Embed Size (px)
Citation preview

Feature Article_829 1..11
Effectiveness of adherence therapy in patientswith early psychosis: A mirror image study
Ellie Brown,1,2 Richard Gray,1,2 Martin Jones2 and Simon Whitfield2
1School of Nursing Sciences, University of East Anglia, Norwich, and 2Surrey and Borders Partnership NationalHealth Service Foundation Trust, Leatherhead, UK
ABSTRACT: In patients with early psychosis, medication non-adherence is associated with morefrequent relapse. Observational studies have reported that up to 60% of patients fail to take medicationas prescribed. This study aimed to establish the effectiveness of adherence therapy (AT) training fortwo multidisciplinary early intervention in psychosis (EIIP) teams in preventing relapse in theirpatients. This intervention involved six 1-day team AT training sessions delivered monthly over a6-month period. Participants were patients with early psychosis who were on the caseload of the EIIPteams during the study period. A mirror-image design was used, comparing clinician ratings of relapsein the year preceding training (year 0) and the subsequent year (year 1). Results showed that in year0, the mean number of relapses was 0.96 (standard deviation (SD) = 1.10). During year 1, relapsesreduced significantly (P < 0.01) to 0.34 (SD = 0.64). No unexpected effects of training were reported.A thematic analysis of staff views of training, and service users’ views of their care received from EIIPteams, was also completed. Challenges in faithfully incorporating AT skills into practice were reported.In conclusion, AT training coincided with reductions in relapse rates in patients receiving servicesfrom an EIIP team, but no other changes in outcomes were detected.
KEY WORDS: adherence therapy, early intervention, psychosis, team training.
BACKGROUND
Early intervention seeks to minimize the time patientsspend experiencing psychosis through intensive supportand intervention, with the aim of improving long-termfunctional outcomes. There is evidence that these servicesreduce relapse and hospital re-admission rates comparedto usual community mental health care (Craig et al. 2004).Treatment with antipsychotic medication is an importantpart of this approach. Robinson et al. (1999), for example,reported that patients with a first episode of psychosisshowed greater symptomatic response to antipsychoticmedication compared with those with an established
illness. In addition, the dose of medication required toachieve this symptomatic response tends to be lower(Oosthuizen et al. 2004). Crossley et al. (2010) empha-sized the importance of a judicious use of medication inpatients with early psychosis to avoid side-effects thatmight colour their views about medication and psychiatrictreatment more generally.
Relapse in psychosis is defined as the re-emergenceor exacerbation of psychotic symptoms (Birchwood &Spencer 2001). The damaging effects of relapse are wellestablished; in the short term, often precipitating theneed for distressing emergency treatment, and in thelong-term, resulting in poorer functional outcomes(Birchwood et al. 2000; Dibben et al. 2009). It is generallyaccepted that adherence to medication is required toreduce the risk of relapse. Many researchers useadmission to hospital as a proxy measure of relapse(Gitlin et al. 2001). With the development of effectivecommunity-based services, such as early intervention inpsychosis (EIIP) teams and home treatment teams, the
Correspondence: Richard Gray, Faculty of Medicine and HealthSciences, University of East Anglia, NR4 7TJ, UK. Email:[email protected]
Ellie Brown, BSc.Richard Gray, RN, PhD.Martin Jones, RN, DProf.Simon Whitfield, BPharm.Accepted March 2012.
bs_bs_banner
International Journal of Mental Health Nursing (2012) ••, ••–•• doi: 10.1111/j.1447-0349.2012.00829.x
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

utility of this measure has decreased (Bebbington et al.2006).
Non-adherence is a major problem in patients takingantipsychotic medication. In younger people (those agedless than 35 years), the problem is even more profound(Awad et al. 1996); it is estimated that up to six in 10patients with early psychosis do not take medication asprescribed (Coldham et al. 2002). The reasons forpatients stopping their medication are complex, andinclude factors related to the illness, the treatment, theprescriber, and the patient, as well as the environmentand culture in which they live (WHO 2003). Mutsatsaet al. (2003) identified that negative medication attitudesand lack of insight were two major factors influencingadherence in patients with early psychosis.
Research focused on testing educational strategies hastended to show an increase in knowledge about illnessand medication, but not significantly improve adherence(Nosé et al. 2003). An approach that seeks to address thecomplex range of factors affecting compliance is adher-ence therapy (AT). AT is rooted in the observation thatpatients’ beliefs impact on medication compliance. Apatient-centred, manualized approach, AT is ideally deliv-ered as a course over a series of 6–8-weekly one-to-onesessions, each with a different focus. Examples of activi-ties carried out during AT sessions are:
1. Assessment: exploring patients’ beliefs about treat-ment, practical problems with medication andside-effects, medicine reconciliation (reviewing allmedication patients are taking, prescribed, orotherwise).
2. Structured medication problem-solving to addresspractical issues with medication (e.g. side-effects orremembering to take medication).
3. Using a medication timeline to help patients reviewpast experiences of illness and treatment.
4. Exploring patients’ ambivalence about taking medica-tion using a decisional matrix (the pros and cons oftaking/not taking medication).
5. Testing patients’ beliefs about medication (e.g. ‘I canstop medication once I start to feel well’, ‘takingmedication is unnatural’).
