Embed Size (px)
Citation preview

Effe
trea
hea
Murat Alkurt, DD
This study was supported by ProjecInternational Congress of the Acade
aResearch Assistant, Department ofbProfessor, Department of ProsthodcResearch Assistant, Department of
Alkurt et al
ct of repair resin type and surface
tment on the repair strength of
t-polymerized denture base resin
S,a Zeynep Yesil Duymus, DDS, PhD,b andMustafa Gundogdu, DDSc
Faculty of Dentistry, Atatürk University, Erzurum, Turkey; Facultyof Dentistry, Recep Tayyip Erdo�gan University, Rize, Turkey
Statement of Problem. Acrylic resin denture fracture is common in prosthodontic practice. When fractured denture bases arerepaired, recurrent fractures frequently occur at the repair surface interface or adjacent areas.
Purpose. The purpose of this study was to evaluate the effect of different surface treatments on the flexural strength ofthe acrylic resin denture base repaired with heat-polymerized acrylic resin, autopolymerizing resin, and light-polymerizedacrylic resin.
Material and Methods. Ninety-six specimens of heat-polymerized acrylic resin were prepared according to the AmericanDental Association Specification No. 12 (65.0 � 10.0 � 2.5 mm) and sectioned into halves to create a repair gap (3.0 �10 � 2.5 mm). The sectioned specimens were divided into 3 groups according to their repair materials. The specimens fromeach group were divided into 4 subgroups according to their surface treatments: a control group without any surfacetreatment; an experimental group treated with methyl methacrylate monomer (MMA group); an experimental group treatedwith airborne-particle abrasion with aluminum oxide particles of 250-mm particle size (abrasion group); and an experimentalgroup treated with erbium:yttrium-aluminum-garnet laser (laser group). After the surface treatments, the 3 materials wereplaced into the repair gaps and then polymerized. After all of the specimens had been ground and polished, they were storedin distilled water at 37�C for 1 week and subjected to a 3-point bend test. Data were analyzed with a 2-way analysis ofvariance, and the Tukey honestly significant difference test was performed to identify significant differences (a¼.05). Theeffects of the surface treatments and repair resins on the surface of the denture base resin were examined with scanningelectron microscopy.
Results. Significant differences were found among the groups in terms of repair resin type (P<.001). All surface-treatedspecimens had higher flexural strength than controls, except the surface treated with the methyl methacrylate in the heat-polymerized group. A significant difference between the control and abrasion groups (P¼.013) was found. The scanningelectron microscopy observations showed that the application of surface treatments modified the surface of the denturebase resin.
Conclusions. The repair procedure with heat-polymerized resin exhibited significantly higher flexural strength thanthat of the autopolymerized and light-polymerized resins. In addition, the airborne-particle abrasion with aluminumoxide particles of 250-mm particle size improved the flexural strength of the specimens tested. (J Prosthet Dent2014;111:71-78)
t No. 2005/102 (Atatürk University). A poster presentation of this study was presented at the 10thmy of Prosthodontics and Gnathological Society, April 2012, Antakya, Turkey.
Prosthodontics, Faculty of Dentistry, Atatürk University.ontics, Faculty of Dentistry, Recep Tayyip Erdo�gan University.Prosthodontics, Faculty of Dentistry, Atatürk University.

72 Volume 111 Issue 1
The Journal of
Clinical Implications
Based on the results of this study, heat-polymerized acrylic resin canbe used to repair acrylic resin denture base. Autopolymerizing resin orlight-polymerized acrylic resin may be the method of choice in a dentalpractice. This study also suggests that airborne-particle abrading thesurface of acrylic resin denture base with 250-mm aluminum oxideparticles enhances the repair.
