Embed Size (px)
Citation preview

Effectiveness of Hypnosis for Post-operative Pain Management of Minimally Invasive Thorascopic Approach to Repair Pectus Excavatum: Retrospective Analysis
Renee C.B. Manworren, PhD, APRN, BC, PCNS-BC 123, Eric Girard, MD12,Ana Maria Verissimo, MD12, Sandra Riccardino, RN1, Kimberly A. Ruscher, MD12, Richard Weiss, MD12, Donald Hight, MD 12
1 Connecticut Children’s Medical Center, Hartford, CT 2 Department of Pediatrics, University of Connecticut School of Medicine, Farmington, CT 3 University of Connecticut School of Nursing, Storrs, CT
Background Pectus excavatum is the most common congenital deformity of the anterior chest wall, occurring in approximately 0.1% of live births.6 Regardless of the surgical approach, correction has been correlated with positive quality of life outcomes and improvement of body image 8, 9, 11 The minimally invasive thorascopic repair (Nuss procedure) results in a smaller scar, but significant pain from the substernal correction. Studies comparing approaches to managing the post-operative pain of this procedure have included systemic opioids by patient-controlled analgesia (PCA), nonsteroidal anti-inflammatory drugs (NSAIDs), and regional analgesia. 1-3, 7, 13An integrative medicine approach to post-surgical pain management may be more effective than traditional analgesics alone. Integrative medicine is defined as a “relationship based care that combines conventional medicine and complementary therapies for which there is some high quality scientific evidence of safety and effectiveness to promote health for the whole person in context of his or her family and community.”(www.nccam.nih.gov). One integrative medicine technique is hypnosis.
A few small studies report the efficacy of hypnosis in the management of children’s post-operative pain after a variety of surgeries 4, 5, 10, 12 One study suggests preoperative hypnosis was associated with a shorter hospital stay after Nuss procedure.12 However, patients in this study who received pre-surgical hypnosis training received PCA supplemented with intravenous (IV) and oral opioids, whereas patients in the non-hypnosis group received regional analgesia supplemented with IV and oral opioids.
At Connecticut Children’s Medical Center, Nuss procedure post-operative pain management plan is standardized to include epidural analgesia with local anesthetic alone, IV PCA opioids, IV NSAIDs and eventual transition to oral opioids and NSAIDs. Patients are invited to learn self-hypnosis prior to Nuss procedure .
Conclusions
Methods DESIGN: Retrospective chart review of all patients 10 to 21 years of age who received Nuss procedure at Connecticut Children’s Medical Center in 2011.
Hypnosis training was provided by a single integrative medicine physician. Patients received IV hydromorphone, morphine, or fentanyl by PCA. Adjustments were made to analgesic orders to facilitate pain relief in all patients. There was variability in whether patients received scheduled or PRN IV NSAIDS. Some patients also received muscle relaxants.
SAMPLE: Children with the cognitive ability to report pain using a 0 to 10 numeric pain rating scale (NRS) and were treated with our standard post-operative pain management regimen.
Results
Results
References
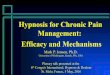
• Patients who received pre-surgical hypnosis training used less milligrams of morphine equivalents/hour over the course of the first 4 days after Nuss procedure. • While there was a difference in the groups mean pain intensity scores over the course of the first 5 days after surgery, there was no difference over the course of the first 4 days after surgery and there was no difference in maximum pain scores for each group over the course of 4 or 5 days after surgery.
The results of this study suggest that hypnosis provides an effective opioid-sparing adjunctive therapy for the management of moderate to severe pediatric post-operative pain after Nuss procedure. More research is needed to determine the effectiveness of hypnosis for symptom management after painful pediatric surgical procedures.
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
0 12 24 36 48 60 72 84 96 108
Mea
n M
axim
um P
ain
Inte
nsity
Sco
res
Time (12 Hour Intervals)
Non-Hypnosis Hypnosis
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
0 12 24 36 48 60 72 84 96 108 120
Pain
Inte
nsity
Sco
res
Time (12 Hour Intervals)
Non-Hypnosis Hypnosis
In 2011, 8 of 22 patients who underwent Nuss procedure received pre-operative self-hypnosis training. The sample was predominantly male and Caucasian. There was no difference in age, weight, sex, race/ethnicity, Haller’s index, surgeon, number of rods or footplates inserted, chest tube insertion, or prevalence of complications between the two groups.
Patients who received self-hypnosis training had statistically significantly improved pain control.
The difference in maximum pain intensity scores between the two groups over the course of the first four days of their hospital stays was not statistically significant (Z= -0.140, p= 0.889) (Figure 1) However, patients who had received pre-surgical self-hypnosis training reported statistically significantly lower mean pain intensity over the first five days of their hospital stay (Z=-2.04, p=0.041) but not for their first four days (Z=-1.612, p= .107) (Figure 2.)