6. Helping patients to move forward in their lives, and toconsider ‘life goals’ and the role medication might playin achieving these.
There have been six randomized, controlled trials(RCT) of AT (nee compliance therapy) to date (Andersonet al. 2010; Gray et al. 2004; 2006; Kemp et al. 1998;Maneesakorn et al. 2007; O’Donnell et al. 2003). Findingshave been equivocal (3 successful, 3 failed). An important
critique of the AT approach is that clinicians (e.g. mentalhealth nurses, psychiatrists) do not generally providecourses of treatment as part of their routine work. Itwould be unusual, for example, for a nurse to a see apatient on their caseload for focused, weekly therapy ses-sions. More typically, new clinical skills will be incorpo-rated into regular meetings that might have multipleissues on the agenda. Gray et al. (2004), Harris et al.(2009) and Byrne and Deane (2011) have extended theAT research by testing the impact of training mentalhealth workers to integrate the approach as part of theirroutine clinical practice. The three published trainingtrials have all reported positive outcomes. To date, therehas not been a test of AT or training for patients with earlypsychosis.
Our study will test the hypothesis that for patients inreceipt of early psychosis services, whole team trainingwill reduce: (i) relapse rates; (ii) the number of psychiatricinpatient admissions; (iii) the length of time as an inpa-tient; (iv) referral to crisis (home treatment) teams; and(v) the length of time under the care of crisis teams.
METHOD
This mixed-method project was in two parts: the first, amirror image study. This design has a long track record ofbeing used in adherence research; for example, to evalu-ate the effectiveness of depot antipsychotics (e.g. Su et al.2009). In a mirror image, design rates of relapse in theyear before and the year after the initiation of an inter-vention are compared. This design confers a number ofadvantages over more classic methodologies, such as theRCT. Specifically, several recent adherence trials havebeen heavily criticized for recruiting a sample of largelyadherent patients; non-adherent patients presumablybeing less likely to consent to participate in research. As aconsequence, the risk of type II error is increased (Grayet al. 2006). In a mirror image study, routinely-collecteddata are used, and patient consent is not required; there-fore, a more representative sample can be accessed. Inthis study, we counted the number of relapses in the yearpreceding AT training (year 0) and in year subsequent totraining starting.
The second part was a thematic qualitative studyexploring patient and professional views of AT training.
Study participantsMental health workersThe study participants were all clinically-qualified and-unqualified members of two established EIIP teams,who were employed by the participating mental health
2 E. BROWN ET AL.
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

service provider on the 1 July 2009. The service in thesouth of England provides secondary mental health ser-vices to a population of 1.3 million, and has at any onetime, approximately 16 000 open cases (Mental HealthMinimum Data Set 2009). At the time of the study, theTrust had two EIIP services comprising 25 staff members:three psychiatrists, 12 mental health nurses, six alliedhealth professionals (e.g. occupational therapists, clinicalpsychologists), one social worker, and three unqualifiedstaff members. The unqualified staff who attended train-ing were a support time recovery (STR) worker and twostudent nurses on placement. Student attendance wasjustified on the grounds that they were considered part ofthe team when the training took place.
All team members were invited to attend an AT train-ing course delivered by an experienced trainer (RG) oversix full days, once a month. None explicitly refused toattend; five (20%) said they were unable to free up time;the majority (n = 20, 80%) committed to the programmeand indicated they wanted to attend as much as the pro-gramme as they could.
PatientsAll patients on the caseload of the participating EIIPteams during the study period (1 July 2008 to 30 June2010), who met the following criteria, were included inthe study: (i) aged 14–35 years; and (ii) within their firstyear of treatment from the EIIP team (i.e. were referredfor EIIP between 1 July 2008 and 30 June 2009). Patientswere excluded from both elements of the project if duringthe study period they were: (i) in prison; (ii) an inpatientfor more than 6 months; and (iii) had, for any reason,been out of contact with the service for more than6 months.
These exclusion criteria were applied to ensure thatpatients in the study would receive care from the EIIPteam during the study period. This would not be possibleif they were in prison or were inpatients when contactwith the team was minimal.
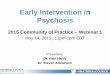
Data about patients in receipt of services from theEIIP team were extracted from the National HealthService (NHS) Trust patient administration system byEB, who was not blinded to whether patients were in thepretraining or training year. We identified 35 eligiblepatients to include in the study. Figure 1 shows thepatient flow though the study.
Qualitative interviewsMental health worker and patient interviews were carriedout between January and March 2011 by EB. Participantsfrom both groups were purposefully sampled and gave
written, informed consent to participate. All interviewswere digitally recorded and transcribed by one of thestudy researchers (EB).
Mental health workersMental health workers were invited to participate if theyhad attended at least 50% of the AT training (n = 10), andwere sampled to included a range of professional (e.g.psychiatry, nurses, occupational therapist) and non-professional (e.g. STR worker) backgrounds, and coveredboth teams.
PatientsPatients were contacted by staff members who hadattended AT training, and were sampled based on theirsex, age, and history of adherence/non-adherence. In thiselement of the study, we added an exclusion criterion anddid not invite patients to participate if they were acutelyunwell.
