Embed Size (px)
Citation preview

Effective and Appropriate Antimicrobial Therapy
for Intra-abdominal Infections

Solomkin JS et al Ann Surg 2003;237:235–245.Yellin AE et al Int J Antimicrob Agents 2002;20:165–173.Fry DE Surg Infect 2001;2(Suppl 1):S3–S11.Pacelli F et al Arch Surg 1996;131:641–645.
The Clinical Impact ofIntra-abdominal Infection (IAI)
Complicated intra-abdominal infections are among the most common infections in general surgery
Even with current management, morbidity rates of 59% and mortality rates of 21% were reported in a retrospective study
Complicated IAI is a major cause of morbidity and mortality

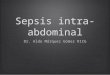
Pathogens Cattan(n=317)
Sendt(n=313)
Gram Positive Cocci Streptococcus spp. Enterococcus spp.Gram Negative Bacilli Escherichia coli Klebsiella spp. Enterobacter spp. Pseudomonas aeruginosaBacteroides fragilisOther Bacteroides spp.
12%7%
40%3%1%4%9%6%
7%6%
47%7%4%4%2%6%
Adapted from Gerth WC et al EJHP 2004;4:78–83.
Most Common Pathogens in 2 Studiesof Community-Acquired IAI

0
25
50
75
100
E. coli Enterococcus B. fragilis E. coli +Enterococcus
E. coli + B. fragilis
Enterococcus +B. fragilis
%
Abscesses
Mortality
Microbial Synergy in Experimental Intra-abdominal Abscess (in Wistar Rats)
Onderdonk AB et al Infect Immun 1976;13:22–26.
Role of Enterobacteriaceae and Anaerobes (rodents)

Appropriate Management ofComplicated IAI
Adequate resuscitation Surgical or radiological intervention Antimicrobial therapy
- Important adjunct to surgery and supportive therapy
- Should have appropriate coverage against gram-positive and gram-negative, aerobic and anaerobic bacteria
Solomkin JS et al Ann Surg 2003;237:235–245.Mazuski JE et al Surg Infect 2002;3:161–173. Yellin AE et al Int J Antimicrob Agents 2002;20:165–173.

Antimicrobial Resistance: A serious problem facing clinicians in the management of IAI
In nosocomial infections, there is an increasing prevalence of resistant Enterobacteriaceae - ESBL-producing E. coli or K. pneumoniae
•Previous fluoroquinolone or cephalosporin use is risk factor•Treatment failure observed with cephalosporins or
β-lactam/β-lactamase inhibitor combination•Increasing quinolone-resistance in ESBL-producing isolates
Carbapenem remains drug of choice Increasing prevalence of Bacteroides fragilis –
resistant to clindamycin, cefotetan, cefoxitin and quinolones
Rodriguez-Bano J et al J Clin Micro 2004;42:1089–1094. Paterson DL et al Ann Intern Med 2004;140:26–32. Paterson DL et al J Clin Micro 2001;39:2206–2212. Paterson DL Clin Microbiol Infect 2000;6:460–463. Paterson DL et al Clin Infect Dis 2000;30:473–478. Oh H, Edlund C Clin Microbiol Infect 2003;9:512–517. Elsaghier AAF et al J Antimicrob Chemother 2003;51:1436–1437.

Considerations in determining appropriate therapy:
Appropriate Antimicrobial Therapy
Spectrum of activity Timing and duration of therapy Dose and dosing frequency Drug interactions and tolerability Adequate drug levels Prior antibiotic treatment Potential for selecting antibiotic
resistance Raymond DP et al Surg Infect 2002;3:375–385. Moellering RM. In: GL Mandell, JE Bennett, R Dolin, eds. Principles and Practice of Infectious Diseases, 5th ed, 2000.

Beneficial Outcomes of Appropriate Antimicrobial Therapy
Improved chance of successful clinical outcome
Reduced mortality Decreased need for re-operation and
second- line therapy Reduced number of IV antibiotic days Shorter hospital length of stay Lower hospital costs Reduction in the emergence of
antimicrobial resistanceDavey P et al. ISPOR 6th Annual International Meeting; Virginia, USA, 2001. Bare M et al. ECCMID, Milan, Italy; 2002. Burke J et al. Presented at the 39th World Congress of Surgery, Brussels, Belgium; 2001. Sendt W et al. Presented at the 12th ECCMID (European Congress of Clinical Microbiology and Infectious Disease), Milan, Italy; 2002. Niederman MS et al Crit Care Med 2003;31:608–616.

