Embed Size (px)
Citation preview

STUDY PROTOCOL Open Access
Effectiveness and cost effectiveness of guidedonline treatment for patients with majordepressive disorder on a waiting list forpsychotherapy: study protocol of a randomizedcontrolled trialRobin Maria Francisca Kenter1,2*, Annemieke van Straten1,2, Sabine Heleen Hobbel1,2, Filip Smit3,4,Judith Bosmans5,6, Aartjan Beekman6,7 and Pim Cuijpers1,2
Abstract
Background: Depressive disorders are highly prevalent and result in negative consequences for both patients andsociety. It is therefore important that these disorders are treated adequately. However, due to increased demand formental healthcare and subsequent increased costs, it would be desirable to reduce costs associated with majordepressive disorder while maintaining or improving the quality of care within the healthcare system. Introducingevidence-based online self-help interventions in mental healthcare might be the way to maintain clinical effectswhile minimizing costs by reducing the number of face-to-face sessions. This study aims to evaluate the clinical andeconomical effects of a guided online self-help intervention when offered to patients with major depressive disorderon a waiting list for psychotherapy in specialized mental health centers (MHCs).
Methods: Patients at mental health centers identified with a Diagnostic and Statistical Manual of Mental Disorders,fourth edition (DSM-IV) diagnosis of major depression who are awaiting face-to-face treatment are studied in arandomized controlled trial. During this waiting list period, patients are randomized and either (1) receive aninternet-based guided self-help treatment or (2) receive a self-help book. The 5-week internet-based guided self-helpintervention and the self-help booklet are based on problem solving treatment. After the intervention, patients areallowed to start regular face-to-face treatment at MHCs. Costs and effects are measured at baseline, after theintervention at 6 to 8 weeks, 6 months and 12 months. The primary outcome measure is symptoms of depression.Secondary outcome measures are diagnosis of depression, number of face-to-face sessions, absence of work andhealthcare uptake in general. Additional outcome measures are anxiety, insomnia, quality of life and mastery.
Discussion: This study evaluates the effectiveness and cost effectiveness of internet-based guided self-help in patientsat specialized mental health centers. The aim is to demonstrate whether the introduction of internet-based self-helpinterventions in regular mental healthcare for depressive disorders can maintain clinical effects and reduce costs.Strengths and limitations of this study are discussed.(Continued on next page)
* Correspondence: [email protected] of Psychology and Education, Department of Clinical Psychology, VUUniversity Amsterdam, Van der Boechorststraat 1, 1081 BT Amsterdam, TheNetherlands2EMGO Institute for Health Care and Research, VU University Medical Centre,Van der Boechorststraat 1, 1081 BT Amsterdam, The NetherlandsFull list of author information is available at the end of the article
TRIALS
© 2013 Kenter et al.; licensee BioMed Central Ltd. This is an open access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly cited.
Kenter et al. Trials 2013, 14:412http://www.trialsjournal.com/content/14/1/412

(Continued from previous page)
Trial registration: Netherlands Trial Register NTR2824
Keywords: Depressive disorders, Internet-based treatment, Online guided self-help, Cost effectiveness, Outpatients,Specialized mental healthcare
BackgroundDepressive disorders are highly prevalent [1-3], and are as-sociated with high costs in the professional, social, per-sonal and financial realms [1,3,4]. Those suffering fromdepression are more often absent from work, and havehigher levels of healthcare consumption compared tohealthy individuals [2]. It is desirable from a clinical pointof view to reduce the burden of depression, as it is from asocietal point of view to reduce the economic costs relatedto increased healthcare uptake, and reduced work prod-uctivity. In addition, given the increased demand for men-tal healthcare and limitation of recourses, it is importantfor mental health centers to optimize the efficient and ef-fective use of resources.
In The Netherlands, a person with symptoms of depres-sion who is seeking help is most likely to be seen first by ageneral practitioner (GP) [5], who acts as a gatekeeper forreferral to specialized mental health services. After regis-tration at a mental health service, patients usually have anassessment and are then assigned to a specific treatment.The time between registration and the first treatment ses-sion is normally at least 6 weeks. Long waiting lists causedby low workforce numbers are common. This time mightbe used to deploy internet-based self-help treatments[6,7], as previous studies have indicated that internet-based self-help therapies are clinically effective in diversepopulations [8-11]. Internet-based treatments require lesstherapist time in comparison with standard face to facetreatments and can therefore offer potential solutions asthey are immediately accessible, less costly and put lessstrain on therapeutic resources. They might serve firststep in a stepped delivery of care. This means that onlythose who do not respond adequately step up to a treat-ment of higher intensity, in this case the regular treatmentin mental health centers. This stepped-care approach issuggested in several guidelines such as the Australian andNational Institute for Health and Care Excellence (NICE)guidelines for depression, which recommend that patientsreceive the least burdensome treatment. Psychologicaltreatments such as computerized cognitive behavioraltherapy (cCBT) and individual guided self-help programsare recommended as low intensity treatments. After re-ceiving such treatments, patients possibly need fewer orno face-to-face sessions.