Although acrylic resins have goodesthetic properties and are easily man-ipulated, they have low fracture re-sistance,1-4 and fractured acrylic resindenture bases are often encountered.1,5
Midline fractures occur twice as often inmaxillary prostheses as in mandibularprostheses.1,6-8 Extensive relief areas,hard and soft tissue undercuts, unbal-anced occlusion, fatigue during masti-cation, and traumatic events (such asdropping the dental prosthesis) inducefractures.1,2,7-12
Fractured denture bases are com-monly repaired, because it is expen-sive and time consuming to remake thedental prosthesis. A satisfactory repairshould have adequate strength10,13-15
and color10,11,13,14 and should beeasy to undertake,10,11 quick,10,11,13,14
dimensionally stable,10,11,13,15 and costeffective.13,14
Heat-polymerized,16 autopolymeriz-ing,17 and light-polymerized acrylicresins15 are used in the repair processesof base materials. The mechanical andchemical properties of acrylic resinsimprove as the temperature during poly-merization is raised.18 Autopolymerizingresins are usually preferred in the repairprocess because they can be applied ina short time and are inexpensive andeasy to use.11-18
The ratio of the repair area strengthto the original strength is 75% to 80%when heat-polymerized acrylic resinsare used17 and 60% to 69% when au-topolymerizing resins are used.9,16 Al-though some research studies5,9,19 havefound that autopolymerizing resinshave a lower flexural strength than heat-polymerized acrylic resins, other studieshave found that they have similar flex-ural strengths.20-22
Prosthetic Dentis
Light-polymerized acrylic resins havevarious advantages, such as superiorstrength, ease of fabrication, ease ofmanipulation, short polymerizationtime, and absence of liquid mono-mer.23-25 The use of light-polymerizedacrylic resin systems for direct intraoralrelining of removable dental prosthesesand the fabrication of denture baseswithout flasking has recently becomepopular.25,26 Polyzois et al27 reportedthat the repair strength was 13 MPa forautopolymerizing resins, 21 to 34 MPafor heat-polymerized acrylic resins, and40 to 44 MPa for light-polymerizedacrylic resins. The authors concludedthat the repair strength was higher inthe heat-polymerized acrylic resins be-cause the base and repair materialshave similar chemical properties. Razaviet al28 reported that base materialsstiffened by light have sufficient strengthfor use as relining materials in clinicalapplications.
Various mechanical and chemical sur-face treatments have been used to improvethe bond strength between the base andrepair materials.29-31 Bur grinding,32
airborne-particle abrasion with 250-mmaluminum oxide (Al2O3) particles, carbondioxide laser application,33 immersion inmethyl methacrylate,20,34,35 and treat-ments with organic solvents such as chlo-roform,30,31,35 acetone,16,20,29-31,36 andmethylene chloride (dichloromethane)29,30
are among these processes. Recently,lasers have been found to provide arelatively safe and easy means of alteringthe surfaces of materials. Although la-sers have not been used to roughenpolymethyl methacrylate (PMMA) sur-faces before a repair process, they havebeen used to etch metals before theapplication of porcelain.37
try
Methylene chloride has a carcino-genic potential38-42; therefore, ethylacetate is used in chemical surfacetreatments as a safer alternative. Therepair strength achieved by applyingethyl acetate for 120 seconds duringthe repair process was equal to thatof applying methylene chloride for 5seconds.43 Shen et al31 reported thatchloroform exposure for 5 secondswas sufficient and that longer chloro-form exposure impaired the structureof the repaired surface of the basematerial.
Some of the studies6,9-11,15,27,44-46
applied a 1.5- to 3-mm distance be-tween the repair surfaces, whereas otherstudies allowed a 10-mm distance be-tween the 2 surfaces.47 Beyli and vonFraunhofer48 reported that the colordifferences between the repair materialand the denture base material de-creased with a decline in the poly-merization contraction level when themaximum distance between the repairsurfaces was 3 mm.
Adhesion between the denture basematerial and the repair material mayincrease depending on the chemicalsapplied to the acrylic resin surface.These chemicals cause morphologicchanges by roughening the surface.Normally, this roughness can be createdby immersing the surface in an acrylicresin monomer.16,31,49
In spite of the high frequency ofdenture fractures, little information isavailable about the effects of surfacetreatments on the repaired prostheses.Therefore, the purpose of this studywas to investigate the effects of var-ious surface treatments on the repairstrength between the baseplate andheat-polymerized, autopolymerizing, and
Alkurt et al

Table I. Two-way analysis of variance to evaluate significant differencesamong groups
Source Sum of Squares Df Mean Square F P
Repair resin 162098 2 81049 273 <.001
Surface treatment 3184 3 1061 4 .017
Repair resin� surface treatment 5208 6 868 3 .012
Error 24905 84 296
Total 497077 96
Table II. Mean flexural strength and standard deviation for repaired acrylic resinspecimens subjected to different surface treatments and use of various repair resins
Treatment Groups
HP AP LP
X (MPa) SD X (MPa) SD X (MPa) SD
Control, no treatment 106 21 21 9 14 4
Abrasion* 118 17 53 22 17 6
MMA 100 26 36 13 27 13
Lasery 127 29 34 10 15 4
HP, repaired with heat-polymerized acrylic resin; AP, repaired with autopolymerizing resin; LP, repairedwith light-polymerized acrylic resin; MMA, treated with methyl methacrylate monomer; X, mean;SD, standard deviation.*Airborne-particle abrasion with aluminum oxide particles.yErbium:yttrium-aluminum-garnet laser.
