Embed Size (px)
Citation preview

Effect of Temperature in Focal Ischemia of Rat Brain Studied by 31P and 'H Spectroscopic Imaging Piotr Kozlowski, Alastair M. Buchan, Ursula I. Tuor, Dong Xue, Zhi-Gao Huang, Karen E. Chaundy, John K. Saunders
3'P, 'H and lactate spectroscopic imaging was used to eval- uate the effects of hypothermia on focal cerebral ischemia produced by middle cerebral artery occlusion. The effects on high energy phosphate metabolism, pH, lactate and NAA were investigated in 24 spontaneously hypertensive rats subjected to either permanent or transient ischemia. Under either nor- mothermic (375°C) or hypothermic (32°C) conditions, with permanent 6-h occlusion, there was little difference between groups in either the NMR measurements or the volume of infarction. In animals that underwent 3 h of ischemia followed by 12 h of reperfusion, the ischemic changes in lactate, pH, NAA, and high-energy phosphate returned toward control val- ues, and there was a protective effect of hypothermia (infarct volume of 211 2 26 and 40 2 14 mm3 in normothermic and hypothermic groups, respectively). Thus, hypothermia did not ameliorate the changes in lactate, pH, NAA, or high energy phosphate levels occurring during ischemia, however, during reperfusion there was an improvement in both the recovery of these metabolites and pathological outcome in hypothermic compared with normothermic animals. Key words: hypothermia; focal cerebral ischemia; rat model; spectroscopic imaging.
INTRODUCTION
It is well established that hypothermia during an episode of cerebral ischemia provides protection against brain damage (1-5). However, details of the mechanisms in- volved in this protection and the metabolic indicators of poor outcome resulting from an episode of cerebral isch- emia remain poorly defined. Reduced energy require- ments, reduced lactate formation, and less profound ac- idosis are among some of the factors that have been proposed to contribute to the improved outcome associ- ated with hypothermia (1). Indeed, a delay in the deple- tion of adenosine triphosphate (ATP) and an improved recovery of high-energy metabolites and pH have been observed in animals that undergo cerebral ischemia un-
MRM 37346-354 (1997) From the Institute for Biodiagnostics. National Research Council, Winnipeg, Manitoba, Canada (P.K., U.I.T., J.K.S.) and University of Ottawa, Ontario, Canada (A.M.B., D.X., Z-G.H.. K.E.C.). Address correspondence to: Piotr Kozlowski, Ph.D., National Research Council, Institute for Biodiagnostics, NMR Technology Group, 435 Ellice Avenue, Winnipeg, Manitoba, R36 1Y6 Canada. Received November 14, 1995; revised July 8, 1996; accepted August 30, 1996. Part of this work was presented at the 1 l t h Annual Meeting of SMRM in Berlin in August 1992.
Copyright 0 1997 by Williams 8 Wilkins All rights of reproduction in any form reserved.
0740-3194/97 $3.00
der hypothermic rather than normothermic conditions (1, 6-91, but how they directly relate to protection of the brain is not always clear as pathological outcome is not always determined. In addition, the effect of hypother- mia on the changes in other metabolites such as lactate and NAA has been less extensively studied, particularly during focal ischemia with reperfusion.One problem with measuring metabolite levels in focal ischemia is localizing the measurement within the ischemic area. In early studies of cerebral ischemia in animal models, sur- face coils have been used to localize the phosphorous or proton magnetic resonance spectra (10-12). More re- cently spectroscopic imaging has been used as a local- ization method to acquire either 'H or 31P h4R spectra in humans and animals following stroke (13-16). One study has reported the application of both 'H and '"P spectro- scopic imaging to evaluate the effects of regional brain injury after ischemia (17). In the present study we use both 'H and 31P spectroscopic imaging techniques (18, 19) to evaluate the effect of temperature on cerebral me- tabolite changes that occur during or after focal cerebral ischemia in rats.
MATERIALS AND METHODS Animal Preparation
Focal ischemia was induced in 24 fasted male spontane- ously hypertensive rats as described in detail previously (20). Animals were anesthetized with halothane ( 3 4 % for induction, 1 . 5 4 % for maintenance), intubated, and attached to a rodent ventilator. The femoral artery was cannulated, and ventilation was adjusted such that arte- rial PCO, was between 35-40 mmHg. The body temper- ature of the rat was monitored with a rectal probe and temperature was controlled with a water blanket. The right common carotid artery was surgically exposed and occluded. A 1- to 2-cm skin incision was made at a location between the right eye and right ear exposing the temporalis muscle. Under a dissecting microscope the right middle cerebral artery (MCA) was exposed through a 2-mm burr hole drilled 2-3 mm rostal to the fusion of the zygomatic arch with the squamosal bone. The dura was retracted and the MCA was occluded with a 1-mm Codman aneurysm microclip.To observe the effect of both ischemia and reperfusion, rats were divided into two groups: transient ischemia and permanent ischemia. For the permanent ischemia group, both the right com- mon carotid and right MCA were permanently occluded and animals were immediately placed in the magnet. For
346

Effect of Temperuture in Focal Ischemia 347
the transient ischemia group, the right common carotid was permanently occluded and the right MCA was tran- siently occluded for 3 h, during which the animals were allowed to recover from anesthesia. The animals were re-anesthetized and placed in the magnet immediately after the microclip was removed and reperfusion estab- lished. The time between the clip removal and the start of the first spectroscopic imaging experiment was typically 20-30 min.To evaluate the effect of temperature, both groups were examined at two temperatures [six rats/ group): 37.5OC (N - normothermic) and 32°C (H - hypo- thermic). For the transient hypothermic group the tem- perature was kept at 32°C (31-32.5"c) throughout the ischemic period, while during reperfusion temperature was maintained at 37.5"C (37-38OC). For the permanent hypothermic group the temperature was maintained at 32°C (31-32.5OC) throughout the entire experiment.Six rats were studied in each group, resulting in a total of 24 animals. During hypothermia, temperature was main- tained between 31OC and 32.5OC. In additional experi- ments (data not shown), rectal temperature was com- pared with the tympanic temperature and the difference between the two was less than 1°C when the animal's
temperature was varied between 30-37°C during isch- emia and reperfusion.
