Embed Size (px)
Citation preview

Strahlenther Onkol 1999;175:382–6 (Nr. 8)382
Originalarbeit
Effectiveness of Hypofractionated Radiotherapy in PainfulBone MetastasesTwo Prospective Studies with 1 ´ 4 Gy and 4 ´ 4 Gy
Michael Bremer1, Dirk Rades1, Marga Blach1, Barbara Krenkel2, Johann Hinrich Karstens1
Background: Although effectiveness of fractionated radiotherapy for painful bone metastases is well documented, thereare unanswered questions regarding the adequacy of low-dose short radiation schedules for long-term pain controlwhich give maximum benefit in patients with a short life expectancy.Patients and Methods: Two consecutive non-randomized prospective follow-up studies were performed at a single insti-tution to analyze pain response and duration of response in patients with a variety of primary tumors. Included were on-ly patients with symptomatic nonvertebral bone metastases and without impending pathologic fracture. Forty-five pa-tients received 1 ́ 4 Gy to 50 different sites (group I) while 86 patients received 4 ́ 4 Gy to 96 sites (group II). Pain reliefto irradiation was evaluated according to patient interviews using a 4-point categorical scale. Follow-up was performed7 and 90 days after radiotherapy.Results: Pain relief after 4 ´ 4 Gy was significantly superior to 1 ´ 4 Gy with pain control rates being 86.5% vs 48% atday 7 (after end of treatment) and 80% vs 55% at day 90, respectively. A subgroup analysis of patients treated with 4 ´4 Gy demonstrated a more favorable outcome for breast cancer patients in comparison to patients with other primariesconcerning pain relief (96% vs 81%), pain control after 90 days (93% vs 72%), median time to pain progression (9 vs 3months), and median overall survival (14 vs 5.5 months).Conclusions: In this study 4 ´ 4 Gy proved to be clearly superior to 1 ´ 4 Gy in relieving pain from symptomatic nonver-tebral bone metastases without impending pathologic fracture. Even if radiotherapy with 1 single fraction seems to beapplicable in specific cases doses higher than 4 Gy should be chosen. In breast cancer patients pain control seems to bebetter compared to other primaries.
Key Words: Radiotherapy · Fractionation · Bone metastases · Pain relief
Wirksamkeit der hypofraktionierten Strahlentherapie bei schmerzhaften Knochenmetastasen. Zwei prospektive Studien mit 1 ´ 4 und 4 ´ 4 Gy
Hintergrund: Obwohl die Strahlentherapie schmerzhafter Knochenmetastasen als etabliertes Verfahren anzusehen ist,gibt es weiterhin offene Fragen zur Angemessenheit der Kurzzeitbestrahlung hinsichtlich lokaler Schmerzkontrolle beiPatienten mit begrenzter Lebenserwartung.Patienten und Methode: In zwei monoinstitutionellen, nichtrandomisierten, prospektiven Follow-up-Studien wurdendie Ansprechrate und Remissionsdauer der Bestrahlung von Patienten mit schmerzhaften Knochenmetastasen ver-schiedenen Ursprungs untersucht, welche ausschließlich außerhalb der Wirbelsäule lagen und nicht frakturgefährdetwaren. 45 Patienten erhielten eine Einmalbestrahlung (single shot) in Höhe von 1 ´ 4 Gy auf 50 Lokalisationen (Grup-pe I), während 86 Patienten vier Fraktionen in Höhe von 4 Gy auf 96 Lokalisationen erhielten (Gruppe II). DasSchmerzansprechen wurde sieben und 90 Tage nach Bestrahlung mittels einer Vier-Punkte-Schmerzskala analysiert.Ergebnisse: Die lokale Schmerzkontrolle nach 4 ́ 4 Gy war derjenigen nach 1 ́ 4 Gy signifikant überlegen mit Schmerz-kontrollraten an Tag 7 (nach Therapieende) von 86,5% vs. 48% und an Tag 90 von 80% vs. 55%. Die Subgruppenana-lyse der Behandlungsgruppe mit 4 ´ 4 Gy zeigte günstigere Therapieresultate bei Brustkrebspatienten (n = 28) gegen-über Patienten mit anderer Tumordiagnose bezüglich primärem Schmerzansprechen (96% vs. 81%), lokalerSchmerzkontrollrate nach 90 Tagen (93% vs. 72%), medianem Intervall bis zur Schmerzprogression (neun vs. drei Mo-nate) und medianem Gesamtüberleben (14 vs. 5,5 Monate).Schlußfolgerungen: In dieser Studie konnte die Überlegenheit von 4 ´ 4 Gy gegenüber 1 ´ 4 Gy in der analgetischen Be-strahlung von Knochenmetastasen, welche außerhalb der Wirbelsäule lagen und nicht frakturgefährdet waren, gezeigt wer-den. Soweit in bestimmten Situtionen eine Einmalbestrahlung angestrebt wird, sollte die gewählte Dosis mehr als 4 Gy be-tragen. Bei Brustkrebspatienten scheint eine bessere Schmerzkontrolle erreichbar zu sein als bei anderen Primärtumoren.