January 2014 73
light-polymerized acrylic resins used asrepair materials. The first null hypoth-esis was that the repair resin typewould increase the repair strength ofthe heat polymerized denture baseresin. The second null hypothesis wasthat the chemical and mechanical sur-face treatments would increase therepair strength of the heat-polymerizeddenture base resin.
MATERIAL AND METHODS
A power analysis found that 96specimens were needed to detect asignificant difference among 3 repairresins and 4 surface treatments (a totalof 12 groups) on the repair strength ofa heat-polymerized denture base resin.Ninety-six rectangular heat-polymerizedacrylic resin (DeTrey QC-20; DentsplyLtd) specimens (65.0 � 10.0 � 2.5mm) were prepared according toAmerican Dental Association Specifi-cation No. 1250 with conventionalprocessing methods.
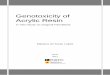
1 Scanning electron microscope image (�2000 magnification) of surface-treated heat-polymerized acrylic resins beforebonding. A, Control. B, Treated with methyl methacrylate monomer. C, Treated with abrasion. D, Treated witherbium:yttrium-aluminum-garnet laser.
Alkurt et al

2 Scanning electronmicroscope image (�2000magnification) of fractured heat-polymerized specimens. A, Control. B, Treatedwith methyl methacrylate monomer. C, Treated with abrasion. D, Treated with erbium:yttrium-aluminum-garnet laser.
74 Volume 111 Issue 1
The specimens were sectioned into 2halves to create a repair gap (3.0 �10 � 2.5 mm) and then divided into 3equal groups (32 specimens per group)according to the repair materials: re-paired with heat-polymerized acrylicresin (HP); repaired with autopolyme-rizing resin (AP) (Takilon; Rodent); andrepaired with light-polymerized acrylicresin (LP) (Versyo.com HD; HeraeusKulzer). The specimens in each group(HP, AP, and LP) were divided into 4subgroups (8 specimens per group)according to the surface treatments: agroup without any surface treatments(control group); an experimental grouptreated with methyl methacrylate mo-nomer for 120 seconds (MMA group);an experimental group treated withairborne-particle abrasion with 250-mmAl2O3 for 10 seconds at a pressure of0.2 MPa, from a distance of 10 mm(abrasion group); and an experimentalgroup processed with an erbium:yttrium-aluminum-garnet (Er:YAG) laser (Doctor
The Journal of Prosthetic Dentis
Smile Erbium & Diode Laser; LambdaSpA) at a wavelength of 2940 nm, a spotsize of 0.8 mm, a pulse frequency of 10Hz, a pulse energy of 150 mJ, and apulse duration of 100 ms (laser group).The laser was applied (scanning) for 60seconds under water irrigation. Duringthe laser application, the distance fromthe laser tip to the specimen was 10 mm.
The surface-treated and controlspecimens that were sectioned into 2halves were embedded in the dentureflask, with a metal mold (3.0 � 10 �2.5 mm) placed in the center of therepair gap for standardization. After thedenture flask was opened, the metalmold that formed the repair gap wasremoved. HP, AP, and LP were appliedto the repair gap of the surface-treatedand control specimens.
The specimens in the HP group werepolymerized by keeping the dentureflask in a thermal chamber (TermotronP-100; Termotron do Brazil Ltda) for9 hours once it reached boiling
try
temperature (74�C) by using the longboiling method. The specimens in theAP group were polymerized by keepingthem under pressure at 55�C for 15minutes. This process was carried outto enhance strength and decreaseporosity. The specimens in the LP groupwere polymerized by reapplying lightwith a UniXS polymerizing box (Her-aeus Kulzer) for 3 minutes for a finalpolymerization after a light applicationof 60 seconds for prepolymerization.When the polymerization processeswere complete, the specimens werecarefully removed from the dentureflask, and residual acrylic resin wasremoved with a tungsten carbide bur atlow speed. The specimens were moldedto the final shape with 600-grit abrasivepaper under running water. All speci-mens were stored in distilled water at37�C for 1 week before testing.