EthicsEthical approval was sought for the entire study, but wasonly required and approved for the qualitative element.The quantitative part of the project was considered aservice evaluation using routinely-collected data. Staffmembers and patients who were interviewed wererequired to give written, informed consent to participate.
Sample sizeFor AT training to be successful, we expected to observea minimum 50% reduction in relapse rates between years
FIG. 1: Patient flow diagram of patient progress through the phases ofthe study.
ADHERENCE THERAPY IN EARLY PSYCHOSIS 3
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

0 and 1; this would represent a medium effect size. Basedon previous studies, we estimated that, on average,patients with early psychosis experience a relapse approxi-mately once a year. Assuming a standard deviation (SD) of1, an alpha of 0.05, a two-tailed test of significance, and80% power, we required a sample of 32 patients in thestudy.
AT trainingThe clinical skill set of AT is built up in layers. Traineesneed to demonstrate competence in each layer beforemoving onto the next. The fundamental clinical skills ofAT (the first layer) include agenda setting, using thepatients own language, collaborative working, linking ses-sions together, and reflective listening. The four corner-stones of AT (the second layer) are keeping the patientengaged, minimizing resistance to change, providinginformation required by the patient about medication andside-effects, and using Socratic dialogue (asking instead oftelling) to generate discrepancies in patients’ beliefs abouttreatment. The third layer consists of the six AT exercisesdescribed above.
The AT training curriculum was structured aroundenabling trainees to acquire competence in each succes-sive layer. A Socratic teaching style was adopted as apowerful method of enabling trainees to engage andunderstand AT. This approach to teaching also affordsthe opportunity to model a way of communicating that iscore to the approach. Trainees also practiced these skillsin role play sessions, taking on the role of both patientand therapist to experience the intervention from bothperspectives. A supporting element of the curriculumwas training in psychopharmacology, which includedbrain structure and function, neurotransmission, mecha-nisms of action, and effects and side-effects of medicinesused to treat early psychosis (e.g. antipsychotics,antidepressants).
We checked the effectiveness of training using a pub-lished measure of knowledge acquisition about AT (theKnowledge about Medication Management Question-naire (KAMMQ; Jones et al. 2010), which was completedby trainees on the first and last days of training.
Outcome measuresPatientThe primary outcome for this study was the differencein relapse rates in year 0 compared to year 1. Our sec-ondary outcome measures were inpatient admission,referral to a crisis team, number of days as an inpatient,and/or under the care of the crisis team in year 0 com-pared to year 1.
Measure of relapseRelapse was determined using the established ‘zoning’system, routinely used in mental health services in the UK.Zoning was initially developed and described by Ryrieet al. (1997), and can be used as a measure of illnessseverity (Gamble 2006; Gamble et al. 2010). Patients arerated on a weekly basis using a traffic light system. Thecriteria for rating red are that the patient is verging on orexperiencing relapse, has stopped medication or has dis-engaged with the service, and has extensive unmet need.Amber criteria are that the patient has symptoms of mentalillness, but does not present with major risk factors.Patients who are stable and receiving maintenance care arerated green. Patients’ zone statuses were extracted directlyfrom the patients’ notes by EB. A relapse was defined as ashift from either green or amber to red. In this study, thezoning of patients was undertaken at weekly team meet-ings. This was routine practice for every patient on theteams’ caseload, and compliance was good. On average,fewer than four of 52 ratings missed a year.
Service use dataThe frequency and duration of inpatient hospital admis-sions and referrals to crisis teams were obtained (by EB)from the hospital patient administration system, and werecross-referenced with the patients’ notes.
Demographic and clinical informationAge, sex, ethnicity, diagnosis, and employment statuswere retrieved from patient electronic and paper records.Any discrepancies in records were checked with theappropriate team manager.
CliniciansKAMMQ A measure of clinicians’ knowledge of AT andpsychopharmacology, the KAMMQ has 28 multiplechoice questions, each with five possible responses.
Demographic and clinical information Demographicand clinical information included age, sex, ethnicity, pro-fession, level of education, years working in mentalhealth, percentage of training completed.
Data analysisData were analysed on an intention-to-treat basis. Themean number of relapses in years 0 and 1 were comparedusing a paired sample t-test. We also calculated the relativerisk (RR; and 95% confidence interval (CI)) of relapse.
Qualitative data analysisWorkers who completed at least 50% of the training wereapproached to be interviewed. Additional interviews were
4 E. BROWN ET AL.
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

conducted by EB with five patients who consented toparticipate and were under the care of the EIIP team.Both worker and patient interviews were audio-recorded,transcribed verbatim, and then coded using thematicanalysis (Braun & Clarke 2006).
Data were analysed using thematic analysis. This pre-dominantly ‘essentialist’ method reports experiences,meanings, and the reality described by participants, butalso allows the researchers to ‘unpick or unravel thesurface of “reality”’ (Braun & Clarke 2006, p. 81). Itentails an integrative, interpretative process between thedata and the researcher in order to ‘code’ the data. Thesecodes are then grouped into themes.
RESULTS
PatientsWe identified 35 patients who were in receipt of servicesfrom the EIIP team for the entire study period and met
our inclusion/exclusion criteria. Table 1 shows the demo-graphic and clinical characteristics of patients.