With the current cuts in healthcare budgets, it would bedesirable to reduce costs associated with major depressivedisorder while maintaining or improving the quality of
care. Introducing evidence-based internet-based self-help in-terventions in mental healthcare might be the way to speedup clinical recovery while minimizing costs by reducing thenumber of face-to-face sessions. However, internet-basedguided self-help interventions are currently not offered as afirst step to those waiting for specialized mental healthcare.In the current study, we offer an internet-based guided
self-help program to patients on a waitlist for psycho-logical treatment. The self-help program is based onproblem-solving therapy and uses self-examination ther-apy as a general framework [12]. This method has beenfound to be effective in several studies in the US [13],and for this study we used a guided self-help programthat has been examined in two earlier trials, and hasproved its effectiveness in reducing depressive symptomsin community samples [14,15].
Aims and hypothesesThis study aims to establish the effectiveness of aninternet-based guided self-help intervention for patientswith major depressive disorder before face-to-face treat-ment in specialized mental healthcare in comparison to acontrol group who are on a waitlist for face-to-face treat-ment. Furthermore, we expect that offering internet-basedtreatment as a first step of care reduces costs as we predictthe internet group to take up fewer regular treatmentsessions.
MethodsStudy designThe study is a randomized controlled trial with an eco-nomic evaluation. We are currently enrolling 248 pa-tients over 2 large mental health centers (MHCs) in 10different locations. We will recruit patients directly afterregistration for regular face-to-face mental health ser-vices who need to wait for at least 6 weeks before theirfirst treatment session. They will be randomized to ei-ther an internet-based guided self-help intervention orthe regular waitlist before the first treatment session.People on the waitlist will receive a self-help book with-out additional guidance in order to motivate them toparticipate in the randomize, controlled trial (RCT).Both groups are allowed to receive regular face-to-face(FTF) therapy at the MHCs after the waitlist period.Participants in both groups complete assessment at base-line, at intervention or waiting list (WL) completion(6 to 8 weeks), at a 6-month follow-up, and at 12 months.
Kenter et al. Trials 2013, 14:412 Page 2 of 10http://www.trialsjournal.com/content/14/1/412

The protocol of this study has been approved by theMedical Ethics Committee of the VU University MedicalCenter (registration number 2011/223).
Inclusion and exclusion criteriaEligible participants are adults, aged 18 or over, registeringfor regular treatment at one of the participating MHCswho meet the criteria for a Diagnostic and StatisticalManual of Mental Disorders, fourth edition (DSM-IV)diagnosis of major depression as measured with the Cli-nical International Diagnostic Interview (CIDI) by a trainedresearch assistant, have access to the internet, and adequateproficiency in Dutch. Exclusion criteria are starting orchanging type of dosage of antidepressant medication, thepresence of a bipolar or psychotic disorder, and an in-creased risk of suicide. Comorbid disorders other than bi-polar or psychotic disorders are allowed.
RecruitmentParticipants will be recruited while registering at theparticipating MHCs. In routine care patients are brieflyscanned by the MHCs (according to MHCs protocol toscreen out patients who are in crisis and need immediatetreatment), and for the purpose of this study, patientswith mood problems who are eligible for an intake as-sessment are asked by the MHC to share their contactdetails with the researchers. Those who are willing to doso, will then be called by a member of the research teamwho further explains the aim of this study and performsan additional check of the inclusion and exclusion cri-teria. If eligible, patients receive a study brochure and aninformed consent form. Patients will only be included inthe study if they meet all the criteria, and sign the in-formed consent form. In order to confirm the diagnosesMajor Depressive Disorder trained interviewers conducta clinical interview (CIDI).
Sample sizeThe trial is powered to detect an effect size of d ≥0.40[10,16] as statistically significant in a two-tailed test withα = 0.05 and power of (1 - β =) 0.80 with N = 99 per con-dition. To compensate for loss of follow-up of 20%, thetrial requires starting with 99/0.8 = 124 participants percondition at baseline. The dropout rate of 20% is con-servative, but from a power perspective a cautiousapproach. As this trial has two conditions, a total ofN = 248 will be necessary for the complete trial.
Mental health centers characteristicsTwo MHCs will be participating in this research. Theyeach offer services at a number of different locations. Inthis trial, a total of ten locations will participate. Thesecenters are chosen for pragmatic purposes, as they have ahigh number of patient enrolment, and have participated
in prior research of the VU University. In general, patientsare referred by their general practitioner to the mentalhealth centers where the patients is screened and placedon a waiting list. Within 6 weeks an initial meeting with atherapist takes place in which the patient’s needs and pref-erences regarding to treatment are determined. At theseparticipating MHCs it normally takes between 7 to 16weeks for patients to have a first treatment session, de-pending on therapist workload, treatment modality andother factors. Treatment in both centers can consist ofpsychological therapies such as CBT, sometimes in com-bination with medication. The researchers are not in-volved in the face-to-face treatment, and neither in thedecision-making process. However, prior to the start ofthis study all therapists at the participating MHCs will beinformed about the goals of this study and the internet-based intervention, they will attend a Q&A session withthe first author and receive the self-help book containingthe intervention. Prior to the start of a patients’ face-to-face treatment at the MHC the therapists will be informedby the aforementioned note in electronic patient recordand through email that their patients are participating inthis study. One of the objectives of the internet-basedintervention is that the subsequent face-to-face treatmentcan be adjusted to fewer sessions. The number and type oftherapeutic sessions patients will receive is based on theneeds of the patient, the judgment of the therapist, andprotocol available at the MHC. The type and number ofsessions will therefore vary per participant, and are outsidethe control of the researchers.
