Embed Size (px)
Citation preview

EFFECTIVELY COMMUNICATING ACTIONABLE IMAGING RESULTS
The best way to predict the future is to create it.”-Peter Drucker
Florida Society for Healthcare Risk Management and
Patient Safety
August 12th & 13th
Dr. Richard Friedland FACR
Disclosure: I am a shareholder and CEO of Radloop

Defining our Terms: Types of Results
• Critical Finding: A diagnostic finding that requires immediate or urgent medical intervention. This finding could lead to death if not promptly acted upon. Example- Rupturing abdominal aortic aneurysm
• Incidental Finding: An incidentally discovered mass or lesion, detected by imaging performed for a reason unrelated to the original reason for the examination. Example – renal cyst or renal mass, unruptured aneurysm when doing a CT abdomen/pelvis for abdominal pain.
• Actionable Finding: A finding that requires non-routine communication because of the importance of the findings or its unexpected nature. Example -a renal cancer when doing a CT scan for abdominal pain
• These findings can fall into 1 of these 3 categories:• Category 1 – communication within minutes (red)• Category 2 – communication within hours (orange)• Category 3 – communication within days (yellow)

Critical Actionable FindingCategory 1 (Red)
Acute Rupture of an Abdominal Aortic Aneurysm

How do Radiologist Feel about the Communication Critical Findings?
AJR 2014; 202:W306 0361–803X/14/2023–W306
•A survey of American College of Radiology members found that 97% agree that communication of emergent findings to referring physicians should be accomplished by telephone or in person.

Critical Actionable FindingCategory 1 (Orange)
Pre-operative CXR CT Chest the next day

Incidental Actionable Finding (Yellow)
Incidental finding 2014EVAR group, (1.5%) patients died, compared to (4.6%)
patients who died in the open surgery group for elective AAA repair.
Critical finding in 2020Ruptured abdominal aortic aneurysms (rAAA) are associated with an overall mortality rate of over 80%, and, according to the US Centers for Disease Control and Prevention.

ACR White Paper on Follow up of Aortic Aneurysms
Aortic Diameter (mm) Imaging Interval2.5-2.9 5 y
3.0-3.4 3 y
3.5-3.9 2 y
4.0-4.4 1 y
4.5-4.9 6 mo.⁎
5.0-5.5 3-6 mo.⁎
Recommended intervals for initial follow-up imaging of ectatic aortas and abdominal aortic aneurysmsNote: For abdominal aortic diameters <2.5 cm, follow-up is generally thought to be unnecessary. Because the rupture of smaller abdominal aortic aneurysms is less likely, we recommend longer intervals between follow-up examinations. Follow-up intervals may vary depending on comorbidities and the growth rate of the aneurysm.*In addition to planning follow-up imaging, one should also consider surgical or endovascular referral.

AJR 2017; 209:W194 0361–803X/17/2093–W194
•Only 24% of Radiologists agreed that significant, unexpected findings should communicated. • The courts have consistently ruled that if Radiologists
find an abnormality that if left untreated could ultimately be fatal to a patient, no matter whether death would occur in an hour, a day, a month, or a year, the Radiologist has an absolute duty to communicate the finding directly to the referring clinician.•Radiologists, what is your strategy for communicating
these significant unexpected results- Hope• This represents is a huge care gap.
How do Radiologists feel about the Communication of Incidental Unexpected Findings ?

58-year-old male, 60 pack-year Smoker, 2016
9
• Radiology report:
• 8 mm irregular nodule left upper lobe recommend- the typical recommendation is to follow up in 8 weeks post treatment with antibiotics.
• In smokers, radiologists see lots of transient lesions and densities. In high-risk patients, the guidelines call for short term CT follow up post treatment for resolution of the findings.

The patient returns to Lung Screening CT in 2019, 3 years later.
10
• Radiology report• 3.0 cm irregular mass left upper lobe dx.-
pathology proven NSCLC
• Lung cancer screening CT has been demonstrated to decrease mortality.
• Over 50% of patient diagnosed with lung cancer already have distant disease, Stage 4 (with 5-year survival less than 6%)... with lung cancer screening there is an opportunity to diagnose localized disease and save lives. The survival for Stage 1 Lung cancer is 90-71%.

