Embed Size (px)
Citation preview

Effectiveness and safety of seasonal and pandemic influenza vaccines: European Perspectives
Angus Nicoll for the European Centre for Disease Prevention and Control
and the European Medicines Agency
1

Declaration of Interest StatementI have no relevant commercial interests www.europa.eu/transparency

The most entrenched conflict of interest in medicine is a
disinclination to reverse a previous opinion
John Yudkin , Bernd Richter & Edwin Gale Lancet 2011 doi:10.1016/S0140-
6736(10)61112-9

Acknowledgements European Medicines Agency
European Centre for Disease Prevention and Control
European Commission DG Health & Consumers Health Threats Unit and the Pharmaceutical Legislation Unit
Epiconcept and I-MOVE Collaboration
VAESCO & the Brighton Collaboration
National Collaborators and Regulatory Agencies
World Health Organization Europe and HQ
The VENICE-II Collaboration
Many many people in each of these 4

Background • Potentially a new seasonal influenza in Europe –
A(H1N1)2009 based
– ? Affecting younger people
– ? Clinical risk group more important
– ? Significant numbers of severe cases in healthy people
• Flu vaccine used to varying degrees routinely in Europe
• Political commitment – since 2009
5

0
10
20
30
40
50
60
70
80
90
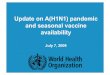
Data available in 2009. No data available from: Austria, Cyprus, Czech Republic, Greece, Latvia
Data from VENICE survey and other sources, version November 2010. Available from http://venice.cineca.org/Final_2009_Seasonal_Influenza_Vaccination_Survey_in_Europe_1.0.pdf and http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19700
Vaccination coverage for seasonal influenza vaccine in older
people (65 years & older) in EU and EEA countries
Latest seasonal data available in spring 2009 - For season 2007/8

Background • Potentially a new seasonal influenza in Europe –
A(H1N1)2009 based
– ? Affecting younger people
– ? Clinical risk group more important
– ? Significant numbers of severe cases in healthy people
• Flu vaccine used to varying degrees routinely in Europe
• Political commitment since 2009
• Mixed experience in Europe in the pandemic - but things that worked well outside the pandemic functioned in the pandemic - conversely …….
7

Pandemic Vaccination coverage in the population (n=21 countries)
Preliminary results http://ecdc.europa.eu/en/ESCAIDE/ESCAIDE%20Presentations%20lib
rary/ESCAIDE2010_Late_Breakers_Mereckiene.pdf

Vaccine Effectiveness
9

Efficacy and Effectiveness of Vaccines – both important
Efficacy • Seen in trials – but
usually optimal subjects
• Can study mild infection only
• Simple
• Through serology – a correlate of protection
• Key in Regulation and annual licensing
Effectiveness• Observed in the field
• Estimates subject to various biases
• Estimates less stable
• Complex - Varying methods
• Can study severe disease and death
• Closer to the individual experience
10

Monitoring influenza vaccine effectiveness in EU: why?
Not the most effective vaccine but recommended in all EU MS
Evaluate influenza vaccination programme
Maintain confidence in vaccination programmes
Influenza VE (IVE) varies from year to year
• clinical IVE cannot be predicted based on antigenic distance
• IVE can vary by age, subgroups and virus suptype
Detect variations in effectiveness due to
• changes in the target population
• changes in the epidemiology of disease
• poor virus-vaccine match
• special field conditions
11

Monitoring influenza vaccine effectiveness in EU: why?
Trigger other public health measures• use of antivirals
For new vaccines IVE could be incorporated as component of post-licensure surveillance
ILI /ARI incidence does not predictably decrease with increased vaccination coverage
• VE cannot be inferred from surveillance data
Trigger research on more effective vaccines
• mode of administration
• adjuvanted vs non-adjuvanted vaccines
• dosages
12

I-MOVE Collaboration (Influenza monitoring VE in Europe)
Objectives
To identify and pilot test methods to measure seasonal and pandemic IVE in EU and EEA
To develop a system to monitor on a routine and real-time basis IVE in EU and EEA– have early estimates during the influenza season
– have a system ready to assess and monitor IVE in a pandemic
13