Schlüsselwörter: Strahlentherapie · Fraktionierung · Knochenmetastasen · Schmerzbestrahlung
Strahlentherapieund Onkologie © Urban & Vogel 1999
1Department of Radiation Oncology, Medical School Hannover, 2Department of Radiation Oncology, Klinikum Technical University Aachen, Germany.
Herrn Univ.-Professor Dr. Dr. J. Ammon zum 65. Geburtstag.
Submitted: 9 Feb 1999.Accepted: 26 May 1999.
STO 663 Bremer UB-neu 25.08.1999 7:55 Uhr Seite 382

Bremer M, et al. Hypofractionated Radiotherapy in Painful Bone Metastases
Strahlenther Onkol 1999;175:382–6 (Nr. 8) 383
Considerable differences in clinical practice are existingamong radiotherapists in palliative treatment of bone metas-tases with fractionation schedules ranging from 1 to 15 or 20fractions. Low-dose short-term radiotherapy is of specialinterest in patients with limited life expectancy when pain re-lief is the predominant aim of therapy because of its mini-mum disruption of the patients remaining life.
In contrast of the large number of analgetic radiotherapytreatments rather few prospective studies have been publishedevaluating the degree and duration of response. Prospectivestudies involving a well definded group of patients may help todefine a more individualized radiotherapeutic approach.
We present a single institution prospective follow-up studycomparing the efficacy of 2 different fractionation schedulesin patients with painful nonvertebral bone metastases.
Patients and Methods
During a time period of 24 months 2 prospective follow-upstudies were performed consecutively at a single institutionto analyze response rates and duration of response in pa-tients with symptomatic bone metastases of a variety of pri-mary tumors where pain relief was the predominant aim oftherapy. Previously published data from a smaller series[12] were included. Patients were eligible only when multi-ple metastases (bone or visceral) were present and the esti-mated life expectancy was 6 months or less. Treatment siteswere restricted to non weight-bearing bones with portalslength not exceeding 14 cm to prevent treatment relatedtoxicity. Patients with a solitary metastasis or with metasta-ses in weight-bearing bones including the vertebral column
and those with manifest or impending pathologic fracturewere not included and received conventionally fractionatedtreatment schedules.
Patients and tumor characteristics are shown in Table 1. Inthe first study 45 patients (group I) received analgetic radio-therapy to 50 different sites, in the second study 86 patients (group II) were treated at 96 different sites. Systemic (endo-crine or cytostatic) therapy was not changed 6 weeks prior toinitiation of radiotherapy, analgesics consumption was con-stant at least 7 days prior to irradiation.
Treatment consisted of 1 single fraction of 4 Gy in group Iand 4 fractions of 4 Gy given once weekly (43 patients) ortwice weekly (43 patients) in group II resulting in an overalltreatment time of 1 day (group I) and 12 respectvely 21 days(group II). Radiotherapy was performed either by a singlefield (60-cobalt or electron beam) or 2 opposing fields (60-cobalt).
Pain relief to local field radiotherapy was evaluated prospec-tively according to patient interviews using a subjective 4-point categorical scale (none, mild, moderate, severe). Painscores and analgesics consumption were recorded before in-itiation of treatment, at day 7 after end of treatment and day90 by the same physician. The succeeding follow-up was per-formed by contacting the involved general practitioner or bydirect telephone interview.
Response was defined as an improved rating by at least 1point on the pain chart compared to pretreatment value withthe same or reduced analgesic requirements. The period ofresponse was computed from the first day of treatment to thedate of first observation of pain progression or an increase ofanalgesics dose. Progression was defined as an increase in the pain score or the analgesics dose as compared with pre-treatment levels. Six patients were lost to follow-up after median 16 months, all other patients could be followed untildeath.