A 3-point bend test was performedimmediately after removing the speci-mens from the distilled water and
Alkurt et al

3 Scanning electron microscope image (�2000 magnification) of fractured autopolymerized specimens. A, Control.B, Treated with methyl methacrylate monomer. C, Treated with abrasion. D, Treated with erbium:yttrium-aluminum-garnet laser.
January 2014 75
without drying the specimens. This testwas carried out on a universal testingmachine (Model 2519-106; InstronCorp). A custom-made stainless steeldevice with a 50-mm span distancebetween the 2 supports was used, andthe crosshead speed was set at 5 mm/min. A load was applied in the centerof the specimens (center of the repairarea). The specimens were loadeduntil the first sound of a crack wasdetected, and the load (N) wasrecorded.
The flexural strength values ofeach specimen were calculated withthe following formula: S¼3WL/2bd2,where S is the flexural strength (inmegapascals), W is the fracture load (innewtons), L is the distance between thesupports (50 mm), b is the specimenwidth (10 mm), and d is the specimenthickness (2.5 mm).
To evaluate the effects of the surfacetreatments and repair resins on the
Alkurt et al
surface of the denture base resin, 4specimens (1 specimen each from thecontrol, MMA, abrasion, and lasergroups) were selected before repair, andrepresentative fractured specimens fromeach group were selected after the 3-point bend test. These selected speci-mens were gold-sputtered and examinedunder a field emission scanning electronmicroscope (SEM) (Zeiss EVO LS 10;Carl Zeiss) at 10.0 kV. The SEM photo-micrographs were made with �2000magnification for visual inspection. Inaddition, the nature of the failure wasnoted as adhesive (interface), cohesive(only at the repair material), or mixed(interface and repair material).
A 2-way analysis of variance(ANOVA) was used to study the effectsof the repair resin type, surface treat-ments, and their interaction on theflexural strength, followed by the Tukeyhonestly significant difference test witha confidence level of .05 to determine
the mean differences. The statisticalanalysis was performed with statisticalsoftware (SPSS v19.0; IBM Inc).
RESULTS
The 2-way ANOVA results are pre-sented in Table I. Significant differenceswere found for repair resin type(P<.001), surface treatments (P<.05),and their interaction (P<.05). Themean and standard deviation values offlexural strength for each of the experi-mental groups are presented in Table II.
The flexural strength of the speci-mens repaired with HP, AP, and LP wasdifferent (P<.001). The lowest flexuralstrength values were observed in the LPgroup (14 MPa to 27 MPa) and thehighest in the HP group (100 MPa to127 MPa).
All surface-treated specimens hadhigher flexural strength than the con-trols, except those treated with the

4 Scanning electron microscope image (�2000 magnification) of fractured light-polymerized specimens. A, Control.B, Treated with methyl methacrylate monomer. C, Treated with abrasion. D, Treated with erbium:yttrium-aluminum-garnet laser.
76 Volume 111 Issue 1
MMA in the HP group. A significantdifference was noted between the con-trol and abrasion groups (P¼.013).However, no significant differences werefound among the control, MMA, andlaser groups.
Representative SEM images of thecontrol, MMA, abrasion, and lasergroup specimens before bonding arepresented in Figure 1. The surfacetreatment resulted in irregularities andmany small pits on the surface of thedenture base resin. The SEM images ofthe representative surfaces of the frac-tured HP specimens are presented inFigure 2; AP specimens are presented inFigure 3; and LP specimens are pre-sented in Figure 4. For all specimens,adhesive failure was observed.
DISCUSSION
This study evaluated the effects ofrepair resin type and surface treatment on
The Journal of Prosthetic Dentis
the repair strength of a heat-polymerizeddenture base resin. For the repair resingroups, significant differences (P<.001)were found. Therefore, the first null hy-pothesiswasnot rejected. For the surface-treatment groups, the analysis found asignificant difference between the controland abrasion (P¼.013) groups. No sig-nificant differences were found amongthe control, MMA, and laser groups.Thus, the second null hypothesis waspartially rejected.