Internet interventionThe internet intervention that will be used is called ‘Tak-ing Control’ (original title: ‘Alles Onder Controle’). Thisintervention uses the self-examination treatment modeldeveloped by Bowman and colleagues [12,13], whichis based on problem-solving therapy and uses self-examination therapy (SET) as a general framework. Wetranslated it into Dutch, elaborated on it, and added infor-mation and exercises. We built a website for this interven-tion and developed a system for email support. Thisintervention has been described in more detail in severalother studies [12-14].In brief, this intervention is short, structured and man-
ualized. It consists of five weekly sessions. Each sessioncontains a structured homework assignment to be com-pleted by the participant. The first session requires par-ticipants to consider what is important in their lives.Next to this, participants will make a list of currentproblems and worries in their lives. This first sessionhelps participants to divide their problems into the fol-lowing three categories: not important (if the problem isnot related to the list of important things), importantand unsolvable (for example, permanent loss of health
Kenter et al. Trials 2013, 14:412 Page 3 of 10http://www.trialsjournal.com/content/14/1/412

or a loved one), or important and solvable. In the sec-ond, third and fourth session participants will be offeredvarious coping skills related to each of the categories ofproblems; the main focus is placed on adopting a struc-tured six-step approach when encountering important,solvable problems. This structured approach is dividedin the following steps: identifying the current problem;finding possible solutions; selecting one solution; createa plan to solve the problem with this solution; executethe plan and evaluate the plan. The last week of theintervention is reserved for both the reflection on long-term goals and the development of a structure to achievethese goals. Participants can only move on to the next ses-sion once the exercise in the current session has beensubmitted and when feedback on this session has beenreleased by the research team.The participants are supported by a coach, who gives
feedback to the homework assignments of the partici-pants in brief, weekly emails. The total amount of timespent on each patient is about 1.5 h (estimate based onour earlier trials). The writing of these emails takesabout 15 or 20 minutes per week, and will be per-formed by a coach. The coaches will be trained by thepsychologists who have developed the intervention andalso wrote the protocol for giving feedback to ensurethe consistency and integrity. An independent psych-ologist will verify whether the coaches have followedthe protocol sufficiently by reading a random selectionof the feedback emails.The feedback has two purposes. Firstly, coaches will
help participants to become familiar with the pre-sented techniques. The second purpose consists ofmotivating the participant to continue with the in-tervention. Feedback will be received by participantswithin 3 working days after a session has been com-pleted and submitted. When participants pose contentrelated questions to their coaches via the website,email or phone, their coaches will provide additionalguidance after receiving the question. After 5 weeks ofguidance, patients can continue to use the internet-based treatment but will not receive any feedback ontheir assignments.
Control conditionTo increase participation rates in the control group, thisgroup receives an unguided self-help book posted totheir home address. This control group will not receiveany feedback from coaches, nor will it have the opportunityto pose questions. Earlier research shows that self-helpwithout any form of guidance only results in a small effecton participants with increased levels of depressive symp-toms [16].Participants in both conditions will be referred for
regular FTF treatment after registration at the MHC.
FTF treatment might consist of additional waiting time;the duration of the waiting time is highly variable with aminimum of 7 weeks and a maximum of 16 weeks de-pending on the location of MHC. Variation fluctuatesboth between locations and over time within the centers,due to availability of therapists. In case the waiting timefor any MHC falls below 8 weeks, new participants fromthis MHC will be temporarily excluded from participat-ing in the research until the waiting time for new pa-tients at this MHC exceeds 8 weeks again. This has beendecided in order to not measure the effects of activetreatment by the MHCs at the first post-interventiontest at 8 weeks.The researchers of this study do not influence the
waiting time at the MHCs, nor will participation in thisstudy influence the waiting time for the participants.
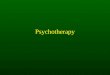
Randomization and blindingThe random allocation sequence will be generated by anindependent researcher in the program ‘Random Alloca-tion Software’ , stratified by location using blocks of six,eight and ten. After each inclusion another independentresearcher will allocate the patient to either the interven-tion or the control condition. Due to the nature of theintervention the treatment group allocation cannot beconcealed from the participants, nor from the researchteam and assessor of outcomes. Participants are assignedto one of two conditions within 2 working days fromtheir baseline assessment Figure 1.
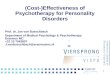
AssessmentsThis study will utilize both clinical and economical out-come measures (see Table 1). Assessments take place atbaseline (before randomization), follow-up assessmentsare at post-intervention (6 to 8 weeks), and at 6 and 12months after baseline.
Outcome measuresOur primary outcome will be symptoms of depression.Secondary outcomes are DSM-IV diagnosis of depres-sion, number of face-to-face sessions in MHC, costs (interms of all healthcare use and work absenteeism), anx-iety, mastery, insomnia, quality of life, and satisfaction.Plausible moderators measured in this study will be al-cohol use, personality, demographic factors and clientexpectations.Because the Composite International Diagnostic Inter-
view (CIDI) is part of the questionnaires at baseline andat post-intervention assessment (Table 1), the baselinequestionnaires and the 6 to 8 week assessment will beadministered by phone. Follow-up assessments at 6 and12 months will be administered online. All question-naires will be in Dutch.