Statistical Analysis: The data were analyzed using a commer-cially available software package (SPSS win). Duration ofpain control was calculated from the date of study entry until
Group I Group II(1 ´ 4 Gy) (4 ´ 4 Gy)
Number of patients 45 86Male/female 24/21 38/48Median age (range) 65 (45–71) years 62 (25–88) yearsMedian ECOG performance status (range) 2 (1–4) 2 (1–3)Primary tumor
Breast 14 (31%) 28 (32.6%)Lung 12 (27%) 18 (20.9%)Prostate 7 (15%) 9 (10.5%)Plasmacytoma 4 (9%) 8 (9.3%)Others 8 (18%) 23 (26.7%)
Treated sites 50 96Shoulder 8 (16%) 19 (19.8%)Ribs 16 (32%) 19 (19.8%)Pelvic 19 (38%) 45 (46.9%)Others 7 (14%) 13 (13.5%)
Median follow-up (range) 6 (0.5–48) months 7 (0.5–74) months
Table 1. Patient and tumor characteris-tics.
Tabelle 1. Patienten- und Tumorcha-rakteristika.
Bone metastases are a frequent source of considerablemorbidity in cancer patients with pain as the most com-
mon symptom. Local field radiotherapy has been well docu-mented as a method for alleviating pain in the majority of pa-tients with few side effects, especially in those patients with asingle or only few symptomatic sites. However, uncertaintyremains regarding the relationship between optimum doselevel or fractionation and the incidence and duration of painrelief.
STO 663 Bremer UB-neu 25.08.1999 7:55 Uhr Seite 383

Strahlenther Onkol 1999;175:382–6 (Nr. 8)384
Bremer M, et al. Hypofractionated Radiotherapy in Painful Bone Metastases
pain progression. Patients who were lost to follow-up or diedduring the pain assessment period were censored from thetime of the last contact. The Kaplan-Meier method was usedto calculate duration of pain control and survival rates. Log-rank tests were used to compare treatment results.
Results
Both treatment groups were comparable regarding age, pri-mary tumors and treated sites. Response rates 1 week afterthe first fraction in group I and group II were 44% and 38%,respectively. Pain relief at day 7 after end of treatment andday 90 as well as duration of pain relief in the respectivetreatment group differed significantly in favor of the grouptreated by 4 ´ 4 Gy (Table 2). Although single fraction radio-
therapy (group I) showed some effectiveness, 4 fractions (group II) proved to be significantly superior obtaining acomplete pain relief in 41 of 86 patients (47.7%). Because ofour restrictions to treated sites (excluding lesions of the ver-tebral column or weight-bearing bones) and field sizes thetreatment schedule was generally well tolerated without not-able adverse effects.
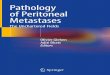
To investigate the possible role of the primary tumor and thelikelihood of pain relief a subgroup analysis was performedin group II (4 ´ 4 Gy) and demonstrated differences of treat-ment response in patients with breast cancer (n = 28) com-pared to patients with other primaries (n = 58). Pain relief atday 90 was 93% in breast cancer patients versus 73% in bonemetastases of other primaries (Table 3). In breast cancer pa-tients pain progression occurred in 23.3% of treated sites aftermedian 9 (1.5 to 27) months while in patients with other pri-maries it occured in 34.8% after median 3 (0.5 to 9) months(Figure 1). Overall survival in breast cancer patients was me-dian 14 (3.5 to 17) months and thereby significant longerwhen compared to median 5.5 (0.5 to 74) months in patientswith other primaries (Figure 2).
Discussion
In patients with bone metastases, palliative radiotherapy isa well established indication for treatment of pain [1, 13, 20,27]. When pain relief is the predominant aim of therapy the
Group I Group II p-value(1 ´ 4 Gy) (4 ´ 4 Gy)
Pain relief at day 7 after 48% 86.5% <0.0001radiotherapyPain control at day 90 55% 80% 0.006Median time to 2.0 (0.5–24) mo. 5.8 (0.5–74) mo. <0.0001progression (range)Median survival time 6.0 mo. 7.0 mo.
Table 2. Treatment results after 1 ´ 4 Gy and 4 ´ 4 Gy.
Tabelle 2. Behandlungsergebnisse nach 1 ´ 4 Gy und 4 ´ 4 Gy.
Breast cancer Other primaries p-value(n = 28) (n = 58)
Pain relief at day 7 after RT 96% 81% 0.032Pain control at day 90 93% 72% 0.022Observed pain progression 23.3% 34.8%Median time to progression (range) 9 (1.5–27) mo. 3 (0.5–9) mo. 0.021Median survival time (range) 14 (3.5–17) mo. 5.5 (0.5–74) mo. 0.012
Table 3. Treatment results after 4 ́ 4 Gydepending on primary tumor.