Davey P et al. Presented at the International Society of Pharmacoeconomics and Outcomes Research Sixth Annual International Meeting; Virginia, USA, 2001.
*Successful outcome was defined as resolution with no change in treatment
IAI patients with adequate empiric therapy were significantly more likely to have successful clinical outcome*
Appropriate Antimicrobial Therapy for IAI: Successful Clinical Outcome
p<0.05
81.9%
58.9%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Empiric antibiotictherapy appropriate
(n=238)
Empiric antibiotictherapy inappropriate
(n=56)
Per
cent
age
of p
atie
nts
with
cl
inic
al s
ucce
ss (
%)

Appropriate Antimicrobial Therapy for IAI: Reduced Mortality
Mortality was substantially lower for IAI patients who received appropriate empiric therapy
Bare M et al. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases, Milan, Italy; 2002.
p<0.05
12%
23%
0.0%
10.0%
20.0%
30.0%
40.0%
Appropriate antibiotic therapy (n=272)
Inappropriate antibiotic therapy (n=93)
Mor
talit
y (%
)

Sendt W et al. Presented at the 12th Annual European Congress of Clinical Microbiology and Infectious Diseases, Milan, Italy; 2002.
Patients (N=425) given appropriate initial empiric therapy for IAI were less likely to undergo re-operation and require second-line antibiotic therapy
Appropriate Antimicrobial Therapy for IAI: Decreased Need for Re-operation and Use of Second-Line Therapy
Patient died
Resolved afterre-operation
Resolved withsecond-linetherapy
Resolved withinitial or step-down therapy
5781
27
12 113
54
0
20
40
60
80
100
Appropriate InitialEmpiric Antibiotic
Therapy
Inappropriate InitialEmpiric Antibiotic
Therapy
Per
cent
age
(%)

Davey P et al. Presented at the International Society of Pharmacoeconomics and Outcomes Research Sixth Annual International Meeting; Virginia, USA, 2001.
10 days
Appropriately treated IAI patients experienced 10 fewer hospital days
Appropriate Antimicrobial Therapy for IAI: Decreased Length of Hospital Stay
(LOS)
22
12
0
5
10
15
20
25
Appropriate EmpiricAntibiotic (n=129)
Inappropriate EmpiricAntibiotic (n=33)
Leng
th o
f Sta
y (D
ays
) p<0.05

“Collateral Damage”
“Collateral damage is ecological adverse effects of antibiotic therapy… that is, the selection of antibiotic-resistant organisms and the unwanted development of colonization or infection with such organisms”
Paterson DL et al Clin Infect Dis 2004;38(Suppl 4):S341–S345.

Selection of Antibiotic-Resistant Pathogens
Summary of potential “collateral damage” from use of cephalosporins and quinolones
Class of agent, pathogen(s) selected for
Third-generation cephalosporinsVancomycin-resistant enterococci (VRE)
Extended-spectrum ß-lactamase–producing Klebsiella species
ß-lactam–resistant Acinetobacter species
Clostridium difficile
QuinolonesMethicillin-resistant Staphylococcus aureus (MRSA)
Quinolone-resistant gram-negative bacilli, including Pseudomonas aeruginosa
Adapted from Paterson DL Clin Infect Dis 2004;38(Suppl 4):S341–S345.

In a single-center retrospective study (880 in-patients; 233 VRE cases and 647 matched controls) an increase in VRE* (54 cases/10,000 admissions) was associated with third-generation cephalosporins (p<0.001), I.V. metronidazole (p=0.008), and longer duration of quinolone use (p=0.05).
In vitro results from patients at 15 Brooklyn hospitals showed that cephalosporin use correlated with emergence of a multi-resistant clone of Acinetobacter spp. *VRE = vancomycin-resistant Enterococcus
Carmeli Y et al Emerg Infect Dis 2002;8:802–807.Landman D et al Arch Intern Med 2002;162:1515–1520.
Risk Factors for VRE andAcinetobacter spp.