Kenter et al. Trials 2013, 14:412 Page 4 of 10http://www.trialsjournal.com/content/14/1/412

Primary outcomeSymptoms of depressionSymptoms of depression will be registered by using theCenter for Epidemiological Studies Depression scale(CES-D) [17]. This scale consists of 20 items, the totalscore ranges between 0 and 60; higher scores indicatehigher levels of depression and a score of 16 and above in-dicates a clinical level of depression. This questionnairehas been tested in various populations and has been foundvalid and reliable [18]. A Dutch version of the CES-D hasbeen validated for internet administration [19].
Secondary outcomesDiagnosis of depressionThe CIDI will be used to assess whether the DSM-IVdiagnosis of depression has been met. The CIDI has been
developed by the World Health Organization to assessDSM-IV Axis-I diagnoses [20]. For the purposes of thisstudy, only section E will be administered, which allowsfor screening for depressive disorders. The CIDI will beconducted by phone by a trained interviewer.
Symptoms of anxietyThe subscale Anxiety of the Hospital Anxiety and De-pression Scale (HADS) will be used to measure symp-toms of anxiety. The depression scale will not beutilized in this research because depression will bemeasured by both CIDI and CES-D. The Anxiety sub-scale consists of 7 items, which scores range from 0 to21; higher scores indicate higher levels of anxiety [21].The HADS has shown to be reliable in Dutch popula-tions [21].
Referral to MHC by GP
Brief screening by MHC RT electronically receive details of potential participants from MHCs
Screening of potential participants by RT by checking for exclusion criteria
Exclusion Criteria:1. Not willing to sign IC2. Instable use of medication3. No current DSM IV disorder4. Suicidal ideation5. Bipolar or psychotic disorder
T0: Baseline measurements
Randomisation
Internet-based intervention Self-help book
Week 1-5: Online treatment with coach Waiting list
Week 8: T1 Assessment: Post-treatment
Start Psychological Treatment As Usual at MHCfor both groups
Week 26: T2 Assessment: Follow-up I
Week 52: T3 Assessment: Follow-up II
RT= Research TeamMHCs= Mental Health Centers
IC= Informed Consent
Figure 1 Study flow chart.
Kenter et al. Trials 2013, 14:412 Page 5 of 10http://www.trialsjournal.com/content/14/1/412

Symptoms of insomniaThe perceived level of insomnia will be measured bythe Insomnia Severity Index (ISI) [22]. This question-naire measures both the concerns associated with theperceived level of insomnia, as well as symptoms andconsequences of insomnia. Each item is rated on a 0 to4 scale; a higher score indicates more severe insomnia.ISI has been found to be internally consistent and reli-able [22].
Quality of lifeThe EuroQol 5-Dimensions questionnaire (EQ-5D),which consists of five items, will be used to measurequality of life. It registers the level of perceived prob-lems (no, some or extreme) in five domains (mobility,self-care, usual activities, pain/discomfort and anxiety/depression). A total of 486 distinct health states can bescored which are located between 0, which indicates
worst health possible, and 1, which indicates perfecthealth [23].
Resource useCosts related to the interventionCosts related to the intervention will be calculatedbased on the costs of running the intervention in bothconditions. To calculate costs related to the internetintervention, the costs of running the website plat-form and the costs of the hours of coaching investedin the intervention will be taken into account. Add-itional costs in the control group are the publishing ofthe self-help books.
Costs related to mental healthcareCosts related to mental healthcare will be measured asthe reported number and type of sessions by the MHC.This information is sent to the first author 12 months
Table 1 Outcome measures
Questionnaires Aim T0 Baseline(pre-test)
T1 Post-test(8 weeks)
T2 Follow-up I(6 months)
T3 Follow-up II(12 months)
Primary outcome
CES-D Symptoms of depression X X X X
Secondary outcomes
CIDI (Section E) Diagnosis of depression X X
HADS(Anxiety section)
Symptoms of anxiety X X
ISI Level of insomnia X X
EQ-5D Quality of life X X X X
Resource use
F2F Number of face-to-face appointmentsin MHC
X
TiC-P General health service uptake andproductivity losses
X X X X
Mediator
Mastery scale Mastery X X X X
Moderators
Demographic factors User characteristics X
NEO-FFI(sections N + C)
Neuroticism and conscientiousness traits X
CAGE Alcohol consumption X
CEQ Expectancy and treatment X
AOCEQ Expectations of the internet intervention X
CSQ-8 Client satisfaction with treatment X
AOCSQ Satisfaction with type of intervention X
AOCEQ ‘Alles Onder Controle’ Expectation Questionnaire, AOCSQ ‘Alles Onder Controle’ Satisfaction Questionnaire, CAGE ‘Cutting down, Annoyance by criticism, Guiltyfeeling, and Eye-openers’, CEQ Credibility/Expectancy Questionnaire, CES-D Center for Epidemiological Studies Depression scale, CIDI Composite International DiagnosticInterview, CSQ-8 Client Satisfactory Questionnaire-8, EQ-5D EuroQol 5-Dimensions, F2F face-to-face, ISI Insomnia Severity Index, HADS Hospital Anxiety Depression Scale,MHC mental health center, NEO-FFI NEO-Five Factor Inventory, TiC-P Trimbos and iMTA Questionnaire on Costs Associated with Psychiatric Illness.