MR Experiments
A detailed description of the NMR experiments has been presented elsewhere (21). The rats were positioned in a stereotactic cradle fixed in the magnet with small pins. Two separate RF coils identical in size and shape were used to acquire the 'H and "P NMR signal. Both coils were inductively coupled elliptical surface coils of 16 mm length and 14 mrn width, and were mounted on the animal holder with nylon screws to ensure that the po- sition for both coils was the same. Switching of the coils was performed between experiments and typically took 3-5 min, including repositioning of the animal in the magnet.Experiments were performed on a 4.7 T/30 cm Bruker system. Two dimensional (2D) spectroscopic im- aging was used to acquire localized spectra in the coronal plane ( X , 2') with a field of view of 4 cm in each direction. The localization in the Y direction was achieved by depth pulse slice selection with a slice thickness of 3.5 mm resulting in a voxel size of 2.5 X 2.5 X3.5 mm ('H spectra), 2.5 X 2.5 X 1.6 mm (lactate spectra) and 5 X 5 x
control
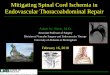
FIG. 1 . Positions of the voxels used to obtain information from 'H, lactate, and 31P spectroscopic images. Ratio of t h e right (ischemic) to the left (control) side was calculated to evaluate high energy phosphates and NAA levels. Lactate levels on the ischemic and control side were normalized to the NAA levels on the control side. Figure also shows typical 31P, 'H, and lactate spectra acquired from ischemic and control sides of the brain.

348 Kozlowski et al.
3.5 mm (31P spectra). The slice position was determined from high resolution images acquired with hard pulses. To assure the same slice thickness and slice position for 'H and 31P experiments, we used as a reference for either coil a 4-mm 0.d. glass sphere that was filled with a 0.5 M aqueous solution of phenyl phosphonic acid (PPA) and positioned in the plane of the coil. Using an MRI se- quence, the pulse angle at the position of the reference was adjusted to 180°, which resulted in the selected slice covering the external layers of the cortex. In the "P experiments the pulse length was also adjusted to 180" for the reference. The transmitter power level was kept at 500 W for both 'H and 31P frequencies, which resulted in pulse lengths of 8 ps for 'H experiments and 13 ps for 31P experiments. The pulse length adjustment was repeated for each animal; however, no variations in pulse lengths were observed.Two contralateral voxels (Fig. 1) were se- lected for data analysis to obtain semiquantitative infor- mation about changes in metabolites levels. The voxel positions were optimized to minimize partial volume effects.
Three types of experiments were performed. The first was a 'H spectroscopic imaging experiment that used a spin-locking water suppression sequence (18) with an echo time of 272 ms. The repetition time was 1200 ms and 8 averages per phase encoding step were performed, resulting in a total acquisition time of 55 min.The second experiment was a lactate spectroscopic image that was obtained by using a single-shot editing sequence (19) with the same echo time, repetition time, and total ac- quisition time as for the first experiment. Finally the third experiment was a j lP spectroscopic image acquired by using a spin-echo sequence with an echo time of 1 ms. Use of a repetition time of 1500 ms and acquisition of 64 averages per phase encoding step resulted in a total ac- quisition time of 1 h and 50 min. Actively shielded gradients with a 64-ps rise time were used for all exper- iments. No distortions in the spectra due to eddy currents were observed.
Rats that underwent permanent MCA occlusion stayed in the magnet for a period of 6 h. During this time five spectroscopic images were acquired in the following or- der: 'H. lactate, '"P, 'H, and an additional lactate spec- troscopic image. Animals from the transient ischemic groups stayed in the magnet for 12 h, during which time each of the spectroscopic images was acquired 3 times.
permanent occlusion
3wJ7
Histopathology
All animals were sacrificed at the end of the experiment. Brains were rapidly removed and frozen in isopentane which had been cooled to -80°C. Coronal sections (20 pm thick) were cut at -20°C, and every 25th section was fixed in 90% ethanol and stained with haematoxylin and eosin.Cerebra1 infarction was defined histologically as those areas that had sustained pannecrosis. The infarcted area of each section was traced by a technician blinded to the treatment using an image processing system (Image Pro 2, Media Cybernetics Inc., Silver Spring, MD). Total infarct volume was calculated by summing the infarcted area of sequential sections (20).
Data Analysis
All the data were processed by using specially developed software. Gaussian apodization with 500 Hz ("P) and 300 Hz ('H) was used in both spatial directions resulting in voxel broadening by 0.9 and 0.7 mm, respectively. In the spectral direction, line broadening of 40 Hz ("P) and 20 Hz ('H) was used.
The 3'P spectroscopic images were used to extract quantitative information about pH. inorganic phosphate (Pi) and the high energy phosphate levels in two con- tralateral voxels (Fig. 1). The pH was calculated from the difference in chemical shift between Pi and creatine phosphate (PCr) and corrected for brain temperature (22). 'H and lactate spectra from right (ischemic) and left (control) voxels were processed to obtain quantitative information about the changes in NAA and lactate levels. Levels of phosphorus metabolites and NAA are ex- pressed as a ratio of values in the right and left voxel. Lactate levels were normalized to the NAA levels on the control side of the brain.
