Embed Size (px)
Citation preview

Henry H Rowshan, DDS, * Mary A. Parham, DVM, t
Dale A. Baur, DDS, MD,! RaeLynn D. McEntee, BBA,.f
Eugene Cauley, fI Dane T Carriere, IIJoseph C Wood, PhD, MD,#
William J Demsar, DMD, MS, **Jose M Pizarro, MS, PhDtt
Effect of Intermittent SystemicAdministration of RecombinantParathyroid Hormone (1-34) on
Mandibular Fracture Healing in Rats
Purpose: To establish a rat mandibular fracture model and investigate the short- and long-term effectsof recombinant parathyroid hormone (PTH 1-34) on mandibular fracture healing in rats.
Materials and Methods: A controlled unilateral mandibular fracture was created surgically in 29 maleSprague-Dawley rats and then stabilized using an external fixation device. The rats were divided into 2groups: 1 group received daily subcutaneous injections of 10 JLg/kg of PTH(l-34) and 1 group served asthe vehicle controL The rats were killed on postoperative days 7 and 21, and radiographic densitometryand histologic evaluation of new bone formation were performed.
Results: A novel unilateral mandibular fracture model was established that has significant differencesfrom preViously published models, both in the location of the osteotomy site and in the rigid externalstabilization device. The PTH(l-34) treated rats showed a statistically significant difference (P < .05) incallous formation compared with the control animals. Radiographic densitometry evaluation of the injurysite revealed an increase in bone denSity, apparent at day 7 in the experimental group. Visual inspectionof the histologic sections stained with Masson's trichrome blue showed an apparent increase in newbone formation at 21 days in the PTH·treated group compared with the control group.
Conclusions: Intermittent systemic administration of PTH(l-34) might enhance the healing of mandibularfractures in the early phase (7-day period). Long-term administration (21-day period) showed no statisticallysignificant differences between the control and experimental group by radiographic densitometry.© 2010 American Association of Oral and Maxillofacial Surgeons] Oral Maxillofac Surg 68:260-267, 2010
"'Chief of Oral and Maxillofacial Pathology, Department of Oral
and MaxillofJcial Surgery, Dwight David Eisenhower Army Medical
Center, Fort Gordon, GA.
ttOfficer in Charge, Department of Clinical Investigation,
DWight David Eisenhower Army Medical Center, Fort Gordon, GA.
This research was supported by internal funding from Southeast
Regional Dental Command and Dental Activity and Dwight David
Eisenhower Army Medical Center. The views of the authors do not
purport to reflect the position of the Depanment of the Anny or
Department of Defense (paragraph 4-3), AR 360-5.
Address correspondence and reprint requests to Dr Bam: De
partment of Oral and Maxillofacial Surgery, Case Western Reserve
Ulliversity!Univcrsiry Hospitals, 212; Abington Olive, Cleveland,
OH .+4106-490-;: e-mail: [email protected]
't' 2010 Amcric.on A'$'Xlotion of Oral ond .'\tIlJxillcfocio: Surge )ns
-' 0278·2391'10/6802{)()()5$36 00/0
doi: lO.1016/j.lom:;2009.09,045
260
:j::Assodate Professor and Chair, Department of Oral and Maxillo
facial Surge!)', Case Western Reserve University, Cleveland. OH.
§Research SpecialisL Department of Clinical Investigation,
Dwight David Eisenhower Anny Medical Center, Fon Gordon, GA.
llRq~istered Animal Technician, Department of Clinic;\l Investi
gation, D",.·ight David Eisenhower Army Medical Center. Fort Gor
don, GA.
IIResearch Specialist. Depanment of Clinical Investigation,
Dwight David Eisenhower ArnlY Medical Center. Fon Gordon, GA.
#Chief, Department of Clinical Investigation, DWight David
Eisenhower Army Medical Center. Fort Gordon. GA.
*Formerly, Chief ReSident, Department of Droll and Maxillofacial
Surgery, Dwight David Eisenhower Ann)' Medical Center, Fon
Gordon, GA; and Currently, Chief, Oral and Maxillofacial Surge!)',
Ft Irwin, CA.
tChief of Veterinary Medicine, Department of Clinical Investiga
tion, Dwight David Eisenhower Army Medical Center, Fort Gordon,
GA.