Kenter et al. Trials 2013, 14:412 Page 6 of 10http://www.trialsjournal.com/content/14/1/412

after participants have registered at the MHCs. The dir-ect costs of the sessions will be calculated based on theDutch standard cost prices [24].
Costs from a societal perspectiveHealthcare costs in general as well as productivity lo-sses will be measured with the revised version of theTrimbos and iMTA Questionnaire on Costs Associatedwith Psychiatric Illness (TiC-P). Direct costs will bemeasured by investigating which contact with healthprofessionals has occurred and which type of medica-tion has been prescribed. Indirect costs will be mea-sured by work absenteeism and reduced productivity.The baseline TiC-P measures the care consumption 4weeks prior to the intervention. The follow-up assess-ments at 6 and 12 months use a 14 and 26 weeks recallperiod respectively. Previous research has shown thatup until half a year later, patients can reliably recalltheir consumption of health services [25]. The TiC-Phas been used previously in a population with depres-sive symptoms in The Netherlands [26].
MediatorMediatorThe amount of perceived control in a person’s life willbe measured by the Pearlin Mastery Scale [27]. Thescale consists of seven distinct items that are rated ona four-point scale. Higher scores indicate more per-ceived control; scores range from 7 to 35. The scalehas good reliability [27].
ModeratorsDemographicsDemographic variables such as age, gender, parental na-tionality, family composition, family income and educa-tional level will be screened for in a general questionnairethat measures user characteristics.
Alcohol useThe use of alcohol will be monitored using the four ques-tions that make up the acronym CAGE: ‘Cutting down,Annoyance by criticism, Guilty feeling, and Eye-openers’[28]. The CAGE is a widely used concise screening toolfor problematic alcohol consumption [29].
PersonalityIn order to measure the constructs neuroticism and con-scientiousness, the NEO-Five Factor Inventory (NEO-FFI)will be administered [30]. Previous research has indi-cated that neuroticism often coincides with depression(for example, [31]). Those scoring higher on conscien-tiousness are expected to adhere better to the homeworkexercises and consequently benefit more from internet-based therapies. Only these two domains will be tested
for to not exhaust participants more than necessary. Atotal of 12 questions on each of the domains will be an-swered on a 5-point Likert scale.
General expectancyThe Credibility/Expectancy Questionnaire of Devillyand Borkovec (CEQ) will be used to measure the ex-pected change and credibility of proposed treatment[32]. It consists of six questions; four questions meas-ure the ‘thinking’ aspects about the treatment, twoquestions measure the ‘feeling’ aspects of the questions.One question in both the ‘feeling’ and ‘thinking’ do-main is rated from 0% to 100%; the remaining fourquestions are rated on a Likert-type scale from 1 to 9.Both factors have been found to have a high internalconsistency and to have high test-retest reliability [32].
Expectancy with internet interventionThe ‘Alles Onder Controle’ Expectancy Questionnaire(AOCEQ) has been designed for this research to askwhat participants’ expectations are about the course. Anopen question investigates in which ways participantsexpect to gain benefits from this course. Three five-point Likert scale questions measure to which degreeparticipants appreciate starting with the intervention im-mediately, that personalized feedback will be given inthe internet group and to which degree they expect thecourse to help them feel less miserable.
General satisfaction with treatmentThe satisfaction with the internet intervention will bemeasured by the Client Satisfactory Questionnaire-8(CSQ-8), which consists of eight questions, each ques-tion is scored on a Likert-type scale from 1 to 4 [33].The questionnaire addresses several elements that con-tribute to overall service satisfaction and is reported in asingle dimension of overall satisfaction. A high internalconsistency has been reported [33].
Satisfaction with the internet interventionThe ‘Alles Onder Controle’ Satisfaction Questionnaire(AOCSQ) has been designed specifically to investigate towhat degree participants are satisfied with this internet-based intervention. It includes questions on the numberof sessions completed and, if applicable, the reasons fornot finishing the course. The questionnaire further re-searches satisfaction with the separate elements of theintervention, such as the quality of the feedback, theclarity of the website and the appropriateness of the ex-amples. Lastly, it explores whether participants were sat-isfied with the provided alternative to waiting, to whichdegree internet interventions are preferred over book in-terventions and to which degree feedback is preferredover non-feedback.
Kenter et al. Trials 2013, 14:412 Page 7 of 10http://www.trialsjournal.com/content/14/1/412

Statistical analysisThe analyses will be conducted in agreement with theintention to treat (ITT) principle, as per the CONSORTstatement [34]. Therefore missing endpoints will be im-puted using state of the art imputation methods, as a reli-able method for handling missing values [35]. Imputationallows for analyzing all participants in the condition towhich they have been randomized, which contributes toguarantee the integrity of the randomization and restoresloss of power due to dropout.To answer the research questions we will first look at
post-test differences between the two groups. We will useanalysis of variance (ANOVA), with the baseline valuesand waiting time as covariates. Subgroup analyses will beperformed for different characteristics. The differencein scores between the intervention group and the con-trol group will also be expressed in effect sizes. We useCohen’s d which is calculated by dividing the differencein mean scores of the two groups by their pooled stand-ard deviation (Xexp-Xctrl/SDpooled). Effect sizes under0.2 are considered to be small, those of 0.5 are moderateand effect sizes of 0.8 are considered to be large [36].Furthermore, we will compare the rate of DSM-IV diag-nosis of depression in both groups with logistic regres-sion analysis. The clinical effects will also be calculatedusing reliable change [37]. The long-term outcomes willbe analyzed with longitudinal analyses.