ECDC
EISN
Health Protection Agency, UK
Health Protection Surveillance Centre, Dublin, Ireland
Instituto de Salud Carlos III, Madrid, Spain
Institut de Veille Sanitaire, Paris, France
National Center for Epidemiology, Budapest, Hungary
National Institute of Research –Development for Microbiological and Immunology, Bucharest, Romania
National Institute for Pubic Health and the Environment (RIVM), Bilthoven, The Nertherlands
Norvegian Institute of Public Health, Oslo, Norway
National Public Health Institute, Helsinki, Finland
National Institute of Public Health, Poland
Publich Health Institute Navarra, Spain
Robert Koch Institute, Berlin, Germany
Scientific Institute of Public Health, Brussels, Belgium
Smittskiddsinstitutet, Stockholm, Sweden
Statens Serum Institut, Copenhagen, Denmark
Scottish Centre for Infection and Environmental Health (CIEH)
Istituto Superiore Di Sanita, Rome, Italy
Greece, National Institute of Health
Royal College of General practitioners Brimingham Research Unit, UK
Instituto Nacional de Saude Dr. Ricardo Jorge, Lisboa, Portugal.
I-MOVE
ECDC
20 EU & EEA Member States
Coordination, EpiConcept
Collaboration with
Australia
Canada
USA
14

Three Methodolgies – all based on laboratory confirmed end-points
Case control
Cohort studies and nested case controls
Screening method
See Valenciano M, Kissling E, Ciancio BC, Moren A. Study designs for timely estimation of influenza vaccine effectiveness using European sentinel practitioner networks. Vaccine. 2010 Oct 8;28(46):7381-8. Epub 2010 Sep 17.
15

Published Results
2008/9 Pre pandemic elderly – seasonal vaccine
2009 Pandemic vaccines – predominately adjuvanted
2010-2011 Post pandemic seasonal vaccine
16

Seasonal vaccine effectiveness 2008-9pooled analysis pilot season (older people) – 5 sites
55.159.1
65.4 59,657.4 56.4
0
20
40
60
80
100
65 - 74 75+
Crude Full model Age Influenza A onlyInfluenza AH3
Vac
cin
e e
ffe
ctiv
en
ess
(%
)
Overall sample size N = 327 Kissling E, Valenciano M, Falcão JM, Larrauri A, Widgren K, Pitigoi D, Oroszi B, Nunes B, Savulescu C, Mazick A, LupulescuE, Ciancio B, Moren A. “I-MOVE” towards monitoring seasonal and pandemic influenza vaccine effectiveness: lessons learnt from a pilot multi-centric case-control study in Europe, 2008-9. Euro Surveill. 2009;14(44):pii=19388. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19388
17
* Study site in model as a fixed effect
‡ adjusted for sex, chronic diseases and related hospitalisations, smoking, previous seasonal influenza vaccination, functional status,

Pandemic vaccine effectiveness 2009-10, imputed dataset, pooled analysis – 7 study sites
83
72
87
78 8173
94
85 85
73
0
10
20
30
40
50
60
70
80
90
100
Crude* Adj ‡ Crude* Adj ‡ Crude* Adj ‡ Crude* Adj ‡ Crude* Adj ‡
All < 65 years 15-64 years < 15 years No chronic disease
PIV
E %
* Study site in model as a fixed effect
‡ adjusted for age-group, sex, month of onset, chronic diseases and related hospitalisations, smoking, seasonal influenza vaccinations and number of practitioner visits in the previous year
Overall sample size N = 2902 Valenciano M Kissling E, Cohen J-M, Oroszi B, Barret AS, Rizzo C et al Estimates of Pandemic Influenza Vaccine Effectiveness in
Europe, 2009–2010: Results of Influenza Monitoring Vaccine Effectiveness in Europe (I-MOVE) Multicentre Case-Control Study. Plos Medicine PLoS Med 8(1): e1000388.
doi:10.1371/ journal.pmed.1000388 http://www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.1000388
18

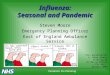
Seasonal vaccine 2010-11 effectivenessby influenza subtype, imputed dataset, pooled
analysis – 8 study sites
Overall sample size N = 4410 : Kissling E, Valenciano M, I-MOVE case–control studies team. Early estimates of seasonal influenza vaccine effectiveness in Europe, 2010/11: I-MOVE, a multicentre case–control study. Euro Surveill. 2011;16(11):pii=19818. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19818
19
64
52
68
56
66
50
0
20
40
60
80
100
Crude* Adjusted‡ Crude* Adjusted‡ Crude* Adjusted‡
All influenza (N=4410) H1N1 (N=3344) B (N=2944)
VE
%
* Study site included in the model as fixed effect‡ Model adjusted for 2009-10 seasonal and pandemic influenza vaccination, least one chronic disease, sex, at least one hospitalisation in previous 12 months, current smoker, age group practitioner visits in previous 12 months, week of symptom onset