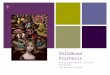
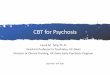
Table 2 shows the number of relapses, and Table 3shows the outcome measures for years 0 and 1. Data wereanalysed using SPSS for Windows, version 15.0 (SPSS,Chicago, IL, USA). Table 2 shows the distribution of thenumber of relapses experienced by patients before andafter training; the majority of patients experienced at leastone relapse in the year preceding training.
In year 0, there were 20 relapses that reduced to ninein year 1l a reduction that was statistically significant,equating to a medium effect size (0.33). The RR was 1.73(95% CI = 1.13–2.66), suggesting that the risk of relapsewas 73% higher in year 0. There was no significant changein any of the other outcome measures. None of thepatients in the study were on community treatmentorders. There were no serious untoward incidents overthe 2 years of the study.
Qualitative themesPatientsWe identified four themes: ‘working collaboratively’,‘indirect benefits’, ‘AT activities’, and ‘I’d rather not’.
Theme 1: Working collaborativelyMost patients interviewed talked about the value of beinginvited to be open with mental health workers about theirexperiences of taking psychiatric medication. This is con-sistent with the ethos of AT that emphasizes the impor-tance of collaborative working. It is noteworthy that twoof five participants said that if workers had adopted apaternalistic approach, they would have stopped takingtheir medication:
It would be a mutual decision, rather than saying ‘This iswhat is happening’. So it’s weighing up the benefits andcomparing how I would be with and without. (Patient 1,female, 22)
TABLE 1: Patient demographic characteristics (n = 35)
Characteristic n (%)
Age in years (mean, SD) 25 (5)Male 25 (71)White 25 (71)No. with psychosis 28 (80)Employed 9 (26)
SD, standard deviation.
TABLE 2: Frequency of relapse (red rating) in years 0 and 1 (n = 35)
No. relapses
Year 0 Year 1
n (%) n (%)
0 15 (43) 26 (74)1 11 (31) 6 (17)2 5 (14) 3 (9)3 3 (9) 0 (0)4 1 (3) 0 (0)
TABLE 3: Outcome measures
Measure n
Year 0 Year 1
P-value†Mean (SD) Mean (SD)
No. relapses 35 0.97 (1.10) 0.34 (0.64) <0.01Weeks relapsed 35 3.43 (6.07) 2.97 (8.18) nsReferrals to home treatment team 35 0.14 (0.43) 0.11 (0.40) nsDays under the care of crisis team 35 4.80 (20.26) 3.26 (12.72) nsNo. acute inpatient admissions 35 0.20 (0.40) 0.23 (0.56) nsNo. days as an inpatient 35 20.03 (52.47) 5.46 (14.12) nsNo. community treatment orders 35 0 0 ns
†Both t-test (parametric) and Mann–Whitney U-test (non-parametric) were performed and produced the same result. SD, standard deviation.
ADHERENCE THERAPY IN EARLY PSYCHOSIS 5
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

It’s quite important, because I wouldn’t like it if they didit without seeing if I was OK. (Patient 5, female, 27)
Theme 2: Indirect benefitsA number of patients talked about how medication hadstabilized their ‘mood’, and this had a positive impact onmany areas of their lives. There was a sense that thebenefits of medication were often indirect. In AT, consid-erable emphasis is placed on helping patient recognizethe personal benefit of medication, rather than tellingthem how treatment will improve their psychosis:
They help me in a lot of ways; they help me with initiativeand (to) become more active. (Patient 3, male, 24)
It stabilizes my irrational mood. . . . Feeling more confi-dent to do things on a daily basis. For me, that’s jobapplications and socializing with people. (Patient 2,female, 31)
Theme 3: AT activitiesReferences to specific AT activities (e.g. exploringambivalence) were made by a number of patients. This isparticularly pertinent to the aims of this study, whichintended to show that training leads to a direct change inclinical practice:
Weighing up the benefits and comparing how I would bewith and without (medication). (AT intervention: explor-ing ambivalence, Patient 1, female, 22)
Medication: it’s 60% with me I’m for, and 40% not. (ATintervention: exploring beliefs, Patient 2, female, 31)
Theme 4: I’d rather notA number of patients acknowledged that mental healthworkers had taken to discussing their treatment withthem, but still felt that the part medication plays in aidingrecovery is overplayed:
I think it is overplayed. There should be more talkingtherapies. I don’t like medication. . . . It’s got side-effects,and I don’t know what it’s doing to my body. (Patient 5,female, 27)
But I do wonder if there is an alternative I can take andalternative herbal medicine. . . . I’m not sure I agree withall the ingredients that go into medicines. (Patient 2,female, 31)
Mental health workersBetween July and December 2009, 20 mental healthworkers attended AT training. The vast majority wereprofessionally qualified. The AT course was 6 days long;on average, workers attended 4 days (SD = 1.35). Thir-
teen (65%) attended over 50% of the course, and can beconsidered to have completed training. During the studyperiod, three workers left the service (retirement, movingplacement, relocation to a different team), and eightjoined EIIP teams, but did not attend any training.Table 3 shows the demographic and clinical characteris-tics of the workers (Table 4).
Effect of training on knowledgeThe mean baseline score for the KAMMQ was 15.25(SD = 3.64). At follow up, this had improved significantly(mean = 20.80, SD = 3.85, P < 0.01), suggesting that theAT course had been effective at increasing trainees’knowledge.