Ogle et al23 reported that light-polymerized acrylic resins had more ac-curate fit and higher strength than heat-polymerized acrylic resins. In this study,the highest repair strength was found inthe HP group, and the lowest repairstrength was in the LP group. Andreo-poulos et al51 found that repairs withlight-polymerized Triad VLC resin(Dentsply Intl Inc) had a much lowerstrength than those with autopolymeriz-ing resins. The authors concluded that
try
theflexural strengthwas lower in the light-polymerized Triad VLC acrylic resinbecause this material has high viscosityand poor adhesion as a repair material.The current study found that the speci-mens in the LP group have a lower repairstrength than the specimens in the APgroup. This result is compatible with thefindings of Andreopoulos et al.51 Theseresults may be attributable to a high rateof cross-linkingbetween similar resinbasematerials and to poor interaction andlack of adhesion or cohesion between theLP repairmaterial and the PMMA. The LPmaterial may not penetrate the PMMA.
Some researchers have reported thatexposing the repair surface to monomerincreases the bond strength.32,49 Olveraand de Rijk52 found that a 4-minuteexposure to monomer increased thefracture strength. Vallittu et al34 estab-lished that immersing the repair surfacesfor 180 seconds in methyl methacrylateincreased the transverse strength
Alkurt et al

January 2014 77
compared with shorter exposures. Expo-sure to monomer softens the PMMA,enhances the spread of superficial fis-sures, and forms pits in the bond sur-face.49 As a result, the repair materialdiffuses into the bond surface and de-velops adhesion. The increased repairstrength found with chemical surfacetreatments may be because of monomerinfiltration into the pits and cracks.
The results showed that HP had thehighest repair strength with the laserpretreatment, the AP with the abrasionpretreatment, and the LP with the MMApretreatment. These surface morpho-logic changes may enhance the me-chanical retention between the fracturedsurface and repaired acrylic resin.
The limitations of the study includethe absence of artificial aging withthermal cycling and the use of rectan-gular specimens instead of more com-plex denture shapes.53,54 In vitro studiesare limited in their ability to predict thesuccess of a material or technique in aclinical situation.22 Further in vitrostudies and clinical research are neces-sary to investigate the effects of differentlaser types on the bonding of the repairresin to the denture base resin.
CONCLUSIONS
1. The results showed that the HPgroup exhibited a significantly higherrepair strength than those of the APand LP groups.
2. The surface treatment to the repairsurface improved the flexural strength,except for the surface treated with theMMA in the HP group.
3. Pretreatment with abrasion pro-vided a significantly higher flexural st-rength than that found in the controls.
REFERENCES
1. Beyli MS, von Fraunhofer JA. An analysis ofcauses of fracture of acrylic resin dentures.J Prosthet Dent 1981;46:238-41.
2. Farmer JB. Preventive prosthodontics: maxil-lary denture fracture. J Prosthet Dent1983;50:172-5.
3. Morris JC, Khan Z, von Fraunhofer JA. Palatalshape and the flexural strength of maxillarydenture bases. J Prosthet Dent 1985;53:670-3.
Alkurt et al
4. Nimmo A, Kratochvil FJ. Preventing fracturesof maxillary overdentures. J Prosthet Dent1986;55:773-5.
5. Faot F, da Silva WJ, da Rosa RS, Del BelCury AA, Garcia RC. Strength of denture baseresins repaired with auto- and visible light-polymerized materials. J Prosthodont2009;18:496-502.
6. Stipho HD, Stipho AS. Effectiveness anddurability of repaired acrylic resin joints.J Prosthet Dent 1987;58:249-53.
7. Darbar UR, Huggett R, Harrison A. Denturefractureda survey. Br Dent J 1994;176:342-5.
8. Schneider RL. Diagnosing functional com-plete denture fractures. J Prosthet Dent1985;54:809-14.
9. Berge M. Bending strength of intact andrepaired denture base resins. Acta OdontolScand 1983;41:187-91.
10. Polyzois GL, Andreopoulos AG, Lagouvardos PE.Acrylic resin denture repair with adhesive resinand metal wires: effects on strength parame-ters. J Prosthet Dent 1996;75:381-7.
11. Polyzois GL, Tarantili PA, Frangou MJ,Andreopoulos AG. Fracture force,deflection at fracture, and toughness ofrepaired denture resin subjected tomicrowave polymerization or reinforcedwith wire or glass fiber. J Prosthet Dent2001;86:613-9.
12. Zappini G, Kammann A, Wachter W. Com-parison of fracture tests of denture basematerials. J Prosthet Dent 2003;90:578-85.
