cortical responses to pain in healthy individualsdepends on pain catastrophizing. Pain, 120, 297–306.
Shapiro, S. L., Oman, D., Thoresen, C. E., Plante, T. G., & Flinders, T. (2008). Cultivatingmindfulness: Effects on well-being. Journal of Clinical Psychology, 64, 840–862.
Sharav, Y., & Tal, M. (2004). Focused analgesia and generalized relaxation produce dif-ferential hypnotic analgesia in response to ascending stimulus intensity. InternationalJournal of Psychophysiology, 52, 187–196.
Sullivan, M. J., Bishop, S. R., & Pivik, J. (1995). The Pain Catastrophizing scale:Development and validation. Psychological Assessment, 7, 524–532.
Sullivan, M. J., & Neish, N. R. (1998). Catastrophizing, anxiety and pain during dentalhygiene treatment. Community Dentistry and Oral Epidemiology, 26, 344–349.

454 TOMONORI ADACHI ET AL.
Sullivan, M. J., Stanish, W., Waite, H., Sullivan, M., & Tripp, D. A. (1998). Catastrophizing,pain, and disability in patients with soft-tissue injuries. Pain, 77, 253–260.
Sullivan, M. J., Thorn, B., Haythornthwaite, J. A., Keefe, F., Martin, M., Bradley, L. A., &Lefebvre, J. C. (2001). Theoretical perspectives on the relation between catastrophizingand pain. The Clinical Journal of Pain, 17(1), 52–64.
Sullivan, M. J., Thorn, B., Rodgers, W., & Ward, L. C. (2004). Path model of psychologicalantecedents to pain experience: Experimental and clinical findings. The Clinical Journalof Pain, 20, 164–173.
Teasdale, J. D., Moore, R. G., Hayhurst, H., Pope, M., Williams, S., & Segal, Z. V. (2002).Metacognitive awareness and prevention of relapse in depression: Empirical evidence.Journal of Consulting and Clinical Psychology, 70, 275–287.
Thorn, B. E., Boothby, J. L., & Sullivan, M. J. (2002). Targeted treatment of catastrophizingfor the management of chronic pain. Cognitive and Behavioral Practice, 9(2), 127–138.
Tomé-Pires, C., & Miró, J. (2012). Hypnosis for the management of chronic and cancerprocedure-related pain in children. International Journal of Clinical and ExperimentalHypnosis, 60, 432–457.
Van Aalderen, J. R., Donders, A. R. T., Giommi, F., Spinhoven, P., Barendregt, H. P.,& Speckens, A. E. M. (2012). The efficacy of mindfulness-based cognitive therapyin recurrent depressed patients with and without a current depressive episode: Arandomized controlled trial. Psychological Medicine, 42, 989–1001.
Wik, G., Fischer, H., Bragée, B., Finer, B., & Fredrikson, M. (1999). Functional anatomyof hypnotic analgesia: A PET study of patients with fibromyalgia. European Journal ofPain, 3(1), 7–12.
Effekte einer hypnotischen Induktion und eineUnannehmlichkeits-fokussierte Analgesie-Suggestion bezogen auf die
Katastrophisierung von Schmerzen infolge eines experimentellenHitzereizes: Eine vorläufige Studie
Tomonori Adachi, Aya Nakae und Jun SasakiAbstract: Die Katastrophisierung von Schmerz ist mit höherenSchmerzleveln assoziiert. Während viele Studien die Effizienz von Hypnosebei Schmerzen unterstützen, bleibt der Effekt auf die Katastrophisierungvon Schmerz unklar. Die aktuelle Studie untersuchte den Effekt vonHypnose auf die Katastrophisierung von Schmerz mittels experimentellerHitzestimulation. 22 Schmerzpatienten wurden 3 Bedingungen zugeordnet:Baseline (keine Suggestion), hypnotische Induktion und hypnotischeInduktion plus Suggestion einer Analgesie. Teilnehmer mit höherembaseline Schmerz zeigten eine signifikante Reduktion der Ruminationauf hypnotische Induktion plus Suggestion einer Analgesie und sig-nifikante Reduktion von Schmerz infolge der hypnotischen Induktion alleinund der hypnotischen Induktion plus Suggestion einer Analgesie. DieErgebnisse lassen vermuten, daß eine Unannehmlichkeiten-fokussiertehypnotische Analgesie den Schmerz mittels ihres Effektes auf dieRuminationskomponente der Schmerzkatastrophisierung vermindernkann.
Stephanie Reigel, MD

HYPNOTIC ANALGESIA FOR PAIN CATASTROPHIZING 455
Effets d’une suggestion d’analgésie axée sur le malaise et d’une inductionhypnotique sur la dramatisation de la douleur à la suite d’un stimulus
thermique expérimental: une étude préliminaire
Tomonori Adachi, Aya Nakae et Jun SasakiRésumé: La dramatisation de la douleur est associée à des niveaux supérieursde douleur. Si de nombreuses études confirment l’efficacité de l’hypnose poursoulager la douleur, l’effet que peut avoir la dramatisation de la douleur surcelle-ci demeure difficile à déterminer. Cette étude a permis d’évaluer l’effetde l’hypnose sur la dramatisation de la douleur à l’aide d’une stimulationthermique expérimentale. Vingt-deux patients éprouvant des douleurs ontété répartis en trois groupes: un groupe de base (absence de suggestion),un groupe avec induction hypnotique, et un groupe avec induction hyp-notique et suggestion d’analgésie. Les participants ayant éprouvé les plusfortes douleurs au début de l’étude ont signalé une réduction significative deleurs ruminations après l’induction hypnotique avec suggestion d’analgésie,et une réduction significative de leurs douleurs à la suite de l’induction hyp-notique seule et de l’induction hypnotique avec suggestion d’analgésie. Cesrésultats semblent indiquer que l’analgésie hypnotique axée sur le malaiseréduit la douleur par son effet sur l’aspect rumination de la dramatisation dela douleur.
Johanne ReynaultC. Tr. (STIBC)
Efectos de una inducción hipnótica y una sugerencia de analgesia enfocadahacia lo desagradable en la catastrofización del dolor ante un estímulo
experimental de calor: Un estudio preliminar.
Tomonori Adachi, Aya Nakae y Jun SasakiResumen: Catastrofizar el dolor está asociado con mayores niveles de dolor.Mientras muchos estudios sustentan la eficacia de la hipnosis para el dolor,el efecto sobre la catastrofización del dolor permanece incierto. El presenteestudio evaluó el efecto de la hipnosis en la catastrofización del dolor usandouna estimulación experimental de calor. Veintidós pacientes participaron entres condiciones: línea basal (sin sugerencias), inducción hipnótica, e induc-ción hipnótica más sugerencias de analgesia. Los participantes con una líneabasal de dolor más alta mostraron una reducción significativa en rumiacióndespués de la inducción hipnótica más sugerencias de analgesia y reduc-ciones significativas de dolor debido tanto a la inducción hipnótica por sí solay la inducción hipnótica más sugerencias de analgesia. Estos hallazgos sug-ieren que la analgesia hipnótica enfocada a lo desagradable reduce el dolora través de sus efectos en el componente de rumiación en la catastrofizacióndel dolor.
Omar Sánchez-Armáss CappelloAutonomous University of San Luis Potosi,Mexico