Economic outcomesThe economic evaluation will be conducted from a societalperspective, therefore it will include not only the interven-tion costs and costs stemming from healthcare uptake (dir-ect medical costs), but also the patients' out of pocket costs(direct non-medical costs) and costs stemming from prod-uctivity losses due to absenteeism and work cutback days(indirect non-medical costs). Costs will be based on theDutch standard cost prices [24] and productivity losses willbe valued using the friction costs method, as per the Dutchguideline for economic evaluation. Quality-adjusted lifeyears (QALYs) will be calculated on the basis of theEQ-5D. Having calculated the costs and QALYs allows fora cost-utility analysis, which can be used to compare thisintervention’s gains against those of other interventionsfor depressive disorders. A cost-effectiveness analysis canbe carried out by dividing the difference in costs by thedifference in effect, as is customary in the field of mentalhealth. Bootstrapping will be used to ascertain the amountof uncertainty surrounding the incremental cost effective-ness ratio (ICER) estimates and graphically depicted onthe ICER plane and in the acceptability curve.
DiscussionThis study will examine the effectiveness of offering aninternet-based guided self-help intervention to patients
before to start of face-to-face treatment in comparison withpatients who have to wait for face-to-face treatment. Wewill also compare the uptake of regular treatment in bothgroups. An economic evaluation will determine whether aguided internet intervention followed by face-to-face treat-ment is economically more sensible compared to waitingfor face-to-face treatment. A number of strengths and chal-lenges have been identified by the researchers in this study.
StrengthsExisting evidence shows that internet-based treatmentsare effective in treating depressive disorders in generalpopulations [9,38]. This trial however, will shed newlight on the question whether patients with major de-pressive disorder waiting for specialized care in MHCscan benefit from this type of internet-based guided self-help intervention. This population has, to the best ofour knowledge, not previously been studied in this man-ner, while the relevance of conducting a study on peoplewith major depressive disorder who receive an internet-based intervention as a first step of treatment is high fora number of reasons. As demonstrated previously, de-pression is a widely prevalent, invasive disorder, whichaffects the patients, their direct environments, and thesociety as a whole in multiple ways. Any measures whichcontribute to more people receiving better care for theirdepression in specialized mental healthcare against alower costs will be welcomed by all stakeholders. Steppedcare is suggested for treating depression in multiple guide-lines, for example the NICE guidelines in the UK (2009)Although there is some supporting evidence, there are fewRCTs to demonstrate the (cost) effectiveness of thisprogram in specialized mental healthcare. Furthermore,considering the increase of online interventions to thestandard treatment in more and more MHCs, this studywill contribute valuable information on the effects ofadding online treatment as a first step towards treatingmajor depressive disorder.An additional strength of this intervention is the on-
line delivery. The online intervention allows participantsnot only to access the intervention any convenient hour,with the rise of portable internet there are hardly anylimitations related to the location of a participant. Inaddition, offering guided online treatment during thetime otherwise lost to waiting may result in benefits forthe patient as well as for the MHCs in terms of patientsatisfaction and clinical effectiveness.A final strength of this study is the possibility of ap-
plicability. If the study indicates that it is economicallyand clinically beneficial to deliver internet interventionsto those with a major depressive disorder as part of theirtreatment, the intervention could easily be integrated asa standard component in the treatment of depression, asonly short training is necessary to become a successful
Kenter et al. Trials 2013, 14:412 Page 8 of 10http://www.trialsjournal.com/content/14/1/412

coach for this intervention. This intervention could beapplied widely in case the intervention is beneficial fortreating people with major depressive disorder.
LimitationsOne of the possible challenges of this study concerns thegeneral attrition from and non-adherence to internet in-terventions. Internet treatments require a degree of mo-tivation of the participant. This study includes depressedpatients who, by definition, have impaired motivationand lack of energy that may make it more difficult forpatients adhere to the intervention. To prevent dropoutsand maximize the uptake rates the participants will re-ceive emails and phone calls stating the importance ad-hering to the intervention.Another challenge for the trial could be the prevailing
attitude of psychologists at several MHCs who fear re-dundancy due to internet interventions. However, whenMHCs would start treating patients online as a first steptowards better health, more patients could be reached asonline treatment seems to be less time consuming forhealth professionals compared to face-to-face treatment.A further challenge is the extent the therapists take into
account that patients might already have acquired skillsand knowledge due to the internet intervention, so thatthere might be no need to start patients a fixed number offace-to-face sessions as prescribed by the standard treat-ment protocol. We aim that only those patients whorequire additional treatment due to a more complexpsychological problem will be seen face-to-face. There-fore, if internet interventions are proven to be moreclinically effective, it is feasible that psychologists atMHCs will be able to treat more patients in a bettermanner because of the implementation of internetinterventions.In summary, existing internet-based guided self-help
treatments focus mainly on depression in the generalpopulation. This trial, however, is to the best of ourknowledge the first effectiveness study of an internet-based guided self-help intervention for major depressivedisorder in specialized mental healthcare that also fo-cuses on reduction of face-to-face sessions and costs ingeneral. The findings of this study will contribute to thebody of knowledge on the additional value of internet-based treatments for depression. And if the low intensityinternet intervention shows to be (cost) effective, it mightserve as a first step towards the treatment of major de-pressive disorder.