ROWSHAN ET AL
The mandible is rhe second most frequently fracturedcomponent of the facial skeleton. Hippocrates described the practice of bandaging fractures to stabilizebone segments to allow healing. I Twentieth centuryadvanced technology allowed surgeons to combinethe principles of immobilization first described byHippocrates with surgical placement of plates andscrews to treat a variety of mandible fractures. Animalmodels continue to aid in the clinical study of facialskeleton fractures. Many unilateral mandibular osteotomy models found in published studies involve per·forming the mandibular osteotomy immediately anterior to the first molar, immediately posterior to thelast molar, or between the second and third molars.l-~
Novel models using alternative locations are neededbecause of the high risk of damage to the tooth rootsand the subsequent increase in oral contamination.Other published techniques have involved a criticalsize defect, '5 which did not achieve the presentstudy's goal of simulating a displaced mandibular fracture requiring stabilization. Surgically created mandib·ular fractures that underwent distraction osteogenesishave been reported,<,·7 as have models in which noform of stabilization was used. A
•9 We used an osteot
omy model that completely transects the ramus fromthe sigmoid notch through the inferior border of themandible, followed by repair with a rigid fixationdevice that is secured by 2 screws on each side of theosteotomy site.
The treatment of the mandible fracture ranges frommaxiUomandibular fixation to open reduction withinternal fixation. Fracture healing is a complex andsequential process, regulated by multiple inflammatory, growth, and hormonal factors. 10-13 Currently, nopharmacologic adjuncts are available to enhance thehealing of mandibular fracnlres. In published orthopedic studies, systemic administration of parathyroidhormone (PTH) has demonstrated enhancement ofhealing in an extremity fracture model using rats I4
.1'5;
however, it should not be assumed that these resultswill apply to mandibular fractures, because the mandible differs significantly from long bones in terms ofdevelopment and force load. The mandible, similar tothe flat bones of the skull, develops primarilythrough the process of intramembranous ossifica·tion. In contrast, long bones develop by endochondral ossification. In addition, although the mandibleand long bones are subjected to the 3 differenttypes of strain (ie, compression, tension, andshear), the predominant force acting on the mandible during physiologic movement is shear, but thelong bones, particularly the femur and tibia (thebones evaluated by most of the studies to date), areprimarily subjected to compression forces. 1(,.17
PTH is an essential regulator of calcium and phosphate metabolism 1'5 bur has also been shown to have
261
anabolic and catabolic effeps on the skeleton. 18 Inrecent years, PTH has been approved for the treat·ment of osteoporosis, and its anabolic effect has beenstudied in clinical trials. Although recent studies onthe use of recombinant PTH (PTIl 1-34) have demonstrated a significant increase in bone denSity and areduction in skeletal fractures in postmenopausalwomen,19 it is not currently prescribed for fracturerepair. From the available data, reason exists to suspect its possible value in such areas. Current researchhas indicated that PTH enhances both caIlus formation and remodeling by stimulating the proliferationof osteoprogenitor cells, synthesis of bone matrixproteins, and osreoclastogenesis.1 4 In 1932, Selye de·termined that once-daily administration of PTH had ananabolic effect on the bones of rats, but larger dosesresulted in bone resorption. .It has since been shownthat intermittent administration increases bone deposition but that continuous administration actually decreases bone mass. This is likely a result of the difference in effects of intermittent versus continuousinfusion of PTH on osteogenesis and osteoclastic activity. Bone deposition occurs with both forms ofadministration; however, with continuous infusion,bone resorption offsets deposition,'l° Dobnig andTurner21 reported that intermittent administration ofPTH increased osteoblast numbers and activity, apparently owing to the activation of resting bone liningceUs to become osteoblasts. In vitro studies haveshown that transient exposure of osteoblasts to PTHstimulates their synthesis of collagen type I but thatcontinuous exposure inhibits its production. 22
.l3
Intermittent PTH also postpones osteoblast apoptosis24 but has no effect on osteoclast numbers.2"i Incontrast, sustained elevation had no effect on osteoblast apoptosis and actually increased osteoclastnumbers. 26 PTH also affects cortical and cancellousbone differently. It has a greater anabolic effect oncancellous bone than on cortical bone. 27 Variousstudies have indicated a greater effect on bonecontaining primarily red marrow compared withbone containing yellow marrow. 16 Intermittenttreatment with PTH has been shown to increasecallus formation and mechanical strength in experimental fracture healing. 1.f.UU8 A daily dose of 200J.Lg/kg was more effective in enhancing callus formation and mechanical strength than a dose of 60J.Lg/kg in rat tibial fractures. 2R Howeyer, irs efficacy,and optimal dosing in treating fractures of the mandible has not been researched. We developed awell-controlled mandible fracture model in rats andexamined the hypothesis that daily systemic admin·istration of PTH(l-34) could enhance mandibularfracture healing.