63-year-old man goes to the Urologist for Hematuria , R/O Bladder lesion
11
• Radiology report:• Impression: 1 cm polypoid mass in the
bladder, no extension though the vesicular wall observed.
• In the body of the report but not in the impression , mildly dilated pancreatic duct, R/o pancreatic mass- recommend at follow up MRI with contrast of the the abdomen.

One year later the man returns to the ER with Abdominal Pain.
12
• Radiology report:
• Dilated pancreatic duct with a 3cm mass in the body of the pancreas. Peripancreatic lymph nodes and infiltration of the peripancreatic fat.
• He now has stage 4 disease. Median survival 4 months. 5-year survival 3%.

What Does Automation and Closed Loop Communication Ensure ?
•Automatically capturing actionable findings from radiology reports ensures important unexpected findings are acted upon.•Closed loop communication of these results protects our patients, in doing so, also protects the doctors and their respective institutions.

Civilization advances by extending the number of important operations which we can perform without thinking of them.
Alfred North Whitehead
Philosopher and Mathematician

• The estimated rate of severe patient harm events directly related to a
breakdown in the communication of abnormal radiology test is
1.33/100,000 studies, with improved follow-up the rate drops to
.35/100,000.1
• For every 100,000 reports one serious incident of patient harm is
eliminated.
• For 1 million reports, we could estimate 10 fewer episodes of severe
patient harm per year.
1 Reducing Delay in Diagnosis: Multistage Recommendation TrackingBen Wandtke and Sarah GallagherAmerican Journal of Roentgenology 2017 209:5, 970-975
Quantifying the Reduction in Patient harm and Risk Reduction

• With 1,000,000 reports, 10 fewer episodes
of severe patient harm per year
• Average cost of defending a lawsuit is
$46,000 in 2016 1
• Average settlement is $425,000 2
• Average Jury Award is over $1,000,000 2
Source:
1 Crico
2 Length and Process of a Medical Malpractice Suit
3 Healthcare Economics & Policy
Legal Costs Potentially Avoided Nov. 2017Patient had a CT scan of abdomen & pelvis for
low grade prostate cancer.
A lung mass was detected, and additional
testing was recommended, but not
communicated to the patient
May 2019Patient returned experiencing pain and
swelling in his shoulder and chest.
New CT scan revealed lung cancer had
metastasized
June 2019Patient passed away
May 2020
$7.5M settlement 3

The Growth of Medical Imaging
• The first patient CT (Computed Tomography) scan was performed in 1971.
• Over 75 million CT scans are performed each year in the United States. This number is forecasted to grow to reach 84 million procedures by 2022.
• The first MR scan of the human body was performed in 1977.
• Nearly 40 million MRI scans are performed annually in the United States.

How Common are Incidental/Actionable Findings?
18
• Incidental findings are an inevitable consequence of increasing imaging volumes and have been found in as many as 55% of trauma patients undergoing whole-body CT.
• The estimated incidence of actionable findings ranges from 9% among screening patients to as high as 31% among patients with known cancer.
• 12.7% rate of recommended follow up imaging in my own practice.
Seah MK, Murphy CG, et. al Incidental findings on whole-body trauma computed tomography: experience at a major trauma center. Injury 2016; 47:691–694Pickhardt PJ, Hanson ME, Vanness DJ, et al. Unsuspected extracolonic findings at screening CT colonography: clinical and economic impact. Radiology 2008; 249:151–159Lardinois D, Weder W, et al. Etiologyof solitary extrapulmonary positron emission tomography and computed tomography findings in patients with lung cancer. J Clin Oncol 2005;23:6846–6853

Alert Fatigue: A Clear and Present Danger
Singh H, et al. JAMA Intern Med 2013
• A survey of PCPs in VAMCs (N=2590)
• Using system where abnormal test result alerts are manually triggered by the radiologist
• Median number of alerts received by PCP each day = 63
• 87% perceived that the quantity of alerts was excessive
• 70% reported receiving more alerts than they could effectively manage
• 30% reported having personally missed results that led to care delays