The data are expressed as mean 5 standard deviation. One factor ANOVA was used to determine statistically significant differences between experimental groups and differences between means were assessed using a Scheffe multiple comparison of means.
RESULTS Histopathological Examination
Of the six rats that underwent transient ischemia under hypothermic conditions, one animal had a permanent
transient occlusion
I 3007 ** 1 -r 200.
,
100-
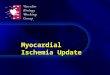
FIG. 2. Infarct volume measured from histopathological studies 6 h after permanent occlusion (left) and 12 h after reperfusion after 3 h of transient MCA occlusion (right). '*, hypothermic group significantly dif- ferent from normothermic group
normothemir hypDthermil
(P < 0.01).
1

Effect of Temperature in Focal Ischemia 349
permanent occlusion transient occlusion
7.50 7
H T 7.25
7.00
6.75 a
6.50
6.25
6.00
hypothetmia - ischemk
E hypothemis- control nonnothermia- ischemk
0 nmothennia- CMltrOl
3 time of occlusion [hrs]
3 7 1 1 time of reperfusion [hrsl
FIG. 3. Mean intracellular pH measured for ischemic and control sides of the brain during permanent ischemia (left) and reperfusion (right). 0, right side significantly different from the left side (P < 0.05); *, hypothermic group significantly different from the normothermic group (P < 0.05); H, hypothermic group: N, normothermic group.
occlusion despite removing the aneurysm clip.This ani- mal was therefore excluded from both histopathological and NMR analysis. In animals subjected to permanent ischemia, the volume of infarction was similar whether ischemia occurred under normothermic or hypothermic conditions (Fig. 2). In the transient ischemia group, the volume of infarction following 1 2 h of reperfusion ex- ceeded that at 6 h of permanent ischemia. Hypothermia during transient ischemia resulted in a marked 81% re- duction in infarct volume compared with animals which were normothermic (211 2 26 mm3 versus 40 t 14 mm3, P < 0.001).
PH
Intracellular pH was measured in ischemic and nonisch- emic tissue during permanent occlusion and during the reperfusion following 3 h of ischemia (Fig. 3). In perma- nent ischemia, both hypothermic and normothermic an- imals had pH values on the ischemic side of the brain which were lower than the control side (6.3 ? 0.1 versus 7.3 2 0.2, P < 0.05, for hypothermic group and 6.4 ? 0.1 versus 7.1 t 0.1 for normothermic animals). In the nor- mothermic group the inorganic phosphate on the control side was detectable only in two out of six animals. As a consequence, the pH value was determined in only two animals. Therefore the difference in pH between isch- emic and control side was not tested statistically for this group.
During transient ischemia, pH was measured at 3, 7, and 11 h after reperfusion. In the case of hypothermia, there was a relatively quick recovery of pH toward con- trol values as only the first pH value measured showed a significant difference between the ischemic (7.0 ? 0.1) and control (7.2 ? 0.1) side. The recovery of pH was slower for the normothermic animals. At 3 h of reperfu- sion, the normothermic animals had a pH value on the ischemic side, which was significantly lower (6.8 0.2) than that of the hypothermic group. In addition, both pH
values measured at 3 and 7 h of reperfusion were signif- icantly lower on the ischemic compared with the con- tralateral side (6.8 ? 0.2 versus 7.1 ? 0.1 and 6.9 ? 0.1 versus 7.1 5 0.1, respectively). The pH values for both normothermic and hypothermic animals recovered to a normal value at 11 h of the reperfusion (7.1 2 0.1 versus 7.2 ? 0.2 and 7.1 ? 0.2 versus 7.2 ? 0.1, respectively).
High Energy P h o s p h a t e s
Pi, phosphocreatine, and ATP measurements were ex- pressed as a ratio of right (ischemic) to left values (Figs. 4a-4c) and have a relatively large standard deviation due to a rather poor signal to noise ratio. Permanent occlu- sion resulted in elevated levels of inorganic phosphate (2.7 ? 1.5 for the hypothermic group and 8.7 2 6.2 for the normothermic group). Creatine phosphate levels were significantly lower on the ischemic side for both experi- mental groups (0.6 t 0.3 and 0.3 2 0.2 during hypother- mia and normothermia, respectively). Similarly, the ATP levels were reduced ipsilateral to the ischemia in both hypothermic and normothermic groups (0.8 ? 0.1 and 0.7 2 0.2, respectively). Although the hypothermic group tended to show less high energy failure than the normo- thermic group during permanent ischemia, this did not reach statistical significance.
During the reperfusion after 3 h ischemia, the hypo- thermic group had near normal levels of inorganic phos- phate (1.8 2 1.0, 1.0 t 0.8, and 1.8 2 0.5 at 3, 7, and 11 h of the reperfusion, respectively). However, in the normo- thermic group within this period, the inorganic phos- phate was elevated compared with the control hemi- sphere and continued to increase (2.8 2 0.9, 5.1 t 4.8, and 9.0 ? 6.7 at 3, 7, and 11 h, respectively). By 11 h of reperfusion, the hypothermic group had a significantly lower level of inorganic phosphate as compared with the normothermic animals.
The hypothermic group had a constant normal level of creatine phosphate during the reperfusion period (1.0 t

350
permanent occlusion transient occlusion
Kozlowski et al.
a permanent occlusion
3 ume of occhslon [hrr]
b permanent occlusion
3 time of accluian Ihm]
C
3 7 1 1 lime of repwhrrlm [hml
transient occlusion
1 .2
1 .o
0.8 W hypothermia
0.6
W mmthermia
0.4
0.2
0.0 3 7 1 1
tlme of reperhuon I h n ]
transient occlusion
T 1 .o
0.8
0.6
0.4
0 2
00 3 7 1 1
tlme of repertusan [hn]
0.4, 1.0 ? 0.6, and 1.0 ? 0.2 at 3 , 7, and 11 h of reperfu- sion, respectively). The normothermic group showed a small variability of creatiiie phosphate levels following ischemia (e.g., 1.1 ? 0.3, 0.8 ? 0.0, and 0.9 ? 0.2). Only the value measured at 7 h of the reperfusion was signif- icantly lower then the control and there was no signifi- cant difference in creatine phosphate levels between two experimental groups.