Previous administration of oxyimino-containing antibiotics (e.g., cefuroxime, cefotaxime, ceftriaxone, ceftazidime, aztreonam) were associated with bacteremia due to ESBL-producing strain
15 (18%) of 83 ESBL-producing strains isolated in 455 episodes of K. pneumoniae bacteremia were ciprofloxacin resistant
43 of 77 strains (55.8%) of ESBL-producing E. coli and K. pneumoniae were resistant to fluoroquinolones
Paterson DL et al Ann Intern Med 2004;140:26–32.Paterson DL et a Clin Infect Dis 2000;30:473–478.Lautenbach E et al Clin Infect Dis 2001;33:1289–1294.
Challenges in the Clinical Management of ESBLs

Community Transmission of ESBLs
Arpin C et al Antimicrob Agents Chemother 2003;47:3506–3514.
Distribution of ESBL producers- 39/2599 (1.5%) detected among the family
Enterobacteriaceae23/887 (2.6%) strains from clinics11/128 (8.6%) strains from nursing homes
Conclusions: - A variety of ESBLs and ESBL producers are present in the
extrahospital setting.- The spread of ESBL-producing organisms to the
community seems to be related to previous nosocomial acquisition.
- Monitoring patients for ESBL-producing Enterobacteriaceae in general practice is required.

Risk Factors for Fluoroquinolone Resistance
Lautenbach E Arch Intern Med 2002;162:2469–2477.
Multivariable analysis of risk factors for fluoroquinolone resistance in E. coli and K. pneumoniae- Prior fluoroquinolone use- LTCF (Long-term care facility) residence- Prior aminoglycoside use- Older age
Correlation of fluoroquinolone resistance and prior fluoroquinolone use- In subanalysis of the 41 patients who received FQ
during the 30 days prior to infection, 35 (85.4%) had an FQ-resistant infection.
In a hospital-based case control investigation (n=205):

Lautenbach E Arch Intern Med 2002;162:2469–2477.
Correlation of Fluoroquinolone-Resistant Pathogens to Other Agents
In a hospital-based case-control investigation (N=205): Antimicrobial susceptibilities of fluoroquinolone-resistant and
fluoroquinolone-susceptible isolates
010203040
50607080
Ampicillin-sulbactam
Cafazolin CeftriaxoneSodium
Sulfa-methoxazole-Trimethoprim
GentamicinSulfate
Imipenem Nitro-furantoin
Tetracycline
FQ Resistant
FQ Susceptible
% R
esis
tan
t

Treatment with any fluoroquinolone for acquiring piperacillin-resistant P. aeruginosa may be a risk factor
If treatment with an antibiotic active against gram-negative bacteria is needed, agents with little antipseudomonal activity should be preferred to limit the emergence of multidrug-resistant Pseudomonas aeruginosa (MDRPA)
Paramythiotou E et al Clin Infect Diseases 2004;38:670–677.
Risk Factors for Selecting Pseudomonal Resistance
In a matched case-control study conducted between 1999 and 2000 in France:

The Role of Carbapenems in the Era of
Antimicrobial Resistance

*Ertapenem has minimal activity against non-fermentative gram-negative bacilli
Shah PM, Isaacs R J Antimicrob Chemother 2003;52:331–344.
Properties of Carbapenems
Excellent clinical efficacy
Broad-spectrum coverage over gram-positive and gram-negative aerobic and anaerobic pathogens*
Rapidly bactericidal
Proven tolerability profile
Low risk for resistance selection

Carbapenems: Low Risk for Resistance Selection
Enterobacteriaceae Resistance to carbapenems remains rare
- as proven with > 18 years of imipenem use
- carbapenem is drug of choice in treating ESBL-producing gram-negative bacilli
-lactamase (ESBL and AmpC) alone cannot cause resistance to carbapenem
Resistance of Klebsiella to ertapenem- requires both hyper-production of -lactamase (e.g., ESBL or AmpC) PLUS
chromosomal mutation (extreme impermeability or efflux mutations)
Little inoculum effect
Gold HS, Moellering RC N Engl J Med 1996;335:1445–1452.Fung-Tomc JC et al Antimicrob Agents Chemother 1996;40:1289–1293.Kohler J et al Antimicrob Agents Chemother 1999;43:1170–1176.Dorso KL et al Presented at the 23rd International Congress of Chemotherapy (ICC), South Africa, 2003.