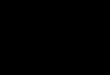
FIGURE 1. Open surgical creation of mandibular fracture that was then stabilized using external fixation device. A.B, Vertical platessurgically placed on mandible. C, Vertical osteotomy was created using sagittal saw. 0, Placement of insulin syringe barrE!l and impressionmaterial filling for plate stabilization (block arrow indicates osteotomy site). E, Wound closed, leaving external fixator device extendingbeyond incision.
ROlI's!:Jrll/ (If al. EJJects oj PTH /)1/ Malldil;ular Fracture HealiJlg. J Oral Maxil/oJae SIII,& 20 W.
262
Materials and Methods
SUBJECTS AND HOUSING
A total of 29 adult male Sprague-Dawley rats(weight 550 to 600 g) were pair-housed until surgerywith food (standard rat chow) and water ad libitum.The rats were kept on a 12-hour light/dark cycle(lights on from 8:00 AM to 8:00 PM). The InstitutionalAnimal Care and Use Committee reviewed and approved all procedures. Research was conducted incompliance with the Animal Welfare Act and otherfederal statutes and regulations relating to animals andexperiments and adhered to principles stated in theGuide for the Care and Use of Laboratory Animals,NRC Publication, edition 1996. Of the 29 rats, ISwere randomly assigned to the experimental group,receiving PTH injections, and 14 rats were assigned tothe control group.
PREPARATION AND ADMINISTRATION OF PTH
PTIi fragment 1-34 (Sigma Chemical, St Louis, MO)was suspended in 1% acidic acid and sterile water anddiluted accordingly to create a ID-/LglmL solution,follOWing the manufacturer's guidelines. The ratswere weighed and injected with 10 /Lglkg of PTIisubcutaneously once daily from the day of surgeryuntil death. The control group received no injections.
EFFECfS OF PTH ON MANDIBULAR FRACfURE HEALING
SURGICAL PROCEDURE
The rats were premedicated with subcutaneousbuprenorphine (0.02 to 0.04 mglkg), and then anesthesia was induced with a mixture of ketamine (80mglkg) and xylazine (4 mglkg), administered intraperitoneally. Anesthesia was maintained with 1% to2% isoflurane in oxygen administered by way of anose cone. No antibiotics were given to any ratsbefore surgery. The rats were placed in a supineposition under a surgical microscope (Carl Zeiss, Berlin, Germany). A 1· to 1. 5-cm incision was made alongthe inferior border of the right mandible. Sharp dissection was carried down to the periosteum throughthe body of the masseter muscle. Subperiosteal dissection w~s conducted in a superior and Iateml direc·tion to expose the sigmoid notch and posterior border of the mandible. Two 5.0-hole plates (OsteoMed,Addison, TX), were placed parallel to the osteotomy,one anterior and one posterior to the sigmoid notch,approximately 4 to 5 mm apan. The plates weresecured with 4, ;-mm·long, 1.8 mm diameter screws,and positioned such that the plates extended throughthe incision. Using a sagittal saw, a vertical osteotomywas created from the sigmoid notch to the inferiorborder of the mandible. The proximal and distal endsof the fractured mandible were then reapproximated

ROWSHAN IT AL
using the previously secured plates and held in position. A small portion of the barrel of an insulin syringewas split longitudinally along one side. positionedwith the ends of the 2 plates inserted into the barrelthrough the split, and filled with Fast Set (BlueMousse-Impression Material Parkell, Farmingdale, NY)
[0 provide rigid external fixation. The mandible wasthen manipulated to ensure that the 2 segments of theosteotomy were fixated securely (Figs lA-D).
POSTOPERATIVE CARE
The wound was then closed in layers around theprotmding ends of the plates (Fig IE). The rats wereallowed to recover, and buprenorphine at the preanesthetic dose was administered subcutaneously every8 to 12 hours for 48 hours for postoperative painmanagement. For the remainder of the experiment.the rats were housed separately and fed a soft diet.The rats were divided into 7- and 21-day groups receiving PTH(I-34) injections, as described previously.The rats were sacrificed on day 7 and 21, and themandibles were harvested and divided into the rightand left sides. The hardware was removed, and the
Control
263
riglu mandibles underwent r..ujiographic and histologic analysis.