13. Ward JE, Moon PC, Levine RA, Behrendt CL.Effect of repair surface design, repair mate-rial, and processing method on the transversestrength of repaired acrylic denture resin.J Prosthet Dent 1992;67:815-20.
14. Ng ET, Tan LH, Chew BS, Thean HP. Shearbond strength of microwaveable acrylic resinfor denture repair. J Oral Rehabil 2004;31:798-802.
15. Stipho HD, Talic YF. Repair of denture baseresins with visible light-polymerized relinematerial: effect on tensile and shear bondstrengths. J Prosthet Dent 2001;86:143-8.
16. Rached RN, Del-Bel Cury AA. Heat-curedacrylic resin repaired with microwave-curedone: bond strength and surface texture. J OralRehabil 2001;28:370-5.
17. Leong A, Grant AA. The transverse strengthof repairs in poly methyl methacrylate. AustDent J 1971;16:232-4.
18. Foo SH, Lindquist TJ, Aquilino SA,Schneider RL, Williamson DL, Boyer DB.Effect of polyaramid fiber reinforcement on thestrength of 3 denture base poly methyl meth-acrylate resins. J Prosthodont 2001;10:148-53.
19. Ruyter IE, Svendsen SA. Flexural properties ofdenture base polymers. J Prosthet Dent1980;43:95-104.
20. Vojdani M, Rezaei S, Zareeian L. Effect ofchemical surface treatments and repairmaterial on transverse strength of repairedacrylic denture resin. Indian J Dent Res2008;19:2-5.
21. Ellakwa AE, El-Sheikh AM. Effect of chemicaldisinfectants and repair materials on thetransverse strength of repaired heat-polymerized acrylic resin. J Prosthodont2006;15:300-5.
22. Rached RN, Powers JM, Del Bel Cury AA.Repair strength of autopolymerizing, micro-wave, and conventional heat-polymerizedacrylic resins. J Prosthet Dent 2004;92:79-82.
23. Ogle RE, Sorensen SE, Lewis EA. A new visiblelight-cured resin system applied to removableprosthodontics. J Prosthet Dent 1986;56:497-506.
24. Shifman A. Clinical applications of visiblelight-cured resin in maxillofacial prosthetics,part I: denture base and reline materials.J Prosthet Dent 1990;64:578-82.
25. Fellman S. Visible light-cured denture baseresin used in making dentures with conven-tional teeth. J Prosthet Dent 1989;62:356-9.
26. Andreopoulos AG, Polyzois GL. Repair ofdenture resins using visible light-cured mate-rials. J Prosthet Dent 1994;72:462-8.
27. Polyzois GL, Handley RW, Stafford GD.Repair strength of denture base resins usingvarious methods. Eur J Prosthodont RestorDent 1995;3:183-6.
28. Razavi R, Khan Z, von Fraunhofer JA. Thebond strength of a visible light-cured relineresin to acrylic resin denture base material.J Prosthet Dent 1990;63:485-7.
29. Sarac YS, Sarac D, Kulunk T, Kulunk S. Theeffect of chemical surface treatments ofdifferent denture base resins on the shearbond strength of denture repair. J ProsthetDent 2005;94:259-66.
30. Seó RS, Neppelenbroek KH, Filho JN. Factorsaffecting the strength of denture repairs.J Prosthodont 2007;16:302-10.
31. Shen C, Colaizzi FA, Birns B. Strength ofdenture repairs as influenced by surfacetreatment. J Prosthet Dent 1984;52:844-8.
32. JaggerRG,al-AthelMS, JaggerDC,VowlesRW.Some variables influencing the bond strengthbetween PMMA and a silicone denture liningmaterial. Int J Prosthodont 2002;15:55-8.
33. Jacobsen NL, Mitchell DL, Johnson DL,Holt RA. Lased and sandblasted denture basesurface preparations affecting resilient linerbonding. J Prosthet Dent 1997;78:153-8.
34. Vallittu PK, Lassila VP, Lappalainen R.Wetting the repair surface with methylmethacrylate affects the transverse strengthof repaired heat-polymerized resin. J ProsthetDent 1994;72:639-43.
35. Minami H, Suzuki S, Minesaki Y,Kurashige H, Tanaka T. In vitro evaluation ofthe influence of repairing condition of den-ture base resin on the bonding of autopoly-merizing resins. J Prosthet Dent 2004;91:164-70.