Tabelle 3. Behandlungsergebnisse nach4 ´ 4 Gy in Abhängigkeit vom Primär-tumor.
1.0
0.8
0.6
0.4
0.2
0.0
pain
con
trol
pro
babi
lity
0 20 40 60 80months
Figure 1. Local pain control probability after treatment with 4 ́ 4 Gydepending on primary tumor, calculated by Kaplan-Meier. Differ-ence between breast cancer patients (solid line) and other primaries(dotted line) was significant (Log-rank test, p = 0.021).
Abbildung 1. Wahrscheinlichkeit lokaler Schmerzkontrolle nach Be-strahlung mit 4 ́ 4 Gy in Abhängigkeit vom Primärtumor, berechnetnach Kaplan-Meier. Der gefundene Unterschied zwischen Brust-krebspatienten (durchgezogene Linie) und anderen Primärtumoren(gepunktete Linie) war signifikant (Log-Rank-Test, p = 0,021).
1.0
0.8
0.6
0.4
0.2
0.0
surv
ival
0 20 40 60 80months
Figure 2. Overall survival after treatment with 4 ´ 4 Gy dependingon primary tumor, calculated by Kaplan-Meier. Difference betweenbreast cancer patients (solid line) and other primaries (dotted line)was significant (Log-rank test, p = 0.0115).
Abbildung 2. Gesamtüberleben nach Bestrahlung mit 4 ´ 4 Gy inAbhängigkeit vom Primärtumor, berechnet nach Kaplan-Meier.Der gefundene Unterschied zwischen Brustkrebspatienten (durch-gezogene Linie) und anderen Primärtumoren (gepunktete Linie)war signifikant (Log-Rank-Test, p = 0,0115).
STO 663 Bremer UB-neu 25.08.1999 7:55 Uhr Seite 384

Bremer M, et al. Hypofractionated Radiotherapy in Painful Bone Metastases
Strahlenther Onkol 1999;175:382–6 (Nr. 8) 385
use of low-dose short-term radiotherapy may offer patientswith limited life expectancy effective palliation with a mini-mum disruption of their remaining life compared to protracted fractionated treatment. The convenience of ashorter overall treatment time may enhance patients acceptance of irradiation for another bone lesion and reduce probability of discontinuation of treatment due toprogression of disease.
In our study we did not include metastases of vertebral orweight-bearing bones due to the uncertainty of adequacy ofshort course radiotherapy to these sites, although spine le-sions made up a major part of irradiation in several othercomparable studies [10, 22, 24, 28]. We analyzed the re-sponse to radiotherapy by using a 4-point categorical scale.Response was defined as an improvement by at least 1point. Same or similar pain scales and response criteriawere used by several authors [6, 9, 10, 12, 16, 28] providingbetter comparability between our results and publisheddata.
Our study compared the 4 ´ 4 Gy schedule with the 1 ´ 4 Gyschedule and established that 4 ´ 4 Gy provides significantlyhigher response rates (86.5% vs 48%) confirming our prelim-inary results from a smaller series published previously [12].Other studies [9, 12, 22] also noticed lower response rates af-ter a single fraction treatment of 4 Gy (between 35% and48%), whereas response rates of 68% to 89% were reportedfor a total dose of 16 to 22.5 Gy given in 4 to 5 fractions [6, 12,16–18, 23, 28].
We found that long-term pain control (3 months after radio-therapy) was significantly superior for the 4 ´ 4 Gy schedule,as well. In literature only few authors report on pain controlwith a follow-up of at least 2 to 3 months [9, 10, 12, 16, 28]with pain control rates after 1 ´ 4 Gy between 55 and 68%and after 4 ´ 4 Gy between 76% and 88% being comparableto our results.
For patients treated with 4 ´ 4 Gy median duration of re-sponse was 5.8 months, median survival 7 months. Other au-thors using similar irradiation schedules report median dura-tion of response between 3 and 8 months and mediansurvival between 5.5 and 7 months [2, 6, 16, 17, 28].