RADIOGRAPHIC DE SITOMETRY ANALYSIS
The right fracture-bearing mandible was radiographed, and the digital images were analyzed withImage] (National Institutes of Health, Bethesda, MD)software. The images were inverted to measure darkness within the fracnrre site. The entire fracture sitefrom the inferior border of the mandible to the sigmoidnotch was outlined and the measurement obtained.Next, the filling of the fracture site representing callousfonnation was outlined and the measurement obtained.The fracture site measurement and the filling measurements were then expressed as a ratio to represent theamount of radiographic callous fonnation witltin thefracture site (Fig 2). All sections were analyzed by 2observers who were unaware of which group was beingmeasured.
HISTOLOGIC PREPARATION AND EXAMINATION
The tissues were fixated in 10% buffered formalinsolution, decalcified using standard procedures, and
PTH(1-34)
7 days
21 days
FIGURE 2. Radiographic images of control at A, 7 days and C, 21 doys and PTH-treated groups 01 B, 7 days and 0, 21 dayspostoperatively. PTH-treoted group showed enhanced bone density 01 7 days followed by a decrease of bone density at 21 days aftersurgery.
RO/l's!:Jall et al. Effects of PTH Oil Jlalldiblllar Fracture Healing J Oral ,11axi!/o/ac Slll:~ .lOlO.

21
Control
c:=lPTH (10uglkg)
n=6
Days
PTH
•n=7
n=8
EFFECTS OF PTH ON MANDIBULAR FRACTURE HEALING
120
o
140
~ 100
~ 80•oe. 60o~ 40
20
Digital photographic analysis was used to determine the radiographic densitometry in the fracturesite at 7 and 21 days postoperatively. Densitometricanalysis of the fracture site showed significant differences between the PTH(I-34)-treated and control ratsat 7 days postoperatively (Figs 2, 4). The PTH(1-34)treated rats showed a statistically significant difference in callous formation compared with the controlrats. Two-way analysis of variance showed a statistically significant interaction between 7 and 21 daygroups and treatment (P < .05). The increase in
RADIOGRAPHIC DENSITOMETRY FINDINGS
FIGURE 4. Histograms representing bone densitometric analysisof PTH( 1-34)-treated and control group at 7 and 21 days postoperatively. Optical density measurements were obtained by tracinginjury site and normalized using area (density/area). Significantincrease seen (P < .05) in bone density in PTH-treated rats compared with controls at day 7. Data shown as mean ratio:!: standard error of mean.
ROlI'S/)(/1/ et at. l:.Jjects oj PTH 011 Mandibular Fracture Heatingj Om/ Maxi//ojac SurJ: 2010.
Control
21 days
264
We established a mandibular fracture model using atechnique that involved placement of the osteotomysite caudal to the molars to avoid damaging the toothroots during the procedure. Also, the fracture wasstabilized using an external fixation device anchoredby 2 screws on either side of the fracture site formaximum stabilization. Finally, a nonadjustable fixator was used to stabilize the osteotomy site (FigslA-E).
FIGURE 3. Histologic evaluation of specimens showing fractured healing differences in PTH-trealed and control groups at 21 days aftersurgery. Sections stained with Masson's trichrome blue 10 stain for collagen formation within osteotomy site. LiHle bone development se~n !ncallus of control group, as denoted by band of light blue collagen. PTH-treated groups, however, showed abundance of bone withinosteotomy site (dark blue; original magnification x60).
Rowshcm et af. Effects of PTH 011 Mandibular Fracture Healing. J Oral Maxillofac Surf!, 20JO.
Results
MANDIBULAR FRACTURE MODEL
The data were analyzed using statistical analysiscomputer software (SigmaStat, version 3.0, SigmaPlot,Point Richmond, CA). The 2-way analysis of variancemethod was used to compare the radiographic measurements between the control and PTH-treated fracture groups. The data are presented as the mean :t
standard error of the mean. The measurements werecompared, and P less than .05 was chosen as thecritical level of statistical significance.
embedded in paraffin wax. Serial, 4-/Lm-thick sectionsof the entire osteotomized right mandibles were cutparallel to the long axis of the osteotomy site. Thesections were stained with Masson's trichrome blueto stain for collagen formation within the osteotomysite. Light microscopic examination was performed atlOX and 6ox. Digital photographs were taken andexamined using Image] (National Institutes of Health)software program. The fracture sites were examinedfor collagen material filling and new bone formation(Fig 3).