Imipenem: Resistance in Enterobacteriaceae
59 / 1.42 million isolatesUSA 1996–2002, TSN
0 / >220,000 isolatesUSA 1998–2001, TSN
2 / >125,000 isolatesEurope 2000–2001, The
Surveillance Network (TSN) databases
Karlowsky JA et al Antimicrob Agents Chemother 2003;47:1672–1680.Wenzel RP et al Antimicrob Agents Chemother 2003;47:3089–3098.Livermore DM Ann Med 2003;35:226–234.

Friedland I et al. Presented at the 13th ECCMID, Glasgow, UK, May 10–13, 2003. Poster #789. Friedland I et al. 3 rd ACCP, Santa Margherita, Portofino, Italy, October 16–19, 2003. Poster #57.Data on file, MSD.
Ertapenem: Low Risk for Resistance Selection
0%
5%
10%
15%
20%
25%
30%
ErtapenemN=348
Piperacillin-TazobactamN=153
Per
cent
of p
atie
nts
% R %ESBL % R %ESBL % R %ESBLCeftriaxone + Metronidazole
N=193
OASIS = Optimising Intra-Abdominal Surgery with INVANZ™ study% R: Enterobacteriaceae resistant to study drug % ESBL: ESBL-producing E. coli and Klebsiella spp.
End of Rx
End of Rx; or test of cure
OASIS I OASIS II

Data from OASIS 1* and 2**: Imipenem-Resistant P. aeruginosa:
*Friedland I et al. 13th ECCMID, Glasgow, UK, May 10–13, 2003**Friedland I et al. 3rd ACCP, Santa Margherita, Italy, October 16–19, 2003 (Poster #57)
0/193 (0.0%)NA2/196 (1.0%)OASIS 2**
NA1/158 (0.6%)0/162 (0.0%)OASIS 1*
Ceftriaxone/Metronidazole
Piperacillin-Tazobactam
Ertapenem
Based on discontinuation of therapy (DCOT) and/or test of cure (TOC) swabs

2003 IDSA Guidelines on Anti-infective Agents for Complicated IAIs
Imipenem, MeropenemErtapenemCarbapenem
Ciprofloxacin + MetronidazoleFluoroquinolone
-based
3rd/4th Gen. Cephalosporin + Metronidazole
Cefazolin or Cefuroxime + Metronidazole
Cephalosporin-basedCombinati
on Regimen
Piperacillin/TazobactamAmpicillin/Sulbactam
Ticarcillin/Clav.
β-lactam/β-lactamase
inhibitorSingle Agent
With Risk Factor*
Without Risk Factor*
Health Care-Associated/ Nosocomial Infections
Complicated Community-Acquired Infections
ClassType of Therapy
Solomkin JS et al Clin Infect Dis 2003;37:997–1005.* Higher APACHE II scores, poor nutritional status, significant cardiovascular disease, patients with
immunosuppression
Fluoroquinolone +
Metronidazole

Major Coverage Requirements
• E. coli and other Enterobacteriaceae
• B. fragilis and other anaerobes
• Streptococci
Patient Origination
• IAI acquired outside the hospital
Carbapenem Classifications
• Enterococcus• Enterobacter spp.• Staphylococcus aureus• P. aeruginosa• E. coli and other Enterobacteriaceae
• IAI acquired during hospitalizations (nosocomial)
Group 1 Carbapenem (e.g., ertapenem)
Group 2 Carbapenem(e.g., imipenem, meropenem)
Shah PM, Isaacs RD J Antimicrob Chemother 2003;52:538–542.Roehrborn A et al Clin Infect Dis 2001;33:1513–1519.

Ruptured appendix Diverticulitis Cholecystitis Acute gastric and
duodenal perforation Traumatic perforation of
the intestines Intra-abdominal abscess
(including liver and spleen)
IAI Patient Types for Ertapenem
• Complicated intra-abdominal infections associated with secondary peritonitis
• Without risk factors*
*Risk factors (e.g.)•high APACHE II scores (>10)•poor nutritional status•significant cardiovascular disease• inability to obtain adequate control of the source of infection•use of corticosteroid therapy

IAI Patient Types for Imipenem
*Risk factors (e.g.)•high APACHE II scores (>10)•poor nutritional status•significant cardiovascular disease• inability to obtain adequate control of the source of infection•use of corticosteroid therapy
Patients with immunosuppression
- e.g., medical therapy for transplantation
Patients at risk for nosocomial infections caused by resistant organisms
- e.g., prolonged length of hospital stay, prior antibiotic therapy
Patients with complicated pancreatitis
- pancreatic abscess and/or necrotizing pancreatitis
• Postoperative peritonitis, tertiary peritonitis, and pancreatitis with risk factors*