Qualitative themesData were again analysed using thematic analysis. Datawere felt to be theoretically saturated (Glaser & Strauss1967; Guest et al. 2006) after eight interviews. Using theprinciples of thematic analysis, data were coded andgrouped into themes. The quality of interviews was good,with rich data being produced (Braun & Clarke 2006).
We identified five main themes: AT skills are used alot, team training is good for the service, AT has a positiveimpact on patients, staff skills have been enhanced, andthe training course needs to be developed further.
Theme 1: AT skills are used a lot in EIIP teamsWorkers talked positively about using AT in an EIIPservice; often describing how well the approach fits withtheir team ethos. This was an important subtheme of thefirst main theme.
Subtheme: AT matches EIIP team ethos
We put in a lot of time with our clients, and probably, weuse more than some of the other teams might do whohaven’t got the intensive input that we have with ourclients. (Worker 2, psychiatrist, female)
TABLE 4: Trainee demographics (n = 20)
Characteristic n (%)
Age (years) (mean, SD) 40 (11)No. females 17 (85)No. white 16 (80)No. nurses 6 (30)No. educated to at least degree level 14 (70)No. with professional registration 17 (85)Years working in mental health (mean, SD) 10 (7)
SD, standard deviation.
6 E. BROWN ET AL.
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

I think it’s largely become embedded in the ethos of theteam; it’s almost unthinkable that we would go back to theold, prescriptive: ‘this is what you’re having’ way ofworking. (Worker 7, psychiatrist, male)
Subtheme: AT is carried out informallyAlthough workers were positive about AT, they tended totalk about using elements of the approach in their day-to-day consultations with patients, rather than offering acourse of formal sessions. This, therefore, constituted afurther subtheme:
You can take the spirit of them (AT techniques) and usethat and then adapt it yourself. (Worker 1, communitypsychiatric nurse, female)
So not formally sitting and going: ‘We’ll do this tool andfocus on this’. Any time I’m discussing medication withpeople, I’m looking at what stops them, what their con-cerns are about stuff; so it does get brought up just aboutevery time that I see somebody. (Worker 2, psychiatrist,female)
Theme 2: Team training is good for the serviceTraining as a team was generally considered a positiveexperience, and was mentioned by a number of theworkers as a key benefit of the course. Therefore, oursecond main theme was the benefit of team training:
Sometimes, actually, the information that is crucial todetermining whether somebody continues on medicationmight not come in a medical review . . . so I think the mixof disciplines is actually crucial (for training). (Worker 4,team leader, female)
I really liked the idea that medication adherence waseveryone’s business in the team, not just the doctors’.(Worker 7, psychiatrist, male)
Theme 3: AT has a positive impact on patientsWorkers stated that AT has enabled patients to thinkdifferently about their illness and treatment; this repre-sents our third major theme:
I want to let him (patient) examine . . . the reasons why hetakes his medication; not just because his parents aremaking him take it or because we are saying he should.(Worker 1, community psychiatric nurse, female)
There’s a lot more discussions about medications, I think,and allowing them (patients) to have the choice . . . wehave to do everything we can so they’ve got all the infor-mation they need and they understand their illness.(Worker 2, psychiatrist, female)
Theme 4: AT has developed workers’ skillsThere was considerable evidence that training had a posi-tive impact on workers’ practice. Under this main theme,the following subthemes were identified: work is morecollaborative, improved confidence, changed clinicalpractice, and better knowledge of medication.
Subtheme: Work is more collaborativeCollaborative working is one of the cornerstones of AT;therefore, it was positive to see this emerge as a subthemein the analysis:
When I worked in an acute ward, it was always aboutadherence and compliance, and getting people to do whatyou wanted them to do. . . . This seemed a much better,more respectful, and more realistic kind of approach totake. (Worker 1, community psychiatric nurse, female)
It crystallized a lot of ideas that I had had around lettingpeople have a choice . . . but it put it in a framework,which made it much easier to use. (Worker 7, psychiatrist,male)
Subtheme: Improved confidenceWorkers reported that they were much more confidenttalking with their patients about medication; that it wasnot an issue that should be purely dealt with by the psy-chiatrist. Positively, this was discussed by workers across arange of disciplines:
I feel confident having that kind of conversation with ayoung person, and feel confident that what I am saying isright . . . I know that there is research done, and it isproved that adhering to your medication is a good idea.(Worker 5, STR worker, female)
I suppose that gave me a bit of confidence, a bit of direc-tion in how to work with people on those issues. (Worker1, community psychiatric nurse, female).
Subtheme: Changed clinical practiceMany of the workers talked about how the training hadhad a significant impact on their day-to-day clinical workwith patients, and as such, this represents a furthersubtheme:
It has changed my practice, which for someone who hasalready been a consultant for 8 years when it started, isquite something, because I don’t think many peoplechange. (W7, psychiatrist, male)
I think my approach has changed in a sense of I don’t justask them if they’ve taken their medication. I’ve changedmy approach to get different answers. (Worker 6, occu-pational therapist, female)
ADHERENCE THERAPY IN EARLY PSYCHOSIS 7
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

The structure of my sessions have changed, as well. I’vebeen more boundaried with times, agendas. (W3, OT,female).