36. Agarwal M, Nayak A, Hallikerimath RB.A study to evaluate the transverse strength ofrepaired acrylic denture resins with conven-tional heat-cured, auto polymerizing andmicrowave-cured resins: an in vitro study.J Indian Prosthodont Soc 2008;8:36-41.
37. Miserendino LJ, Pick RM. Lasers in dentistry.Chicago: Quintessence Publishing Co Inc;1995. p. 17-25.
38. National Toxicology Program. NTP toxi-cology and carcinogenesis studies ofdichloromethane (methylene chloride) (CASNo. 75-09-2) in F344/N rats and B6C3F1mice (inhalation studies). Natl Toxicol Pro-gram Tech Rep Ser 1986;306:1-208.

78 Volume 111 Issue 1
39. Dell LD, Mundt KA, McDonald M,Tritschler JP 2nd, Mundt DJ. Critical reviewof the epidemiology literature on the po-tential cancer risks of methylene chloride.Int Arch Occup Environ Health 1999;72:429-42.
40. Devereux TR, Foley JF, Maronpot RR,Kari F, Anderson MW. Ras proto-oncogeneactivation in liver and lung tumors fromB6C3F1 mice exposed chronically to meth-ylene chloride. Carcinogenesis 1993;14:795-801.
41. Kari FW, Foley JF, Seilkop SK, Maronpot RR,Anderson MW. Effect of varying exposureregimens on methylene chloride-induced lungand liver tumors in female B6C3F1 mice.Carcinogenesis 1993;14:819-26.
42. Maronpot RR, Devereux TR, Hegi M, Foley JF,Kanno J, Wiseman R, et al. Hepatic andpulmonary carcinogenicity of methylenechloride in mice: a search for mechanisms.Toxicology 1995;102:73-81.
43. Shimizu H, Ikuyama T, Hayakawa E, Tsue F,Takahashi Y. Effect of surface preparationusing ethyl acetate on the repair strength ofdenture base resin. Acta Odontol Scand2006;64:159-63.
44. Minami H, Suzuki S, Kurashige H,Minesaki Y, Tanaka T. Flexural strengths ofdenture base resin repaired with autopoly-merizing resin and reinforcements afterthermocycle stressing. J Prosthodont2005;14:12-8.
The Journal of Prosthetic Dentis
45. Yunus N, Harrison A, Huggett R. Effect ofmicrowave irradiation on the flexural strengthand residual monomer levels of an acrylicresin repair material. J Oral Rehabil 1994;21:641-8.
46. Moradians S, Fletcher AM, Amin WM,Ritchie GM, Purnaveja J, Dodd AW. Somemechanical properties including the repairstrength of two self-curing acrylic resins.J Dent 1982;10:271-80.
47. Lewinstein I, Zeltser C, Mayer CM, Tal Y.Transverse bond strength of repaired acrylicresin strips and temperature rise of denturesrelined with VLC reline resin. J Prosthet Dent1995;74:392-9.
48. Beyli MS, von Fraunhofer JA. Repair of frac-tured acrylic resin. J Prosthet Dent 1980;44:497-503.
49. Anusavice KJ, Phillips RW. Phillips’ science ofdental materials. 11th ed. Philadelphia: WBSaunders; 2003. p. 237-71.
50. Revised American Dental Association Speci-fication No. 12 for denture base polymers.J Am Dent Assoc 1975;90:451-8.
51. Andreopoulos AG, Polyzois GL,Demetriou PP. Repairs with visible light-curing denture base materials. QuintessenceInt 1991;22:703-6.
52. Olvera N, de Rijk WG. Effect of surfacetreatments on the repair strength of alight-activated denture repair resinusing censored data. Dent Mater 1994;10:122-7.
try
53. Bural C, Bayraktar G, Aydin I, Yusufo�glu I,Uyumaz N, Hanzade M. Flexural properties ofrepaired heat-polymerising acrylic resin afterwetting with monomer and acetone.Gerodontology 2010;27:217-23.
54. Pereira Rde P, Delfino CS, Butignon LE,Vaz MA, Arioli-Filho JN. Influence ofsurface treatments on the flexural strengthof denture base repair. Gerodontology2012;29:e234-8.
Corresponding author:Dr Zeynep Yesil DuymusRecep Tayyip Erdo�gan UniversityFaculty of DentistryDepartment of ProsthodonticsRizeTURKEYE-mail: [email protected]
Copyright ª 2014 by the Editorial Council forThe Journal of Prosthetic Dentistry.
Alkurt et al