What is the Down Stream Effect of Increased Imaging Volumes on our Colleagues
20
• The typical clinician is responsible for reviewing 1000 test results per week.• The most common missed results were imaging
studies.•30-70% of radiology recommendations do not result
in completion of the recommended imaging test .
Wahls TL, Cram PM. BMC Family Prac 2007Lorincz CY, et. al. Research in Ambulatory Patient Safety 2000-2010. AMA

Artificial Intelligence and Radiology• AI right now is narrow. It can find an intracranial bleed or a subtle
pulmonary embolus and move it to the top of the read list.
• AI will improve radiologist's workflow and allow them to be more efficient and evaluate more images in less time.
• The promise of AI is to lower the cost, decrease human labor (address burnout) and improve diagnostic accuracy.
• AI will increase the number findings that need to be communicated.
• In doing so there will more, not less need for communication of important imaging findings.

Data & Doctors
22
• Radiologist • Referring Doctor

2015 - CT shows a small lung
nodule, stage 1 cancer , with a 71%
- 5-year survival1
2018 - the small nodule is now a
mass, stage 4 cancer with a 6%
- 5-year survival1
57-year-old male smoker comes to the ER for kidneys stones 2015, he is lost to follow-up, but returns to the ER
for abdominal pain in 2018.
1 American Cancer Society information from the SEER database, maintained by the National Cancer Institute (NCI)

The Problem : What Happened to the Imaging Result ?
24
• We don’t know what happened to the report or the results. • Should all these incidental actionable findings be called?• Did the report reach the ER doctor, did he/she see the report? • Did he/she see the recommendation in the report ? • Did the patient’s PCP ever see the report ?• Was the patient notified of a significant finding that needed follow up ?• If the someone had seen the recommendation:
• A follow up exam may have been performed.• The patient may go to see a pulmonologist or thoracic surgeon.• The definitive diagnosis would have been made sooner.• The patient may or may not have had the chance for a curative procedure• The patient may have had a longer life by starting treatment sooner.• The family would have some sense of closure and no nagging doubts due to the delay in
diagnosis.• Potential reputational damage to the Doctors and Institution spared.• No lawsuit would have been filed.

Chronic Repetitious Problems: The Handoff
Dutta S, Long WJ, Brown DF, Reisner AT. Automateddetection using natural language processingof radiologists recommendations for additionalimaging of incidental findings. Ann Emerge Med2013; 62:162–169
•One review of ED’s discharge instructions revealed that only about half of radiologists’ follow-up recommendations were conveyed to patients.

Transitions of Care are a Serious Risk
Deficits in Communication and Information Transfer Between Hospital-Based and Primary Care Physician implications for Patient Safety and Continuity of CareSunil Kripalani, MD, MSc; Frank LeFevre, MD; Christopher O. Phillips, MD, MPH; et alMark V. Williams, MD; Preetha Basaviah, MD; David W. Baker, MD, MPHJAMA. 2007;297(8):831-841. doi:10.1001/jama.297.8.831
•Direct communication between hospital physicians and primary care physicians occurred infrequently (3%-20%).
•Discharge summaries often lacked important information such as diagnostic test results (missing from 33%-63%), and test results pending at discharge (65%).

The ED is the “Perfect Storm” for Test Tracking Errors
• The ED is particularly challenging for test-result follow up due to the focus on rapid turnover and high-volume patient throughput, team-based care, handoffs and lack of continuous relationships between patients and clinicians.•Current EMR’s seem particularly vulnerable to
longitudinally following patients from different settings.

Failure to Comply with Follow up Radiology Report Recommendations
J Am Coll Radiol 2018;15:422-428.
•Recommendations are not always followed up by referring physicians and patients.
•Based on 2,972,164 examinations, the overall follow-up adherence rate within 14 months of the index examination was 58%, with mammography having the highest adherence rate at 69% and nuclear medicine having the lowest adherence rate at 38%.