Subtheme: Better knowledge about medicationsEnhancing workers’ knowledge about medication was animportant learning outcome from the AT course. This wasreferenced by several workers, who talked about develop-ing useful knowledge about medication that was retainedover time:
I really liked the stuff about medications and how they allwork and the different receptor sites and things, but do Iremember this? No. (W2, psychiatrist, female)
Because of the medication side of things, that’s not myforte; that was really quite useful finding out a bit moreabout that side of things. (W3, OT, female)
Theme 5: The training course needs to bedeveloped furtherWorkers who were interviewed contended a number ofrestrictions that prevented the successful implementationof the AT training. Time and resource constraints weremost commonly cited, and this was the main subtheme.Skills being forgotten and patients needing to be readywere the other two subthemes.
Subtheme: Time and resources limit the useof ATRepeatedly, a lack of time was identified as the mainreason why AT was not carried out more frequently:
I think those things should be routine (e.g. physical healthchecklists), but the resources here, we don’t have them todo that, it’s stretching, and unfortunately, other thingstake priority. (W4, team leader, female)
Often, you identify that it (AT) could be beneficial to dosome particular sessions, focused work on adherence, butthat can often get overruled by some kind of crisis orsomething, and it always feels like that is being put off andput off. (W6, OT, female)
Subtheme: Skills being forgottenAlthough infrequently mentioned, there was a sense fromworkers that unless skills were used regularly, they couldbe forgotten:
With certain people, there’s no problem with their medi-cation,; that’s probably true with most of them actually. . . but (using AT more) might be an issue that needs tobe thought about again. (W1, CPN, female)
I think there is a tendency for things to get forgottenif you don’t start using them fairly quickly. (W6, OT,female)
Subtheme: Patients need to be readyA theme emerged around some patients not being readyfor AT, because they were to acutely unwell or difficult toengage:
I suppose it really just depends on the patient’s mindsetabout their illness . . . I think it’s a like a lot of things withearly intervention; it’s about timing, really. (W8, OT,female)
I think that the people I would want to do that (adherenceassessment) with, I’d need to think about quite carefully,because there are some people I can just imagine theywouldn’t want to go there, really. (W1, CPN, female)
DISCUSSION
Poor treatment adherence is a major cause of relapse inpatients with early psychosis. In the present study, wetested the effect of team training in AT. Relapse, the mainoutcome of interest in this project, was determined usingthe NHS zoning system as a clinician rating of illnessseverity, assessed weekly by EIIP workers. Compared tothe year preceding training, relapse rates reduced signifi-cantly, providing tentative evidence that training mighthave been effective. This observation is consistent withthe three previous studies of AT (type) training that havebeen reported in the literature (Gray et al. 2004; Harriset al. 2009; Byrne & Deane 2011). The present study alsoadvances our understanding of how workers incorporateAT skills into their daily practice.
There have been six trials of AT delivered as an adjunc-tive ‘therapy’, typically delivered over a prescribed periodof time, that have been inconclusive in those authors’findings. One reason for this might be that providing atime-limited therapy is not an ideal way of working withpatients who require long-term adherence support.Simply put, patients might receive AT that clashes withthe usual care provided by their treating team. Forexample, within AT, great emphasis is placed on the useof Socratic dialogue to enable patients to think throughtheir decisions about taking or not taking medication.Within routine clinical practice, there might be a ten-dency towards a more paternalistic approach to instruct-ing patients to ‘take medication to treat their psychosis’.One of our thematic themes seems to emphasize thispoint; more collaborative working was valued as a positiveeffect of training, and was identified by both patients and
8 E. BROWN ET AL.
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

workers. We suggest that team training is effective, atleast in part, because it engenders a consistent shared wayof working between the patient and all workers involvedin their care.
Evidence of worker fidelity to the AT treatment modelwas lacking in our qualitative findings. Workers describedregularly using some aspects of the AT model, but in aninformal and unstructured way. Because patients are notgetting the whole treatment package, we would expectthis to dilute the effectiveness of the intervention, but thisdid not appear to be the case. Perhaps the more modestchanges in the way of working that we observed, deliveredover a sustained period of time, had a greater effect onrelapse than a high intensity (8 sessions) ‘blast’ of therapy.
Team training has been proposed to be a potentiallymore potent way of equipping staff with new competen-cies, because colleagues from different professional per-spectives work together to input into a shared way ofworking. This makes training particularly challenging toeffectively facilitate, because trainees come from radicallydifferent philosophical backgrounds (e.g. social work, psy-chology, medicine) and academic preparation (unquali-fied through to doctoral qualification). Participants in thestaff interviews acknowledged the challenges of providingtraining across disciplines, but generally seemed to appre-ciate the benefits of whole team training.
It was disheartening that all team members did notattend all training days. This might reflect a lack of com-mitment among team members or a lack of resourceswithin the service to ensure trainees were able to get totraining. Trainees’ failure to faithfully use all the AT skillsthey had been taught was also disappointing, if not sur-prising. Our observation suggests that consideration begiven to how fidelity to an AT model can be enhanced.One possible approach might be the provision of super-vision groups or the addition of top-up training.