Of the high energy phosphate measurements, ATP lev- els measured during the reperfusion period showed the greatest differences between normothermic and hypo- thermic animals. The hypothermic group had ATP levels near normal throughout the reperfusion period (0.9 -t 0.1, 1.0 ? 0.2, and 0.9 -t 0.1 at 3, 7 , and 11 h of reperh-
FIG. 4. Changes in P, (a), PCr (b), and ATP (c) levels during perma- nent ischemia (left) and reperfusion (right). Figures show the ratio of ischemic to control side of the brain. Dashed line corresponds to the value of ratio equal to 1. 0,00, ischemic/control ratio significantly different from 1 (P < 0.05 and P < 0.01 respectively). *, **, hypother- mic group significantly different from the normothermic group (P < 0.05 and P < 0.01, respectively).
sion). The normothermic group had slightly lower levels of ATP during the early part of the reperfusion period (0.9 t- 0.2 and 0.9 ? 0.2) , which finally dropped to a level significantly lower than the control value at 11 h of reperfusion (0.7 ? 0.0). There was a significant difference in ATP levels between the hypothermic and normother- mic group at the end of the reperfusion period.
NAA
NAA levels were expressed as a ratio of right to left values. They were measured at 1 and 5 h of permanent ischemia and at 1, 5, and 9 h of reperfusion after 3 h of ischemia (Fig. 5) . In the case of permanent ischemia,

Effect of Temperature in Focal Ischemia 351
permanent occlusion transient occlusion
1.4 - 1.4 -
1.2- 1.27
1 .o 1 .o
0.8 0.8
a hypothemla 0.6 0.6 nmothermla
0.4 0.4
0.2 0.2
0.0 0.0 0.5 4.5
time of occlusion [hn] 0.5 4.5 8.5
time of reperfusion [hn]
FIG. 5. Changes in NAA levels during permanent ischemia (left) and reperfusion (right). Figure shows the ratio of ischemic to control side of the brain. Dashed line corresponds to the value of ratio equal to 1. 0, ischemic/control ratio significantly different from 1 (P < 0.05); **, ***, hypothermic group significantly different from the normothermic group (P < 0.01 and P < 0.001. respectively).
hypothermic rats had a constant, normal level of NAA in the ischemic brain (1.0 ? 0.2 and 1.0 2 0.1 measured at 1 and 5 h of permanent occlusion). The normothermic group showed a slight decrease NAA levels ipsilaterally (0.9 2 0.1 and 0.9 * 0.1); however, these values were not significantly less than the controls.
During the reperfusion after 3 h of ischemia, the hypo- thermic group had near normal NAA levels (1.0 ? 0.0, 1.1 2 0.1, and 1.0 t 0.1 measured at 1, 5, and 9 h of the reperfusion). In contrast, normothermic animals showed a constant decrease in NAA levels during the whole reperfusion period (0.9 ? 0.0.0.8 t 0.1, and 0.7 -C 0.1 at 1 , 5 , and 9 h. respectively). Values measured at 5 and 9 h of the reperfusion period were significantly lower in the
permanent occlusion
I
1.5 5.5
time of occlusion [hn]
normothermic group when compared with the hypother- mic group.
Lactate The lactate editing method used in this study resulted in an acquisition of the NAA signal, which was about 10% of the nominal value (19). NAA on the control (left) side served as a reference for semiquantitative lactate mea- surements. Therefore the numbers reflect the changes in lactate levels rather than the ratios of absolute concen- tration of lactate and NAA in the region of interest. Lac- tate levels for the ischemic and control sides are pre- sented in Fig. 6. In the case of permanent occlusion, lactate levels were significantly elevated on the ischemic
transient occlusion
1.5 5.5 9.5 time of reperfision [hn]
hypothermia- ischemic hypothermia- control
Mnothermia - ischemic normothermia - control
FIG. 6. Changes in lactate levels during permanent ischemia (left) and repetfusion (right). Figure shows the ratio of lactate level on the ischemic and control sides to the NAA level on the control side of the brain. 00,000, ischemic side significantly different from the control side (P < 0.01 and P < 0.001. respectively): **, ***, hypothermic group significantly different from the normothermic group (P < 0.01 and P < 0.001. respectively); H, hypothermic group; N, norrnothermic group.

352 Kozlowski et al.
side of the brain during the entire period of ischemia for both the hypothermic (3.8 5 1.4 versus 0.8 -t 0.3, 5 .6 -t 1.0 versus 0.6 2 0.7) and normothermic (3.1 t 1.4 versus 0.6 2 0.3, 5.1 2 2.5 versus 1.1 2 0.2) groups. There was no statistically significant difference between lactate lev- els in two groups during permanent ischemia. The large standard deviations obtained appear to result from a large variability between animals since the signal to noise ratio and the spectral quality indicate a much smaller measurement error.