STATISTICAL ANALYSIS

ROWSHAN IT AL
radiographic densitometry was evident in the earlyphase (7 days) of fracrure healing; however, as shownin Figure 4, a decrease in optical densiry had occurredat 21 days after surgery. Moreover, these differencesbetween the control and treated rats on day 21 didnot reach statistical significance.
HISTOLOGIC EXAMINATION FINDINGS
The effects of PTH(l-3~) treatment were examinedusing light microscopy at lOX to 60x magnificationand the Image] digital photographic analysis softwareprogram (Fig 3). Visual inspection of the histologicsections stained with Masson's trichrome blueshowed a general [feod in the collagen deposition andvoid filling in the early 7- and 21-day PTH-treatedexperimental group. Masson's trichrome blue stainsdark blue for old bone and light blue for collagen andnew bone formation. This finding was consistent inthe early ;-day group and 21-day experimental group.Also, subjective evaluation of the slides showed anapparent trend toward increased new bone fOffilationin the osteotomy site in the 2 I-day PTH-treated groupcompared with the 21-dar controls.
Discussion
Postfracture bone healing is a complex processinfluenced by many molecular, cellular. and biomechanical factors. 10.1 I Recent studies have been conducted to evaluate the effect of several biologic substances on bone fracture healing, induding bonemorphogenetic protein, transforming growth factor-f3. platelet-derived growth factor. and vascular endothelial growth factor. 29-3 I A systemically administered medication that enhances fracture healing couldhave a dramatically positive effect on the clinicalmanagement of fracture treatment. To study novelpharmacologic adjuncts to enhance the healing ofmandibular fractures, we established a unique rodenthemimandibular fracture model. Our mandibular fracture model involved the placement of the osteotomysite caudal to the molars to avoid damaging the toothroots during the procedure. This technique variesconsiderably from previous studies that used a distraction technique to examine mandibular fractures. ~.-I..:U
The distraction method involved the creation of anosteotomy site that ran between the second and thirdmolars, and the fixation device was attached by implantation of one post on either side of the osteotomysite. TIle device was also designed to place graduallyincreasing distraction forces on the osteotomy site to
study the effects of such forces on fracture healing.Daily subcutaneous injections of PTH (l0 lLg/kg)
were used with our unique rodent mandibular fracture model as a pharmacologic adjunct to enhance thehealing of mandibular fractures. PTH is produced by
265
the chief cells of the parathyroid gland. It is an R4amino acid polypeptide that physiologically regulatesserum calcium and phosphate levels by increasingbone resorption. increasing gastrointestinal calciumabsorption. and increasing renal calcium and phosphate reabsorption.IK..\.\..\~ The continuous administration of PTH results in net bone resorption; however, intermittent administration causes a net increasein bone deposition.I~.IH.3(,Because of the very shorthalf-life of PTH, apprOXimately I hour in humans aftersubcutaneous injection. daily dosing such as was conducted in the present experiment would constituteintermittent administration ..\-;- Andreassen et al lR
showed that intermittent administration of high (200lLg/kg) doses of PTH( 1-3~) significantly increased fracture caUus fOffilation in a rat model. In addition,PTH(l-34) has been administered to patients withosteoporosis, with dosages of 10 to 40 ILg and hasbeen shown to effectively increase bone mass after a21-month clinical triai lO We chose the low IQ-ILg/kgdosage to avoid the side effects of high-dose administration of PTH, and because it is comparable to theproven clinical dose given for the treatment of osteoporosis. Additionally, Nakajima et all-i demonstratedthat dosages as low as 10 lLg/kg in a rat fracture modelincreased both mechanical strength and bone mass ofcallus formation in a rat femur fracture model.