Lost to Follow up
Lost to Follow-Up: Analysis of Never-Viewed Radiology ExaminationsAnthony Galinato, Matthew D. Alvin, David M. YousemJournal of the American College of RadiologyPublished online: November 2, 2018
•7,438 Imaging studies were completed.
•622 (8.4%) had neither the images nor the imaging reports viewed in either the PACS or EMR the 8 months after the imaging order was placed.•247 cases (39.7%) classified as Grade 3 (findings
requiring intervention or follow-up)•3 cases (0.5%) classified as Grade 4 (critical)

If you had a Time Machineyou could go back to the future and alter outcomes and save lives.
We do not have a Time Machine but….
but we have tools at our disposal right now that can alter outcomes and save lives.
30

British science fiction writer Arthur C. Clarke formulated three adages that are known as Clarke's three laws.
1. When a distinguished but an elderly scientist states that something is possible, he is almost certainly right. When he states that something is impossible, he is very probably wrong.
2. The only way of discovering the limits of the possible is to venture a little way past them into the impossible.
3. Any sufficiently advanced technology is indistinguishable from magic.

What ”Magic” /Technology would we build to Alter the Future for our Patients?
• A scalable system automatically identifies, and extracts follow up recommendations using NLU AI (which reads the whole report).
• Recommendations are sent to the clinician's smart phone, tablet or desktop via a dedicated application.
• The asymmetric communication allows the ordering clinician to review the actionable recommendation and act on it, when and where he/she chooses without being intrusive or interrupting their workflow.
• The actionable recommendation can be easily translated into an order on an app, allowing the physician to promptly and efficiently handle follow up recommendations in a matter of seconds or rapidly sent to a navigator to handle.
• Everything is documented in the medical record, protecting all the parties, while delivering effective follow up care to the patient.
• Either phone call, email, mail would notify the patient of a significant finding and document the interaction.
• The system would have inherent redundancy and administrative oversight.

A Flexible Solution is Required:Not all Doctors or Departments , Healthcare systems work the same way
7/25/2021 33
Doctors may want to do the follow ups on their phone or on the web app or doctors can delegate follow ups to staff via the web app.
Doctors can consult with each other on the app increasing communication and facilitating better care
If the referring Doctors do not respond, letters can be sent to the patient.
There is administrative oversite to ensure loop closure, so that no one can fall through the cracks.

Why a Mobile App?• Mobile apps are an asymmetric form of communication.
• The information is automatically pushed to you.• It is available whenever and wherever you and your
phone/tablet are.• This form of communication does not disrupt the provider
particularly when he/she are with patients.• The rest of the world works on their phones and their
laptop (just ask my kids).• The mobile apps need to communicate with the EMR to
maintain a permanent record of all interactions. (Think Amazon, order on your phone but its on your webpage in the computer.)

Why a Mobile App?
• “In 2017, 46% of respondents in a survey about Christmas spending said they use their smart phones for online shopping, which is a 6% increase from the preceding year. In 2019, around 70% of consumers used smartphones for holiday purchases.”
• Fotunly Jun 18, 2020

An App integrated into your EMR can ultimately function like a Radiology EMR+.
1. Think about doing away with paper.2. How about never using 1980’s fax technology.3. Having all your reports available all the time.4. Never having to call the radiology department
for your results5. Immediately being able to the Radiologist6. Having the actionable results separated into a
different inbox7. Important results can get pushed on request.8. You can order the follow up exam immediately
and easily on the phone.9. You can call/notify your patient immediately.

Web Based Desktop Application

Why use a Desktop Navigator Tool?• Many doctors do not want to use an app.
• Many department/offices will designate one person to manage all the follow ups for the whole department or office. This is analogous to tracking mammography results.
• Different departments/offices can use the navigator for follow up tracking. Pulmonary/GI/Surgical Oncology and Radiology can have navigators that are linked to ensure patient follow up.
• Non-imaging follow ups can be easily communicated, recommend surgical consult, recommend colonoscopy.
• Letters/Email/Text/Phone calls can be sent to the referring and/or the patients.

Why use a Desktop Application?
• A desk top tool can have many roles• Administrative oversite of all follow-up management.
• One place that oversee the whole program.
• Analytics• How are we doing as an organization doing or at a particular site ?
• How are individual physicians doing with both recommendations and follow ups ?
• What is our rate of recommendation, what is our follow up rate , how do we improve that rate ?
• How much revenue is this program providing the organization ?
• Navigator
• Physician role

Sample Analytics Dashboard
©2021 Radloop. All Rights Reserved
Radiologist Feedback Report

Web Navigational DashboardClinician Mobile Application
©2021 Radloop. All Rights Reserved

RL & the Community Grant:What was Evaluated
• Improving Diagnostic Accuracy through Improved Communication to Patients with Incidental Findings on ED Medical Imaging Studies
• The project began in January 2019 and concluded March 2021, during which time we reviewed 138,603 ED-based imaging reports with a high probability of having IFs, identified 9,577 studies with follow-up recommendations, determined through navigation that 5,999 IFs needed to be communicated, and communicated those results to 4,962 patients and 300 PCPs. The grant covered 8 radiology group’s emergency rooms from around the USA.