The reperfusion after 3 h of ischemia resulted in lactate levels near normal for the hypothermic group (2.2 2 1.5 versus 1.4 2 0.7, 2.0 2 0.6 versus 1.7 2 0.8, and 1.9 2 1.1 versus 1.3 +- 1.3 measured at 2, 6 , and 10 h of reperfu- sion, respectively). The normothermic group however had significantly elevated lactate levels throughout the whole reperfusion period (7.1 2 3.0 versus 1.3 ? 0.3, 6.2 2 1.9 versus 1.8 IT 0.7, and 5.9 It_ 1.0 versus 1.9 2 0.6 at 2, 6 , and 10 h, respectively). The lactate levels tended to decline as the reperfusion proceeded but all three values were significantly higher than the corresponding values for the hypothermic group.
DISCUSSION
The present study has used localized MR spectroscopy to examine the effect of temperature on the changes in cerebral high energy phosphates, lactate, NAA, and pH, which occur either during cerebral ischemia or at re- peated times after reperfusion. Since damage to the tissue was also assessed histopathologically in these animals, we were able to relate alterations in these metabolites directly to outcome: i.e., the degree of protection ob- served with hypothermia. Some of the important results of the study include the observation that (i) during nor- mothermia, infarction occurs after severe transient cere- bral ischemia despite a gradual recovery of pH and an early recovery of Pi. phosphocreatine, and ATP; (ii) with permanent cerebral ischemia, hypothermia did not sig- nificantly ameliorate ischemic changes in lactate, pH, NAA, or high energy phosphate metabolites or provide protection against infarction: (iii) during reperfusion with transient cerebral ischemia, animals that had under- gone a hypothermic ischemia had a better recovery of pH, lactate, and high energy phosphates and an improved pathological outcome compared with normothermic an- imals; and (iv) reductions in NAA progressively in- creased with time after reperfusion in the normothermic but not the hypothermic group, thereby correlating well with extent of pathological damage.
Changes in Metabolite Levels during Ischemia
It is well known that there is a decrease in ATP, an increase in inorganic phosphate and a decrease in phos- phocreatine during cerebral ischemia and such changes in phosphate metabolites were observed during perma- nent ischemia in the present study (6 , 8, 23-26). Mea- surements of ATP during cerebral ischemia are often difficult due to a low signal to noise ratio and, when reported, the reductions are often modest, e.g., a 17% decrease being reported previously during ischemia in a
rat focal model of hypoxia-ischemia (12). Presently, ATP within the ischemic hemisphere decreased approxi- mately 25% during MCA occlusion. This reduction is likely an underestimate due to partial volume effects related to a relatively large sample voxel resulting in spectra from tissue within the core, penumbra, and pe- riphery of the ischemic territory and the inclusion of temporalis muscle. A larger voxel size than is ideal is often unavoidable to obtain the necessary signal to noise within the sampling time constraints dictated by the physiological conditions. Variations in the T, and T, relaxation times with ischemia should also be considered a potential factor influencing the estimates of metabolite levels. However no changes in T, of major metabolites had been found in the studies of cerebral ischemia (27), and there have been conflicting reports regarding changes in T2, especially for proton metabolites (27-29), making it difficult to assess the true effect of transverse relaxation times during different stages of cerebral isch- emia.
With reperfusion following transient ischemia, there was initially a recovery of phosphate metabolites to- wards control levels in the first 3 h after ischemia. A recovery of ATP, PCr, and Pi is usually observed after transient focal or global ischemia or even during perma- nent focal ischemia (6, 8, 12, 26). Somewhat unexpected is that in the present study, as reperfusion continued there was a subsequent reduction of energy charge with a significant decrease in ATP and a trend for an increase in inorganic phosphate at 11 h of reperfusion. “Chronic” or secondary decreases in ATP have been observed 1 week after ischemic injury in the gerbil and by 48 h after hypoxic-ischemic injury in the piglet (30, 31). Such de- creases in ATP likely reflect the fact that many of the cells within the MCA territory are dying and have lost cellular function and integrity. Indeed, in the present animals, well developed neuronal necrosis and infarc- tion are evident in the histological sections obtained at 12 h of reperfusion.
It is also well established that during cerebral ischemia there is an accumulation of lactic acid associated with anaerobic glycolysis resulting in an intracellular acidosis (8, 9 , 24, 26, 32, 33). Thus, it was not surprising to observe reductions in pH and marked elevations in lac- tate during focal ischemia in the present study. However, the observation of dissociation between the recovery of intracellular pH and lactate during reperfusion was somewhat unexpected. Soon after removal of the clip on the MCA in the hypothermic group and by 11 h after its removal in normothermic animals, pH had returned to control levels but lactate levels continued to be markedly elevated in the normothermic group. Previous studies that have followed changes in lactate and pH after cere- bral ischemia have found some variability in their inter- relationship. Similar recoveries of the two or a slightly delayed recovery of lactate compared with pH (32, 33) have been observed after transient cerebral ischemia. However, in studies of chronic infarction, a prolonged elevation in lactate has also been reported (34-37). Some of these differences are likely related to differing severi- ties andlor types of cerebral ischemia being studied. The protracted high levels of lactate within cerebral infarcts

Effect of Temperature in Focal Ischemia 353
have been suggested to be the result of a low cerebral perfusion and poor washout of lactate, continued lactate generation or a production of lactate by phagocytic cells infiltrating the brain (34-36,38). None of these proposals likely explain the continued high levels of lactate after clip removal in the present study. With transient isch- emia, there is a reperfusion of the tissue sufficient to result in some recovery of ATP and pH but not lactate, particularly in normothermic animals. The partial and later full recoveries of pH also suggest that it is unlikely there is a continued production of lactate in the paren- chyma. Instead, elevated lactate levels appear related to final tissue damage and thus appear to provide the best early indicator of poor outcome. It is unlikely that this elevation in lactate corresponds to macrophage infiltra- tion as this is usually observed days and not hours after the insult. Instead, it is possible that transporters for lactate, which would help remove lactate from the neu- rons and from the extracellular space into the blood andlor CSF appear to be impaired by ischemia so that the continued high lactate levels likely reflect high amounts of lactate remaining in damaged cells (39, 40). This would be consistent with a previous study in which a high level of lactate observed 24-48 h after cerebral infarction in rats was shown to be due to elevated levels of lactate produced before and not during that period (41).