A 36-year-old male experiencing bloating, abdominal distention, nausea, and vomiting
A double-barrel sigmoidostomy was inserted the previous month due to extensive perianal fistulas and abscess formation
Ultrasound: Significant colon enlargement, evacuation obstruction in the colostomy area, suspected kinking, and colon wall thickening
Has not received any previous antibiotic medication
Diagnosed as perforated colon with secondary peritonitis
IAI Patient Case Study 1 – Previous History
Ertapenem A 72-year-old female,
transferred to the surgical ICU, controlled with mechanical ventilation
Perforation of the sigmoid colon due to diverticulitis with localized peritonitis
6 days after initial treatment (surgical intervention + antimicrobial therapy with piperacillin-tazobactam 13.5g/day), showed rapid clinical deterioration
Diagnosed as severe post-operative peritonitis with multi-organ dysfunction
Imipenem

A 44-year-old male, brought to the emergency department
Onset of chills during the past 24 hours, experienced mild nausea and abdominal pain 2 days ago
Ultrasound: Fluid in the periappendiceal area, along with thickening and edema of appendix
History of recent antibiotic treatment with oral ceftriaxone
Blood cultures obtained preoperatively grew ESBL+ E. coli
IAI Patient Case Study 2 – Emergence of ESBL
A 65-year-old male, admitted to the surgical ICU
At laparoscopy noted to have a duodenal perforation with extensive peritonitis
Postoperatively, on parenteral nutrition along with antibiotic therapy of ceftriaxone 2g+metronidazole 500mg /6q a day
Patient initially improves but on day 9 post-op, recurrence of fever despite antibiotic therapy
ESBL+ K. pneumoniae were isolated
Ertapenem Imipenem

Intra-abdominal infection is still a major cause of morbidity and mortality
Principles of management of intra-abdominal infections include adequate surgical procedures as well as antimicrobial therapy
Due to the increasing prevalence of antibiotic-resistant strains of bacteria, it is important to understand
- the role of antibiotics in leading to resistance
- the potential of more judicious antibiotic usage in minimizing resistance selection and colonization
Summary

INVANZTM† (ertapenem) and TIENAMTM† (imipenem) in general share the similar properties of carbapenems with broad-spectrum coverage and excellent clinical efficacy*
INVANZ and TIENAM have demonstrated a low risk for resistance selection
Each agent is well suited for different patient types- INVANZ for the treatment of complicated intra-abdominal
infections associated with secondary peritonitis with or without abscess formation
- TIENAM for the treatment of postoperative peritonitis, tertiary peritonitis and complicated pancreatitis
Ongoing surveillance study: SMART**
*Ertapenem has minimal activity against non-fermentative gram-negative bacilli**Study for Monitoring Antimicrobial Resistance Trends †Trademarks of Merck & Co., Inc., Whitehouse Station, NJ, USA
Summary (cont’d)