According to our and published data radiotherapy with 1 ´ 4Gy seems to be inadequate to treat bone metastases relatedpain, whereas for higher single doses (e. g. 1 ́ 8 Gy) responserates as high as 69% and 74% and pain control rates between71% and 78% were described [9, 10, 16, 21]. The efficiency ofour 4 ´ 4 Gy schedule was comparable to more conventional-ly fractionated treatment regimens with published responserates varying between 66% and 86% and pain control rates
between 82% and 84% [2, 4, 17, 21, 24], but somewhat inferiorto the fractionated higher dose treatments of the RTOG 74-02 study as reported by Tong et al. [28]. In a recently pub-lished review [25] the improved pain relief of higher dosefractionated treatments as observed in the RTOG trial wasconsidered to be worth the additional efforts of the moreprotracted schedules.
In the group irradiated with 4 ´ 4 Gy we found that breastcancer patients showed significantly better response, dura-tion of pain control, and overall survival. Although the ma-jority of publications did not observe such a difference [3, 8,9, 14, 15, 19, 21, 27], recent studies support our findings [2, 6,10].
Due to the treatment sites in our study recalcification of ir-radiated bone was not a major goal and therefore notsystematically analyzed. Recalcification effects of radio-therapy depend on the characteristics of the bone metasta-ses (osteolytic, osteosclerotic, mixed type). In osteolyticmetastases a distinct increase of bone mineral density canbe found about 3 months after treatment as analyzed byquantitative CT-measurements [29]. Only few authors re-port on recalcification comparing a short course to a moreprotracted radiotherapy schedule observing equal results[17, 24].
In treatment of bone metastases the fractionation scheduleshould always be related to the patient’s prognosis and indi-vidual conditions including performance status [5, 7, 26]. Inour study patients were eligible to receive a short course ofpalliative radiation when multiple metastasis (bone or viscer-al) were present and the estimated life expectancy was 6months or less. The observed better survival of some sub-groups, e. g. breast cancer patients, demonstrates the need ofa more accurate definition of a group of patients with verylimited life expectancy, in whom hypofractionated radiother-apy appears to be appropriate.
In general patients with solitary metastasis, manifest or im-pending pathological fracture or metastases of weight-bear-ing bones with remineralization as a major aim of therapyshould be considered for irradiation with conventionallyfractionated higher dose treatments.
In summary, the present study showed a statistically signifi-cant advantage in pain relief after 4 ´ 4 Gy as compared to 1 ´ 4 Gy resulting in response rates comparable to those of more conventionally fractionated schedules. If single fraction schedules seem to be preferable for patients’ con-venience in specific situations doses higher than 4 Gy shouldbe applied to avoid major loss in palliative effect.
References1. Adamietz IA. Die Wahl der Behandlungsziele in der palliativen Radio-
therapie. Forum DKG 1997;12:400–4.2. Arcangeli G, Giovinazzo G, Saracino B, et al. Radiation therapy in the
management of symptomatic bone metastases: the effect of total dose andhistology on pain relief and response duration. Int J Radiat Oncol BiolPhys 1998;42:1119–26.
3. Bates T, Yarnold JR, Blitzer P, et al. Bone metastasis consensus state-ment. Int J Radiat Oncol Biol Phys 1992; 23:215–6.
4. Benson RC, Hasan SM, Jones AG, et al. External beam radiotherapy forpalliation of pain from metastatic carcinoma of the prostate. J Urol1982;127:69–71.
5. Eble MJ, Wannenmacher M. Lokale Strahlentherapie bei der Behand-lung von Skelettmetastasen. Orthopäde 1998;27:245–9.
6. Gaze MN, Kelly CG, Kerr GR, et al. Pain relief and quality of life follo-wing radiotherapy for bone metastases: a randomised trial of two fractio-nation schedules. Radiother Oncol 1997;45:109–16.
STO 663 Bremer UB-neu 25.08.1999 7:55 Uhr Seite 385

Strahlenther Onkol 1999;175:382–6 (Nr. 8)386
Bremer M, et al. Hypofractionated Radiotherapy in Painful Bone Metastases
7. Hess CF, Weiss E, Schmidberger H. Symptomorientierte Strahlenthera-pie. Onkologe 1996;2:540–7.
8. Hoskin PJ. Scientific and clinical aspects of radiotherapy in the relief ofbone pain. Cancer Surv 1988;7:69–86.
9. Hoskin PJ, Price P, Easton D, et al. A prospective randomised trial of 4Gy or 8 Gy single doses in the treatment of metastatic bone pain. Radio-ther Oncol 1992;23:74–8.
10. Jeremic B, Shibamoto Y, Acimovic L, et al. A randomized trial of threesingle-dose radiation therapy regimens in the treatment of metastatic bone pain. Int J Radiat Oncol Biol Phys 1998;42:161–7.