N-acetyl-L-aspartate is the major contributor to a prom- inent resonance in the water-suppressed proton spec- trum from normal adult brain. Although the function of NAA remains poorly understood, evidence indicates that it is present predominantly if not exclusively in neurons (38, 42). NAA has been shown to be reduced after cere- bral ischemia in the rat or human as soon as 1 h or as long as 1 year after the insult (36, 43-45). The present study demonstrates that reductions NAA can be detected very early, within the first half hour after reperfusion. Even during ischemia, there was a trend for NAA to be de- creased but inter-animal variability was high, possibly because changes in physiological conditions can alter NAA concentrations. For example, application of high K' can cause an increase in extracellular NAA as mea- sured by microdialysis in rat cerebral cortex (39). Thus, depending on the severity or progression of the ischemic insult, NAA within the cells may be differentially af- fected.
Differences between Normothermia and Hypothermia
Similar to the results of Ridenour et al. (3), hypothermia produced a reduction in infarct volume in animals with transient but not permanent MCA occlusion. Although several groups have examined the effects of hypothermia on various metabolite levels, none have followed the changes of ATP, PCr, Pi, pH, lactate, and NAA in the same animals for 12 h of reperfusion and directly related these to subsequent pathological outcome. Thus, hypo- thermia has been demonstrated to retard the rate of high- energy phosphate depletion during ischemia and to pro- mote the post-ischemic rate of metabolic recovery (1, 6-9). However, the importance of these differences in providing neuroprotection is not clear since a reduction in ischemic damage occurs even if ATP is depleted and
lactate is elevated to similar levels in normothermic and hypothermic groups (23,30,46). Similarly, in the present study there was a statistically comparable reduction in ATP and PCr in normothermic and hypothermic groups during ischemia and a similar recovery in normothermic and hypothermic groups post-ischemia yet damage was greatest in the normothermic group. Thus, the reduction in ATP during ischemia and recovery post-ischemia does not predict outcome. Instead, the delayed secondary changes in ATP may provide a better prognostic indica- tor correlating better with the extent of pathological dam- age. Shortly after reperfusion, differences were greatest in the levels of lactate between normothermic and hypo- thermic groups suggesting that a lack of recovery of lac- tate is indicative of permanent brain damage. The changes occurring in NAA during and after normother- mic or hypothermic ischemia have not been studied ex- tensively, thus, the present study is the first to demon- strate a preservation of NAA with hypothermic ischemia and not normothermic ischemia. One of best late corre- lates with the extent of brain injury was a reduction in NAA that occurred early after ischemia in animals that had undergone normothermic but not hypothermic ischemia.
The present results do not resolve how hypothermia produces protection of the brain during ischemia. How- ever, the data do indicate that a better maintenance of high energy phosphates, reduced acidosis or decreased lactate accumulation during the ischemia do not readily account for the reduced damage observed in the hypo- thermic animals. The results also do not indicate a major role for a better recovery of high energy phosphate me- tabolism after hypoxia-ischemia in the hypothermic an- imals. During reperfusion higher levels of lactate and reduced levels of NAA may simply represent damaged tissue. However, a recovery of lactate toward normal levels after ischemia is likely predictive of a good out- come. In hypothermic animals, lactate accumulated to high levels within the brain during ischemia but on reperfusion homeostatic cellular mechanisms clearly re- mained functional so that lactate levels returned to con- trol correlating well with reduced infarct size.
REFERENCES 1. M. D. Ginsberg. L. L. Sternau, M. Y.-T. Globus, W. D. Dietrich. R. Busto,
Therapeutic modulation of brain temperature: relevance to ischemic brain injury. Cerebruvasc. Brain Metab. Rev. 4. 189-225 (1992).
2. S. Nurso. D. Corbett. Direct measurement of brain temperature during and after intraischemic hypothermia: correlation with behavioral. physiological, and histological endpoints. 1. Neurosci. 14, 7726-7734 (1994).
3. T. R. Ridenour, D. S. Warner, M. M. Todd, A. C. McAllister, Mild hypothermia reduces infarct size resulting from temporary but not permanent focal ischemia in rats. Stroke 23, 733-738 (1992).
4. H . Chen. M. Chopp, Z. G. Zhang, J. H. Garcia, The effect of hypother- mia on transient middle cerebral artery occlusion in the rat. 1. Cereb. Blood Flow Metob. 12. 621-628 (19921.
5 . Q. Jiang, M. Chopp. Z. G. Zhang, J . A. Helpern. R. 1. Ordidge, J. Ewing, P. Jiang. B. A. Marchese, The effect of hypothermia on transient focal ischemia in rat brain evaluated by diffusion- and perfusion-weighted NMR imaging. 1. Cereb. Blood Flow Metab. 14. 732-741 (19941.
6. M. Chopp. R. Knight, C. D. Tidwell, J. A. Helpern, E. Brown, K. M. A. Welch. The metabolic effects of mild hypothermia on global cerebral ischemia and recirculation in the cat: comparison to normothermia and hyperthermia. 1. Cereb. Blood Flow Metab. 9, 141-148 (1989).
7. T. Hosaka. Y. L. Yamamoto. M. Diksic, Efficacy of retrograde perfu-

354 Kozlowski et al.
sion of the cerebral vein with verapamil after focal ischemia in rat brain. Stroke 22, 1562-1566 (1991).