References1. Solomkin JS et al, for the Protocol 017 Study Group. Ertapenem versus piperacillin/tazobactam in the treatment of complicated intraabdominal
infections: Results of a double-blind, randomized comparative phase III trial. Ann Surg 2003;237:235–245.2. Yellin AE et al. Ertapenem monotherapy versus combination therapy with ceftriaxone plus metronidazole for treatment of complicated intra-
abdominal infections in adults. Int J Antimicrob Agents 2002;20:165–173.3. Fry DE. Basic aspects of and general problems in surgical infections. Surg Infect 2001;2(Suppl 1):S3–S11.4. Pacelli F et al. Prognosis in intra-abdominal infections: Multivariate analysis on 604 patients. Arch Surg 1996;131:641–645.5. Gerth WC et al. Economic considerations when choosing parenteral antibiotic treatment for complicated community-acquired intra-abdominal
infections. EJHP 2004;4:78–83.6. Mazuski JE et al. The Surgical Infection Society guidelines on antimicrobial therapy for intra-abdominal infections: Evidence for the
recommendations. Surg Infect 2002;3:175–233.7. Onderdonk AB et al. Microbial synergy in experimental intra-abdominal abscess. Infect Immun 1976;13:22–26.8. Solomkin JS et al. Guidelines for the selection of anti-infective agents for complicated intra-abdominal infections. Clin Infect DIs 2003;37:997–
1005.9. Mazuski JE et al. The Surgical Infection Society guidelines on antimicrobial therapy for intra-abdominal infections: An executive summary. Surg
Infect 2002;3:161–173.10. Cattan P et al. Outcomes of empiric antibiotic therapy for hospitalized patients with community-acquired intra-abdominal infection. Presented
at the 11th Annual European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), Istanbul, Turkey; 2001.11. Rodriguez-Bano J et al. Epidemiology and clinical features of infections caused by extended-spectrum beta-lactamase-producing Escherichia
coli in nonhospitalized patients. J Clin Microbiol 2004;42:1089–1094.12. Paterson DL et al. International prospective study of Klebsiella pneumoniae bacteremia: Implications of extended-spectrum ß-lactamase
production in nosocomial infections. Ann Intern Med 2004;140:26–32.13. Paterson DL et al. Outcome of cephalosporin treatment for serious infections due to apparently susceptible organisms producing extended-
spectrum beta-lactamases: Implications for the clinical microbiology laboratory. J Clin Microbiol 2001;39:2206–2212.14. Paterson DL. Recommendations for treatment of severe infections caused by Enterobacteriaceae producing extended-spectrum beta-
lactamases (ESBLs). Clin Microbiol Infect 2000;6:460–463.15. Paterson DL et al. Epidemiology of ciprofloxacin resistance and its relationship to extended-spectrum ß-lactamase production in Klebsiella
pneumoniae isolates causing bacteremia. Clin Infect Dis 2000;30:473–478.16. Oh H, Edlund C. Mechanism of quinolone resistance in anaerobic bacteria. Clin Microbiol Infect 2003;9:512–517.17. Elsaghier AAF et al. Bacteraemia due to Bacteroides fragilis with reduced susceptibility to metronidazole. J Antimicrob Chemother
2003;51:1436–1437.18. Moellering RC. Principles of anti-infective therapy. In: GL Mandell, JE Bennett, R Dolin, eds. Principles and Practice of Infectious Diseases. 5th
ed., Churchill Livingstone, Philadelphia, PA, 2000, pp. 223–235.19. Raymond DP et al. Preventing antimicrobial-resistant bacterial infections in surgical patients. Surg Infect 2002;3(4):375–385.20. Davey P et al. How important is appropriate empirical antibiotic treatment for intra-abdominal infections? Presented at the International
Society of Pharmacoeconomics and Outcomes Research (ISPOR) Sixth Annual International Meeting; Virginia, USA, 2001.21. Bare M et al. Excess mortality associated with inappropriate initial empiric antibiotic therapy in patients undergoing surgery for intra-
abdominal infection. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), Milan, Italy; 2002.22. Burke J et al. Effect of adequate empiric antibiotic therapy on outcomes among patients with complicated intra-abdominal infections.
Presented at the 39th World Congress of Surgery, Brussels, Belgium; 2001.23. Sendt W et al. Association between inappropriate initial empiric antibiotic therapy and the need for reoperation and second-line therapy
among German patients undergoing surgery for community-acquired intra-abdominal infections. Presented at the 12th Annual European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), Milan, Italy; 2002.
24. Niederman MS. Appropriate use of antimicrobial agents: Challenges and strategies for improvement. Crit Care Med 2003;31:608–616.