Limitations of the studyAlthough relapse determined using the red, amber, green(RAG) system was the primary outcome and produced apositive finding, it was disappointing that other measureswere not significantly affected. This would have providedadditional evidence for the effectiveness of the interven-tion. The lack of effect might be explained by the rela-tively small sample size. However, the signal we detectedsuggested that further work evaluating AT in EIIP team isjustified.
The use of relapse as the primary end-point in thisstudy is justified, because it has meaning to patients, theircarers, workers, and service providers, and is relativelystraightforward to record. Alternative end-points include
treatment adherence or psychopathology. Direct mea-sures of adherence are notoriously unreliable, and there isno agreement about which represents the gold standard.Psychopathology, which has been used as an outcome inadherence research, is perhaps less clinically meaningful,and more challenging and expensive to assess.
Our use of the RAG zoning system as a clinician-determined measure of relapse is noteworthy. Thismethod of determining relapse might be criticizedbecause of a lack of established validity. However, moretraditional measures of determining relapse lack sensitiv-ity, effectively requiring a dramatic worsening of symp-toms to a point where hospitalization is required. SinceEIIP teams are well resourced to support people to stay athome (e.g. by visiting the patient daily), this measure has,to an extent, become somewhat redundant, even duringperiods of crisis. RAG zoning might also be prone to bias,because workers who are participants in the study arerating illness severity on a weekly basis, and in the experi-mental year of the study, might have been more likely tounderreport illness severity. This project was considered aservice evaluation; therefore, participants were conse-quently not informed what the primary end-point of thestudy was, effectively minimizing the potential for bias. Itis a further limitation of zoning that it was entirely pos-sible that some ‘red’ ratings were not true relapses (i.e.they were false positives). This limitation is, of course,true of other proxy measures of relapse.
It could be argued that the reduction in the number ofrelapses would have been observed, regardless of ourintervention, as the patients continued to receive carefrom the EIIP service. However, Addington et al.’s (2007)review of relapse rates in early psychosis showed a rangefrom 30% to 61% when patients are followed up over1–5 years. Their study measured the relapse numbers ofpatients in an ‘early psychosis programme’, and found that36% of their cohort experienced a relapse within the2-year timeframe.
We interviewed five patients for the qualitativeelement of the study. The recruitment of patients into thiscomponent of the study was challenging; 10 patientsdeclined to be interviewed, and many more were not feltto be ‘well enough’ to be interviewed by their care coor-dinators. Despite being interviewed by an experiencedqualitative researcher, participants gave minimalresponses to questions, resulting in fewer themes beinggenerated from this element of the project.
ImplicationsTo enable evidence -based interventions to be translatedinto routine practice, clinicians will need to acquire the
ADHERENCE THERAPY IN EARLY PSYCHOSIS 9
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

necessary competencies to do this work. Training isperhaps the only realistic way of achieving this. It is alarm-ing, given the amount of resources spent on trainingmental health workers, how little evidence there is thatcourses are effective at delivering a competent workforcethat improves patient outcomes. While we acknowledgethe methodological limitations of our study, we extend theargument that the evidence presented informs a view thatAT training for EIIP teams should be routinely available.
ACKNOWLEDGEMENTS
This project was supported by Culyer funds, awarded toSurrey and Borders NHS Foundation Trust in December2007.
REFERENCESAddington, D., Addington, M. & Pattern, S. (2007). Relapse
rates in an early psychosis treatment service. Acta Psychiat-rica Scandinavica, 115, 126–131.
Anderson, K., Ford, S., Robson, D., Cassis, J., Rodrigues, C. &Gray, R. (2010). An exploratory, randomized controlled trialof adherence therapy for people with schizophrenia. Inter-national Journal of Mental Health Nursing, 19 (5), 340–349.
Awad, A., Voruganti, L., Heslegrave, R. & Hogan, T. (1996).Assessment of the patient’s subjective experience in acuteneuroleptic treatment: Implications for compliance andoutcome. International Clinical Psychopharmacology, 11(2), 55–59.
Bebbington, P., Craig, T., Garety, P. et al. (2006). Remissionand relapse in psychosis: Operational definitions based oncase-note data. Psychological Medicine, 36, 1551–1562.
Birchwood, M. & Spencer, E. (2001). Early intervention inpsychotic relapse. Clinical Psychology Review, 21 (8), 1221–1226.
Birchwood, M., Spencer, E. & McGovern, D. (2000). Schizo-phrenia: Early warning signs. Advances in Psychiatric Treat-ment, 6, 93–101.
Braun, V. & Clarke, V. (2006). Using thematic analysis in psy-chology. Qualitative Research in Psychology, 3 (2), 1478–0895.
Byrne, M. & Deane, F. (2011). Enhancing patient adherence:Outcomes of medication alliance training on therapeutic alli-ance, insight, adherence, and psychopathology with mentalhealth patients. International Journal of Mental HealthNursing, 20, 284–295.
Coldham, E., Addlington, J. & Addlington, D. (2002). Medica-tion adherence of individuals with a first episode of psychosis.Acta Psychiatrica Scandinavica, 106 (4), 286–290.
Craig, T., Garety, P., Power, P., Rahaman, N., Colbert, S. &Fornells-Ambrojo, M. (2004). The Lambeth Early Onset
(LEO) Team: Randomised controlled trial of the effective-ness of specialised care for early psychosis. British MedicalJournal, 329, 1067–1069.