Trial statusThe status of the trial is ongoing recruitment.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsPC, AvS and JB obtained funding for this study. PC, AvS, JB, and FScontributed to the design of the study. PC and AvS created the intervention.RK coordinates the recruitment of patients and data collection. AB, PC andAvS are responsible for the overall supervision. RK and SHH wrote themanuscript. All authors read, contributed towards and approved of the finalmanuscript.
AcknowledgementsThis study is funded by ZonMw (project number 80-82310-97-11047).
Author details1Faculty of Psychology and Education, Department of Clinical Psychology, VUUniversity Amsterdam, Van der Boechorststraat 1, 1081 BT Amsterdam, TheNetherlands. 2EMGO Institute for Health Care and Research, VU UniversityMedical Centre, Van der Boechorststraat 1, 1081 BT Amsterdam, TheNetherlands. 3Trimbos Institute, Postbus 725, 3500 AS Utrecht, TheNetherlands. 4Department of Epidemiology and Biostatistics, VU UniversityMedical Centre, Postbus 725, 3500 AS Utrecht, The Netherlands. 5Departmentof Health Sciences, VU University Amsterdam and EMGO institute for HealthCare, De Boelelaan 1085, 1081 HV Amsterdam, The Netherlands. 6Research,VU University Medical Centre, De Boelelaan 1085, 1081 HV Amsterdam, TheNetherlands. 7Department of Psychiatry, VU University Medical Centre, DeBoelelaan 1085, 1081 HV Amsterdam, The Netherlands.
Received: 11 July 2013 Accepted: 18 November 2013Published: 1 December 2013
References1. Mathers CD, Loncar D: Projections of global mortality and burden of
disease from 2002 to 2030. PLoS Med 2006, 3:e442.2. Sobocki P, Lekander I, Borgström F, Ström O, Runeson B: The economic
burden of depression in Sweden from 1997 to 2005. Eur Psychiatry 2007,22:146–152.
3. Watkins KE, Burnam MA, Orlando M, Escarce JJ, Huskamp HA, Goldman HH:The health value and cost of care for major depression. Value Health2009, 12:65–72.
4. Berto P, D’Ilario D, Ruffo P, Di Virgilio R, Rizzo F: Depression: cost-of-illnessstudies in the international literature, a review. J Ment Health Policy Econ2000, 3:3–10.
5. Nuijen J: Tweedelijns GGZ voor volwassenen: ontwikkelingen in toegangen gebruik. In Trendrapportage GGZ 2010 deel 2. 1st edition. Edited byNuijen J. Utrecht, The Netherlands: Trimbos Instituut; 2010:59–114.
6. Andrews G, Cuijpers P, Craske MG, McEvoy P, Titov N: Computer therapyfor the anxiety and depressive disorders is effective, acceptable andpractical health care: a meta-analysis. PLoS One 2010, 5:e13196.
7. McCrone P: Cost-effectiveness of computerised cognitive-behaviouraltherapy for anxiety and depression in primary care: randomisedcontrolled trial. Br J Psychiatry 2004, 185:55–62.
8. Cuijpers P, Van Straten A, Schaik A, Andersson G: Psychological treatment ofdepression in primary care: a meta-analysis. Br J Gen Pract 2009, 59:e51–e60.
9. Richards D, Richardson T: Computer-based psychological treatments fordepression: a systematic review and meta-analysis. Clin Psychol Rev 2012,32:329–342.
10. Andersson G, Cuijpers P: Internet-based and other computerizedpsychological treatments for adult depression: a meta analysis.Cogn Behav Ther 2009, 38:196–205.
11. Tate DF, Finkelstein EA, Khavjou O, Gustafson A: Cost effectiveness of internetinterventions: review and recommendations. Ann Behav Med 2009, 38:40–45.
12. Bowman DG: Self-examination therapy: treatment for anxiety anddepression. In Innovations in Clinical Practice: A Source Book. Edited byVandeCreek L. Sarasota, FL: Professional Resource Press; 1995.
13. Bowman D, Scogin F, Lyrene B: The efficacy of self-examination therapyand cognitive bibliotherapy in the treatment of mild to moderatedepression. Psychother Res 1995, 5:131–140.
14. Van Straten A, Cuijpers P, Smits N: Effectiveness of a web-based self-helpintervention for symptoms of depression, anxiety, and stress:randomized controlled trial. J Med Internet Res 2008, 10:e7.
15. Warmerdam L, Van Straten A, Twisk J, Riper H, Cuijpers P: Internet-basedtreatment for adults with depressive symptoms: randomized controlledtrial. J Med Internet Res 2008, 10:e44.