8. 0. Haraldseth. T. Gronas, T. Southon. L. Thommessen, G. Borchgre- vink, P. Jynge. S. E. Gisvold. G. Unsgard. The effects of brain temper- ature on temporary global ischemia in rat brain. A 31-phosphorous NMR spectroscopy study. Acto Anoesthesiol, Scond. 36. 393-399 (1992).
9. G. R. Sutherland. H. Lesiuk. P. Hazendonk. J . Peeling, R. Buist. P. Kozlowski. A. Jasinski. J. K. Saunders, Magnetic resonance imaging and 31P magnetic resonance study of the effect of temperature on ischemic brain injury. Con. j . Neurol. Sci. 19, 317-325 (1992).
10. M. E. Moseley. Y. Cohen. 1. Mintorovitch. L. Chileuitt. H. Shimizu, J. Kucharczyk. M. F. Wendland. P. R. Weinstein. Early detection of regional cerebral ischemia in cats: comparison of diffusion- and T,- weighted MRI and spectroscopy. Magn. Reson. Med. 14. 330-346 (1990).
11. K. Houkin. T. Nakada, N. Suzuki, 1. L. Kwee, ."P magnetic resonance spectroscopy of chronic cerebral infarction in rats. NMR Biomed. 2. 83-86 (1989).
12. 1. M. Germano. L. H. Pitts. 1. Berry. S. 1. De Armond. High energy phosphate metabolism in experimental permanent focal cerebral ischemia: an iri vim J I P magnetic resonance spectroscopy study. J. Cereb. Blood Flow Metab. 8. 74-31 (1988).
13. J. van der Grond. R. Balm, L. J. Kappelle. B. C. Eikelboom. W. P. Mali, Cerebral metabolism of patients with stenosis or occlusion of the internal carotid artery. A 'H-MR spectroscopic imaging study. Stroke
14. S. H. Graham, D. J. Meyerhoff. L. Bayne. F. R. Sharp, M. W. Weiner, Magnetic resonance spectroscopy of N-acetylaspartate in hypoxic- ischemic encephalopathy. Ann. Neurol. 35. 490-494 (1994).
15. P. Kozlowski. A. Jasinski. G. R. Suthcrland, J. Peeling, A. M. Buchan. J. K. Saunders. Magnetic resonance evaluation of regional brain in- jury following cerebral ischemia. Can. ]. Appl . Spsctr. 37, 106-111 (19921.
16. J . W. Hugg. G. B. Matson, D. B. Twieg, A. A. Maudsley. D. Sappey- Marinicr. M. W. Weiner, Phosphorus-31 MR spectroscopic imaging (MRSI) of normal and pathological human brains. Mogn. Reson. Im- aging 10, 227-243 (1992).
17. L. H. Chang, Y. Cohen. P. R. Weinstein. L. Chileuitt, T. L. James, Interleaved 'H and "P spectroscopic imaging for studying regional brain injury. Magn. Reson. Imtiging 9, 223-227 (1991).
18. D. Bourgeois, C. Remy. Y. Lefur. P. Devoulon, A. L. Benabid, M. Decorps. Proton spectroscopic imaging: a tool for studying intracere- bra1 tumor models in rat. M o p . Reson. Med. 21. 10-20 (1991).
19. D. Bourgeois. P. Kozlowski. A highly sensitive lactate editing tech- nique for surface coil spectroscopic imagingin vivo. Mogn. Reson. Med. 29, 402-406 (1993).
20. A. M. Buchan, D. Xue. A. Slivka, A new model of temporary focal neocortical ischemia in the rat. Stroke 23. 273-279 (1992).
21. P. Kozlowski. D. Bourgoois. A. M. Buchan. D. Xue, J. F. Shen. J. K. Saunders. ."P and 'H spectroscopic imaging studies of focal ischemia in rat brain. Con. 1. Appl. Speclr. 40, 1-8 (1995).
22. G. I. Kost, pH standardization for phosphorous-31 magnetic reso- nance heart spectroscopy at different temperatures. Mogn. Reson. Med. 14. 496-506 (1990).
23. R. Busto, W. D. Dietrich. M. Y.-T. Globus, 1. Baldes, P. Scheinberg. M. D. Ginsburg, Small differences in intraischemic brain temperature critically determine the extent of ischemic neuronal injury. 1. Cereb. Blood Flow Metobol. 7. 729-738 (1987).
24. H. A. Crockard. D. G. Gadian, R . S. J. Frackowiak, E. Proctor, K. Allen, S. R. Williams, R. W. R. Russell. Acute cerebral ischaemia: concurrent changes in cerebral blood flow, energy metabolites. pH. and lactate measured with hydrogen clearance and "P and 'H nuclear magnetic resonance spectroscopy. 11. Changcs during ischaemia. J . Cereb. Blood Flow Metob. 7 , 394-402 (1987).
25. K . L. Allen. A. L. Busza. E. Proctor, M. D. King. S.R. Williams, H. A. Crockard, D. G. Gadian. Controllable graded cerebral ischaemia in the gerbil: studies of ccrebral blood flow and energy metabolism by hydrogen i:li:arance and ."P NMR spectroscopy. NMR Biomed. 6 . 181-186 (lY93).
26. K. A. Conger. J. H. Halsey, K. -L. Luo. M. -J . Tan. G . M. Pohost. H. P. Hetherington. Concomitant EEG, lactate. and phosphorus changes by 'H and .j'P NMR spectroscopy during repeated brief cerebral isch- emia. /. Cereb. Blood Flow Metcib. 15, 26-32 (1995).
27. K. Kamada. K. Houkin. K. Hida. H. Matsuzawa. Y. twasaki. H. Abe, T.
26. 822-828 (1995).