In the present study, the radiographic densitometryanalysis results revealed that at 7 days after fracture,an increase occurred in callus and density in thePTH-treated group compared with the control group.However, although the optical denSity levels appeared to decline with time, the levels were notsignificantly different from those of the controls at 21days. Nakajima et al 14 showed that daily subcutaneousinjection of 10 lLg/kg of PTH(l-34) induced a significant increase in the osteoclast index in the hard callusand an increase in insulin-like growth factor-I, rype Icollagen (COLlAI), osteonectin, and osteacalcinmRNA expression at 7 days after a femoral fracture.These cellular and molecular events are perhaps indicative of the enhancement of fracture healing usinglow-dose PTH(l-34) during the early stages of femoralbone healing. Our data have also indicated thatPTH(l-34) has enhancement properties in the earlystages of mandibular fracture healing. At days 14 and21, Nakajima et a1 14 observed mature trabeculae inthe PTH·treated group but no significant difference inthe osteoclast index. Although in their study they didnot meaSllre the bone mineral density at 21 days, theyclearly showed a significant increase at 28 and 42 daysafter femoral fracture. In our study, we found a decrease-although not significant-in the radiographicoptical density in the PTH·treated rats compared withthe control group. l1lis is consistent with the findingof Alkhiary et aI, I' in which they compared the effect

I!
II
266
of PTH(l·:'-i) daily suhcutaneous injections un femordl bone fracture healing. The)' found that at 21 daysafter fracture, the animals treated with the lower doseof 5 fLg/kg PTH(l-34) did not show any differences inbone mineral density compared with the control animals. However, they observed a significant differencein bone mineral density with the lower dose at 35days after fracture.
Visual inspection of the histOlogic sections stainedwith Masson's trichrome blue also suggested that administration of PTH might playa role in overall cartilage remodeling and bone formatioo. Even at a lowdosage of 10 fLg/kg, these histOlogic sections showeda general trend in collagen deposition and void fillingin the PTH-treated group. On visual inspection at 60Xmagnification, a trend also appeared toward an increase in bone fill in the PTH group compared withthe controls at 21 days. In our study, subjective analysis of the 21-day PTH-treated group displayed anincrease in staining and callus maturity comparedwith the control group.
In conclusion, we were able to show evidence thata low dosage of PTH administration might enhancethe healing process in the early phase of a mandibularfracture model in rats. Although low-dose PTH administration showed evidence of enhanced bone healing,additional studies are needed to quantify these results.In addition, additional research is needed to determine the parathyroid hormone receptor activitywithin the bone after fracture to establish the optimaltime of drug administration in rdation to the fracturehealing mechanism. Furthermore, the effects of different dosages of PTH on our fracture model shouldbe examined at different intervals. Biomechankal testing to evaluate the strength of the callus formation isan an~a of future intt'rest. These tests might prove thatPTH is the first systemic drug to enhance the fracturerepair of patients with mandible fracture.
A ck110ll 'IedgIllel1t
The l"ditoriaJ assis!ancl" of N:lznn'n S. Kaka is gn.·atly apprt.:l:i·atnl.
References,1:UlH:S IUl. Frl"dricksOll C. Kl"nt .IN: Prospl'etin' stlld~- of mandihul:lr fr:lCtun.::' . .I Or:ll Surg :\9:2""'''. Il.JH I
1. Cll11pbi P. HanH..Iy He. Lallzicr D. et al: Expres:-.ioll of honemllrpJltJ~L'nctk pnJteins ullring mandihul:lr di~lr;ll'tiun IlsteogL·nt·sis. Plast HI'Ulllstr S\,r~ 111:201. 2(}(1.-\
.'\. Howe Ni\l. .\khr:lr:l I~J. Dudziak ;\IE. t·t aJ: R:H mandihulartlistr.lL·tion l):->tl'l)gelll..:sb. Pan I. IlistoJo~ic anti r.lllill~raphk
allal~-sis. Plast RI..:L·oll:-.tr Surg 102:2022. 19l.JH-L Stdnhrt:l.."h DS . .\khrar:l B.I. Hm\"(,' ~.\1. et al: Gelw L·xpre.;sion of
T{ir-ht·t;l. T(iF-heta rl·(:t.:ptor. :lIld extran:J111lar matrix pmtt·in....duril1~ IlH::mhrallou:-. honl" hl'aling in rats. PJast Ikl'onstr :-iurg10":2021{.200t)
;. Am:-ill"ena OA. Collin ... \\'1..: Ddel."t n:pair in the r.1I mandihlL'with hol1t:: lllorphogcnk protdn " :l1lU prost:lgl:llldin E I . ArchOlolaryngol Hcatl Ned.: Surg 12l): 112':,. 200:'!