11. Karstens JH, Schnabel B, Ammon J. Management of metastatic bonepain: preliminary results with single fraction (4 Gy) radiotherapy. Onko-logie 1989;12:41–2.
12. Karstens JH, Blach M, Ammon J. Pain management policy: comparisonof two irradiation schedules in metastatic bone pain. Onkologie 1991;14:341–3.
13. Müller RP. Palliative Strahlentherapie. In: Pichlmaier H, Hrsg. PalliativeKrebstherapie, 1. Aufl. Berlin-Heidelberg-New York-London-Paris-Tokyo-Hong Kong-Barcelona: Springer, 1991:115–31.
14. Needham PR, Mithal NP, Hoskin PJ. Radiotherapy for bone pain. J RSoc Med 1994;87:503-5.
15. Nielsen OS, Munro AJ, Tannock IF. Review article: bone metastases: pa-thophysiology and management policy. J Clin Oncol 1991;9:509–24.
16. Nielsen OS, Bentzen SM, Sandberg E, et al. Randomized trial of singledose versus fractionated palliative radiotherapy of bone metastases. Radiother Oncol 1998;48:233–40.
17. Niewald M, Tkocz HJ, Abel U, et al. Rapid course radiation therapy vsmore standard treatment: a randomized trial for bone metastases. Int JRadiat Oncol Biol Phys 1996; 36:1085–9.
18. Okawa T, Kita M, Goto M, et al. Randomized prospective clinical studyof small, large, and twice-a-day fraction radiotherapy for painful bone me-tastases. Radiother Oncol 1988;13:99–104.
19. Poulsen HS, Nielsen OS, Klee M, et al. Palliative irradiation of bone me-tastases. Cancer Treat Rev 1989; 16:41–8.
20. Powers WE, Ratanatharathorn V. Palliation of bone metastases. In: PerezCA, Brady LW, eds. Principles and practice of radiation oncology, 3rdedn. Philadelphia: Lippincott-Raven, 1997:2199–217.
21. Price P, Hoskin PJ, Easton D, et al. Prospective randomized trial of singleand multifraction radiotherapy schedules in the treatment of painful bonymetastases. Radiother Oncol 1986;6:247–55.
22. Price P, Hoskin PJ, Easton D, et al. Low-dose single fraction radiotherapyin the treatment of metastatic bone pain: A pilot study. Radiother Oncol1988;12:297–300.
23. Quasim MM. Single dose palliative irradiation for bony metastases. Strah-lentherapie 1977;153:531–2.
24. Rasmusson B, Vejborg I, Jensen AB, et al. Irradiation of bone metastasesin breast cancer patients: a randomized study with 1 year follow-up. Radiother Oncol 1995;34:179–84.
25. Ratanatharathorn V, Powers WE, Moss WT, et al. Bone metastasis: Re-view and critical analysis of random allocation trials of local field treat-ment. Int J Radiat Oncol Biol Phys 1999;44:1–18.
26. Schnabel K (Koordinator), Adamietz A, Haase W, et al. Strahlentherapievon Knochenmetastasen. Metastatische Myelonkompression. Leitlinien inder Radioonkologie R 20, Deutsche Gesellschaft für Radioonkologie(DEGRO), Deutsche Gesellschaft für Medizinische Physik (DGMP), Ar-beitsgemeinschaft Radiologische Onkologie (ARO) in der DeutschenKrebsgesellschaft (DKG), Berufsverband Deutscher Strahlentherapeuten(BVDSt.) 1998:1–8.
27. Schüle-Hein K. Palliative Strahlentherapie. In: Aulbert E, Zech D, Hrsg.Lehrbuch der Palliativmedizin, 1. Aufl. Stuttgart-New York: Schattauer,1997:260–78.
28. Tong D, Gillick L, Hendrickson FR. The palliation of symptomatic osseous metastases. Final results of the study by the Radiation TherapyOncology Group. Cancer 1982;50:893–8.
29. Wachenfeld I, Sanner C, Böttcher HD, et al. Remineralisation von Wir-belkörpermetastasen des Mammakarzinoms nach Radiotherapie. Strah-lenther Onkol 1996;172:332–41.
Address for Correspondence: Dr. Michael Bremer, Abteilung fürStrahlentherapie und spezielle Onkologie, Medizinische Hochschule,D-30625 Hannover,Fon (+49/511) 532-2575, Fax -3796e-mail: [email protected]
STO 663 Bremer UB-neu 25.08.1999 7:55 Uhr Seite 386