Nakada. Localized proton spectroscopy of focal brain pathology in humans: significant effects of edema on spin-spin relaxation time. Magn. Reson. Med. 31, 537-540 (1994).
28. P. Gideon. 0. Henriksen, In vivo relaxation of N-acetyl-aspartate, creatine plus phosphocreatine,and choline containing compounds during the course of brain infarction: a proton MKS study. Mogn. Reson. Imaging 10. 983-988 (1992).
29. J. Kuhmonen. J. Sivenius. P. J. Riekkinen. R. A. Kauppinen. Decrease in brain choline-containing compounds following a short period of global ischemia in gerbils as detected by 'H NMR spectroscopy in vivo. N M R Biomed. 7. 231-236 (1994).
30. F. A. Welsh, R. E. Sims. V. A. Harris, Mild hypothermia prevents ischemic injury in gerbil hippocampus. 1. Cereb. Blood Flow Metobol. 10, 557-563 (1990).
31. A. Lorek. Y. Takei. E. B. Cady. J. S. Wyatt, J. Penrice. A. D. Edwards, D. Peebles. M. Wylezinska, H. Owen-Reece, V. Kirkbride. C. E. Coo- per. R. F. Aldridge, s. C. Roth. G. Brown, D. T. Delpy, E. 0. R. Reynolds, Delayed ("secondary") cerebral energy failure after acute hypoxia-ischemia in the newborn piglet: continuous 48-hour studies by phosphorus magnetic resonance spectroscopy. Pediotr. Res. 36, 699-706 (1994).
32. L. Cyulai, M. Schnall. A. C. McLaughlin. J. S. Leigh, Jr.. B. Chance, Simultaneous "P and 'H-nuclear magnetic resonance studies of hyp- oxia and ischemia in the cat brain. J. Cereb. Blood Now Metob. 7,
33. K. Allen, A. L. Busza. H. A. Crockard. R. S. J . Frackowiak. D. G . Gadian. E. Proctor. R. W. R. Russell, S. R. Williams. Acute cerebral ischaeniia: concurrent changes in cerebral blood flow, energy metab- olites, pH, and lactate measured with hydrogen clearance and "P and 'H nuclear magnetic resonance spectroscopy. 111. Changes following ischaemia. /. Cereb. Blood Flow Metob. 8. 816-821 (1988).
34. K. Houkin, K. Kamada. H. Kamiyama. Y. Iwasaki, H. Abe. T. Kashi- waba, Longitudinal changes in proton magnetic resonance spectros- copy in cerebral infarction. Stroke 24, 1316-1321 (1993).
35. G. D. Graham, A. M. Blamire. A. M. Howseman, D. L. Rothman. P. B. Fayad. L. M. Brass, 0. A. C. Petroff. R. G. Shulman. J. W. Prichard. Proton magnetic resonance spectroscopy of cerebral lactate and other metabolites in stroke patients. Stroke 23, 333-340 (19921.
38. H. Lanfermann, H. Kugel, W. Hrindel. K. Herholz, W. D. Heiss. K. Lackner. Metabolic changes in acute and subacute cerebral infarc- tions: findings at proton MR spectroscopic imaging. Radiology 196.
37. K. Houkin, 1. L. Kwee. T. Nakada. Persistent high lactate level as a sensitive MR spectroscopy indicator of completed infarction. J. Neu- rosurg. 72. 763-766 (1990).
38. B. L. Miller, A review of chemical issues in 'H NMR spectroscopy: N-acetyl-L-aspartate, creatine and choline NMR Biomed. 4, 47-52 (1991).
39. W. G. Kuhr. C. I . van den Berg, J. Korf. In vivo identification and quantification of carrier-mediated transport of lactate at the cellular level in the striatum of conscious freely moving rats. J . Cereb. Blood Flow Metob 8, 848-856 (1988).
40. W. Walz, S. Mukerji. Lactate release from cultured astrocytes and neurons: a comparison. Glia 1. 366-370 (1988).
41. T. Nakada. K. Houkin, K. Hida. 1. L. Kwee. Rebound alkalosis and persistent lactate: multinuclear ('Ha 'T, "P) NMR spec:troscopic studies in rats. Mogn. Reson. Med. 18, 9-14 (1991).
42. D. L. Birken. W. H. Oldendorf, N-acetyl-l-aspartic acid: a literature review of a compound prominent in 'H-NMR spectroscopic studies of brain. Neurosci. Neurobehov. Rev. 13, 23-31 (1989).
43. M. Peres, D. Bourgeois, S. Koussel. Y. Lefur. P. Devoulon. C. Remy. B. Barrere, M. Decorps, E. Pinard. D. Riche, A-L. Benabid, J. Seylaz. Two-dimensional 'H spectroscopic imaging for evaluating the local metabolic response to focal ischemia in the conscious rat. NMR Biomed. 5, 11-19 (1992).
44. S. H. Graham. D. J. Meyerhoff. L. Bayne. F. R. Sharp, M. W. Weiner. Magnetic: resonance spectroscopy of N-acetylaspartate in hypoxic- ischcmic encephalopathy. Ann. Neurol. 35, 490-494 (1994).
45. G. D. Graham. P. Kalvach. A. M. Blamire. L. M. Brass, P. 8. Fayad. J. W. Prichard. Clinical correlates of proton magnetic resonance spec- troswpy findings after acute cerebral infarction. Stroke 26. 225-229 (1995).
46. B. Lin, R. Busto. M. Y.-T. Glohus. E. Martinez, M. D. Ginsberg. Brain temperature modulations during global ischemia fail to influence extracellular lactate levels in rats. SIroke 26, 1634-1638 (1995).
543-551 (1987).
203-210 (1995).