EFFECTS OF PTH ON MANDIBULAR FRACTURE HEALING
6. E....ki 1\1. Nbanci .\1. Cil Y. l't a[: A l.."ll:,(ulll-madt' di:-tractiolldl.·vin: fur cxpcrimt·nt;ll mam..lihul;lr distr.ll'tion oSleogcllt:sis. JCmniofac Surg 16:6-". 200')
- Buchman SH. 19ndzi MAJr. Radu C, (.'( al: Uniqut: rodent modt:!of distraction osteiJgcne~is of Ihe: mandihle:. Ann Plast Surg-t9:511. 2002
R. Fukunaga T. Yamashiro T. Ora S, et <II: Connec(i"e: tissuegrowlh facwr mRNA expression pattern in canilage:s is assod·ated with thdr type I collagen expression. Bone 33:911. 2003
9. Zheng L Yamashiro T. Fukunaga T, et al: Bone morphogeneticprotein 3 expression patlem in rat condylar cartilage, femoralcanilage and mandibular fracture callus. Eur J OraJ Sci 113:,31 B.2005
1O. Childs SG: Stimulator~ of bone healing: Biologic and biOOll:chanica I. Onhop Nllrs 22:421. 2003
11. Ordfo RO: Growth factors for skeletal reconstruction andfraClure repair. Curl' Opin Invt'stig Drugs 5:419. 200-1
12. Bolander ME: Regulation of fmcture re:pair br growth faclors.Proc Soc Exp Bioi Med 200: 165. 1992
1:\. Chapman MW: Thol\ght~on clinical tri:tls to e:valu:lle the actionand dft:ctivt:ne:ss of BMPs in hone healing. J Bone Joint 5urgAm H:\A(Suppl. 1):SI6:\. 2UOI
14. Nakajima A. Shimoji N. Shiomi K. e[ al: Ml:ch:lllisll1s for tIll:enhanceml:nt of fracture hc:aling in rats tre:Hed with intermittent low-dose human parmhyroid hormone (1-:\4). .I BoneMiner Res 17:2038. 2<X12
1'). Alkhiarr YM. (ierstenfdd LC, KrJIJ E. l't al: Enh:mcemt:nt ofe:xrx:rimt:l1Ial franurc·he:lling hy systemic :ldministr.ttion ofrecomhinant human parathyroid hormone (PTH 1-:\-0. .J BoneJoint Slirg Am H"':7:\I, 200')
16. Rudman KE. kspde:n RM. Meakin .IR: Compre:ssion or tension?'nle stress distrihution in the: pmximal femur. Bionled Eng(}nlim: 5: 12. 2006
17. vall Eijden TM: Biol1le:dlar1ics of the mandible. Cdt Rev OralBioI Meu I I: 11:\. 200t)
IH. Holzer G. Majeska HJ, Llinur MW. et al: ParJthrroid hormoneenhanet:s fracture healing: A prdiminarr rc:pon. Clin OrthopRd:u Rcs 25H. 1999
19. Ne:e:r RM. Amalld CD, Zanchetta JR, e( al: Effh.1 of parathyroidhomlOne (l.:\-i) on tbCHlre~and hone mincr.J.l dcn~i(r in postOleno·pallSLI womell with osteoporosis. N EnglJ l\-kd :\-i-4:1-t3-t. 200l
20, Seehach C. Skripitl. R. Andreassen n', t:t al: Intemliut:l1t par.lthyroid honllont" (1-_'\4) t'nhanct:s me:chankal strength anddcnsity of llCW hont: after distraction ostt'ogenesis in rals.J Ortllop Res 22:-i72. 200..