1. Butkovi, D., Kralik, S., Matolic, M., Kralik, M., Toljan, S., & Radesic, L. (2007). Postoperative analgesia with intravenous fentanyl PCA vs epidural block after thoracoscopic pectus excavatum repair in children. British Journal of Anaesthesia 98 (5): 677-681. 2. Cucchiaro, G., Adzick, SN, Rose, JB, Maxwell, L, Watch, M. (2006). A comparison of epidural bupivicaine-fentanyl and bupivicaine-clonidine in children undergoing the Nuss procedure. Anesthesia & Analgesia 103: 322-7. 3. Densmore, JC., Peterson, D. B., Stahovic, L.L, Czarnecki, ML., Hainsworth, KR., Davies, HW., Cassidy, LD, Weisman, SJ, & Oldham, KT. (2010). Initial surgical and pain management outcomes after Nuss procedure. Journal of Pediatric Surgery 45: 1767-1771. 4. Huth MM, Broome, ME, & Good, M. (2004). Imagery reduces children’s post operative pain. Pain. 110:439-448. 5. Huth MM, Daraiseh NM, Henson MA, & McLeod SM. (2009). Evaluation of Magic Island: Relaxation of Kids © compact disc. Pediatric Nursing, 35 (5): 290-5. 6. Kelly, Jr. RE, Lawson ML, Paida CN, & Hruben, RH. (2005). Pectus excavatum in a 112 year autopsy series: anatomic findings and the effect on survival. Journal of Pediatric Surgery 40: 1275-8. 7. Kelly, RE, Shamberger, RC., Mellins, RB., Mitchell, KK., Lawson, ML, Oldham, K., Azizkhan, RG, Hebra, AV, Nuss, D., Goretsky, MJ, Sharp, RJ, Holcomb, GW, Shim, WKT, Megison, SM, Moss, RL, Fecteau AH, Columbani, PM, Bagley, TC, & Moskowitz, AB. (2007). Prospective multicenter study of surgical correction of pectus excavatum: design, perioperative complications, pain and baseline pulmonary function facilitated by internet-based data collection. Journal of the American College of Surgeons 205: 2, 205-216. 8. Kelly, RE, Shamberger, RC., Mitchell, KK., Mellins, RB., Lawson, ML, Oldham, K., Azizkhan, RG, Hebra, AV, Nuss, D., Goretsky, MJ, Sharp, RJ, Holcomb, GW, Shim, WKT, Megison, SM, Moss, RL, Fecteau AH, Columbani, PM, Bagley, TC, Quinn, A. & Moskowitz, AB. (2008). Surgical repair of pectus excavatum markedly improves body image and perceived ability for physical activity: multicenter study. Pediatrics 122: 6, 1218-1222. 9. Krasopoulos, G, Dusmet, M, Lada, G, & Goldstraw, P. (2006). Nuss procedure improves the quality of life in young male adults with pectus excavatum deformity. European Journal of Cardiothoracic Surgery 29: 1-5. 10. Lambert, SA. (1996). The effects of hypnosis/guided imagery on the postoperative course of children. Journal of Developmental and Behavioral Pediatrics, 17 (5), 307-310. 11. Lawson ML Cash TF, Akers R, Vasser, E, Burke, B, Tabangin, M, Welch, C, Droitoru, DP, Goretsky, MJ, Nuss, D, & Kelly RE. A pilot study of the impact of surgical repair on disease-specific quality of life among patients with pectus excavatum. Journal of Pediatric Surgery 38: 916-18. 12. Lobe, TE. (2006). Perioperative hypnosis reduces hospitalization in patients undergoing the Nuss procedures for pectus excavatum. Journal of Laparoendoscopic and Advanced Surgical Techniques 16; 639-642. 13. St Peter, SD, Weesner, KA, Sharp, RJ, Sharp, SW, Ostlie, DJ, & Holcomb, GW. (2008). Is epidural anesthesia truly the best pain management strategy after minimally invasive pectus excavatum repair? Journal of Pediatric Surgery 43: 79-82.
Figure 2: Mean Pain Intensity Scores in Non-hypnosis vs. Hypnosis Patients
Figure 1: Mean Maximum Pain Intensity Scores in Non-hypnosis vs. Hypnosis Patients
Figure 3: Morphine Equivalents (with and without ketorolac) in Non-hypnosis vs. Hypnosis Patients
Patients’ opioid use by PCA was converted to milligrams (mg) of morphine equivalents per hour. A factor of 6.7 was used to convert mg of hydromorphone administered per hour to morphine equivalents (1.5mg IV hydromorphone equianalgesic to 10 mg IV morphine). Patients who had received pre-surgical self-hypnosis training used statistically significantly less mg per hour of morphine equivalents (Z=-2.521, p=.012) (Figure 3). We noted variability in the dose and frequency of post-operative parenteral ketorolac administration and wanted to determine if the analgesia provided by ketorolac altered the magnitude or significance of the opioid-sparing effect of self-hypnosis training. Using the equianalgesic dose conversion of 30 mg ketorolac to 12 mg morphine, a similar statistically significant difference between the two groups (Z=-2.521, p=.012) was found (Figure 3).
The aim of this retrospective study was to analyze our initial experience of using hypnosis as a patient chosen adjunct for pain management after Nuss procedure. Post-operative pain management outcomes were compared between adolescents who did and did not receive hypnosis training before undergoing the procedure. Primary outcomes : pain control as measured by • self-reported pain scores (0-10 NRS) • IV opioid use
Secondary outcomes: • length of stay • opioid-related side effects: nausea, vomiting, constipation, pruritis, sedation, need for supplemental oxygen, respiratory distress, urinary retention, and mental status changes/hallucinations.
Study Aim
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
0 12 24 36 48 60 72 84 96 108
Aver
age
Mor
phin
e E
quiv
alen
ts (m
g/hr
)
Time(12 Hour Intervals)
Non-Hypnosis Morphine Equivalents/hr (with ketorolac) Hypnosis Morphine Equivalents/hr (with ketorolac) Non-Hypnosis Morphine Equivalents/hr (without ketorolac) Hypnosis Morphine Equivalents/hr (without ketorolac)