25. Paterson DL. “Collateral damage” from cephalosporin or quinolone antibiotic therapy. Clin Infect Dis 2004;38(Suppl 4):S341–S345.
26. Carmeli Y et al. Antecedent treatment with different antibiotic agents as a risk factor for vancomycin-resistant Enterococcus. Emerg Infect Diseases 2002;8:802–807.
27. Landman D et al. Citywide clonal outbreak of multiresistant Acinetobacter baumannii and Pseudomonas aeruginosa in Brooklyn, NY. Arch Intern Med 2002;162:1515–1520.
28. Paterson DL et al. International prospective study of Klebsiella pneumoniae bacteremia: Implications of extended-spectrum beta-lactamase production in nosocomial infections. Ann Intern Med 2004;140:26–32.
29. Paterson DL et al. Epidemiology of ciprofloxacin resistance and its relationship to extended-spectrum beta-lactamase production in Klebsiella pneumoniae isolates causing bacteremia. Clin Infect Dis 2000;30;473–478.
30. Lautenbach E et al. Epidemiological investigation of fluoroquinolone resistance in infections due to extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae. Clin Infect Dis 2001;33:1288–1294.
31. Arpin C et al. Extended-spectrum ß-lactamase-producing Enterobacteriaceae in community and private health care center. Antimicrob Agents Chemother 2003;47:3506―3514.
32. Lautenbach E et al. Risk factors for fluoroquinolone resistance in nosocomial Escherichia coli and Klebsiella pneumoniae infections. Arch Intern Med 2002;162:2469–2477.
33. Paramythiotou E et al. Acquisition of multi-drug resistant Pseudomonas aeruginosa in patients in intensive care units: Role of antibiotics with antipseudomonal activity. Clin Infect Diseases 2004;38:670–677.
34. Trouillet JL et al. Pseudomonas aeruginosa ventilator-associated pneumonia: Comparison of episodes due to piperacillin-resistant versus piperacillin-susceptible organisms. Clin Infect Dis 2002;34:1047-1054.
35. Livermore DM et al. Properties and potential of ertapenem. J Antimicrob Chemother 2003;52:331–344.36. Shah PM, Isaacs RD. Ertapenem, the first of a new group of carbapenems. J Antimicrob Chemother 2003;52:538–542.37. Gold HS, Moellering RC. Antimicrobial drug resistance. N Engl J Med 1996;335:1445–1453.38. Fung-Tomc JC et al. Differences in the resistant variants of Enterobacter cloacae selected by extended-spectrum cephalosporins.
Antimicrob Agents Chemother 1996;40:1289―1293.39. Kohler J et al. In vitro activities of the potent, broad-spectrum carbapenem MK-0826 (L-749,345) against broad-spectrum beta-
lactamase- and extended spectrum beta-lactamase-producing Klebsiella pneumoniae and Escherichia coli clinical isolates. Antimicrob Agents Chemother 1999;43:1170–1176.
40. Dorso KL et al. In vitro killing of gram-negative enteric pathogens by ertapenem and other beta-lactams: Effect of inoculum size and serum. Presented at the 23rd International Congress of Chemotherapy (ICC), South Africa, 2003.
41. Karlowsky JA et al. Trends in antimicrobial susceptibilities among Enterobacteriaceae isolated from hospitalized patients in the United States from 1998 to 2001. Antimicrob Agents Chemother 2003;47:1672–1680.
42. Wenzel RP et al. In vitro susceptibilites of gram-negative bacteria isolated from hospitalized patients in four European countries, Canada, and the United States in 2000-2001 to expanded-spectrum cephalosporins and comparator antimicrobials: Implications for therapy. Antimicrob Agents Chemother 2003;47:3089–3098.
43. Livermore DM. The threat from the pink corner. Ann Med 2003;35(4):226–234.44. Friedland I et al. Presented at the 13th European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), Glasgow,
UK, May 10-13, 2003. Poster #789.45. Friedland I et al. 3rd International Meeting on Antimicrobial Chemotherapy in Clinical Practice (ACCP), Santa Margherita, Portofino,
Italy, October 16-19, 2003. Poster #30.46. Data on file, MSD .47. Roehrborn A et al. The microbiology of postoperative peritonitis. Clin Infect Dis 2001;33:1513–1519.48. Friedland I et al. Antimicrobial susceptibility in Enterobacteriaceae causing intraabdominal infections: Results from SMART in the
US and Asia, 2002. Presented at the 43rd ICAAC, Chicago, Illinois, 2003.
References

Copyright © 2004 Merck & Co., Inc., Whitehouse Station, NJ, USA. All rights reserved.
8-05 INV 2004-W-6307-SS
Please Consult the Summary of Product Characteristics
before Prescribing











![Efficacy of ceftazidime-avibactam in a rat intra-abdominal ...eprints.whiterose.ac.uk/131151/3/Sleger 2018 submitted version.pdf · 55 070], Interscience Conference of Antimicrobial](https://img.pdfslide.us/doc/110x75/5fd968a58b919d5c4256c8ae/efficacy-of-ceftazidime-avibactam-in-a-rat-intra-abdominal-2018-submitted-versionpdf.jpg)