Importance of Laboratory Confirmed End-points
20

Cohort study to evaluate the
IVE in preventing MA-ILI
Test negative case-control study
to evaluate the IVE in preventing
laboratory-confirmed influenza
IVE 2010-11 against MA-ILI and lab confirmed influenza in pop with chronic conditions, Navarra
* Euro Surveill 2011;16(7):pii=19799.
Courtesy Jesús Castilla
21

22
I-MOVE future
To monitor influenza VE against severe outcomes
Network of EU hospitals
– similar protocol pooling
– can be used for other diseases
ECDC EVER programme
– collect, analyse, communicate data and information on immunisation programmes in EU
– bring under same umbrella activities previously covered by different projects
– integrate the elements of vaccine preventable disease surveillance programme: disease surveillance, vaccine effectiveness, vaccination safety and vaccination coverage

Effectiveness Acknowledgements Sentinel networks
Partners conducting studies in 2010/11
– England and Wales, RCGP: Douglas Fleming, Haylay Durnall,
– France, OpenRome / GROG: Jean-Marie Cohen, Anne Mosnier, Isabelle Daviaud
– Hungary, NCE, : Beatrix Oroszi, Krisztina Horvath, Marta Melles, Agnes Csohan
– Ireland, HSE: Anne-Sophie Barret , Joan O'Donnell, Darina O’Flanagan, Aidan O´Hora,
– Italy, ISS: Caterina Rizzo, Paolo Dancona, Antonino Bella , Maria Cristina Rota
– Portugal, Inst Nac Saude Dr Ricardo Jorge: Baltazar Nunes, José Marinho Falcão, Raquel Guiomar
– Romania, Cantacuzino Institut: Viorel Alexandrescu, Daniela Pitigoiti, Emilia Lupulescu,
– Scotland, HPS: Jim McMenamin, Chris Robertson, Arlene Reynolds
– Spain, ISCIII: Amparo Larrauri, Silvia Jiménez, Salvador De Mateo
– Spain, Navarra Public Health Institute: Jesús Castilla , Iván Martínez
– Poland, National Institute of Public Health: Iwona Paradowska-Stankeiwicz, Malgosia Fluchowska, Pawel Stefanoff
– UK, HPA: Richard Pebody, Nick Andrews, Pia Hardelid
ECDC: Bruno Ciancio, Piotr Kramarz, Angus Nicoll
EpiConcept: A Moren, M Valenciano, E Kissling, C Savulescu, T Seyler, A Halm, V Nancey, N Colombo, G Jeannerod
Other Partner Institutes
– Belgium, IPH– Denmark, SSI– Finland, THL– France, InVS– France, Sentinelles– Italy, Campobasso, Catholic University– Greece, KEEPNO – Norway, FHI– Spain, Valencia CSISP– Sweden, SMI– The Netherlands, RIVM– The Netherlands, Erasmus University,
23

An agency of the European Union
Vaccine Safety Monitoring and investigating in Europe
24

Content
2525
• Methods of safety monitoring
• General Safety
• Investigating Adverse Events Following
Immunisations
• Guillain-Barré syndrome
• Narcolepsy

Methods of safety monitoring and
investigation Spontaneous Reporting by Clinicians and (increasingly) the public
National Systems
Feed into EMA System Eudravigilance
Special Systems and outputs in the Pandemic (EMA Pandemic
Pharmacovigilance Summaries http://www.ema.europa.eu/influenza/updates.html )
EU Vaccine Task Force
http://www.ema.europa.eu/docs/en_GB/document_library/Report/2011/04/WC500105820.pdf
Rapid Evaluation Group – (PREG) -
Review by Committee on Human Medical Products
Formal requests for special studies when signal appears 26

ADJUVANTED pandemic
influenza vaccines “
NON-ADJUVANTED
pandemic influenza vaccines
**
Number ADRs with
Autoimmune Disorders 126 12
Number ADRs total 49,236 4,048
% 0.26 0.30
CI 95 % [0.21 - 0.30] [0.13 - 0.46]
27
* Arepanrix™, Celtura™, Fluval P™, Focetria™, Pandemrix™, Humenza™
** Cantgrip™, Celvapan™, Panenza™
Preliminary analyses from EudraVigilance: reporting proportion of Autoimmune
disorders (MedDRA HLGT ‘Autoimmune disorders’) amongst all ADR reports, 1st
October 2009 to 31st December 2010
2. Analysis restricted to Autoimmune Disorders with causality related (certain,
probable, possible), time to onset 1→42 days for GBS and 1→30 days for
other reactions and BC 1-3 (GBS), 1-2 (ITP), 1-3 (ADEM)