Crossley, N., McGuire, P. & Power, P. (2010). Efficacy of atypi-cal v. typical antipsychotics in the treatment of early psycho-sis: Meta-analysis. The British Journal of Psychiatry, 196,434–439.
Dibben, C., Rice, C., Laws, K. & McKenna, P. (2009). Is execu-tive impairment associated with schizophrenic syndromes? Ameta-analysis. Psychological Medicine, 39 (3), 381–392.
Gamble, C. (2006). The zoning revolution. Mental Health Prac-tice, 10 (4), 14–17.
Gamble, C., Grellier, J., O’Conner, C., Chipere, R. & Ness, M.(2010). Zoning: Focused support: A trust wide implementa-tion project. Journal of Psychiatric and Mental HealthNursing, 17, 79–86.
Gitlin, M., Nuechterlein, K., Subotnik, K. L. et al. (2001). Clini-cal outcome following neuroleptic discontinuation in patientswith remitted recent-onset schizophrenia. American Journalof Psychiatry, 158, 1835–1842.
Glaser, B. & Strauss, A. (1967). The Discovery of GroundedTheory: Strategies for Qualitative Research. New York:Aldine Publishing Company.
Gray, R., Wykes, T. & Gournay, K. (2003). The effect of medi-cation management training on community mental healthnurses’ clinical skills. International Journal of NursingStudies, 40, 163–169.
Gray, R., Wykes, T., Edmonds, M., Leese, M. & Gournay, K.(2004). Effect of a medication management training packagefor nurses on clinical outcomes for patients with schizophre-nia: Cluster randomised controlled trial. British Journal ofPsychiatry, 185, 157–162.
Gray, R., Leese, M., Bindman, J. et al. (2006). Adherencetherapy for people with schizophrenia. European multicen-tre randomised controlled trial. British Journal of Psychiatry,189, 508–514.
Guest, G., Bunce, A. & Johnson, L. (2006). How many inter-views are enough? An experiment with data saturation andvariability. Field Methods, 18 (1), 59–82.
Harris, N., Lovell, K., Day, J. & Roberts, C. (2009). An evalua-tion of a medication management training programme forcommunity mental health professionals; service user leveloutcomes. A cluster randomised controlled trial. Interna-tional Journal of Nursing Studies, 46, 645–652.
Jones, M., Robson, D., Whitfield, S. & Gray, R. (2010). Doespsychopharmacology training enhance the knowledge ofmental health nurses who prescribe? Journal of Psychiatricand Mental Health Nursing, 17 (9), 804–812.
Kemp, R., Kirov, G., Everitt, B. et al. (1998). Randomised con-trolled trial of compliance therapy. 18-month follow-up. TheBritish Journal Of Psychiatry, 172, 413–419.
Maneesakorn, S., Robson, D., Gournay, K. & Gray, R. (2007).An RCT of adherence therapy for people with schizophreniain Chiang Mai, Thailand. Journal of Clinical Nursing, 16,1302–1312.
10 E. BROWN ET AL.
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

McCrone, P., Craig, T. & Power, P. (2010). Cost-effectivenessof an early intervention service for people with psychosis.The British Journal of Psychiatry, 196, 377–382.
Mental Health Minimum Data Set (2009). [Cited 6 Jul 2011].Available from: URL: [http://www.mhmdsonline.ic.nhs.uk/]
Mutsatsa, S., Joyce, E. M., Hutton, S. et al. (2003). Clinicalcorrelates of early medication adherence: West London firstepisode schizophrenia study. Acta Psychiatrica Scandinav-ica, 108, 439–446.
Nosé, M., Barbui, C., Gray, R. & Tansella, M. (2003). Clinicalinterventions for treatment non-adherence in psychosis:Meta-analysis. British Journal of Psychiatry, 183, 197–206.
O’Donnell, C., Donohoe, G., Sharkey, L. et al (2003). Compli-ance therapy: A randomised controlled trial in schizophrenia.British Medical Journal, 327, 834–837.
Oosthuizen, P., Emsley, R., Jadri, T. & Keyter, N. (2004). Arandomized, controlled comparison of the efficacy and toler-ability of low and high doses of haloperidol in the treatment
of first-episode psychosis. International Journal of Neurop-sychopharmacology, 7, 125–131.
Robinson, D., Woerner, M., Alvir, J. et al. (1999). Predictors oftreatment response from a first episode of schizophrenia orschizoaffective disorder. American Journal of Psychiatry,156, 544–549.
Ryrie, I., Hellard, L., Kearns, C. et al. (1997). Zoning: A systemfor managing case work and targeting resources in commu-nity mental health teams. Journal of Mental Health, 6, 515–523.
Su, K.-P., Chang, H.-C., Tsai, S.-J., Yen, F.-C. & Tang, C.-H.(2009). Relapse and long-acting injectable risperidone: A1-year mirror image study with a national claims database inTaiwan. Value in Health, 12, S118–S121.
World Health Organization (2003). Adherence to Long-TermTherapies: Evidence for Action World Health Organization.Geneva, CH: World Health Organization.
ADHERENCE THERAPY IN EARLY PSYCHOSIS 11
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.