Grant Conclusions
• 6.91% of all cases reviewed included follow-up recommendations.
• Stakeholders agreed that there is a great opportunity to improve the process resulting in improved communication, increased follow up on recommended exams, increased patient engagement, and ultimately better outcomes through outreach.
• Radiologists are open to feedback on opportunities we uncovered to improve documentation in reports.

Community Grant Lessons
• Additional IFs and follow-up recommendations not included in the grant were identified by navigator and practice physicians as gaps in care, for example liver masses, thyroid nodules, ovarian cysts, colonoscopy, and breast masses.
• Patients shared that they had been to the ED for events that led to longer hospital stays or extended stays in rehab. The letter helped them to reach out to their physicians.
• Patients provided the letter to their physicians resulting in physicians reaching out to navigator to request findings.

Community Grant Findings So Far
• Patients were surveyed post communication, the majority who responded were satisfied with receiving a letter.• 68% were not aware/unsure of a follow-up recommendation for IFs
associated with their ED visit
• 86.8% said they would contact their physician for follow up based on the letter you received
• Just 7.18% of patient records included their PCP, a figure that might be improved with changes to intake protocol to ensure that primary care physicians names and contact information is obtained.

Key Insights from the Community Grant On IF in the ER
• Feedback from patients, physicians, and the practices has been very positive.
• The practices involved in the grant are now offering a program with their affiliated healthcare systems to reproduce the grant’s efforts on a national scale. The program is called RadReachtm.
• The findings from the Grant were presented 2 months ago to the sponsor/medical malpractice carrier.
• The results of the grant were so compelling that our sponsor spontaneously told us they would fund us to continue the study in the middle of our grant presentation.

• 1,000,000 radiology reports/year
• 13% follow-up recommendation rate for radiologists
• 130,000 exams with F/U recommendations
• 91% of exam recommendations are accepted by clinicians
• 118,300 exams approved for follow-up by the referring clinician.
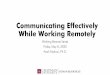
Recapture Revenue from follow up studies
Assumptions
• 26% of the 118,300 recommended
exams are lost to follow-up or 30,758
exams.
• Greater than 90% of follow-ups are
MRI or CT at a conservative
$500/exam global fees.
Total lost revenue = $14,196,000
• Recapturing 50% of the lost to follow-up
results in:
Revenue recaptured = $7,098,000
Outcome

Quality Pays
48
•“Good quality is less costly because of more accurate diagnoses, fewer treatment errors, lower complication rates, faster recovery, less invasive treatment, and the minimization of the need for treatment. More broadly, better health is less expensive than illness.”
― Michael E. Porter, Bishop William Lawrence University Professor at HBS, Redefining Health Care: Creating Value-Based Competition on Results

In Summary: How does Tracking Follow Ups with Closed loop Communication Improve Patient Care and Reduce Risk?
Wandtke and Gallagher. AJR 2017; 209:1–6
• Increases exam completion rate
• Identifies exam completed outside your institution
• Ensures Closure • Follow up Imaging• Biopsy or surgical excision• Limited life expectancy / palliative care• Specialist referral / management• Clinical resolution• Identification of additional non studies
• Moves the needle on real Quality and Safety/Risk
• Increases referring Doctor Satisfaction
• Increases Patient Satisfaction
• Increases Revenue
• Decreases liability & associated costs
• Creates a Strategic Advantage to your Organization

• “Give me a lever long enough and a fulcrum on which to place it, and I shall move the world”
• Archimedes
• "Whoever saves one life, saves the world entire.”
• Schindler’s List, paraphrasing The Talmud
•With the proper tools we do not have to go ”Back to the Future “, we can alter outcomes and change the future for our patients right now.