2 J. Dohnig Ii, Turner RT: Evidence thal imemliUem lrt:atmt:l1Iwith par.lthrroid hormollc increast:s bone formation in adultr.HS hy anh'alion of honc lining n·lls. Endocrinology J:\6::\6:\2.Il)l)')
22. Canalis E. Centrdla M. I3un:h W. et al: Immlin-Iike growthfactor I mediates Sdeeti"e: :ll1aholic effects of par:uhrrokl llormone in hont: Cl1ltllrL's. .J Clin Invcst H5:60. 19H9
25. C:lllalis E. P:lsh J. Var~hest: S: Skektal growth factors. Cril RL'"Eukaryot (i(".'111;" Expr .1:1')';.199.1
2-i. Jilk:l RI.. \Vt.:instdn RS. Bdlido T. t:t :II: Increasl'U hOI1t' forma·tion h~' prevention of ostl.'ohlast apopwsis wilh parathyroidIHlfllml1c. .J elin Inn:st 1O-i: ... 5l). 1999
2". Hdlido T. Ali AA. Plotkin L1. t:t al: Proteasom:ll ul'graU:lIion ofHUllX2 shortens pa['atlJ~T(Jid hllrllllllle-induccd anti-:lpl)pltJticsiWlaling in ostl'oblasts: A put:lti\,e explanation for wily inttTlllith:nt :llJministr.nion is nn·uL·d for hone anaholislll . .1 RiolChem TH:')02:'i9. 200.~
26. Skripitz H. :\.spl·nlX'r~ P: Par:lIh~ mid homlOlll:-A drug forllnhopl'llic surgery~ Acta Onlwp Scam! -':;:6"-i. 200-1
r Billlkb RJ Dempslt"r .lA. R:ll1lakers PI.. t't al: Effect of proteinkin;lst: (: :Kti"ati(lll ;lntl dllwnregulatitJll on :It"tin: t':llcilllllIf'Jnspon. Kidnt'Y 1m -i5:2l)". \l)95
2H. Amlre;l:,sen rL EjeNnl C. Oxlund H: Intermittent paralhyroidhormone (I·.~-t) treltmenl increasL's call1l-'' forlllation and me·d1:ll1ical strt·ngth of healing rat fraullre~. .J BOlle Mint:r Hes10-1:960. 1999
2l). Ah(: N. Lee YP. Saw.\1. t:t al: Enhaneelllcnt of hone repair witha he1rx:r-ucpl.·ndent adl'nm'ir:11 trJllsft:r of h()J1e llll)rphogem:tic.:prllteill·2. Bioc1wm Biophrs Hes Commun 29::-;2.~. 2002

ROWSI-lAN ET AL
.~(). Yogdin .\!DE. .rOlH:S NF. Lieberman JR. et at: Prdahrication ofbOlle by usc of a \";lscularizl·d periosteal tlap and hone morphogenetic protein. Plas! Ik<.:onstf Surg Itl'-}:ll)O. 2002
:i I Lieherman JR. Daluiski A. Einhorn Tr\: The rok of growthfactors in the n:pair of hone: lIiology and clinical applications,J BOll<: J()int Surg Am H-iA:I0:'2. 20()2
~2 \'"illiams.lK. Rowe N.\-I, .\lackooj R). et al: Controlled l11ultipJaoar di.o;traction of the mandible. Part II: Laboratory studies ofsagittal (;.lIltcroposterior) and vertical (superoinferior) movements. ] Craniofac Surg 9:'504, 1998
~.3 Habener JF. Kronenberg H.\1: Parathyroid hormone biosynthesis: Structure and function of biosynthetic precursors. Fed Procr:2.,61, 19-H
26
.3-1. Hdnrich G, Kronenberg t-1i\L Polts .IT .Jr. l't al: Pamth' .hormone messenger rihonlll:!l'ie add' Fffcct. r ,'.} fOUj. _ . ., .' . .'"' ." s () ca ('nml on
(dlul.lr .1t.:gl~.LI.IIOI~ In \ 1110, EndolTllhllogy 1 12: 1-.i9. 1<)83
y; H~ISk.a KA. Ll\"I{c~ It DUIlCU1 H: ct al: H('guJation of skdctal rl'lllod_dmg by 11;U~lthyrold hOnllOne, Contnh Ncphrol <)1..~K. 1')l->1
."!(J. Sllirot;l T: Tashiro M. ()h~o K. ct al: Effl'ct ut intermittentparathyrOId hon1H~ne (1"5-1) treatmcnt on thc bonc rl':-,pOl1seafter placement ot titanium implants into the tibia uf O\"ariec.wmized rats. J Oral ,\laxillufac Surg 6l:-i~1. 2()D."!
37. Schwif;'ren HR. Groen EW. Sollie FA. l't al: Single-dose subcutaneOllS administration of recombinant human parathyroid hormone [rhPTH(l-84)] in healthy postmenopausal volunteersClin Pharmacol Ther 61 :.160. 1997
Ii
!
I
il
fli.1I'·,1itIIiI
i


![Case Report Treatment of Fracture Sequel in the Mandibular …downloads.hindawi.com/journals/cris/2019/4627301.pdf · 2019-07-30 · of mandibular fractures [4], agreeing with the](https://img.pdfslide.us/doc/110x75/5f481aad7067477107549e69/case-report-treatment-of-fracture-sequel-in-the-mandibular-2019-07-30-of-mandibular.jpg)