Vaccine Safety Signal detection and assessment in Europe
Routine reporting of adverse events following immunization
Validation of safety concerns – case ascertainment
Causal association studies
Benefit/risk evaluations
Risk communication
28
Post-licensure monitoring for AEFIs shared responsibility between manufacturers, Public Health Institutes/ECDC and National Regulatory Agencies/EMA
However, should a signal arise sustainable European infrastructure only now being built

VAESCO ECDC since 2008 funds and collaborates closely with
a consortium of researchers in Denmark, Finland, France, Germany, Italy, Netherlands, Norway, Spain, Sweden, Switzerland, and UK:
Vaccine Adverse Event Surveillance & Communication
– Coordination of the VAESCO consortium – Brighton Collaboration
– Central data analyses by Erasmus University
Major component - data linkage of different health registries
Rationale: For rare events populations of one country is too small
Project was accelerated due to use of new pandemic vaccines – unprecedented effort - need for €€€infusion
29

EUROPEAN LEVELPooling of national/regional aggregated
data at Erasmus university medical center
Jerboa vaccine
module software
Database in
country 1
…
Jerboa vaccine
module software
Database in
country 2
Jerboa vaccine
module software
Database in
country..n
Country borders
The European Vaccine Safety Data linkage system
*this comes from the drug safety area where it is proven to work well and also in the US CDC Vaccine Safety Datalink system
*

On-going and completed studiesEstablishing Base-line for selected conditions – undergoing validation
Assessment of GBS and pandemic vaccines – € 1,1 million
TP and MMR – proof of
concept, Vaccine 2011
CCS – accepted BMJ
SCCS – in manuscript
Assessment of narcolepsy and pandemic vaccines – € 524,000
Case definition finalized together with European network of narcolepsy experts
Background incidence being developed
Case control study on-going31

Proof of concept – using data linkage in Denmark and England*
Results obtained from data linkage can be pooled from different countries using MMR vaccine and a
known adverse event trombocythopenic purpura
following MMR
Figure1: Timing of ITP around MMR
0
10
20
30
40
50
60
13 to 18 7 to 12 0 to 6 0 to 6 7 to 12 13 to 18 19 to 24 25 to 32 33 to 40
Interval from MMR (weeks)
Count of IT
P
Denmark
England
Post MMRPre MMR
Period after MMR (days)
Analysis 0-13 14-27 28-42 0-42
RI (95% CI) [n] RI (95% CI) [n] RI (95% CI) [n] RI (95% CI) [n]
Pooled data with
common age effect
1.38 (0.76-2.50) 3.09 (2.02-4.73) 1.97 (1.18-3.28) 2.13 (1.55-2.94)
Pooled data with country
specific age effects
1.30 (0.71-2.38) 2.87 (1.85-4.46) 1.81 (1.07-3.05) 1.98 (1.41-2.78)
Meta-analysis 1.30 (0.71-2.38) 2.84 (1.82-4.43) 1.83 (1.08-3.09) 1.98 (1.41-2.78)
Table 3: Relative incidence of ITP after MMR vaccination in children aged 12-23 months using
SCCS analysis of pooled data from Denmark and England and using meta-analysis of each countries individual SCCS RI estimates.
32Andrews N et al Vaccine 2011

Background incidence results pooledimportance of age and sex standardisation *
IR
*Unpublished – validation on-going

Results GBS case control study*
9.6
2.31.85
2.5
0.41
1.3
0.89
2.8
0.62
2.01
0.91
0.03125
0.0625
0.125
0.25
0.5
1
2
4
8
16
32
64
unadj. adj unadj adj unadj adj unadj adj unadj adj unadj adj
DK SW NL UK Pooled UK/NL Pooled UK/SW/NL
We can exclude a relative risk increase beyond 2.7 based on
the 95% confidence interval. Less than 3 attributable cases per
1,000,000 vaccinated persons
*Dieleman et al BMJ 2011 http://www.bmj.com/cgi/doi/10.1136/bmj.d3908

Conclusions
Field vaccine effectiveness system can be established - need infrastructure and some expert capacity
Don’t over-state effectiveness
Vaccine safety again need infrastructure
Simple signal reporting - need independent systems for rapid investigation – but its never fast
Linked data-bases and registries are a way to go
How to make the systems sustainable? 35

Acknowledgements European Medicines Agency
European Centre for Disease Prevention and Control
European Commission DG Health & Consumers Health Threats Unit and the Pharmaceutical Legislation Unit
Epiconcept and I-MOVE Collaboration
VAESCO & the Brighton Collaboration
National Collaborators and Regulatory Agencies
World Health Organization Europe and HQ
The VENICE-II Collaboration
Many many people in each of these 36

Thank you
37