Kenter et al. Trials 2013, 14:412 Page 9 of 10http://www.trialsjournal.com/content/14/1/412

16. Cuijpers P, Donker T, Johansson R, Mohr DC, Van Straten A, Andersson G:Self-guided psychological treatment for depressive symptoms: a meta-analysis. PLoS One 2011, 6:e21274.
17. Radloff LS: The CES-D scale: a self-report depression scale for research inthe general population. Appl Psychol Meas 1997, 1:385–401.
18. Beekman AT, Deeg DJ, Van Limbeek J, Braam AW, De Vries MZ, Van TilburgW: Criterion validity of the center for epidemiologic studies depressionscale (CES-D): results from a community-based sample of older subjectsin The Netherlands. Psychol Med 1997, 27:231–235.
19. Donker T, Van Straten A, Marks I, Cuijpers P: Brief self rated screening fordepression on the internet. J of Affect Disord 2010, 122(3):253–259.
20. Kessler RC, Abelson J, Demler O, Escobar JI, Gibbon M, Guyer ME, HowesMJ: Clinical calibration of DSM-IV diagnoses in the World Mental Health(WMH) version of the World Health Organization (WHO) CompositeInternational Diagnostic Interview (WMH-CIDI). Int J Methods Psychiatr Res2004, 13:122–139.
21. Spinhoven P, Ormel J, Sloekers PP, Kempen GI, Speckens AE, Van Hemert AM:A validation study of the Hospital Anxiety and Depression Scale (HADS) indifferent groups of Dutch subjects. Psychol Med 1997, 27:363–370.
22. Bastien CH, Morin CM, Ouellet M-C, Blais FC, Bouchard S: Cognitive-behavioraltherapy for insomnia: comparison of individual therapy, group therapy,and telephone consultations. J Consult Clin Psychol 2004, 72:653–659.
23. Brooks R: EuroQol: the current state of play. Health Policy 1996, 37:53–72.24. Hakkaart-Van Roijen L, Tan SS, Bouwmans CAM: Handleiding voor
kostenonderzoek: methoden en standaard kostprijzen voor economischeevaluaties in de gezondheidszorg. College voor zorgverzekeringen.Geactualiseerde versie; 2010. http://www.cvz.nl/binaries/content/documents/zinl-www/documenten/publicaties/overige-publicaties/1007-handleiding-voor-kostenonderzoek/Handleiding+voor+kostenonderzoek.pdf.
25. Van Den Brink M, Van Den Hout WB, Stiggelbout AM, Putter H, Van DeVelde CJH, Kievit J: Self-reports of health-care utilization: diary orquestionnaire? Int J Technol Assess Health Care 2005, 21:298–304.
26. Smit F, Willemse G, Koopmanschap M, Onrust S, Cuijpers P, Beekman A:Cost-effectiveness of preventing depression in primary care patients:randomised trial. Br J Psychiatry 2006, 188:330–336.
27. Pearlin LI, Schooler C: The structure of coping. J Health Soc Behav 1978, 19:2–21.28. Ewing JA: Detecting alcoholism: the CAGE questionnaire. JAMA 1984,
252:1905–1907.29. O’Brien CP: The CAGE questionnaire for detection of alcoholism: a
remarkably useful but simple tool. JAMA 2008, 300:2054–2056.30. Costa PT, Mccrae RR: Normal personality assessment in clinical practice:
the NEO personality inventory. Psychol Assess 1992, 4:5–13.31. Clark LA, Watson D, Mineka S: Temperament, personality, and the mood
and anxiety disorders. J Abnorm Psychol 1994, 103:103–116.32. Devilly GJ, Borkovec TD: Psychometric properties of the credibility/
expectancy questionnaire. J Behav Ther Exp Psychiatry 2000, 31:73–86.33. De Brey H: A cross-national validation of the client satisfaction
questionnaire: the Dutch experience. Eval Program Plann 1983, 6:395–400.34. Schulz KF, Altman DG, Moher D, for the CONSORT Group: CONSORT 2010
Statement: updated guidelines for reporting parallel group randomisedtrials. Br Med J 2010, 340:c332.
35. Little RJA, Rubin DB: The analysis of social science data with missingvalues. Sociol Methods Res 1989, 18:292–326.
36. Cohen J: Statistical Power Analysis for the Behavioral Sciences. Hillsdale NJ:Erlbaum; 1988.
37. Koopmanschap MA, Van Exel NJ, Van Den Bos GA, Van Den Berg B, BrouwerWB: The desire for support and respite care preferences of Dutchinformal caregivers. Health Policy 2004, 68:309–320.
38. Sarrami Foroushani P, Schneider J, Assareh N: Meta-review of the effectivenessof computerised CBT in treating depression. BMC Psychiatry 2011, 11:131.
doi:10.1186/1745-6215-14-412Cite this article as: Kenter et al.: Effectiveness and cost effectiveness ofguided online treatment for patients with major depressive disorder ona waiting list for psychotherapy: study protocol of a randomizedcontrolled trial. Trials 2013 14:412.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit
Kenter et al. Trials 2013, 14:412 Page 10 of 10http://www.trialsjournal.com/content/14/1/412